

Finite Element Modeling of the Fingers and Wrist Flexion/Extension Effect on Median Nerve Compression


Abstract
1. Introduction
2. Materials and Methods
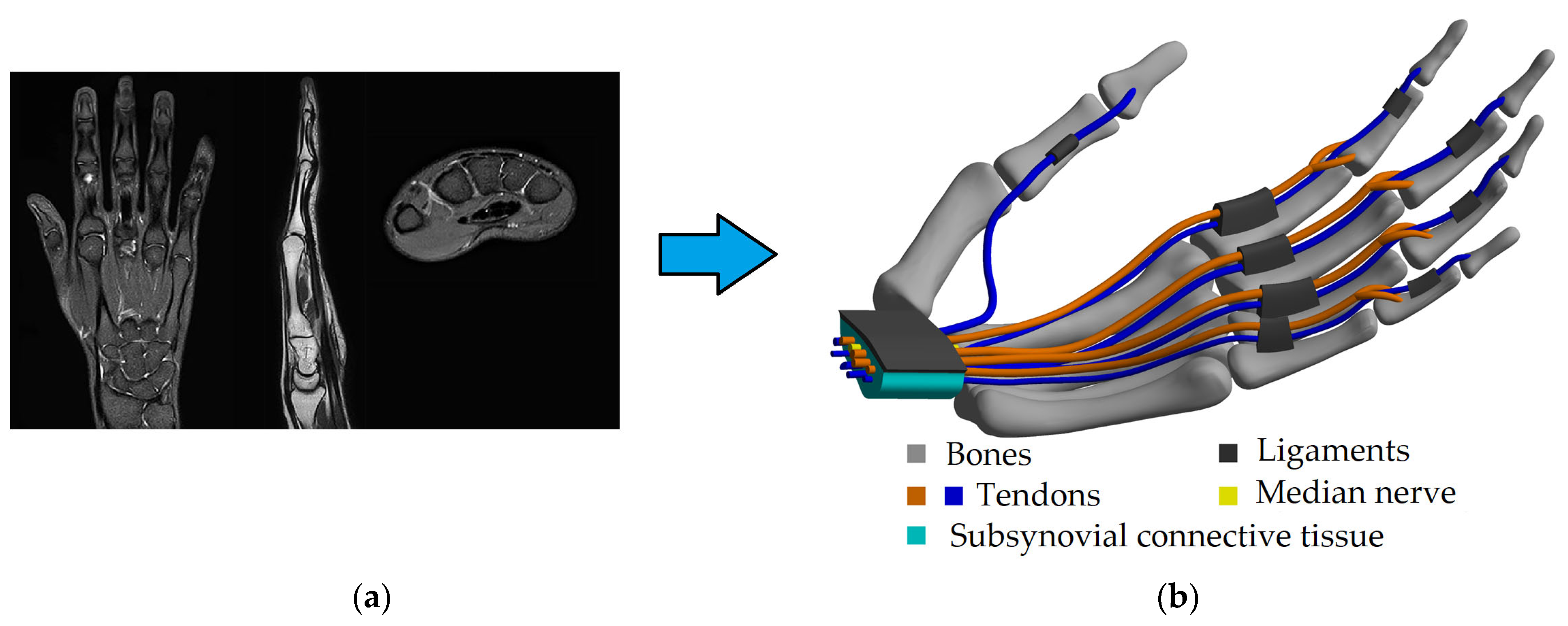
2.1. Geometry Modeling
2.2. Mechanical Properties
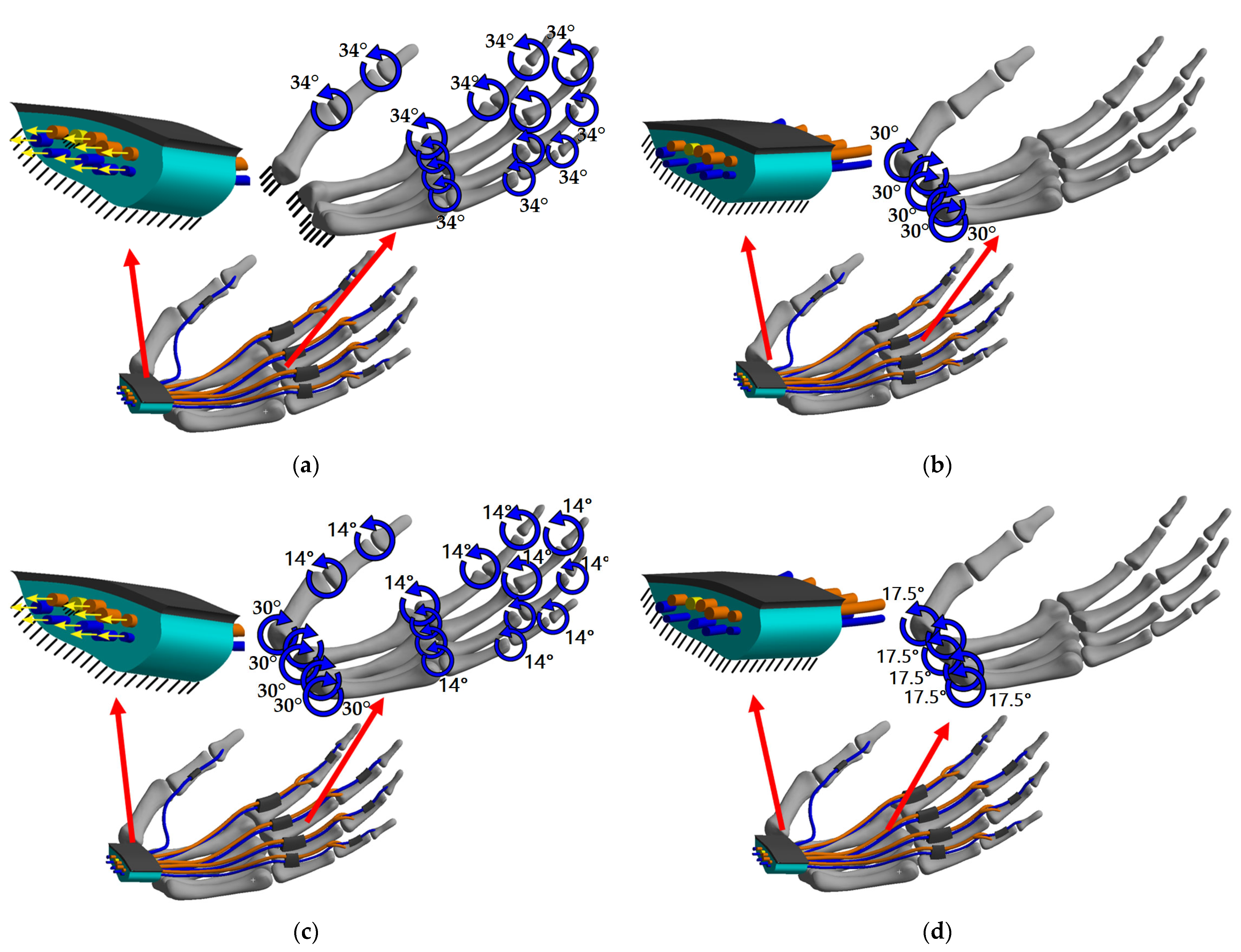
2.3. Boundary and Contact Conditions
2.3.1. Finger Flexion (Case 1)
2.3.2. Wrist Extension (Case 2)
2.3.3. Wrist Extension and Subsequent Fingers Flexion (Case 3)
2.3.4. Wrist Flexion (Case 4)
3. Results
3.1. Case 1: Fingers Flexion
3.2. Case 2: Wrist Extension
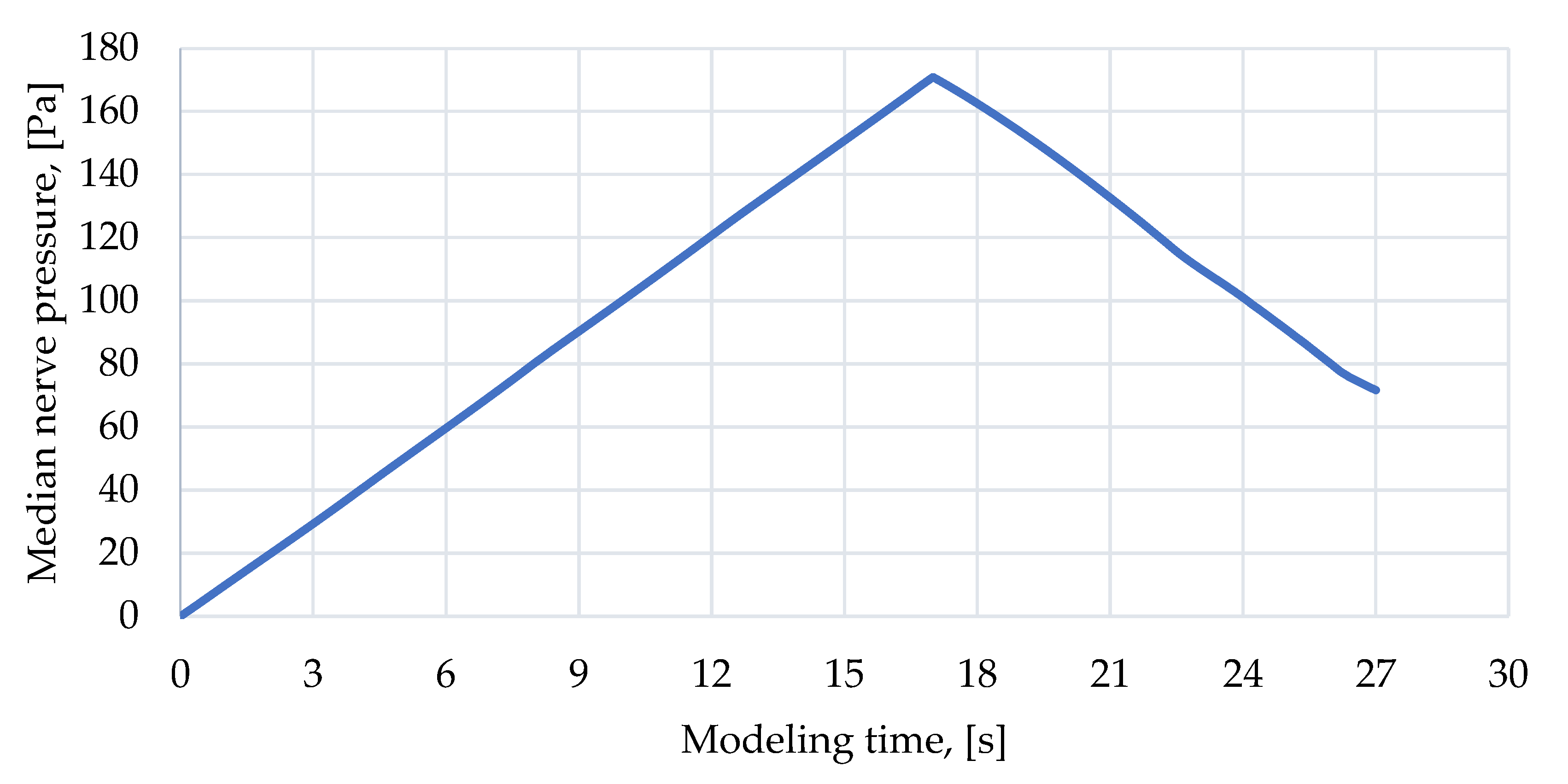
3.3. Case 3: Wrist Extension and Subsequent Fingers Flexion
3.4. Case 4: Wrist Flexion
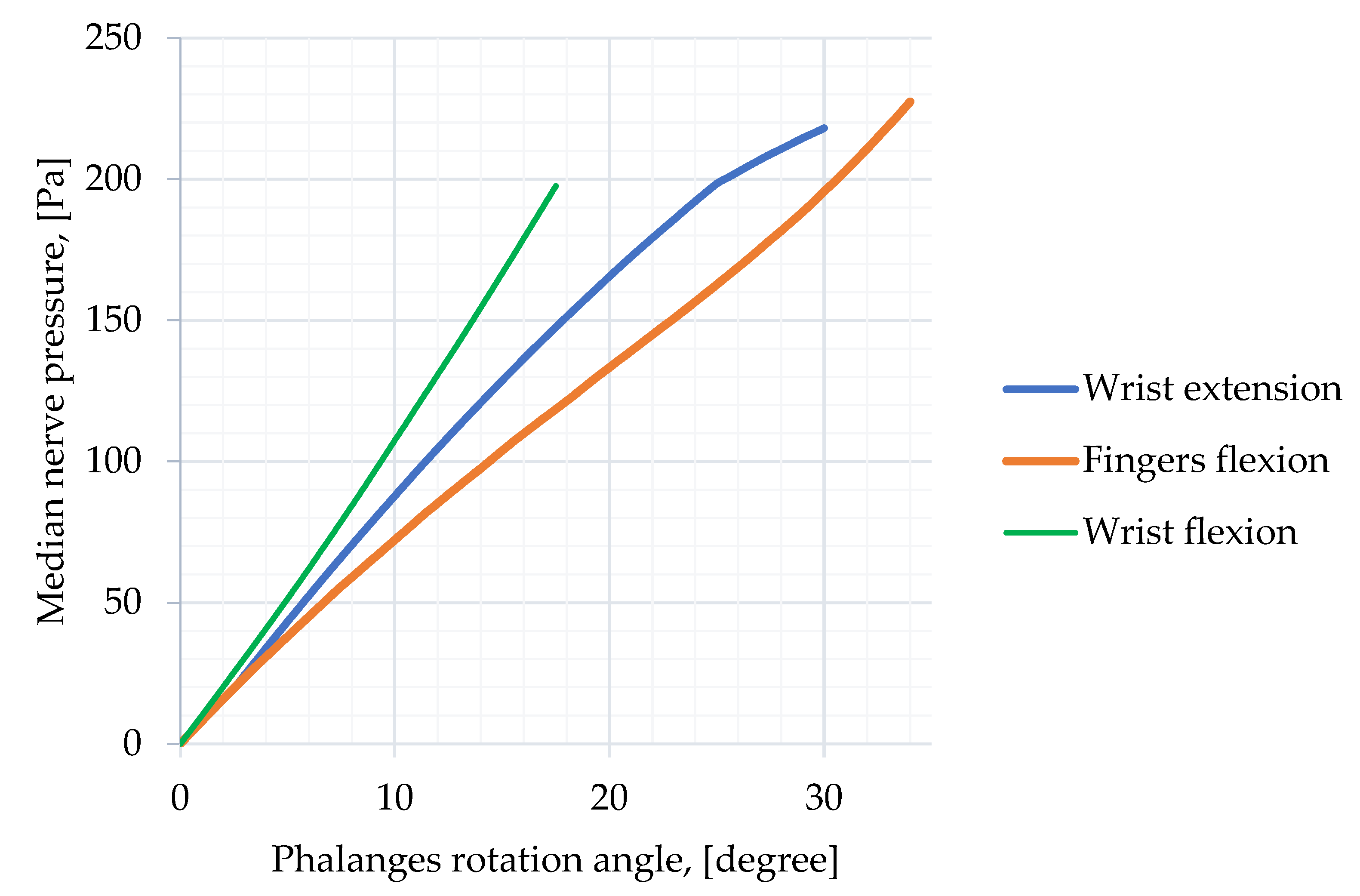
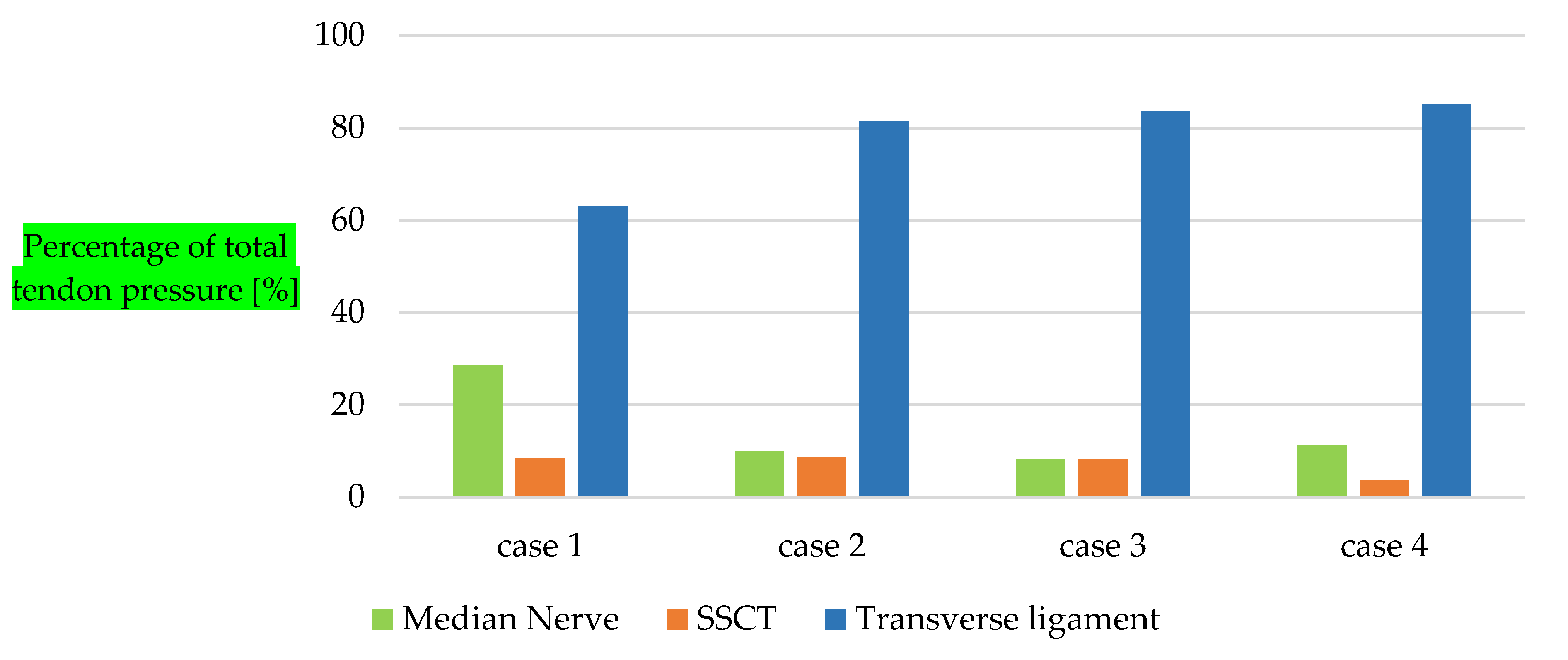
3.5. Comparison of Compression Rate
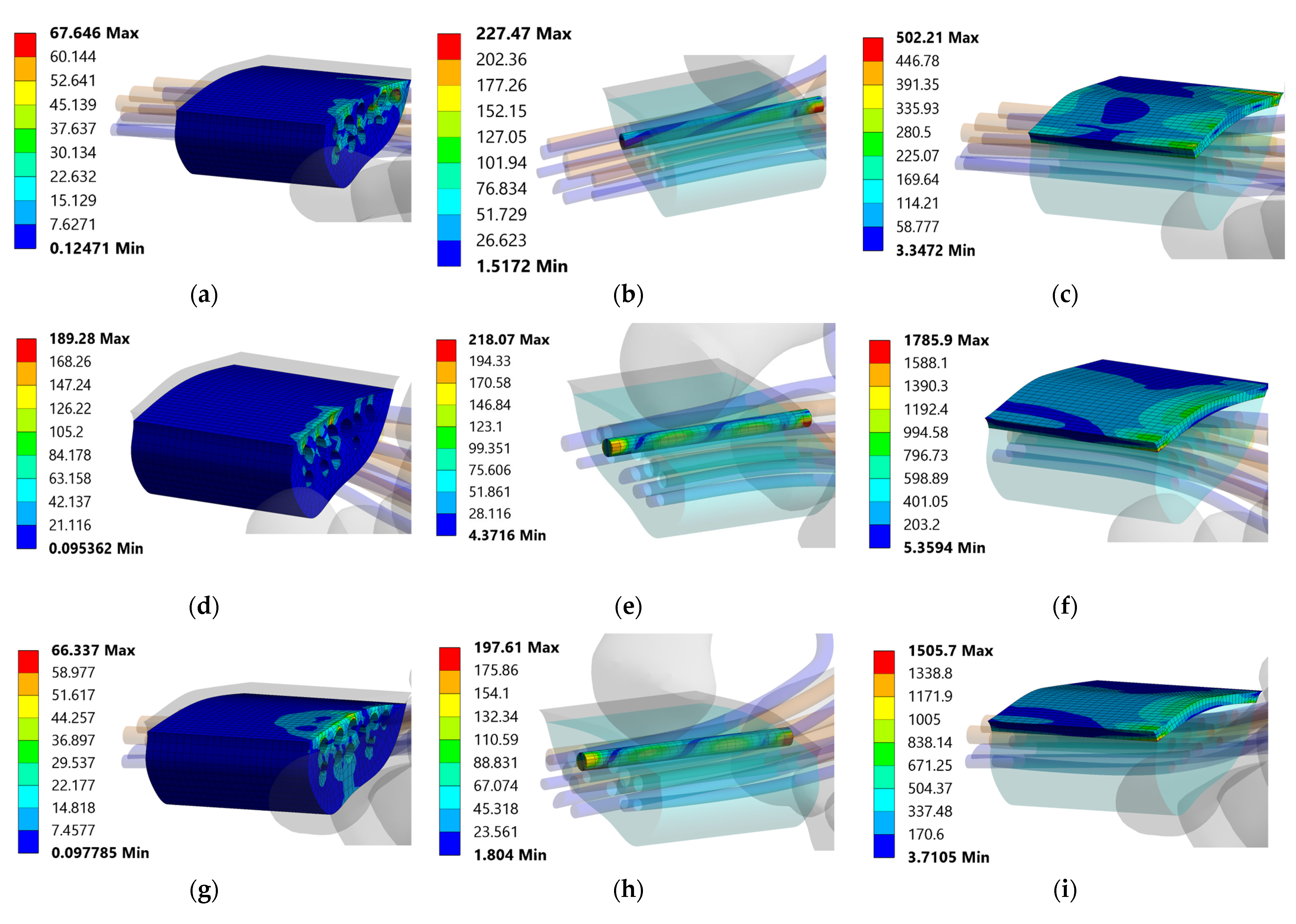
3.6. Pressure Distribution
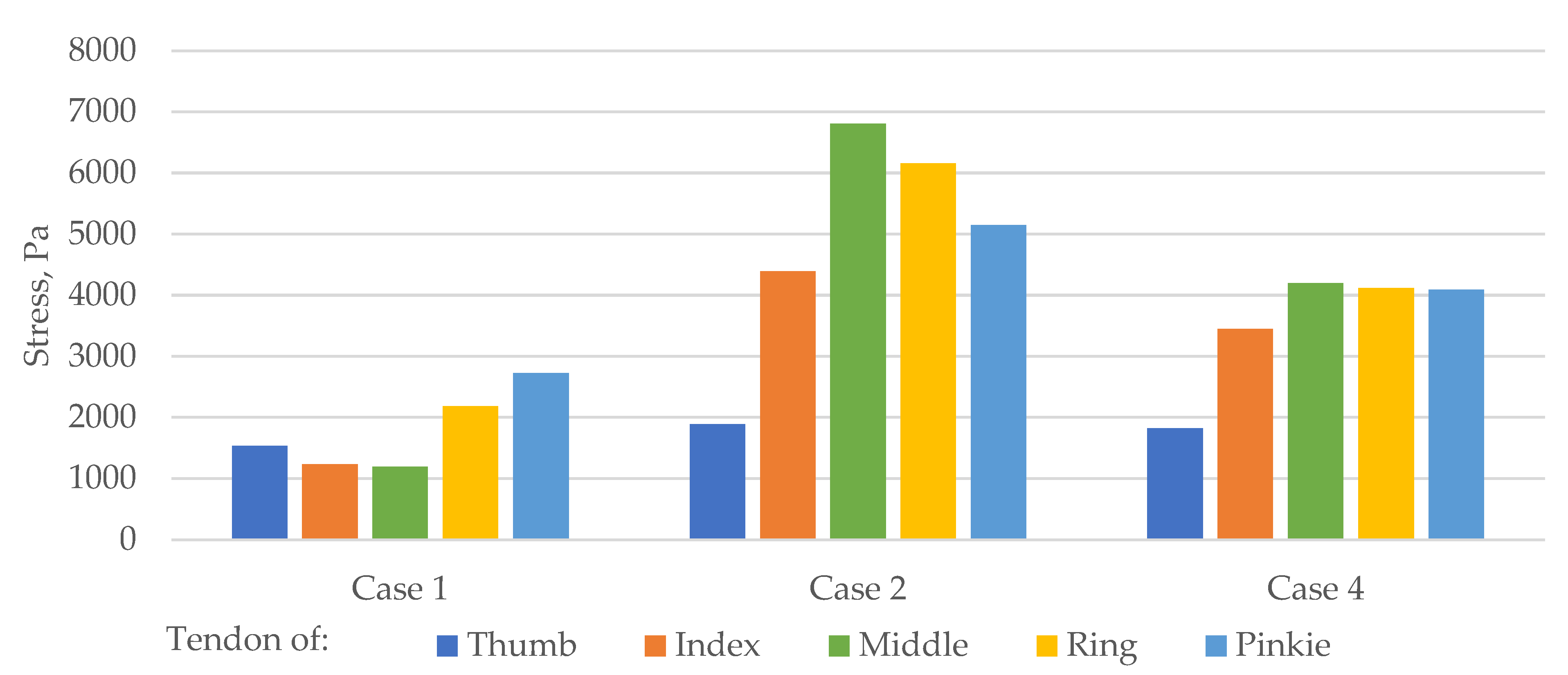
3.7. Tendon Stress in Carpal Tunnel Area
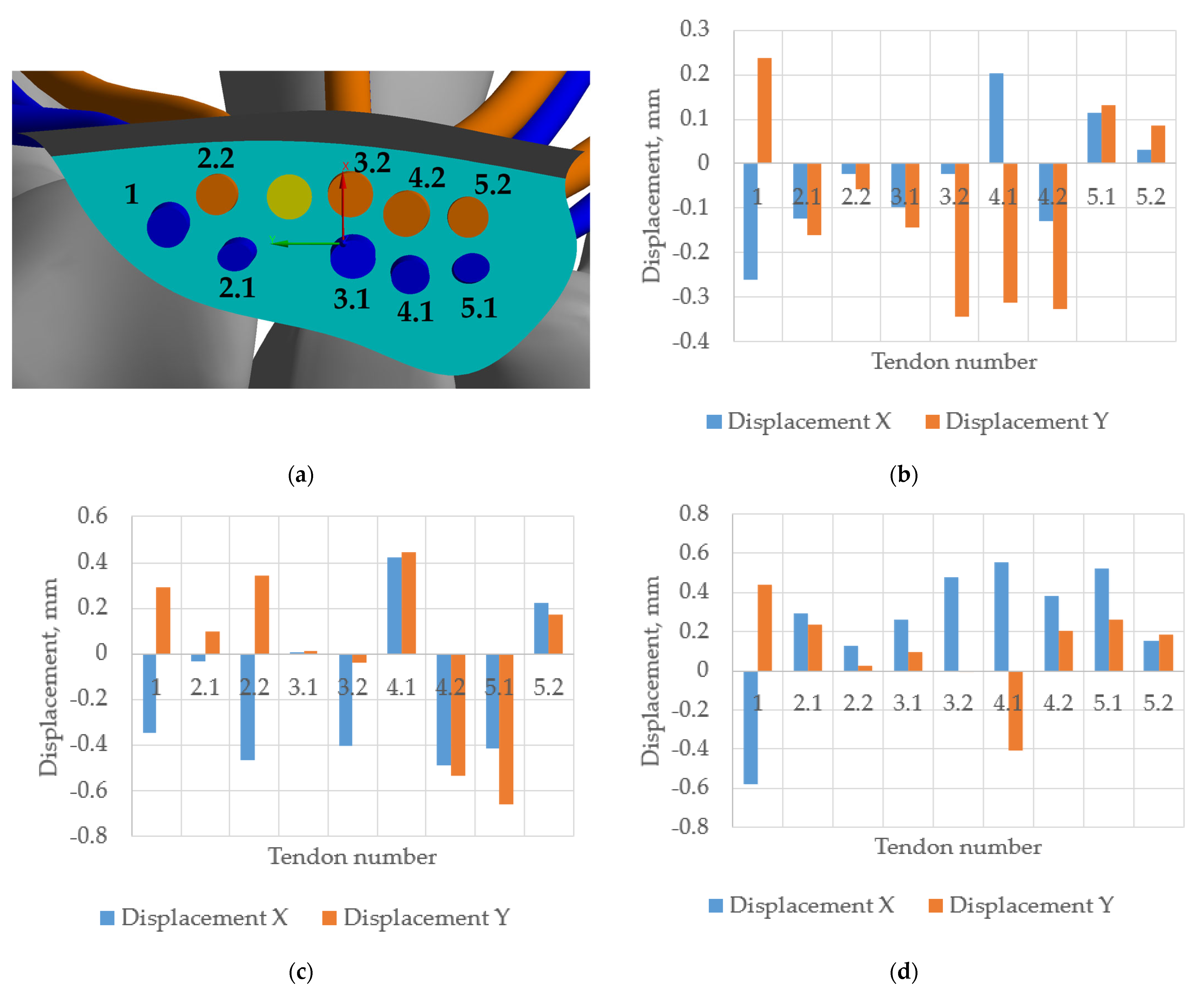
3.8. Tendons Displacement in Carpal Tunnel Area
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Laymon, M.; Petrofsky, J.; Mc Kivigan, J.; Lee, H.; Yim, J. Effect of Heat, Cold, and Pressure on the Transverse Carpal Ligament and Median Nerve: A Pilot Study. Med. Sci. Monit. 2015, 21, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Lundborg, G.; Gelberman, R.H.; Minteer-Convery, M.; Lee, Y.F.; Hargens, A.R. Median Nerve Compression in the Carpal Tunnel—Functional Response to Experimentally Induced Controlled Pressure. J. Hand Surg. Am. 1982, 7, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Werner, R.A.; Andary, M. Electrodiagnostic Evaluation of Carpal Tunnel Syndrome. Muscle Nerve 2011, 44, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Sonoo, M.; Menkes, D.L.; Bland, J.D.P.; Burke, D. Nerve Conduction Studies and EMG in Carpal Tunnel Syndrome: Do They Add Value? Clin. Neurophysiol. Pract. 2018, 3, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Peshin, S.E.; Karakulova, Y.V.; Nyashin, Y.I.; Nyashin, M.M. Carpal Tunnel Syndrome in Terms of Biomechanics. Literature Review. Russ. J. Biomech. 2022, 26, 9–13. [Google Scholar]
- Guo, X.; Fan, Y.; Li, Z.M. Three Dimensional Finite Element Analysis on the Morphological Change of the Transverse Carpal Ligament. In Proceedings of the 2007 IEEE/ICME International Conference on Complex Medical Engineering, CME, Beijing, China, 23–27 May 2007. [Google Scholar]
- Ko, C.; Brown, T.D. A Fluid-Immersed Multi-Body Contact Finite Element Formulation for Median Nerve Stress in the Carpal Tunnel. Comput. Methods Biomech. Biomed. Eng. 2007, 10, 343–349. [Google Scholar] [CrossRef]
- Javanmardian, A.; HaghPanahi, M. 3 Dimensional Finite Element Analysis of the Human Wrist Joint without Ligaments under Compressive Loads. In Proceedings of the 2010 17th Iranian Conference of Biomedical Engineering, ICBME, Isfahan, Iran, 3–4 November 2010. [Google Scholar]
- Mouzakis, D.E.; Rachiotis, G.; Zaoutsos, S.; Eleftheriou, A.; Malizos, K.N. Finite Element Simulation of the Mechanical Impact of Computer Work on the Carpal Tunnel Syndrome. J. Biomech. 2014, 47, 2989–2994. [Google Scholar] [CrossRef]
- Yao, Y.; Erdemir, A.; Li, Z.M. Finite Element Analysis for Transverse Carpal Ligament Tensile Strain and Carpal Arch Area. J. Biomech. 2018, 73, 210–216. [Google Scholar] [CrossRef]
- Oflaz, H.; Gunal, I. Maximum Loading of Carpal Bones during Movements: A Finite Element Study. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 47–50. [Google Scholar] [CrossRef]
- Perevoshchikova, N.; Moerman, K.M.; Akhbari, B.; Bindra, R.; Maharaj, J.N.; Lloyd, D.G.; Cerezo, M.G.; Carr, A.; Vaquette, C.; Saxby, D.J. Finite Element Analysis of the Performance of Additively Manufactured Scaffolds for Scapholunate Ligament Reconstruction. PLoS ONE 2021, 16, e0256528. [Google Scholar] [CrossRef]
- Marqués, R.; Melchor, J.; Sánchez-Montesinos, I.; Roda, O.; Rus, G.; Hernández-Cortés, P. Biomechanical Finite Element Method Model of the Proximal Carpal Row and Experimental Validation. Front. Physiol. 2022, 12, 2429. [Google Scholar] [CrossRef]
- Yokota, H.; Yasui, M.; Hirai, S.; Hatayama, N.; Ohshima, S.; Nakano, T.; Naito, M. Evaluation of the Pressure on the Dorsal Surface of the Distal Radius Using a Cadaveric and Computational Model: Clinical Considerations in Intersection Syndrome and Colles’ Fracture. Anat. Sci. Int. 2020, 95, 38–46. [Google Scholar] [CrossRef]
- Wei, Y.; Zou, Z.; Wei, G.; Ren, L.; Qian, Z. Subject-Specific Finite Element Modelling of the Human Hand Complex: Muscle-Driven Simulations and Experimental Validation. Ann. Biomed. Eng. 2020, 48, 1181–1195. [Google Scholar] [CrossRef]
- Natali, A.N.; Carniel, E.L.; Pavan, P.G.; Dario, P.; Izzo, I. Hyperelastic Models for the Analysis of Soft Tissue Mechanics: Definition of Constitutive Parameters. In Proceedings of the First IEEE/RAS-EMBS International Conference on Biomedical Robotics and BiomechatronicsBioRob, Pisa, Italy, 20–22 February 2006. [Google Scholar]
- Ogden, R. Non-Linear Elastic Deformations. Eng. Anal. Bound. Elem. 1984, 1, 119. [Google Scholar] [CrossRef]
- Main, E.K.; Goetz, J.E.; Baer, T.E.; Klocke, N.F.; Brown, T.D. Volar/Dorsal Compressive Mechanical Behavior of the Transverse Carpal Ligament. J. Biomech. 2012, 45, 1180–1185. [Google Scholar] [CrossRef]
- Main, E.K.; Goetz, J.E.; James Rudert, M.; Goreham-Voss, C.M.; Brown, T.D. Apparent Transverse Compressive Material Properties of the Digital Flexor Tendons and the Median Nerve in the Carpal Tunnel. J. Biomech. 2011, 44, 863–868. [Google Scholar] [CrossRef]
- Ma, Z.; Hu, S.; Tan, J.S.; Myer, C.; Njus, N.M.; Xia, Z. In Vitro and in Vivo Mechanical Properties of Human Ulnar and Median Nerves. J. Biomed. Mater. Res. Part A 2013, 101A, 2718–2725. [Google Scholar] [CrossRef]
- Chang, C.T.; Chen, Y.H.; Lin, C.C.K.; Ju, M.S. Finite Element Modeling of Hyper-Viscoelasticity of Peripheral Nerve Ultrastructures. J. Biomech. 2015, 48, 1982–1987. [Google Scholar] [CrossRef]
- Matsuura, Y.; Thoreson, A.R.; Zhao, C.; Amadio, P.C.; An, K.N. Development of a Hyperelastic Material Model of Subsynovial Connective Tissue Using Finite Element Modeling. J. Biomech. 2016, 49, 119–122. [Google Scholar] [CrossRef]
- Festen-Schrier, V.J.M.M.; Amadio, P.C. The Biomechanics of Subsynovial Connective Tissue in Health and Its Role in Carpal Tunnel Syndrome. J. Electromyogr. Kinesiol. 2018, 38, 232–239. [Google Scholar] [CrossRef]
- Kuchumov, A.G.; Vedeneev, V.; Samartsev, V.; Khairulin, A.; Ivanov, O. Patient-Specific Fluid–Structure Interaction Model of Bile Flow: Comparison between 1-Way and 2-Way Algorithms. Comput. Methods Biomech. Biomed. Engin. 2021, 24, 1693–1717. [Google Scholar] [CrossRef] [PubMed]
- Pistoia, W.; Van Rietbergen, B.; Lochmüller, E.M.; Lill, C.A.; Eckstein, F.; Rüegsegger, P. Estimation of Distal Radius Failure Load with Micro-Finite Element Analysis Models Based on Three-Dimensional Peripheral Quantitative Computed Tomography Images. Bone 2002, 30, 842–848. [Google Scholar] [CrossRef] [PubMed]
- Bauman, T.D.; Gelberman, R.H.; Mubarak, S.J.; Garfin, S.R. The Acute Carpal Tunnel Syndrome. Clin. Orthop. Relat. Res. 1981, 156, 151–156. [Google Scholar] [CrossRef]
- Kuschner, S.H.; Ebramzadeh, E.; Johnson, D.; Brien, W.W.; Sherman, R. Tinel’s Sign and Phalen’s Test in Carpal Tunnel Syndrome. Orthopedics 1992, 15, 1297–1302. [Google Scholar] [CrossRef] [PubMed]
- Lundborg, G.; Myers, R.; Powell, H. Nerve Compression Injury and Increased Endoneurial Fluid Pressure: A “Miniature Compartment Syndrome”. J. Neurol. Neurosurg. Psychiatry 1983, 46, 1119–1124. [Google Scholar] [CrossRef]
- Rojviroj, S.; Sirichativapee, W.; Kowsuwon, W.; Wongwiwattananon, J.; Tamnanthong, N.; Jeeravipoolvarn, P. Pressures in the Carpal Tunnel. A Comparison between Patients with Carpal Tunnel Syndrome and Normal Subjects. J. Bone Jt. Surg. Ser. B 1990, 72, 516–518. [Google Scholar] [CrossRef]
- Luchetti, R.; Schoenhuber, R.; Alfarano, M.; Deluca, S.; De Cicco, G.; Landi, A. Carpal Tunnel Syndrome: Correlations between Pressure Measurement and Intraoperative Electrophysiological Nerve Study. Muscle Nerve 1990, 13, 1164–1168. [Google Scholar] [CrossRef]
- Hamanaka, I.; Okutsu, I.; Shimizu, K.; Takatori, Y.; Ninomiya, S. Evaluation of Carpal Canal Pressure in Carpal Tunnel Syndrome. J. Hand Surg. Am. 1995, 20, 848–854. [Google Scholar] [CrossRef]
- Dilley, A.; Greening, J.; Lynn, B.; Leary, R.; Morris, V. The Use of Cross-Correlation Analysis between High-Frequency Ultrasound Images to Measure Longitudinal Median Nerve Movement. Ultrasound Med. Biol. 2001, 27, 1211–1218. [Google Scholar] [CrossRef]
- Guo, X.; Fan, Y.; Li, Z.M. Effects of Dividing the Transverse Carpal Ligament on the Mechanical Behavior of the Carpal Bones under Axial Compressive Load: A Finite Element Study. Med. Eng. Phys. 2009, 31, 188–194. [Google Scholar] [CrossRef]
- Schweizer, A.; Frank, O.; Ochsner, P.E.; Jacob, H.A.C. Friction between Human Finger Flexor Tendons and Pulleys at High Loads. J. Biomech. 2003, 36, 63–71. [Google Scholar] [CrossRef]
- Moor, B.K.; Nagy, L.; Snedeker, J.G.; Schweizer, A. Friction between Finger Flexor Tendons and the Pulley System in the Crimp Grip Position. Clin. Biomech. 2009, 24, 20–25. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hyperelastic Parameter | Reference | ||
|---|---|---|---|
| Tissues | α | µ [Pa] | |
| Annular ligaments | 10.9 | 24.900 | Main E.K. et al. [18] |
| Transverse ligament | 10.9 | 24.900 | Main E.K. et al. [18] |
| Flexor digitorum deep tendon | 8.89 | 37.600 | Main E.K. et al. [19] |
| Flexor digit superficial tendon | 8.89 | 37.600 | Main E.K. et al. [19] |
| Subsynovial connective tissue | 4.51 | 12.500 | Matsuura Y. et al. [22] |
| Median nerve | 6.5 | 12.900 | Main E.K. et al., Ma Z. et al. [19,20] |
| Elastic | |||
| ν | E [MPa] | ||
| Phalanges and carpal bones | 0.3 | 10,000 | Pistoia W. et al. [25] |
| Solid Body Pair | Interaction/Contact Type |
|---|---|
| Distal phalange to Middle phalange | Revolute |
| Middle phalange to Proximal phalange | Revolute |
| Proximal phalange to Metacarpal | Revolute |
| Deep flexor tendon to Distal phalange | Bonded |
| Superficial flexor tendon to Middle phalange | Bonded |
| Superficial and Deep flexor tendon to Annular ligament | No separation |
| Superficial and Deep flexor tendon to SSCT | No separation |
| Median nerve to SSCT | No separation |
| Annular ligament to phalanges | Bonded |
| Transverse carpal ligament to SSCT | Bonded |
| Stress, Pa | |||
|---|---|---|---|
| Movement | SSCT | Median Nerve | Transverse Ligament |
| fingers flexion | 67.6 | 227.5 | 502.2 |
| wrist extension | 189.3 | 218.1 | 1785.9 |
| wrist flexion | 66.3 | 197.6 | 1905.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peshin, S.; Karakulova, Y.; Kuchumov, A.G. Finite Element Modeling of the Fingers and Wrist Flexion/Extension Effect on Median Nerve Compression. Appl. Sci. 2023, 13, 1219. https://doi.org/10.3390/app13021219
Peshin S, Karakulova Y, Kuchumov AG. Finite Element Modeling of the Fingers and Wrist Flexion/Extension Effect on Median Nerve Compression. Applied Sciences. 2023; 13(2):1219. https://doi.org/10.3390/app13021219
Chicago/Turabian StylePeshin, Saveliy, Yulia Karakulova, and Alex G. Kuchumov. 2023. "Finite Element Modeling of the Fingers and Wrist Flexion/Extension Effect on Median Nerve Compression" Applied Sciences 13, no. 2: 1219. https://doi.org/10.3390/app13021219
APA StylePeshin, S., Karakulova, Y., & Kuchumov, A. G. (2023). Finite Element Modeling of the Fingers and Wrist Flexion/Extension Effect on Median Nerve Compression. Applied Sciences, 13(2), 1219. https://doi.org/10.3390/app13021219