
Skeletal and Dentoalveolar Effects of Maxillary Protraction Using Tooth- and Miniscrew-Anchored Devices in Patients with Class III Malocclusion with Maxillary Deficiency: A Retrospective Follow-Up Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
- Skeletal Class III malocclusion (relative anteroposterior position between the maxilla and mandible (ANB) <2°) measured on initial lateral cephalograms and evaluator.
- Anterior cross (including edge-to-edge) bite.
- Cervical vertebral maturation stages (CVMS) I–III.
- No craniofacial malformations or systemic disease.
- No temporomandibular joint disorder (TMD).
- No history of orthodontic treatment.
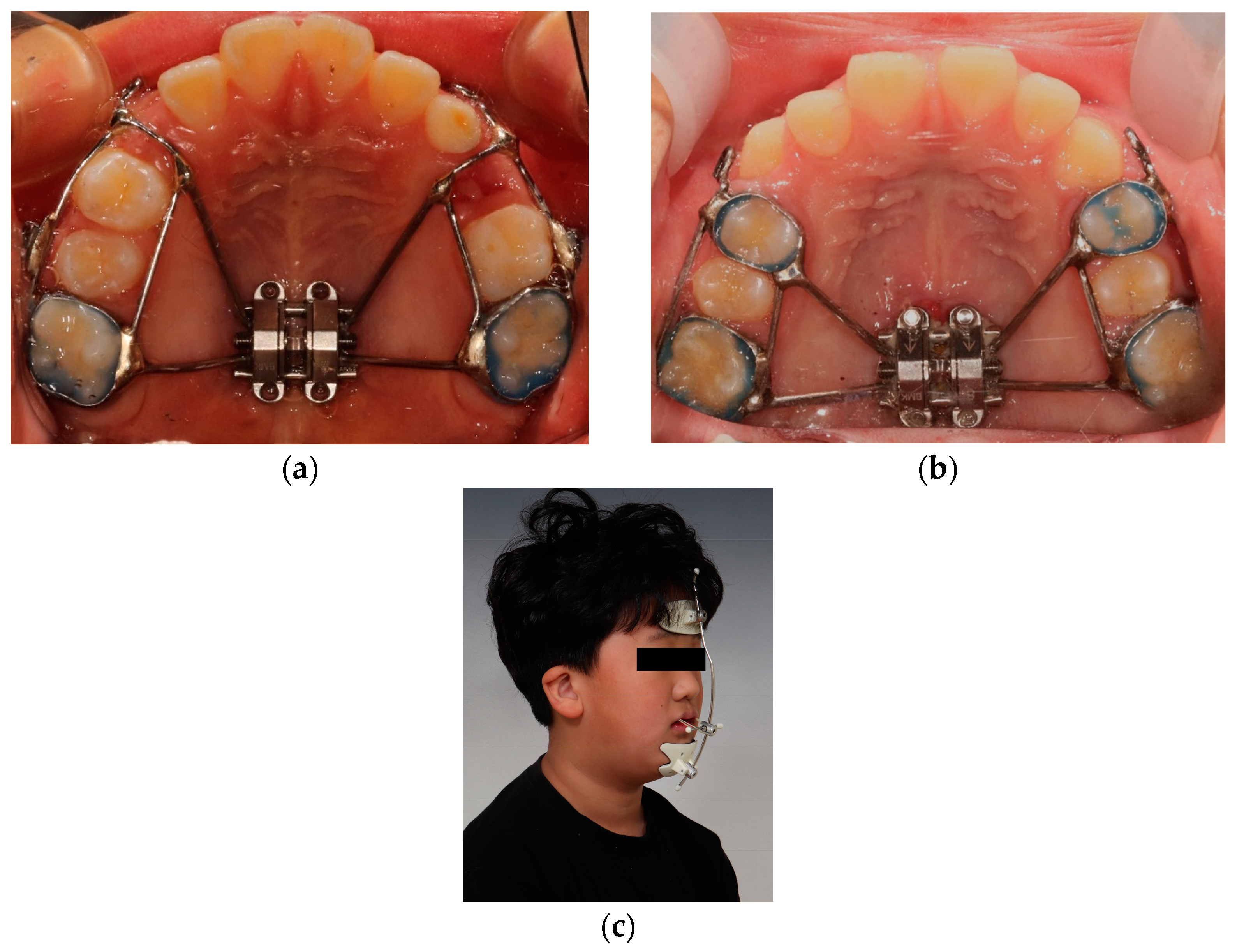
2.1. Treatment
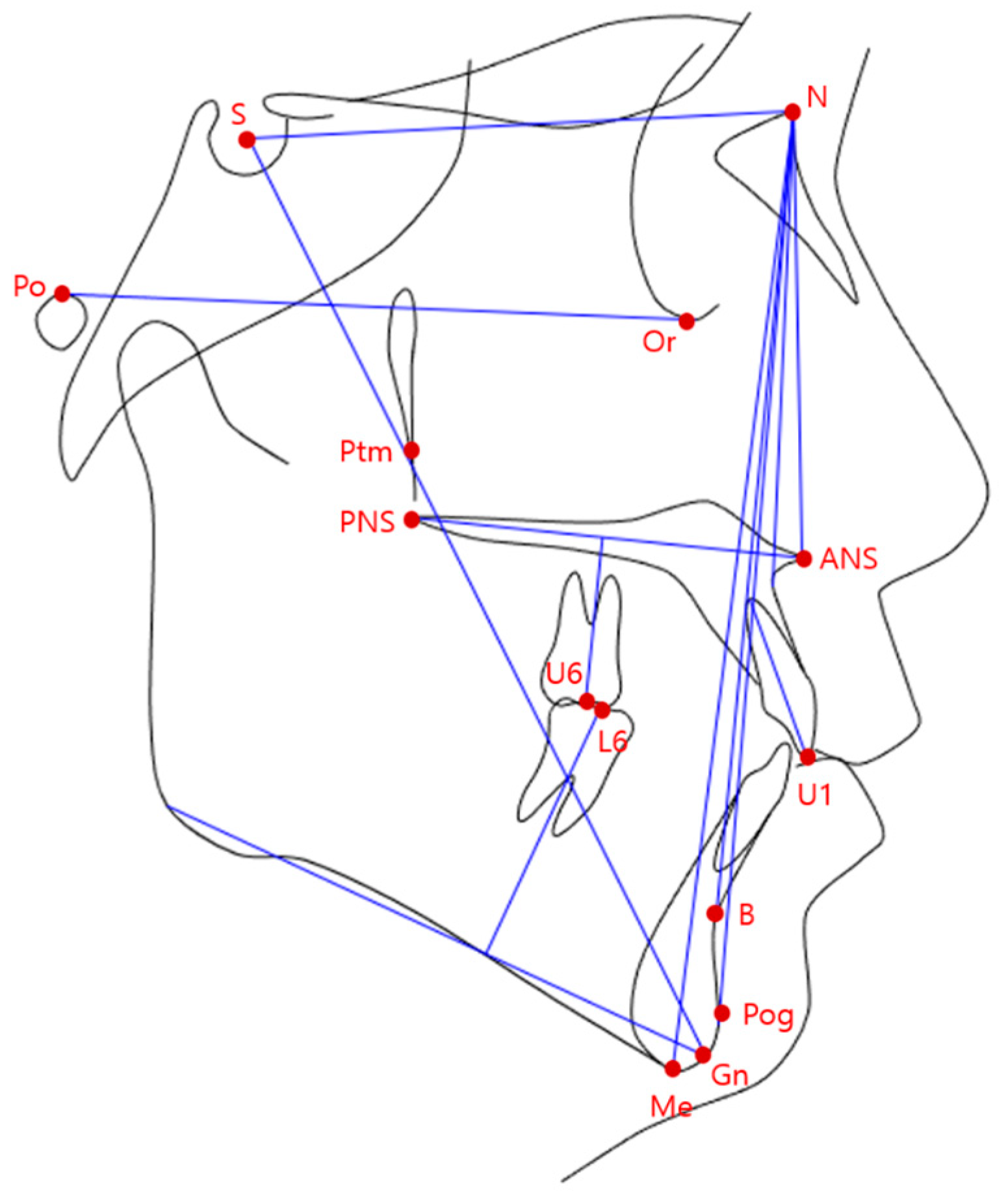
2.2. Lateral Cephalometric Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Skeletal and Dental Changes during Maxillary Protraction (between T1 and T2)
4.2. Skeletal and Dental Changes between T2 and T3
4.3. Overall Skeletal and Dental Changes (T1–T3)
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baik, H.-S.; Kim, K.-H.; Park, Y. The distributions and trends in maloclusion patients-A 10 year study of 2155 patients from YDSH. Korean J. Orthod. 1995, 25, 87–100. [Google Scholar]
- Ishii, H.; Morita, S.; Takeuchi, Y.; Nakamura, S. Treatment effect of combined maxillary protraction and chincap appliance in severe skeletal Class III cases. Am. J. Orthod. Dentofac. Orthop. 1987, 92, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Allwright, W.C. A survey of handicapping dentofacial anomalies among Chinese in Hong Kong. Int. Dent. J. 1964, 14, 505–519. [Google Scholar]
- Nanda, R. Biomechanical and clinical considerations of a modified protraction headgear. Am. J. Orthod. 1980, 78, 125–139. [Google Scholar] [CrossRef]
- Roberts, C.A.; Subteiny, J.D. An american board of orthodontics ease report, use of the face mask in the treatment of maxillary skeletal, retrusion. Am. J. Orthod. Dentofac. Orthop. 1988, 93, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Delaire, J. Manufacture of the “orthopedic mask”. Revue Stomatol. Chir. Maxillo-Fac. 1971, 72, 579–582. [Google Scholar]
- Nartallo-Turley, P.E.; Turley, P.K. Cephalometric effects of combined palatal expansion and facemask therapy on Class III malocclusion. Angle Orthod. 1998, 68, 217–224. [Google Scholar]
- Kama, J.D.; Baran, S. Orthodontic and orthopaedic changes associated with treatment in subjects with Class III malocclusions. Eur. J. Orthod. 2006, 28, 496–502. [Google Scholar] [CrossRef]
- De Clerck, H.J.; Cornelis, M.A.; Cevidanes, L.H.; Heymann, G.C.; Tulloch, C.J. Orthopedic traction of the maxilla with miniplates: A new perspective for treatment of midface deficiency. J. Oral Maxillofac. Surg. 2009, 67, 2123–2129. [Google Scholar] [CrossRef]
- Cha, B.-K.; Lee, N.-K.; Choi, D.-S. Maxillary protraction treatment of skeletal Class III children using miniplate anchorage. Korean J. Orthod. 2007, 37, 73–84. [Google Scholar]
- Cha, B.-K.; Choi, D.-S.; Ngan, P.; Jost-Brinkmann, P.-G.; Kim, S.-M. Maxillary protraction with miniplates providing skeletal anchorage in a growing Class III patient. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 99–112. [Google Scholar] [CrossRef]
- Nienkemper, M.; Wilmes, B.; Pauls, A.; Drescher, D. Maxillary protraction using a hybrid hyrax-facemask combination. Prog. Orthod. 2013, 14, 5. [Google Scholar] [CrossRef] [PubMed]
- Ngan, P.; Wilmes, B.; Drescher, D.; Martin, C.; Weaver, B.; Gunel, E. Comparison of two maxillary protraction protocols: Tooth-borne versus bone-anchored protraction facemask treatment. Prog. Orthod. 2015, 16, 26. [Google Scholar] [CrossRef] [PubMed]
- Cha, B.-K.; Ngan, P.W. Skeletal anchorage for orthopedic correction of growing class III patients. Semin. Orthod. 2011, 17, 124–137. [Google Scholar] [CrossRef]
- Seiryu, M.; Ida, H.; Mayama, A.; Sasaki, S.; Sasaki, S.; Deguchi, T.; Takano-Yamamoto, T. A comparative assessment of orthodontic treatment outcomes of mild skeletal Class III malocclusion between facemask and facemask in combination with a miniscrew for anchorage in growing patients: A single-center, prospective randomized controlled trial. Angle Orthod. 2020, 90, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-J.; Choi, D.-S.; Jang, I.; Cha, B.-K. Comparison of facemask therapy effects using skeletal and tooth-borne anchorage: A longitudinal retrospective study. Angle Orthod. 2022, 92, 307–314. [Google Scholar] [CrossRef]
- Choi, Y.-K.; Park, J.-J.; Jeon, H.-R.; Kim, Y.-I. Comparison of the skeletodental effects of miniscrew-anchored and tooth-anchored facemask treatment in growing patients with skeletal class III malocclusions. Orthod. Craniofac. Res. 2023; Online ahead of print. [Google Scholar] [CrossRef]
- Chieruzzi, M.; Pagano, S.; De Carolis, C.; Eramo, S.; Kenny, J.M. Scanning Electron Microscopy Evaluation of Dental Root Resorption Associated with Granuloma. Microsc. Microanal. 2015, 21, 1264–1270. [Google Scholar] [CrossRef]
- Kircelli, B.; Pektas, Z. Midfascial protraction with skeletally anchored facemask therapy: A novel approach and preliminary results. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 440–449. [Google Scholar] [CrossRef]
- Maino, G.B.; Cremonini, F.; Maino, G.; Paoletto, E.; De Maio, M.; Spedicato, G.A.; Palone, M.; Lombardo, L. Long-term skeletal and dentoalveolar effects of hybrid rapid maxillary expansion and facemask treatment in growing skeletal Class III patients: A retrospective follow-up study. Prog. Orthod. 2022, 23, 44. [Google Scholar] [CrossRef]
- Lee, W.-C.; Shieh, Y.S.; Liao, Y.F.; Lee, C.-H.; Huang, C.-S. Long-term maxillary anteroposterior changes following maxillary protraction with or without expansion: A meta-analysis and meta-regression. PLoS ONE 2021, 16, e0247027. [Google Scholar] [CrossRef]
- Mandall, N.; Cousley, R.; DiBiase, A.; Dyer, F.; Littlewood, S.; Mattick, R.; Nute, S.J.; Doherty, B.; Stivaros, N.; McDowall, R.; et al. Early class III protraction facemask treatment reduces the need for orthognathic surgery: A multi-centre, two-arm parallel randomized, controlled trial. J. Orthod. 2016, 43, 164–175. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Measured Item | Description |
|---|---|
| SNA (°) | Sella-Nasion to A Point Angle |
| SNB (°) | Sella-Nasion to B Point Angle |
| ANB (°) | A Point to B Point Angle |
| SN–ANS (°) | Sella-Nasion to ANS Angle |
| Mandibular plane angle (Go–Gn to SN) (°) | Sella-Nasion to Gonion–Gnathion Angle |
| U1–SN (°) | Sella-Nasion to U1 Angle |
| N–Me (mm) | Distance between Nasion and Menton |
| U6/NF (mm) | Distance between U6 and Nasal Floor (ANS–PNS) |
| L6/MP (mm) | Distance between L6 and Mandibular Plane (Gonion–Menton) |
| Facial angle (°) | Angle between Nasion–Pogonion and Frankfurt Horizontal Line |
| Y axis (°) | Sella Gnathion to Frankfurt Horizontal Plane |
| IMPA | Mandibular Incisor to Mandibular Plane Angle |
| Overjet | The Overlap of The Teeth in The Horizontal Dimension |
| T-A Group (n = 25) | M-A Group (n = 25) | Significance | ||
|---|---|---|---|---|
| Age (T1) a | Mean | 7.92 | 9.84 | <0.01 * |
| SD | 1.12 | 1.09 | ||
| Min | 6 | 7.8 | ||
| Max | 10.7 | 11.9 | ||
| Age (T3) a | Mean | 12.12 | 13.34 | 0.16 |
| SD | 2.12 | 1.15 | ||
| Min | 8.1 | 10.9 | ||
| Max | 16.1 | 16.5 | ||
| CVMS (T1) b | Median | I | II | 0.15 |
| SD | 0.76 | 0.80 | ||
| 25% | I | II | ||
| 75% | II | III | ||
| CVMS (T3) b | Median | IV | V | 0.2 |
| SD | 0.86 | 0.71 | ||
| 25% | III | IV | ||
| 75% | V | V | ||
| Treatment period (T1–T2) a | Mean | 9.43 | 10.59 | 0.61 |
| SD | 9.51 | 5.96 | ||
| Min | 2.93 | 4.40 | ||
| Max | 35.9 | 31.10 | ||
| Treatment period (T1–T3) a | Mean | 52.05 | 42.19 | 0.33 |
| SD | 20.19 | 9.09 | ||
| Min | 30.4 | 31.83 | ||
| Max | 96.1 | 74.77 |
| T-A Group (n = 25) | B-A Group (n = 25) | Difference | p | Significance | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | 95% CI | Mean | SD | 95% CI | ||||||
| T2–T1 | |||||||||||
| SNA (°) | 1.43 | 0.72 | 1.13 | 1.73 | 2.07 | 0.91 | 1.69 | 2.44 | 0.63 | 0.009 | * |
| SNB (°) | −0.79 | 0.83 | −1.13 | −0.44 | −0.89 | 1.50 | −1.50 | −0.27 | 0.98 | 0.77 | NS |
| ANB (°) | 2.22 | 0.93 | 1.83 | 2.61 | 2.88 | 1.22 | 2.38 | 3.39 | 0.66 | 0.03 | * |
| SN–ANS (°) | 1.18 | 1.56 | 0.53 | 1.83 | 1.98 | 1.59 | 1.32 | 2.64 | 0.79 | 0.82 | NS |
| MP–SN (°) | 1.74 | 1.92 | 0.94 | 2.53 | 0.53 | 0.77 | 0.21 | 0.84 | 1.21 | 0.005 | ** |
| U1–SN (°) | 0.77 | 4.36 | −1.02 | 2.57 | 1.44 | 5.44 | −0.80 | 3.69 | 0.66 | 0.63 | NS |
| N–Me, mm | 3.14 | 1.68 | 2.45 | 3.84 | 2.17 | 1.25 | 1.65 | 2.69 | 0.97 | 0.02 | * |
| U6/NF, mm | 1.88 | 1.23 | 1.37 | 2.39 | 0.71 | 0.49 | 0.51 | 0.91 | 1.17 | <0.001 | ** |
| L6/MP, mm | 1.06 | 1.10 | 0.60 | 1.51 | 1.68 | 1.00 | 1.27 | 2.09 | 0.62 | 0.41 | * |
| Facial A | −0.77 | 2.10 | −1.64 | 0.09 | −0.49 | 1.52 | −1.12 | 0.12 | 0.27 | 0.60 | NS |
| Y axis | 1.22 | 1.97 | 0.40 | 2.04 | 0.62 | 1.31 | 0.08 | 1.16 | 0.59 | 0.21 | NS |
| Overjet | 4.26 | 2.08 | 3.40 | 5.12 | 4.87 | 2.03 | 4.03 | 5.72 | 0.61 | 0.29 | NS |
| IMPA | −5.04 | 4.26 | −6.80 | −3.28 | −2.61 | 3.09 | −3.89 | −1.33 | 2.42 | 0.02 | * |
| T3–T2 | |||||||||||
| SNA (°) | 1.22 | 2.20 | 0.31 | 2.13 | 1.22 | 1.23 | 0.71 | 1.72 | 0.004 | 0.99 | NS |
| SNB (°) | 2.71 | 2.42 | 1.70 | 3.71 | 1.66 | 1.32 | 1.11 | 2.21 | 1.04 | 0.65 | NS |
| ANB (°) | −1.48 | 1.57 | −2.13 | −0.83 | −0.37 | 1.17 | −0.86 | 0.10 | −1.1 | 0.007 | * |
| SN–ANS (°) | 0.73 | 2.14 | −0.14 | 1.62 | 1.40 | 1.85 | 0.63 | 2.16 | −0.66 | 0.24 | NS |
| MP–SN (°) | −3.98 | 2.44 | −4.99 | −2.97 | −2.09 | 1.14 | −2.56 | −1.62 | −1.88 | 0.001 | * |
| U1–SN (°) | 6.13 | 4.63 | 4.21 | 8.04 | 2.35 | 4.71 | 0.40 | 4.29 | 3.78 | 0.006 | * |
| N–Me, mm | 7.09 | 4.12 | 5.38 | 8.79 | 5.60 | 3.17 | 4.29 | 6.91 | 1.48 | 0.16 | NS |
| U6/NF, mm | 2.67 | 1.79 | 1.93 | 3.41 | 1.89 | 1.45 | 1.29 | 2.49 | 0.78 | 0.09 | NS |
| L6/MP, mm | 1.54 | 1.00 | 1.13 | 1.96 | 1.18 | 0.91 | 0.80 | 1.56 | 0.36 | 0.19 | NS |
| Facial A | 2.88 | 2.28 | 1.93 | 3.82 | 1.83 | 1.74 | 1.10 | 2.55 | 1.05 | 0.07 | NS |
| Y axis | −1.38 | 2.28 | −2.32 | −0.43 | −0.36 | 1.40 | −0.94 | 0.21 | −1.01 | 0.06 | NS |
| Overjet | −1.37 | 1.41 | −1.96 | −0.79 | −1.29 | 2.06 | −2.15 | −0.44 | −0.08 | 0.87 | NS |
| IMPA | 4.72 | 4.56 | 2.83 | 6.60 | 3.14 | 3.80 | 1.57 | 4.71 | 1.57 | 0.19 | NS |
| T3–T1 | |||||||||||
| SNA (°) | 2.65 | 2.31 | 1.70 | 3.61 | 3.29 | 1.55 | 2.65 | 3.93 | 0.63 | 0.26 | NS |
| SNB (°) | 1.92 | 2.61 | 0.84 | 2.99 | 0.77 | 1.67 | 0.08 | 1.46 | 1.14 | 0.07 | NS |
| ANB (°) | 0.73 | 1.55 | 0.09 | 1.38 | 2.51 | 1.34 | 1.95 | 3.06 | 1.77 | <0.001 | ** |
| SN–ANS (°) | 1.92 | 2.90 | 0.72 | 3.12 | 3.38 | 2.18 | 2.48 | 4.28 | 1.45 | 0.05 | NS |
| MP–SN (°) | −0.24 | 3.06 | −3.50 | −0.97 | −1.56 | 1.17 | −2.04 | −1.08 | 0.67 | 0.311 | NS |
| U1–SN (°) | 6.91 | 4.29 | 5.14 | 8.68 | 3.79 | 5.87 | 1.37 | 6.22 | 3.11 | 0.03 | * |
| N–Me, mm | 10.24 | 4.36 | 8.43 | 12.04 | 7.90 | 3.52 | 6.44 | 9.35 | 2.33 | 0.04 | * |
| U6/NF, mm | 4.56 | 1.57 | 3.91 | 5.21 | 2.60 | 1.35 | 2.04 | 3.16 | 1.95 | <0.001 | ** |
| L6/MP, mm | 2.60 | 1.58 | 1.95 | 3.26 | 2.87 | 1.33 | 2.32 | 3.42 | 0.26 | 0.52 | NS |
| Facial A | 2.11 | 2.21 | 1.19 | 3.02 | 1.33 | 1.92 | 0.53 | 2.12 | 0.77 | 0.19 | NS |
| Y axis | −0.15 | 2.68 | −1.26 | 0.95 | 0.26 | 1.81 | −0.48 | 1.0 | 0.41 | 0.52 | NS |
| Overjet | 2.88 | 2.71 | 1.76 | 4.00 | 3.58 | 2.24 | 2.65 | 4.51 | 0.69 | 0.32 | NS |
| IMPA | −0.31 | 3.83 | −1.89 | 1.26 | 0.53 | 3.83 | −1.05 | 2.11 | 0.85 | 0.43 | NS |
| Measurement | T1 | T2 | T3 | Adjusted p Value | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| SNA | 79.76 a | 3.09 | 81.23 b | 3.14 | 82.25 c | 3.40 | <0.001 ** |
| SNB | 79.64 a | 3.17 | 78.93 b | 3.26 | 81.64 c | 3.95 | <0.001 ** |
| ANB | −0.13 a | 1.75 | 2.09 b | 2.01 | 0.60 a | 2.28 | 0.026 * |
| MP–SN | 28.29 a | 5.83 | 30.30 b | 5.38 | 26.05 c | 5.49 | 0.001 * |
| N–Me | 101.53 a | 4.45 | 104.68 b | 4.81 | 111.77 c | 6.04 | <0.001 ** |
| U6/NF | 14.27 a | 1.66 | 16.15 b | 1.56 | 18.83 c | 1.82 | <0.001 ** |
| Measurement | T1 | T2 | T3 | Adjusted p Value | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| SNA | 79.21 a | 2.80 | 81.28 b | 3.2 | 82.5 c | 3.04 | <0.001 ** |
| SNB | 80.51 a | 2.89 | 79.62 b | 3.08 | 81.29 a | 3.0 | 0.029 * |
| ANB | −1.30 a | 1.46 | 1.58 b | 1.65 | 1.20 c | 1.42 | <0.001 ** |
| MP–SN | 28.47 a | 4.64 | 29.00 b | 4.50 | 26.9 c | 4.46 | <0.001 ** |
| N–Me | 110.10 a | 5.35 | 112.28 b | 5.39 | 118.01 c | 6.37 | <0.001 ** |
| U6/NF | 18.06 a | 1.62 | 18.77 b | 1.74 | 20.67 c | 1.54 | <0.001 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baik, J.-C.; Choi, Y.-K.; Jeon, H.H.; Kim, S.-H.; Kim, S.-S.; Park, S.-B.; Kim, Y.-I. Skeletal and Dentoalveolar Effects of Maxillary Protraction Using Tooth- and Miniscrew-Anchored Devices in Patients with Class III Malocclusion with Maxillary Deficiency: A Retrospective Follow-Up Study. Appl. Sci. 2023, 13, 10530. https://doi.org/10.3390/app131810530
Baik J-C, Choi Y-K, Jeon HH, Kim S-H, Kim S-S, Park S-B, Kim Y-I. Skeletal and Dentoalveolar Effects of Maxillary Protraction Using Tooth- and Miniscrew-Anchored Devices in Patients with Class III Malocclusion with Maxillary Deficiency: A Retrospective Follow-Up Study. Applied Sciences. 2023; 13(18):10530. https://doi.org/10.3390/app131810530
Chicago/Turabian StyleBaik, Jong-Chan, Youn-Kyung Choi, Hyeran Helen Jeon, Sung-Hun Kim, Seong-Sik Kim, Soo-Byung Park, and Yong-Il Kim. 2023. "Skeletal and Dentoalveolar Effects of Maxillary Protraction Using Tooth- and Miniscrew-Anchored Devices in Patients with Class III Malocclusion with Maxillary Deficiency: A Retrospective Follow-Up Study" Applied Sciences 13, no. 18: 10530. https://doi.org/10.3390/app131810530
APA StyleBaik, J.-C., Choi, Y.-K., Jeon, H. H., Kim, S.-H., Kim, S.-S., Park, S.-B., & Kim, Y.-I. (2023). Skeletal and Dentoalveolar Effects of Maxillary Protraction Using Tooth- and Miniscrew-Anchored Devices in Patients with Class III Malocclusion with Maxillary Deficiency: A Retrospective Follow-Up Study. Applied Sciences, 13(18), 10530. https://doi.org/10.3390/app131810530