
Microfluidic Microcirculation Mimetic as a Tool for the Study of Rheological Characteristics of Red Blood Cells in Patients with Sickle Cell Anemia

 , ,
, , 
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Setting, Ethical Approval, Participants, Informed Consent and Sample Collection
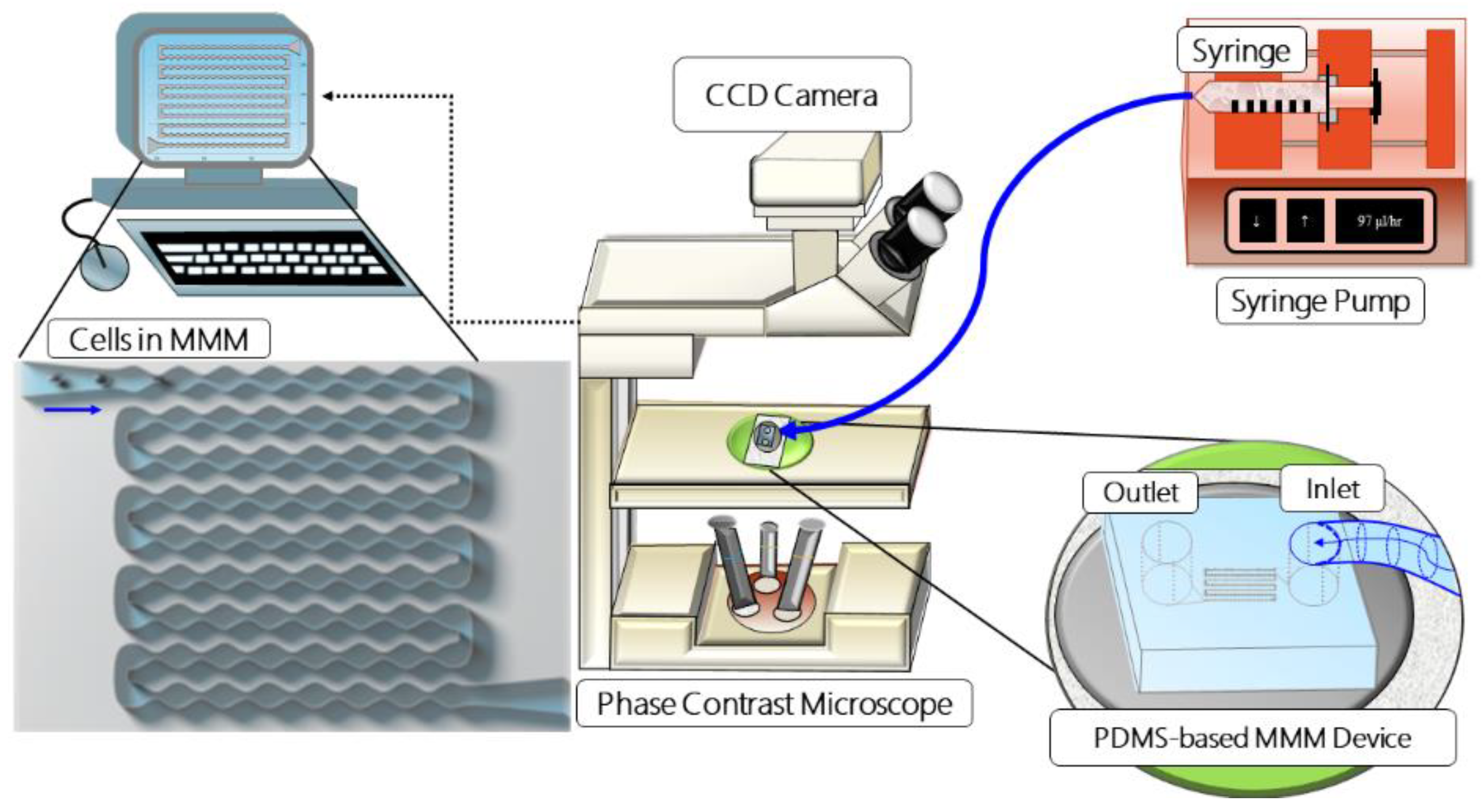
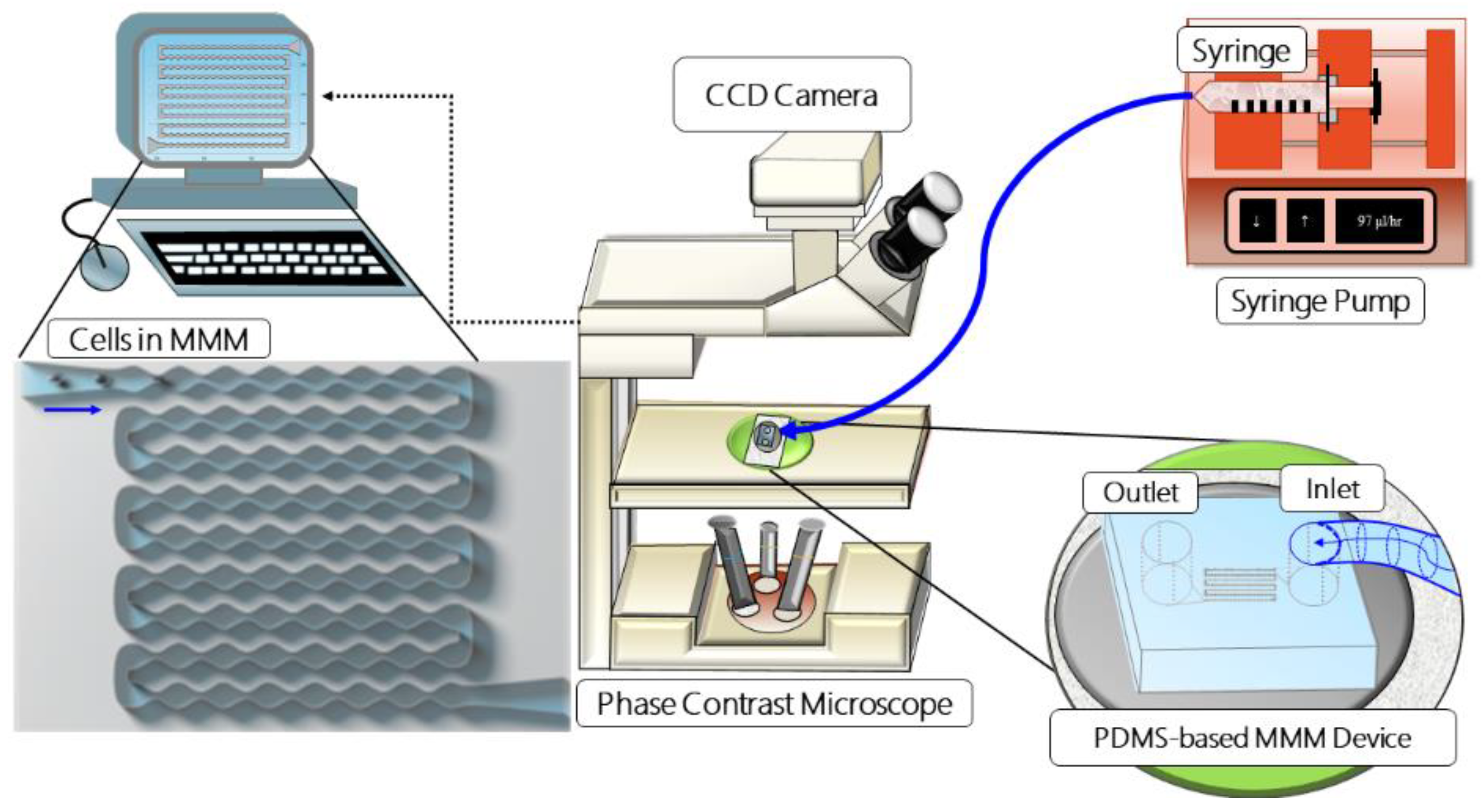
2.2. Microfluidic Microcirculation Mimetic
2.3. Morphometry during MMM Measurements
3. Results
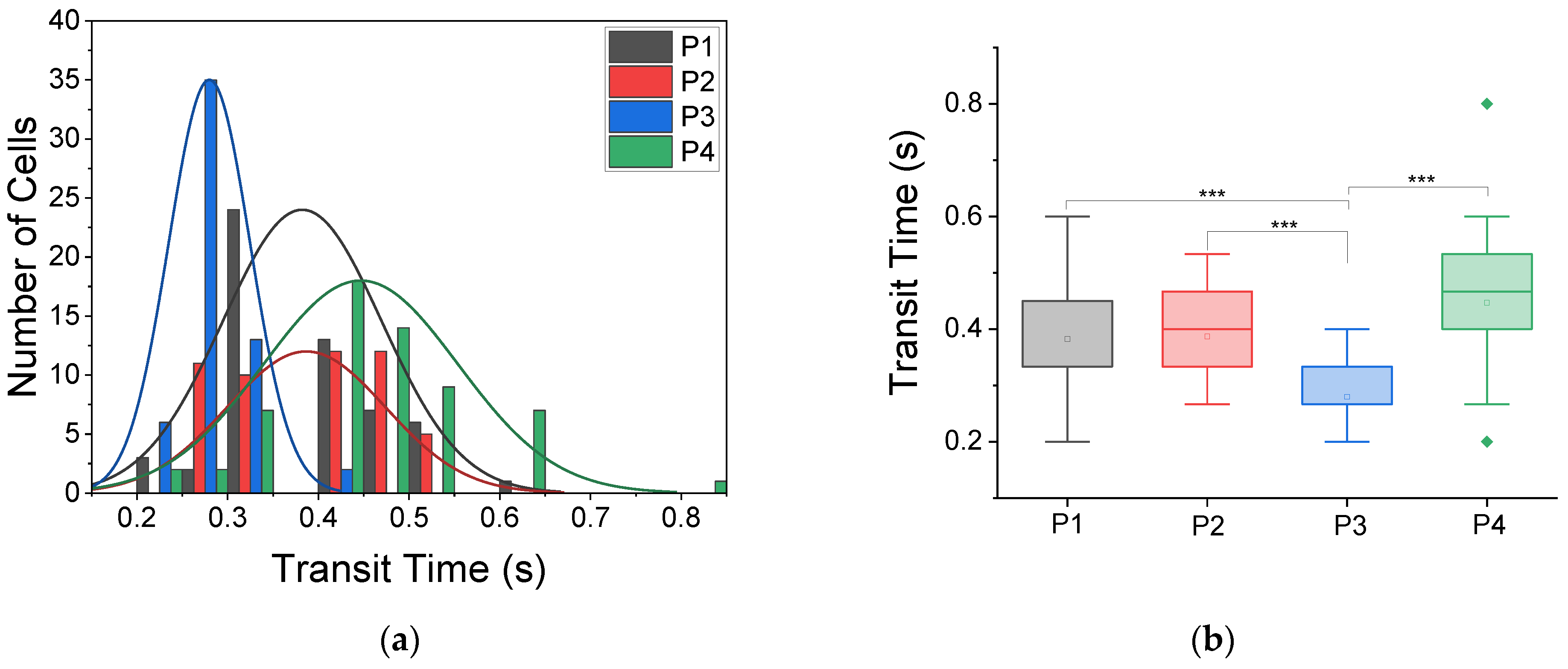
3.1. Morpho-Rheological Properties of Sickle RBCs Are Patient-Specific
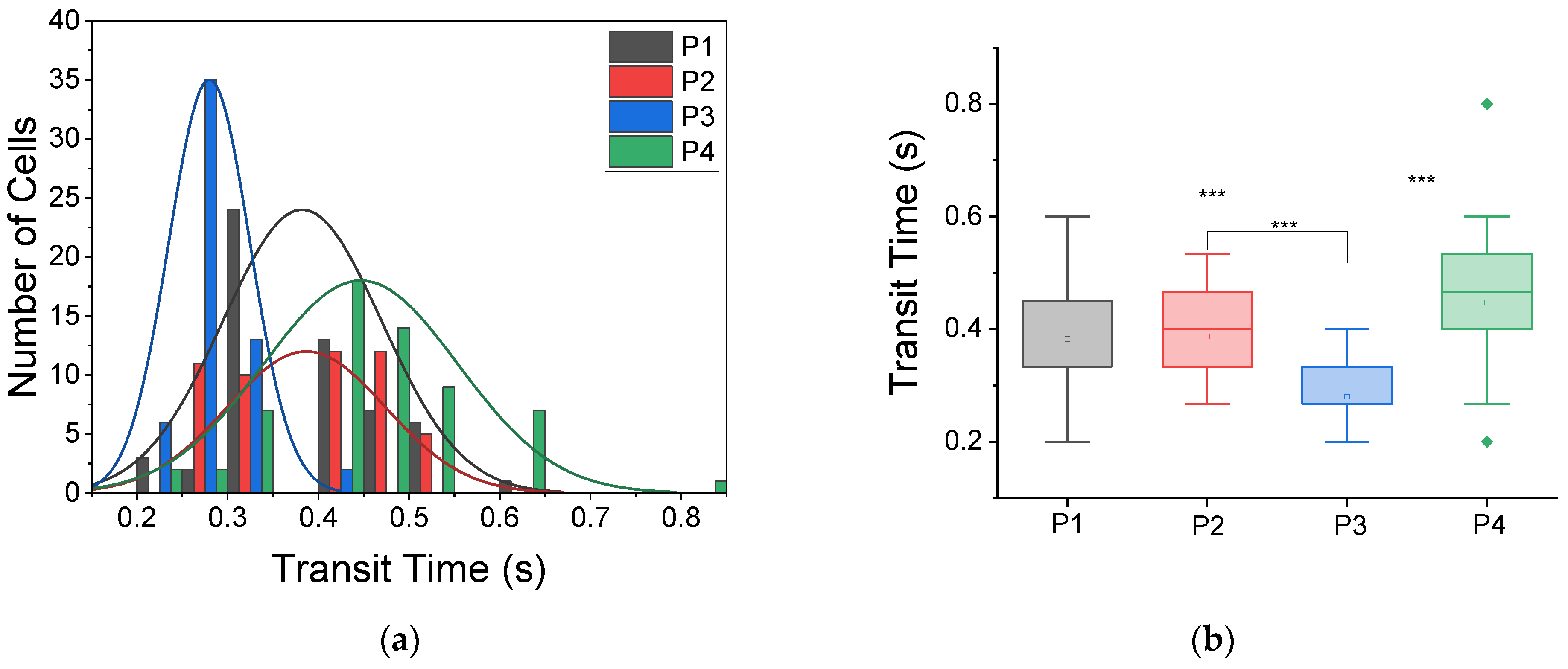
3.1.1. Transit Times through Microcapillary-like Constrictions
3.1.2. Morphometry Post-Microcapillary-like Constrictions
3.2. Ex Vivo Active Monitoring of Patients’ RBC
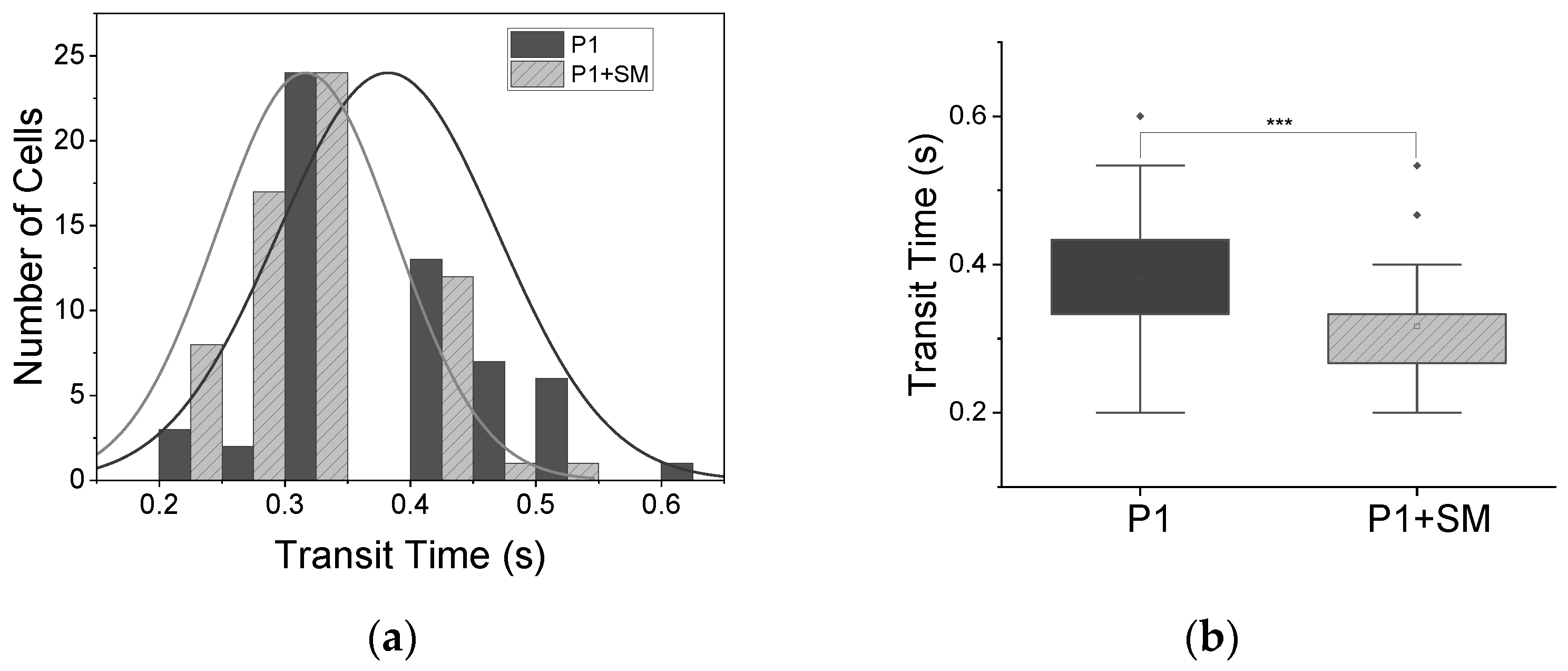
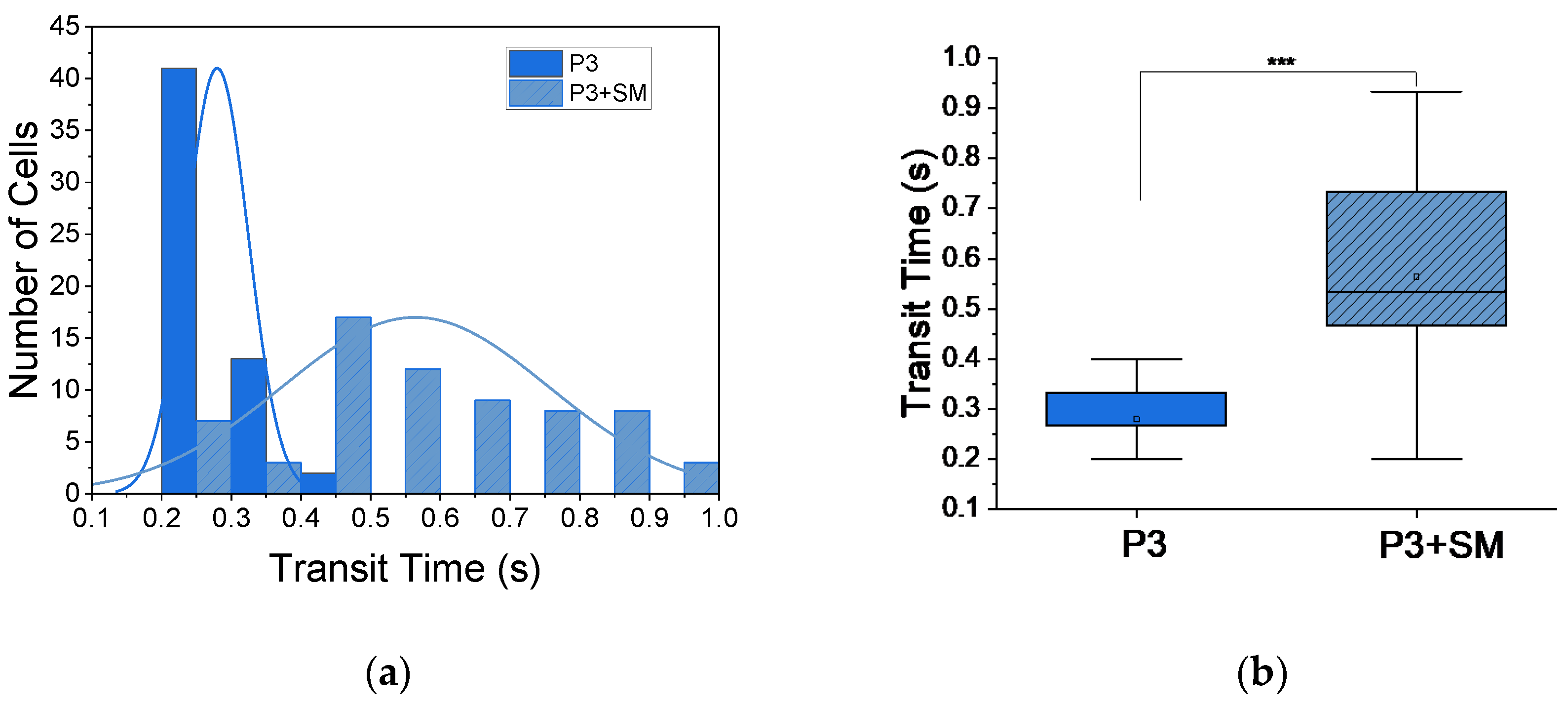
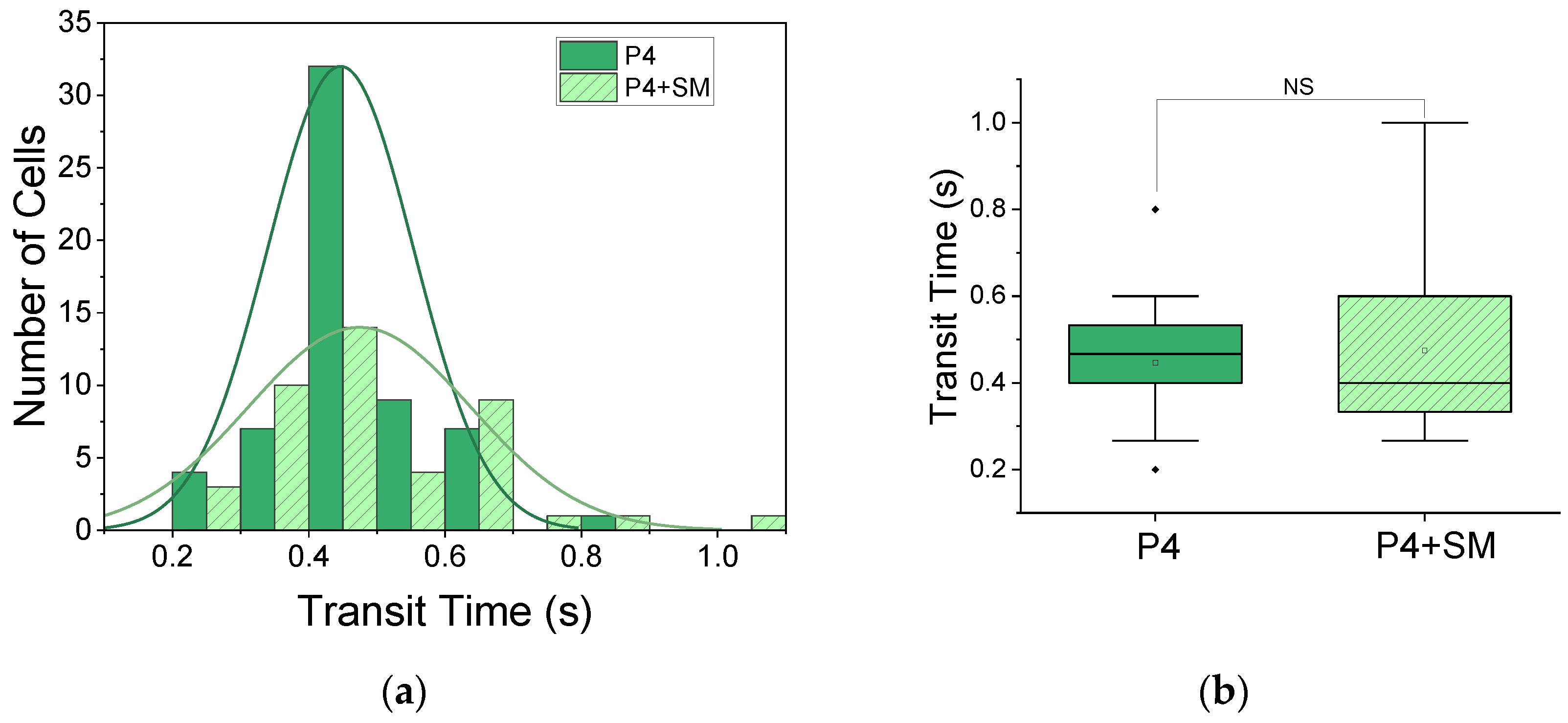
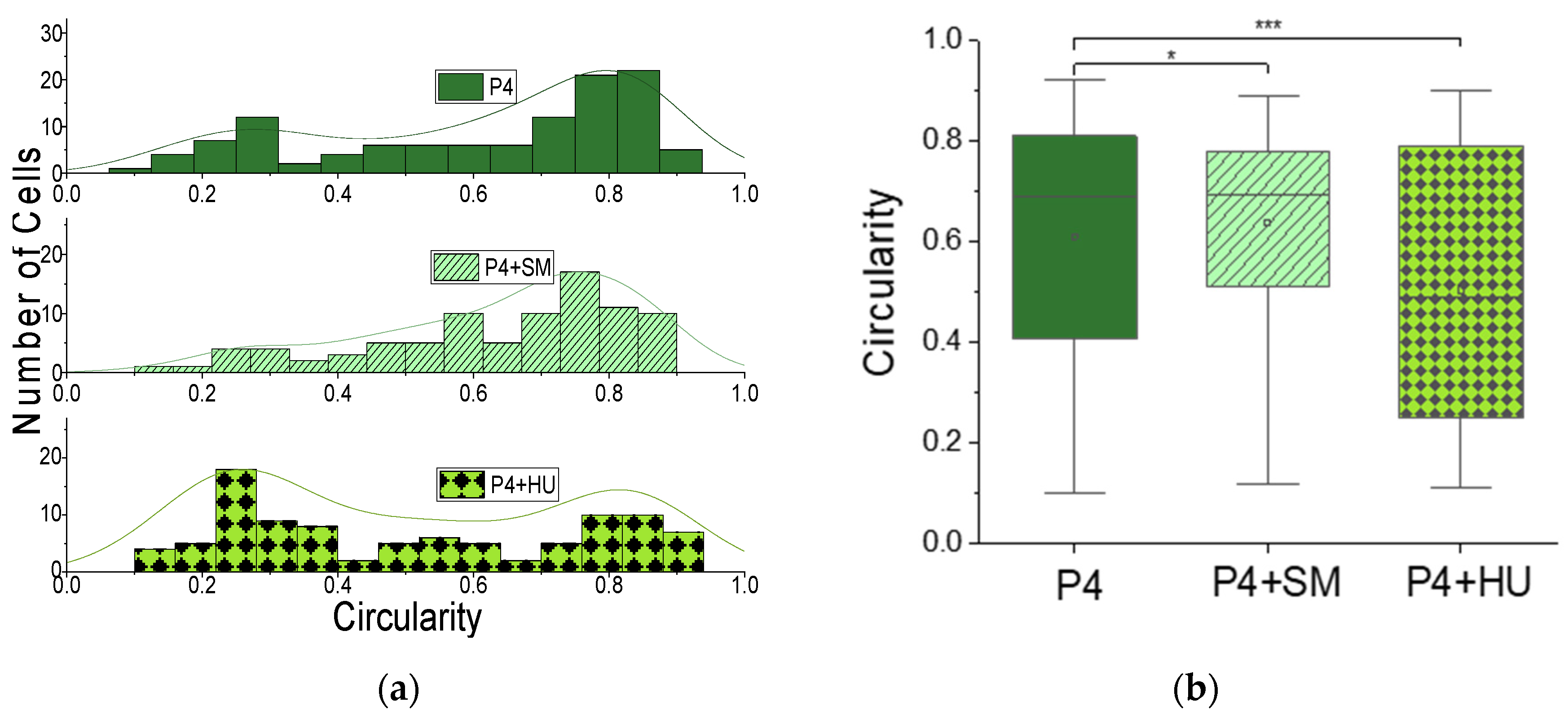
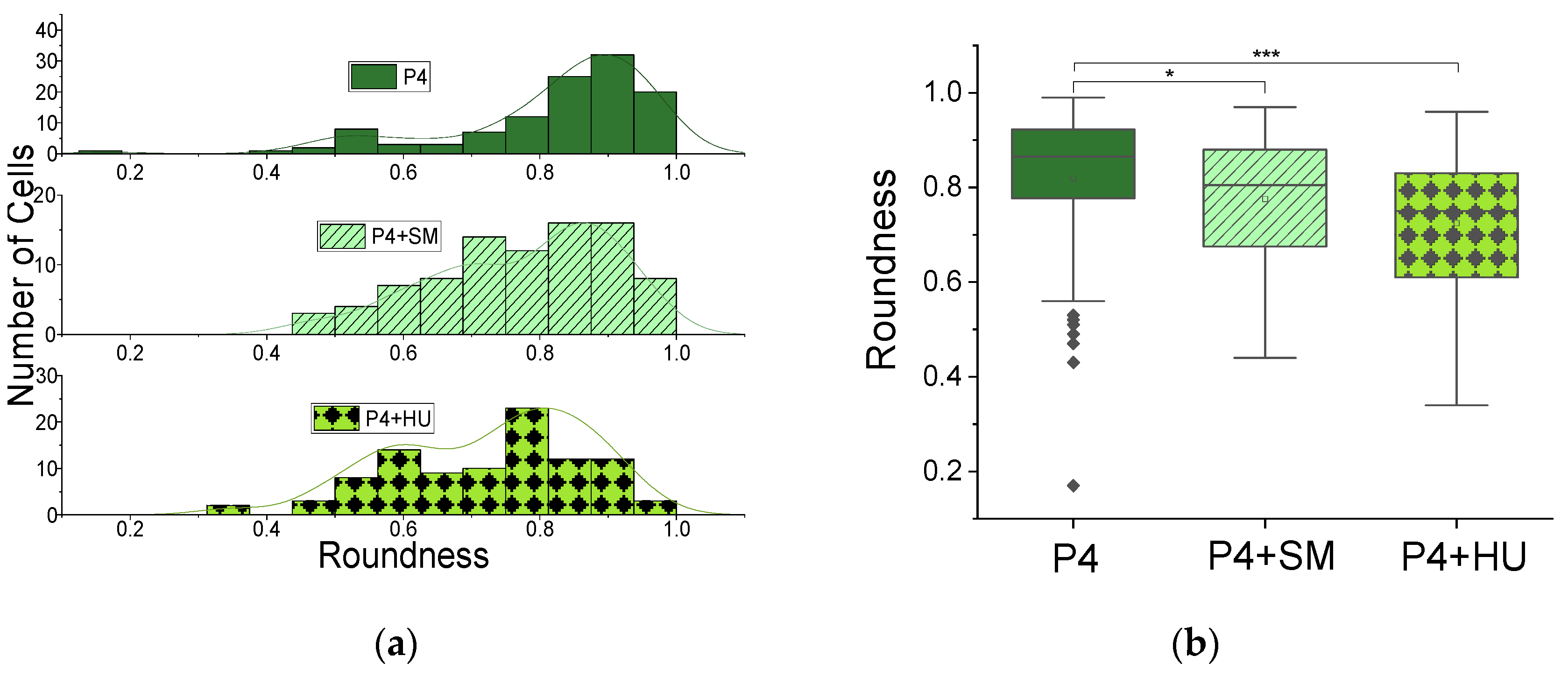
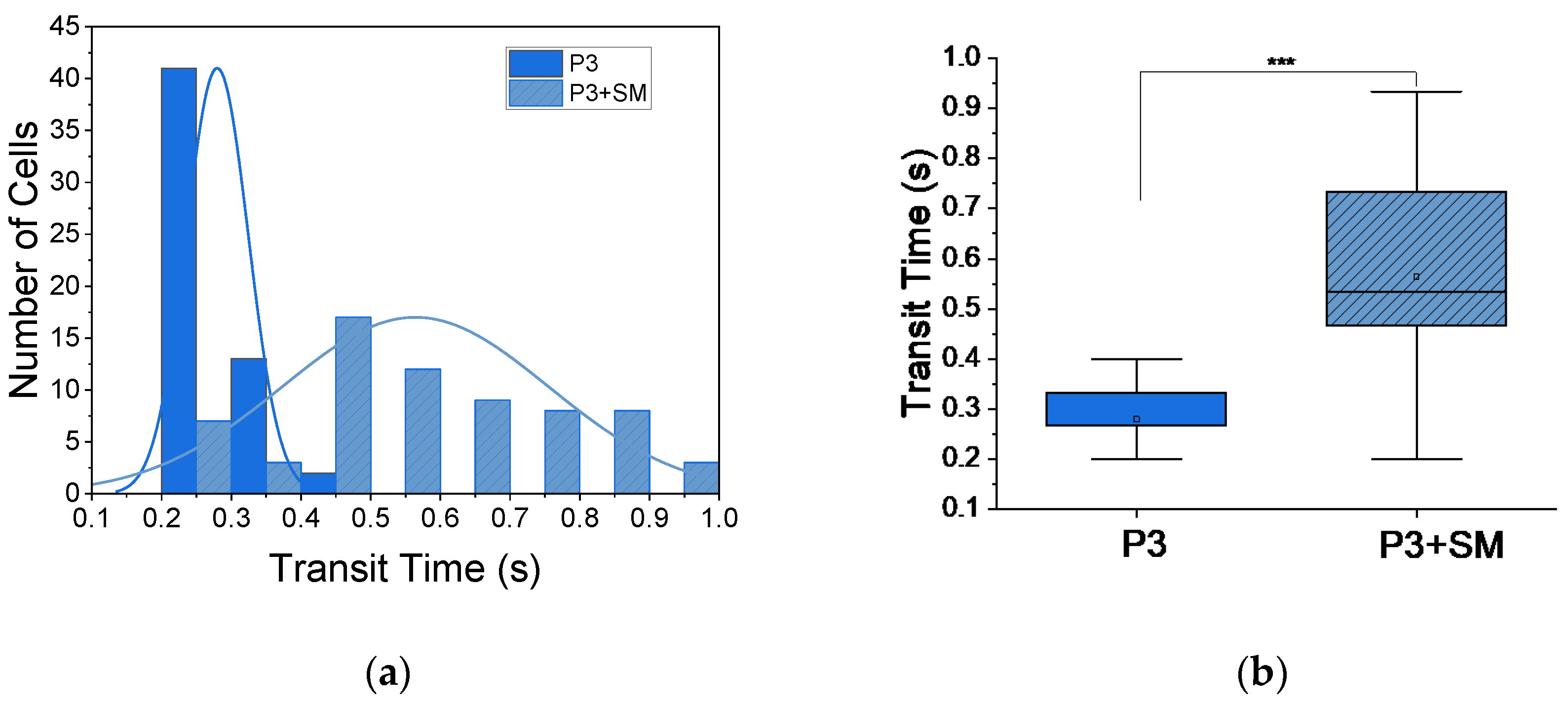
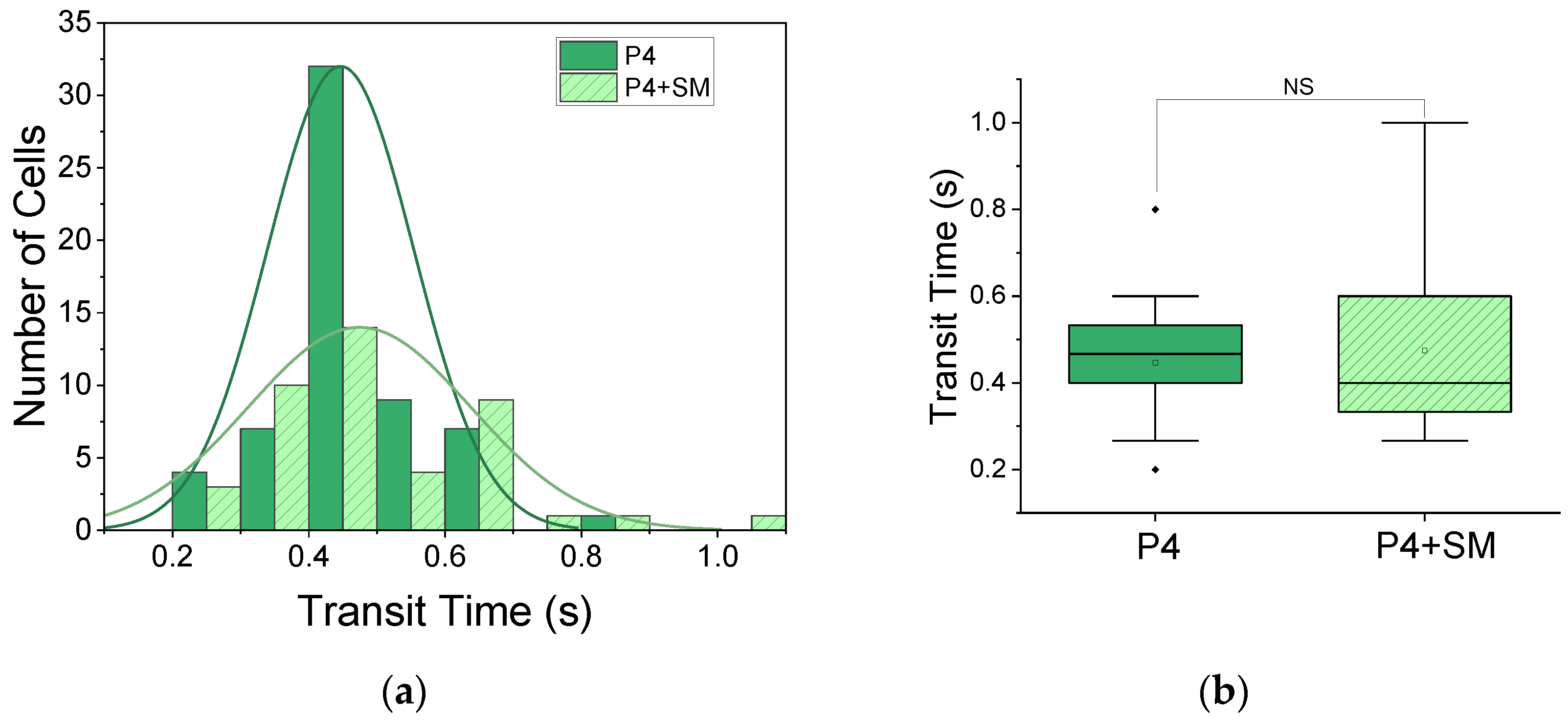
3.2.1. Monitoring of “VOC” via Induced Hypoxia
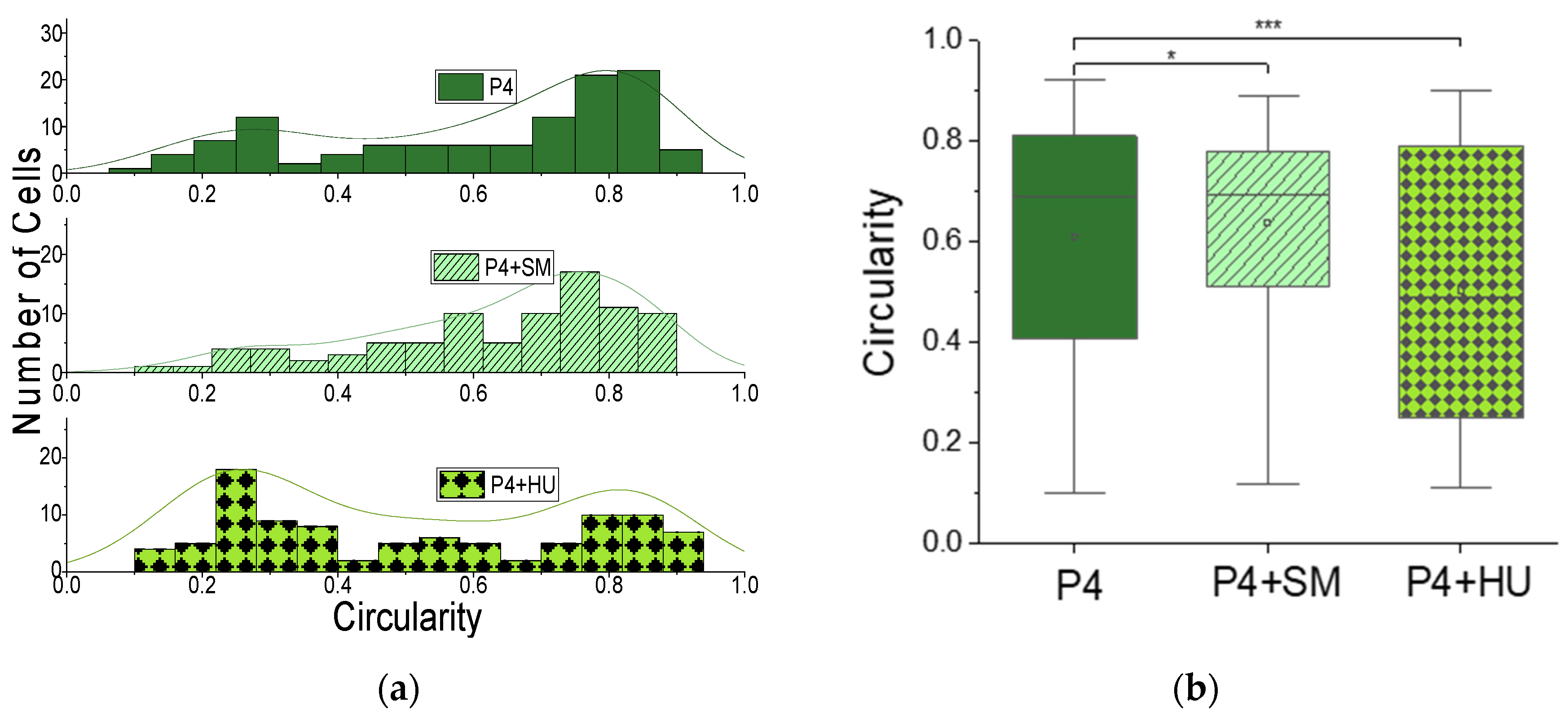
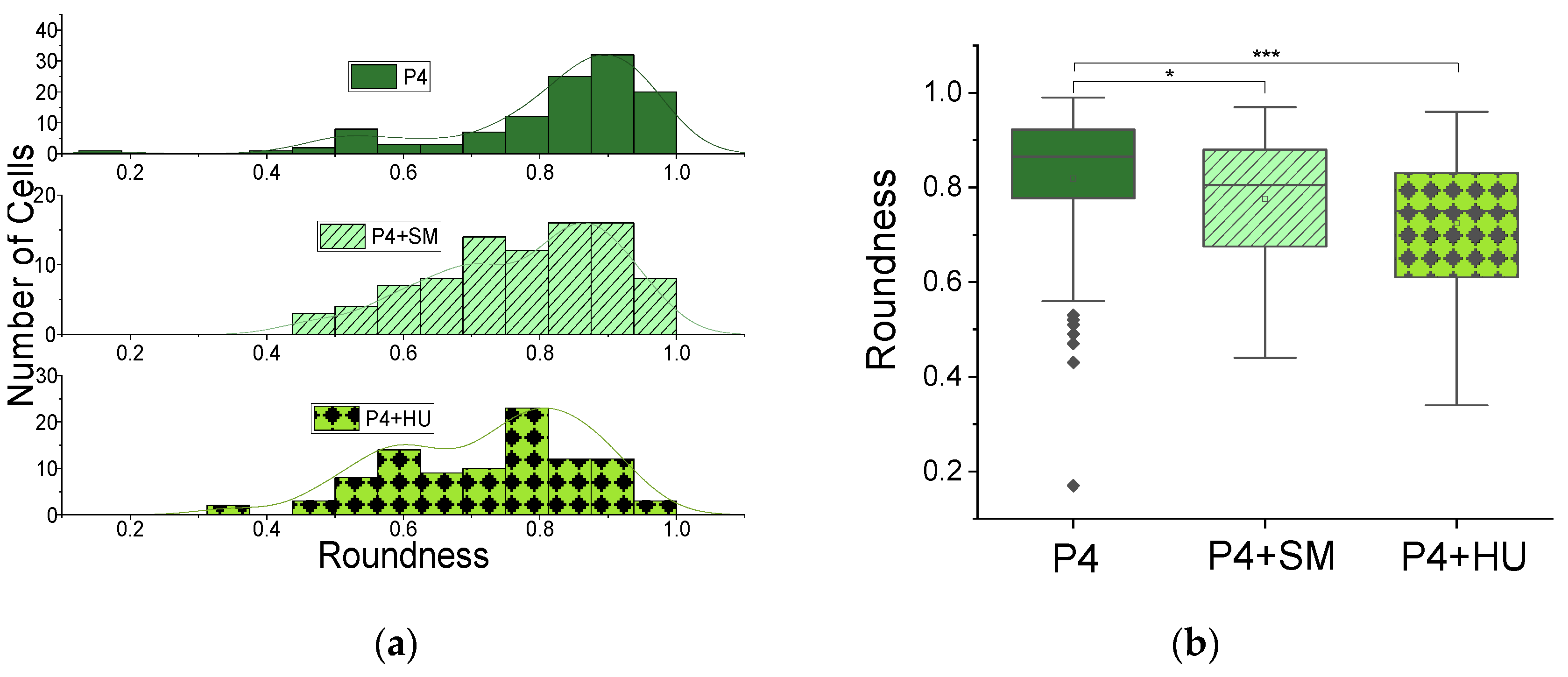
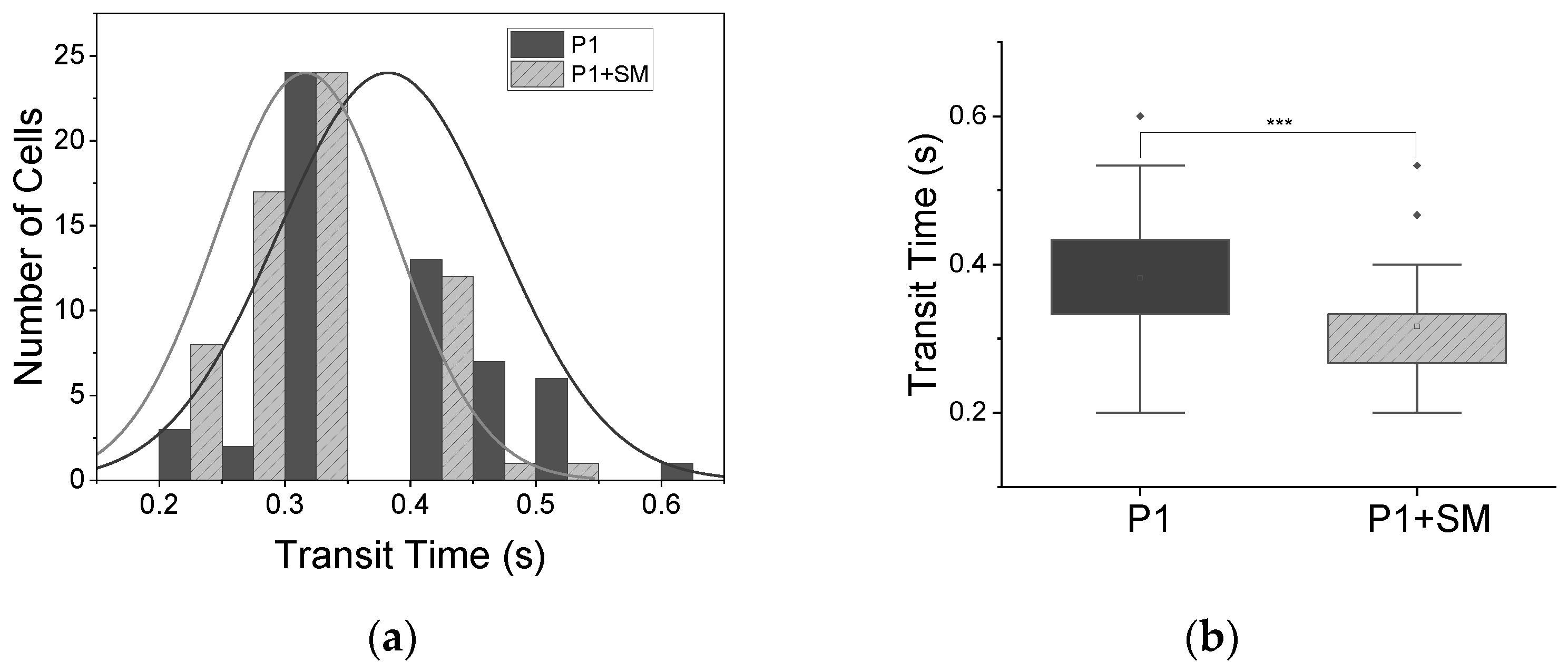
3.2.2. Monitoring of Drug Impact on ‘VOC’
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stuart, M.J.; Nagel, R.L. Sickle-cell disease. Lancet 2004, 364, 1343–1360. [Google Scholar] [CrossRef]
- WHO. Sickle Cell Disease: A Strategy for the WHO African Region. Report of the Regional Director; World Health Organization Regional Office for Africa AFR/RC60/8: Malabo, Equatorial Guinea, 2010. [Google Scholar]
- Piel, F.B.; Hay, S.I.; Gupta, S.; Weatherall, D.J.; Williams, T.N. Global burden of sickle cell anaemia in children under five, 2010-2050: Modelling based on demographics, excess mortality, and interventions. PLoS Med. 2013, 10, e1001484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- “Data & Statistics on Sickle Cell Disease | CDC.” [Online]. Available online: https://www.cdc.gov/ncbddd/sicklecell/data.html (accessed on 15 January 2021).
- Pauling, L.; Itano, H.A.; Singer, S.J.; Wells, I.C. Sickle cell anemia a molecular disease. Science 1949, 25, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Ingram, V.M. Haemoglobin, Gene mutations in human haemoglobin: The chemical difference between normal and sickle cell. Nature 1957, 180, 326–328. [Google Scholar] [CrossRef] [PubMed]
- Bunn, H.F. Pathogenesis and treatment of sickle cell disease. N. Engl. J. Med. 1997, 337, 762–769. [Google Scholar] [CrossRef]
- Bookchin, R.; Lew, V. Progressive inhibition of the Ca pump and Ca:Ca exchange in sickle red cells. Nature 1980, 284, 561–563. [Google Scholar] [CrossRef]
- Gibson, J.S.; Elory, J. Membrane transport in sickle cell disease. Blood Cells Mol. Dis. 2002, 28, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.J.; Ekpenyong, A.; Golfier, S.; Li, W.; Chalut, K.; Otto, O.; Elgeti, J.; Guck, J.; Lautenschläger, F. Myosin II activity softens cells in suspension. Biophys. J. 2015, 108, 1856–1869. [Google Scholar] [CrossRef] [Green Version]
- Ekpenyong, E.; Toepfner, N.; Chilvers, E.R.; Guck, J. Mechanotransduction in neutrophil activation and deactivation. Biochim. Biophys. Acta-Mol. Cell Res. 2015, 1853, 3105–3116. [Google Scholar] [CrossRef] [Green Version]
- Ekpenyong, E.; Toepfner, N.; Fiddler, C.; Herbig, M.; Li, W.; Cojoc, G.; Summers, C.; Guck, J.; Chilvers, E.R. Mechanical deformation induces depolarization of neutrophils. Sci. Adv. 2017, 3, e1602536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prathivadhi-Bhayankaram, S.V.; Ning, J.; Mimlitz, M.; Taylor, C.; Gross, E.; Nichols, M.; Guck, J.; Ekpenyong, A.E. Chemotherapy impedes in vitro microcirculation and promotes migration of leukemic cells with impact on metastasis. Biochem. Biophys. Res. Commun. 2016, 479, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Tietze, S.; Kräter, M.; Jacobi, A.; Taubenberger, A.; Herbig, M.; Wehner, R.; Schmitz, M.; Otto, O.; List, C.; Kaya, B.; et al. Spheroid Culture of Mesenchymal Stromal Cells Results in Morphorheological Properties Appropriate for Improved Microcirculation. Adv. Sci. 2019, 6, 1802104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lautenschläger, F.; Paschke, S.; Schinkinger, S.; Bruel, A.; Beil, M.; Guck, J. The regulatory role of cell mechanics for migration of differentiating myeloid cells. Proc. Natl. Acad. Sci. USA 2009, 106, 15696–15701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekpenyong, E.; Whyte, G.; Chalut, K.; Pagliara, S.; Lautenschläger, F.; Fiddler, C.; Paschke, S.; Keyser, U.F.; Chilvers, E.R.; Guck, J. Viscoelastic Properties of Differentiating Blood Cells Are Fate- and Function-Dependent. PLoS ONE 2012, 7, e45237. [Google Scholar]
- Fletcher, D.A.; Mullins, R.D. Cell mechanics and the cytoskeleton. Nature 2010, 463, 485–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Weaver, V.M. Mechanics, malignancy, and metastasis: The force journey of a tumor cell. Cancer Metastasis Rev. 2009, 28, 113–127. [Google Scholar] [CrossRef] [Green Version]
- Remmerbach, T.W.; Wottawah, F.; Dietrich, J.; Lincoln, B.; Wittekind, C.; Guck, J. Oral cancer diagnosis by mechanical phenotyping. Cancer Res. 2009, 69, 1728–1732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guck, J.; Chilvers, E.R. Mechanics meets medicine. Sci. Transl. Med. 2013, 5, 212fs41. [Google Scholar] [CrossRef]
- Nader, E.; Skinner, S.; Romana, M.; Fort, R.; Lemonne, N.; Guillot, N.; Gauthier, A.; Antoine-Jonville, S.; Renoux, C.; Hardy-Dessources, M.-D.; et al. Blood rheology: Key parameters, impact on blood flow, role in sickle cell disease and effects of exercise. Front. Physiol. Front. Media S.A. 2019, 10, 1329. [Google Scholar] [CrossRef] [Green Version]
- Otto, O.; Rosendahl, P.; Mietke, A.; Golfier, S.; Herold, C.; Klaue, D.; Girardo, S.; Pagliara, S.; Ekpenyong, A.; Jacobi, A.; et al. Real-time deformability cytometry: On-the-fly cell mechanical phenotyping. Nat. Methods 2015, 12, 199–202. [Google Scholar] [CrossRef]
- Guruprasad, P.; Mannino, R.G.; Caruso, C.; Zhang, H.; Josephson, C.D.; Roback, J.D.; Lam, W.A. Integrated automated particle tracking microfluidic enables high-throughput cell deformability cytometry for red cell disorders. Am. J. Hematol. 2019, 94, 189–199. [Google Scholar] [CrossRef] [Green Version]
- Herrick, J.B. Peculiar elongated and sickle-shaped red blood corpuscles in a case of severe anemia. Yale J. Biol. Med. 2001, 74, 179–184. [Google Scholar] [PubMed]
- Hankins, J.S.; Ware, R.E.; Rogers, Z.R.; Wynn, L.W.; Lane, P.A.; Scott, J.P.; Wang, W.C. Long-term hydroxyurea therapy for infants with sickle cell anemia: The HUSOFT extension study. Blood 2005, 106, 2269–2275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaston, M.H.; Verter, J. Sickle cell anaemia trial. Stat. Med. 1990, 9, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M. Clinical aspects of sickle cell disease in sickle cell anemia and other hemoglobinopathies. In Sickle Cell Anemia and Other Haemoglobinopathies, 1st ed.; Levere, R., Ed.; Academic Press: New York, NY, USA, 1975; pp. 87–112. [Google Scholar]
- Manwani, D.; Frenette, P.S. Vaso-occlusion in sickle cell disease: Pathophysiology and novel targeted therapies. Blood 2013, 122, 3892–3898. [Google Scholar] [CrossRef] [PubMed]
- Randolph, T.R.; Le, A.; Demond, J. A Modified Sodium Metabisulfite Method to Distinguish Sickle Cell Disease from Sickle Cell Trait for Use in Underdeveloped Countries. Am. Soc. Clin. Lab. Sci. 2019, 30, ascls.119.002030. [Google Scholar] [CrossRef] [Green Version]
- Nader, E.; Grau, M.; Fort, R.; Collins, B.; Cannas, G.; Gauthier, A.; Walpurgis, K.; Martin, C.; Bloch, W.; Poutrel, S.; et al. Hydroxyurea therapy modulates sickle cell anemia red blood cell physiology: Impact on RBC deformability, oxidative stress, nitrite levels and nitric oxide synthase signaling pathway. Nitric Oxide-Biol. Chem. 2018, 81, 28–35. [Google Scholar] [CrossRef] [Green Version]
- Alapan, Y.; Kim, C.; Adhikari, A.; Gray, K.E.; Cavusoglu, E.G.; Little, J.A.; Gurkan, U.A. Sickle cell disease biochip: A functional red blood cell adhesion assay for monitoring sickle cell disease. Transl. Res. 2016, 173, 74–91.e8. [Google Scholar] [CrossRef] [Green Version]
- Alapan, Y.; Fraiwan, A.; Kucukal, E.; Hasan, M.N.; Ung, R.; Kim, M.; Odame, I.; Little, J.A.; Gurkan, U.A. Emerging point-of-care technologies for sickle cell disease screening and monitoring. Expert Rev. Med. Devices 2016, 13, 1073–1093. [Google Scholar] [CrossRef] [Green Version]
- Myers, D.R.; Sakurai, Y.; Chappa, P.; Barabino, G.; Archer, D.R.; Lam, W. Measuring the Direct Effects of Sickle Cell Vaso-Occlusion on Endothelial Cells Using Microfluidic Technology. Blood 2011, 118, 897. [Google Scholar] [CrossRef]
- Schneider, A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Du, E.; Lei, H.; Tang, Y.-H.; Dao, M.; Suresh, S.; Karniadakis, G.E. Patient-specific blood rheology in sickle-cell anaemia. Interface Focus 2016, 6, 20150065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, C.; Jung, F.; Kelm, M. The microcirculation in hypoxia: The center of the battlefield for oxygen. Clin. Hemorheol. Microcirc. 2016, 63, 169–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballas, S.K.; Connes, P. Rheological properties of sickle erythrocytes in patients with sickle-cell anemia: The effect of hydroxyurea, fetal hemoglobin, and α-thalassemia. Eur. J. Haematol. 2018, 101, 798–803. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Skewness (@Circularity) | Kurtosis (@Circularity) | Circularity Equation (1) | Skewness (@Roundness) | Kurtosis (@Roundness) | Roundness Equation (2) | |
|---|---|---|---|---|---|---|
| P4 | −0.64 | −0.98 | 0.61 ± 0.02 | −1.59906 | 2.79852 | 0.81 ± 0.01 |
| P4 + SM | −0.81 | −0.26 | 0.64 ± 0.02 | −0.59224 | −0.46862 | 0.78 ± 0.01 |
| P4 + HU | 0.17 | −1.54 | 0.50 ± 0.03 | −0.49392 | −0.46354 | 0.72 ± 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asuquo, M.I.; Effa, E.; Gbotosho, O.; Otu, A.; Toepfner, N.; Ameh, S.; Bhayankaram, S.-P.; Zetocha, N.; Nwakama, C.; Egbe, W.; et al. Microfluidic Microcirculation Mimetic as a Tool for the Study of Rheological Characteristics of Red Blood Cells in Patients with Sickle Cell Anemia. Appl. Sci. 2022, 12, 4394. https://doi.org/10.3390/app12094394
Asuquo MI, Effa E, Gbotosho O, Otu A, Toepfner N, Ameh S, Bhayankaram S-P, Zetocha N, Nwakama C, Egbe W, et al. Microfluidic Microcirculation Mimetic as a Tool for the Study of Rheological Characteristics of Red Blood Cells in Patients with Sickle Cell Anemia. Applied Sciences. 2022; 12(9):4394. https://doi.org/10.3390/app12094394
Chicago/Turabian StyleAsuquo, Marcus Inyama, Emmanuel Effa, Oluwabukola Gbotosho, Akaninyene Otu, Nicole Toepfner, Soter Ameh, Sruti-Prathivadhi Bhayankaram, Noah Zetocha, Chisom Nwakama, William Egbe, and et al. 2022. "Microfluidic Microcirculation Mimetic as a Tool for the Study of Rheological Characteristics of Red Blood Cells in Patients with Sickle Cell Anemia" Applied Sciences 12, no. 9: 4394. https://doi.org/10.3390/app12094394
APA StyleAsuquo, M. I., Effa, E., Gbotosho, O., Otu, A., Toepfner, N., Ameh, S., Bhayankaram, S.-P., Zetocha, N., Nwakama, C., Egbe, W., Guck, J., & Ekpenyong, A. (2022). Microfluidic Microcirculation Mimetic as a Tool for the Study of Rheological Characteristics of Red Blood Cells in Patients with Sickle Cell Anemia. Applied Sciences, 12(9), 4394. https://doi.org/10.3390/app12094394