
Are the Currently Available Elastography Methods Useful in the Assessment of Chronic Kidney Disease? A Systematic Review and a Meta-Analysis

 ,
, 
 and
and
Abstract
:1. Introduction
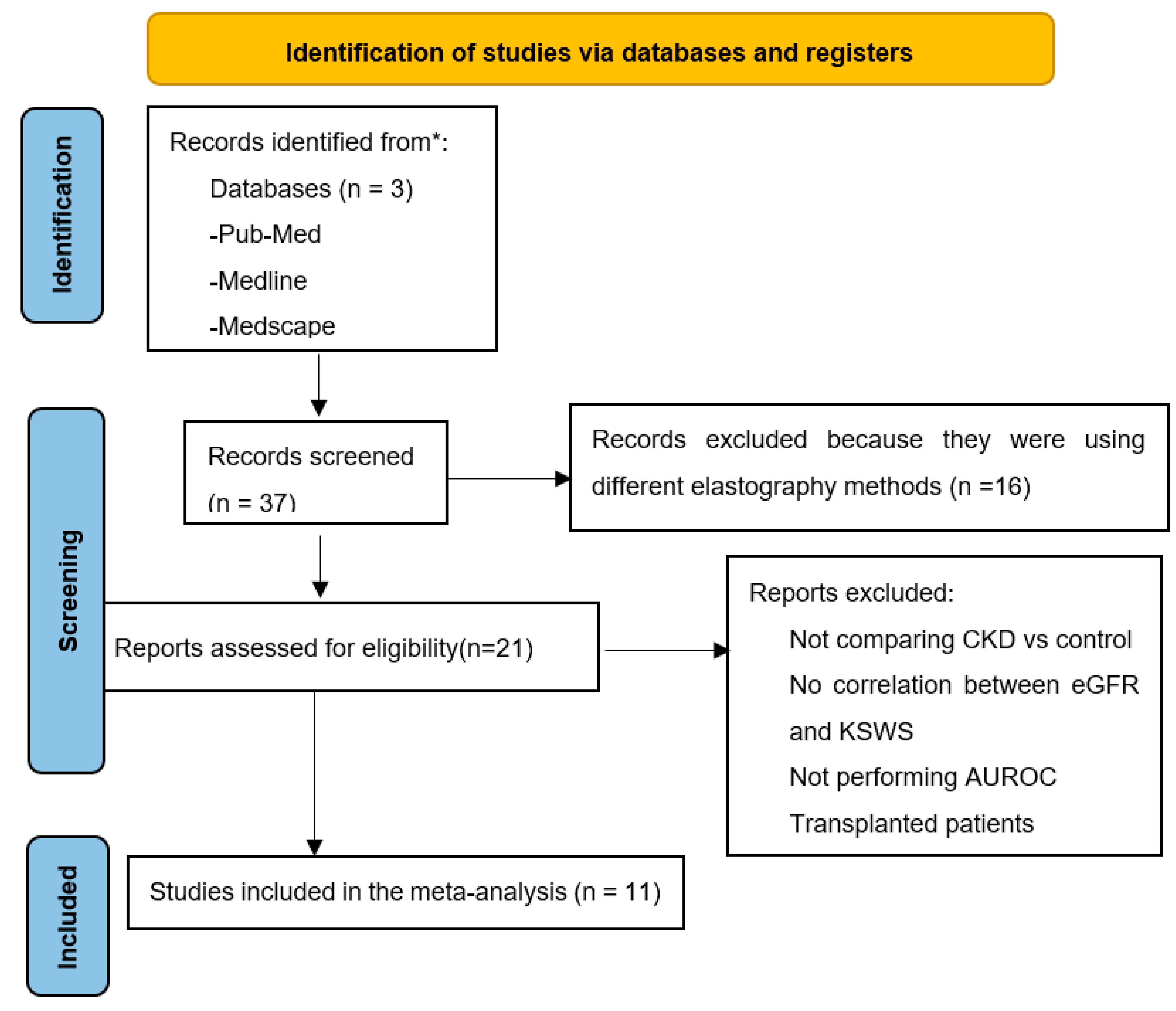
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Data Sources and Searches
2.3. Study Selection and Data Extraction
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Turner, N.; Lameire, N.; Goldsmith, D.J.; Winearls, C.G.; Himmelfarb, J.; Remuzzi, G. Oxford Textbook of Clinical Nephrology, 4th ed.; Oxford University Press: Oxford, UK, 2016. [Google Scholar]
- Hu, Q.; Zhang, W.J.; Lin, Z.Q.; Wang, X.Y.; Zheng, H.Y.; Wei, H.M.; He, H.G. Combined acoustic radiation force impulse and conventional ultrasound in the quantitative assessment of immunoglobulin a nephropathy. Ultrasound Med. Biol. 2019, 45, 2309–2316. [Google Scholar] [CrossRef] [PubMed]
- Moghazi, S.; Jones, E.; Schroepple, J.; Arya, K.; Mcclellan, W.; Hennigar, R.A.; O’Neill, W.C. Correlation of renal histopathology with sonographic findings. Kidney Int. 2005, 67, 1515–1520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ophir, J.; Ccspedes, I.; Ponnekanti, H.; Yazdi, Y.; Li, X. Elastography: A quantitative method for imaging the elasticity of biological tissues. Ultrason. Imaging 1991, 13, 111–134. [Google Scholar] [CrossRef] [PubMed]
- Hou, X.J.; Sun, A.X.; Zhou, X.L.; Ji, Q.; Wang, H.B.; Wei, H.; Sun, J.W.; Liu, H. The application of Virtual Touch tissue quantification (VTQ) in diagnosis of thyroid lesions: A preliminary study. Eur. J. Radiol. 2013, 82, 797–801. [Google Scholar] [CrossRef]
- Nierhoff, J.; Chávez Ortiz, A.A.; Herrmann, E.; Zeuzem, S.; Friedrich-Rust, M. The efficiency of acoustic radiation force impulse imaging for the staging of liver fibrosis: A meta-analysis. Eur. Radiol. 2013, 23, 3040–3053. [Google Scholar] [CrossRef]
- Chen, C.; Wang, C.; Hu, C.; Han, Y.; Zhao, L.; Zhu, X.; Xiao, L.; Sun, L. Normoalbuminuric diabetic kidney disease. Front. Med. 2017, 11, 310–318. [Google Scholar] [CrossRef]
- Shiina, T.; Nightingale, K.R.; Palmeri, M.L.; Hall, T.J.; Bamber, J.C.; Barr, R.G.; Castera, L.; Choi, B.I.; Chou, Y.H.; Cosgrove, D.; et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 1: Basic principles and terminology. Ultrasound Med. Biol. 2015, 41, 1126–1147. [Google Scholar] [CrossRef] [Green Version]
- Săftoiu, A.; Gilja, O.H.; Sidhu, P.S.; Dietrich, C.F.; Cantisani, V.; Amy, D.; Bachmann-Nielsen, M.; Bob, F.; Bojunga, J.; Brock, M.; et al. The EFSUMB guidelines and recommendations for the clinical practice of elastography in non-hepatic applications: Update 2018. Ultraschall Der Med. 2019, 40, 425–453. [Google Scholar] [CrossRef] [Green Version]
- Bob, F.; Grosu, I.; Sporea, I.; Timar, R.; Lighezan, D.; Popescu, A.; Sirli, R.; Buzas, R.; Petrica, L.; Munteanu, M.; et al. Is Kidney stiffness measured using elastography influenced mainly by vascular factors in patients with diabetic kidney disease? Ultrason. Imaging 2018, 40, 300–309. [Google Scholar] [CrossRef]
- Arndt, R.; Schmidt, S.; Loddenkemper, C.; Grünbaum, M.; Zidek, W.; Van Der Giet, M.; Westhoff, T.H. Noninvasive evaluation of renal allograft fibrosis by transient elastography—A pilot study. Transpl. Int. 2010, 23, 871–877. [Google Scholar] [CrossRef]
- Lukenda, V.; Mikolasevic, I.; Racki, S.; Jelic, I.; Stimac, D.; Orlic, L. Transient elastography: A new noninvasive diagnostic tool for assessment of chronic allograft nephropathy. Int. Urol. Nephrol. 2014, 46, 1435–1440. [Google Scholar] [CrossRef] [PubMed]
- Nakao, T.; Ushigome, H.; Nakamura, T.; Harada, S.; Koshino, K.; Suzuki, T.; Ito, T.; Nobori, S.; Yoshimura, N. Evaluation of renal allograft fibrosis by transient elastography (fibro scan). Transplant. Proc. 2015, 47, 640–643. [Google Scholar] [CrossRef] [PubMed]
- Sommerer, C.; Scharf, M.; Seitz, C.; Millonig, G.; Seitz, H.K.; Zeier, M.; Mueller, S. Assessment of renal allograft fibrosis by transient elastography. Transpl. Int. 2013, 26, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Menzilcioglu, M.S.; Duymus, M.; Citil, S.; Avcu, S.; Gungor, G.; Sahin, T.; Boysan, S.N.; Altunoren, O.; Sarica, A. Strain wave elastography for evaluation of renal parenchyma in chronic kidney disease. Br. J. Radiol. 2015, 88, 20140714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menzilcioglu, M.S.; Duymus, M.; Citil, S.; Gungor, G.; Saglam, M.; Gungor, O.; Boysan, S.N.; Sarıca, A.; Avcu, S. The comparison of resistivity index and strain index values in the ultrasonographic evaluation of chronic kidney disease. Radiol. Med. 2016, 121, 681–687. [Google Scholar] [CrossRef]
- Lin, H.Y.H.; Lee, Y.L.; Lin, K.D.; Chiu, Y.W.; Shin, S.J.; Hwang, S.J.; Chen, H.C.; Hung, C.C. Association of renal elasticity and renal function progression in patients with chronic kidney disease evaluated by real-time ultrasound elastography. Sci. Rep. 2017, 7, 43303. [Google Scholar] [CrossRef]
- Guo, L.H.; Xu, H.X.; Fu, H.J.; Peng, A.; Zhang, Y.F.; Liu, L.N. Acoustic radiation force impulse imaging for noninvasive evaluation of renal parenchyma elasticity: Preliminary findings. PLoS ONE 2013, 8, e68925. [Google Scholar] [CrossRef] [Green Version]
- Stock, K.F.; Klein, B.S.; Cong, M.T.; Regenbogen, C.; Kemmner, S.; Büttner, M.; Wagenpfeil, S.; Matevossian, E.; Renders, L.; Heemann, U.; et al. ARFI-based tissue elasticity quantification and kidney graft dysfunction: First clinical experiences. Clin. Hemorheol. Microcirc. 2011, 49, 527–535. [Google Scholar] [CrossRef]
- Syversveen, T.; Brabrand, K.; Midtvedt, K.; Strøm, E.H.; Hartmann, A.; Jakobsen, J.A.; Berstad, A.E. Assessment of renal allograft fibrosis by acoustic radiation force impulse quantification—A pilot study. Transpl. Int. 2011, 24, 100–105. [Google Scholar] [CrossRef]
- Hu, Q.; Wang, X.Y.; He, H.G.; Wei, H.M.; Kang, L.K.; Qin, G.C. Acoustic radiation force impulse imaging for non-invasive assessment of renal histopathology in chronic kidney disease. PLoS ONE 2014, 9, e115051. [Google Scholar] [CrossRef] [Green Version]
- Yu, N.; Zhang, Y.; Xu, Y. Value of Virtual Touch tissue quantification in stages of diabetic kidney disease. J. Ultrasound Med. 2014, 33, 787–792. [Google Scholar] [CrossRef] [PubMed]
- Asano, K.; Ogata, A.; Tanaka, K.; Ide, Y.; Sankoda, A.; Kawakita, C.; Nishikawa, M.; Ohmori, K.; Kinomura, M.; Shimada, N.; et al. Acoustic radiation force impulse elastography of the kidneys: Is shear wave velocity affected by tissue fibrosis or renal blood flow? J. Ultrasound Med. 2014, 33, 793–801. [Google Scholar] [CrossRef]
- Wang, L.; Xia, P.; Lv, K.; Han, J.; Dai, Q.; Li, X.M.; Chen, L.M.; Jiang, Y.X. Assessment of renal tissue elasticity by acoustic radiation force impulse quantification with histopathological correlation: Preliminary experience in chronic kidney disease. Eur. Radiol. 2014, 24, 1694–1699. [Google Scholar] [CrossRef] [PubMed]
- Cui, G.; Yang, Z.; Zhang, W.; Li, B.; Sun, F.; Xu, C.; Wang, K. Evaluation of acoustic radiation force impulse imaging for the clinicopathological typing of renal fibrosis. Exp. Ther. Med. 2013, 7, 233–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bob, F.; Bota, S.; Sporea, I.; Sirli, R.; Popescu, A.; Schiller, A. Relationship between the estimated glomerular filtration rate and kidney shear wave speed values assessed by acoustic radiation force impulse elastography: A pilot study. J. Ultrasound Med. 2015, 34, 649–654. [Google Scholar] [CrossRef] [PubMed]
- Bob, F.; Bota, S.; Sporea, I.; Sirli, R.; Petrica, L.; Schiller, A. Kidney shear wave speed values in subjects with and without renal pathology and inter-operator reproducibility of acoustic radiation force impulse Elastography (ARFI)—Preliminary results. PLoS ONE 2014, 9, e113761. [Google Scholar] [CrossRef] [Green Version]
- Takata, T.; Koda, M.; Sugihara, T.; Sugihara, S.; Okamoto, T.; Miyoshi, K.; Matono, T.; Hosho, K.; Mae, Y.; Iyama, T.; et al. Renal shear wave velocity by acoustic radiation force impulse did not reflect advanced renal impairment. Nephrology 2016, 21, 1056–1062. [Google Scholar] [CrossRef]
- Alan, B.; Göya, C.; Aktan, A.; Alan, S. Renal acoustic radiation force impulse elastography in the evaluation of coronary artery disease. Acta Radiol. 2017, 58, 156–163. [Google Scholar] [CrossRef]
- Bob, F.; Grosu, I.; Sporea, I.; Bota, S.; Popescu, A.; Sima, A.; Şirli, R.; Petrica, L.; Timar, R.; Schiller, A. Ultrasound-based shear wave elastography in the assessment of patients with diabetic kidney disease. Ultrasound Med. Biol. 2017, 43, 2159–2166. [Google Scholar] [CrossRef]
- Bilgici, M.C.; Bekci, T.; Genc, G.; Tekcan, D.; Tomak, L. Acoustic radiation force impulse quantification in the evaluation of renal parenchyma elasticity in pediatric patients with chronic kidney disease: Preliminary results. J. Ultrasound Med. 2017, 36, 1555–1561. [Google Scholar] [CrossRef]
- Grass, L.; Szekely, N.; Alrajab, A.; Bui-Ta, T.T.T.; Hoffmann, G.F.; Wühl, E.; Schenk, J.P. Point shear wave elastography (pSWE) using Acoustic Radiation Force Impulse (ARFI) imaging: A feasibility study and norm values for renal parenchymal stiffness in healthy children and adolescents. Med. Ultrason. 2017, 19, 366–373. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, Y.; Hirooka, Y.; Kawashima, H.; Ishikawa, T.; Takeshita, K.; Goto, H. Measurements of renal shear wave velocities in chronic kidney disease patients. Acta Radiol. 2018, 59, 884–890. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, N.; Yu, J.; Wang, H.; Li, X. Virtual touch tissue quantification for assessing renal pathology in idiopathic nephrotic syndrome. Ultrasound Med. Biol. 2018, 44, 1318–1326. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Oh, Y.T.; Joo, D.J.; Ma, B.G.; Lee, A.L.; Lee, J.G.; Song, S.H.; Kim, S.U.; Jung, D.C.; Chung, Y.E.; et al. Acoustic radiation force impulse measurement in renal transplantation: A prospective, longitudinal study with protocol biopsies. Medicine 2015, 94, e1590. [Google Scholar] [CrossRef] [PubMed]
- Yoǧurtçuoǧlu, B.; Damar, Ç. Renal elastography measurements in children with acute glomerulonephritis. Ultrasonography 2021, 40, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Caraba, A.; Munteanu, A.; Iurciuc, S.; Iurciuc, M. Renal acoustic radiation force impulse elastography in hypertensive nephroangiosclerosis patients. Appl. Sci. 2021, 11, 612. [Google Scholar] [CrossRef]
- Grosu, I.; Bob, F.; Sporea, I.; Popescu, A.; Şirli, R.; Schiller, A. Correlation of point shear wave velocity and kidney function in chronic kidney disease. J. Ultrasound Med. 2018, 37, 2613–2620. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.Y.; Duan, Q.; Fu, X.H.; Fu, L.Q.; Xia, H.W.; Wan, Y.L. Value of elastography point quantification in improving the diagnostic accuracy of early diabetic kidney disease. World J. Clin. Cases 2019, 7, 3945–3956. [Google Scholar] [CrossRef]
- Sumbul, H.E.; Koc, A.S.; Gülümsek, E. Renal cortical stiffness is markedly increased in pre-diabetes mellitus and associated with albuminuria. Singap. Med. J. 2020, 61, 435–442. [Google Scholar] [CrossRef]
- Leong, S.S.; Wong, J.H.D.; Md Shah, M.N.; Vijayananthan, A.; Jalalonmuhali, M.; Chow, T.K.; Sharif, N.H.; Ng, K.H. Shear wave elastography accurately detects chronic changes in renal histopathology. Nephrology 2021, 26, 38–45. [Google Scholar] [CrossRef]
- Grenier, N.; Poulain, S.; Lepreux, S.; Gennisson, J.L.; Dallaudière, B.; Lebras, Y.; Bavu, E.; Servais, A.; Meas-Yedid, V.; Piccoli, M.; et al. Quantitative elastography of renal transplants using supersonic shear imaging: A pilot study. Eur. Radiol. 2012, 22, 2138–2146. [Google Scholar] [CrossRef] [PubMed]
- Samir, A.E.; Allegretti, A.S.; Zhu, Q.; Dhyani, M.; Anvari, A.; Sullivan, D.A.; Trottier, C.A.; Dougherty, S.; Williams, W.W.; Babitt, J.L.; et al. Shear wave elastography in chronic kidney disease: A pilot experience in native kidneys. BMC Nephrol. 2015, 16, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radulescu, D.; Peride, I.; Petcu, L.C.; Niculae, A.; Checherita, I.A. Supersonic shear wave ultrasonography for assessing tissue stiffness in native kidney. Ultrasound Med. Biol. 2018, 44, 2556–2568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, X.; Hou, F.L.; Zhao, C.; Jiang, C.Y.; Li, X.M.; Yu, N. The role of real-time shear wave elastography in the diagnosis of idiopathic nephrotic syndrome and evaluation of the curative effect. Abdom. Radiol. 2020, 45, 2508–2517. [Google Scholar] [CrossRef]
- Grosu, I.; Bob, F.; Sporea, I.; Popescu, A.; Sirli, R.; Schiller, A. Two-dimensional shear-wave elastography for kidney stiffness assessment. Ultrasound Q. 2021, 37, 144–148. [Google Scholar] [CrossRef]
- Wang, L. New insights on the role of anisotropy in renal ultrasonic elastography: From trash to treasure. Med. Hypotheses 2020, 143, 110146. [Google Scholar] [CrossRef]
- Wu, J.F.; Ge, L.J.; Ye, X.B.; Sun, Y.; Wang, Y.L.; Wang, Z.P. Can acoustic radiation force impulse imaging (ARFI) accurately diagnose renal masses?: A protocol of systematic review and meta-analysis. Medicine 2020, 99, e21500. [Google Scholar] [CrossRef]
- Hwang, J.; Kim, H.W.; Kim, P.H.; Suh, C.H.; Yoon, H.M. Technical performance of acoustic radiation force impulse imaging for measuring renal parenchymal stiffness: A systematic review and meta-analysis. J. Ultrasound Med. 2021, 40, 2639–2653. [Google Scholar] [CrossRef]
- Cosgrove, D.; Piscaglia, F.; Bamber, J.; Bojunga, J.; Correas, J.M.; Gilja, O.H.; Klauser, A.S.; Sporea, I.; Calliada, F.; Cantisani, V.; et al. EFSUMB guidelines and recommendations on the clinical use of ultrasound elastography. Part 2: Clinical applications. Ultraschall Der Med. 2013, 34, 238–253. [Google Scholar] [CrossRef] [Green Version]
- Garcia, S.R.M.; Grossmann, M.; Lang, S.T.; Trong, M.N.; Schultz, M.; Guo, J.; Hamm, B.; Braun, J.; Sack, I.; Tzschätzsch, H. Full-Field-of-view time-harmonic elastography of the native kidney. Ultrasound Med. Biol. 2018, 44, 949–954. [Google Scholar] [CrossRef]
- Grossmann, M.; Tzschätzsch, H.; Lang, S.T.; Guo, J.; Bruns, A.; Dürr, M.; Hoyer, B.F.; Grittner, U.; Lerchbaumer, M.; Nguyen Trong, M.; et al. US time-harmonic elastography for the early detection of glomerulonephritis. Radiology 2019, 292, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Barr, R.G. Can accurate shear wave velocities be obtained in kidneys? J. Ultrasound Med. 2020, 39, 1097–1105. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nr. | Study | Elastography Method | CKD Patients | Healthy Subjects | Kidney SWS in CKD | CKD vs. Control Group | Correlation Coefficient Kidney SWS < >eGFR(p < 0.05) | AUROC/Cut-Off Values |
|---|---|---|---|---|---|---|---|---|
| 1. | Arndt et al., 2010 [11] | TE | 57 transplanted patients | - | High | - | Correlated | - |
| 2. | Lukenda V et al., 2014 [12] | TE | 23 transplanted patients | - | High | - | Correlated | - |
| 3. | Nakao et al., 2015 [13] | TE | 27 transplanted patients | - | High | - | Correlated | - |
| 4. | Sommerer et al., 2013 [14] | TE | 164 transplanted patients | - | High | - | - | - |
| 5. | Menzilcioglu et al., 2015 [15] | SE | 58 | 40 | High | Yes | - | Performed |
| 6. | Menzilcioglu et al., 2016 [16] | SE | 121 | 40 | High | Yes | - | Performed |
| 7. | Lin et al., 2017 [17] | RTE | 148 | 277 | Low | Yes | Correlated | - |
| 8. | Guo et al., 2013 [18] | VTQ | 64 | 327 | Low | Yes | Correlated | Performed |
| 9. | Stock et al., 2011, [19] | VTQ | 18 transplanted patients | - | High | - | - | - |
| 10. | Syversveen et al., 2011, [20] | VTQ | 30 transplanted patients | - | No relationship | - | - | - |
| 11. | Hu et al., 2014 [21] | VTQ | 163 | 32 | Low | Yes | Correlated | Performed |
| 12. | Yu et al., 2014 [22] | VTQ | 120 | 30 | High | Yes | - | Performed |
| 13. | Asano K et al., 2014 [23] | VTQ | 309 | 14 | Low | - | Correlated | - |
| 14. | Wang et al., 2014 [24] | VTQ | 45 | - | No relationship | - | - | - |
| 15. | Cui et al., 2014 [25] | VTQ | 76 | - | High | Yes | - | Performed |
| 16. | Bob et al., 2015 [26] | VTQ | 46 | 58 | Low | - | Correlated | - |
| 17. | Bob et al., 2015 [27] | VTQ | 20 | - | Low | Yes | - | Performed |
| 18. | Takata et al., 2015 [28] | VTQ | 90 | 39 | Low | Yes | - | - |
| 19. | Alan et al., 2016 [29] | VTQ | 76 | 79 | Low | Yes | - | - |
| 20. | Bob et al., 2017 [30] | VTQ | 80 | 84 | Low | Yes | Correlated | - |
| 21. | Bilgici et al., 2017 [31] | VTQ | 30 pediatric patients | 38 | Low | Yes | - | Performed |
| 22. | Grass et al., 2017 [32] | VTQ | - | 264 healthy children | No relationship | - | - | - |
| 23. | Sasaki et al., 2018 [33] | VTQ | 187 | - | No relationship | - | - | - |
| 24. | Yang et al., 2018 [34] | VTQ | 90 idiopathic nephrotic syndrome | 30 | High | Yes | - | Performed |
| 25. | Hu et al., 2019 [2] | VTQ | 146 | 39 | Low | Yes | - | Performed |
| 26. | Lee et al., 2015 [35] | VTQ | 73(biopsies of kidney donors before transplant) | - | Low | - | Correlated | - |
| 27. | Yoǧurtçuoǧlu et al., 2021 [36] | VTQ | 30 acute glomerulonephritis | 30 | High | Yes | - | - |
| 28. | Caraba et al., 2021 [37] | VTQ | 80 | 50 | Low | Yes | Correlated | Performed |
| 29. | Grosu et al., 2018 [38] | Elast-PQ | 102 | 22 | Low | Yes | Correlated (but with no statistical performance) | Performed (CKD vs. control group) |
| 30. | Liu et al., 2019 [39] | Elast-PQ | 102 | 22 | Low | - | - | Performed (only patients with type 2 diabetes) |
| 31. | Sumbul et al., 2020 [40] | Elast-PQ | 22 | 103 | High | Yes | Correlated | Performed(non-diabetic, pre-diabetic, diabetic patients) |
| 32. | Leong et al., 2021 [41] | ElastPQ | 75 | - | High | Yes | - | Performed (differentiating between mildly and moderately impaired kidneys) |
| 33. | Grenier et al., 2012 [42] | 2D SWE-SSI | 43 transplanted patients | - | No relationship | - | - | - |
| 34. | Samir et al., 2015 [43] | 2D SWE-SSI | 25 | 20 | High | Yes | - | Performed |
| 35. | Radulescu et al., 2018 [44] | 2D-SWE-SSI | 32 | 22 | High | Yes | - | Performed |
| 36. | Yang et al., 2020 [45] | 2D-SWE-SSI | 120 idiopathic nephrotic syndrome | - | High | Yes | - | Performed |
| 37. | Grosu et al., 2021 [46] | 2D-SWE-GE | 42 | 50 | Low | Yes | - | Performed |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maralescu, F.-M.; Chiodan, M.; Sircuta, A.; Schiller, A.; Petrica, L.; Bob, F. Are the Currently Available Elastography Methods Useful in the Assessment of Chronic Kidney Disease? A Systematic Review and a Meta-Analysis. Appl. Sci. 2022, 12, 2359. https://doi.org/10.3390/app12052359
Maralescu F-M, Chiodan M, Sircuta A, Schiller A, Petrica L, Bob F. Are the Currently Available Elastography Methods Useful in the Assessment of Chronic Kidney Disease? A Systematic Review and a Meta-Analysis. Applied Sciences. 2022; 12(5):2359. https://doi.org/10.3390/app12052359
Chicago/Turabian StyleMaralescu, Felix-Mihai, Milena Chiodan, Alexandru Sircuta, Adalbert Schiller, Ligia Petrica, and Flaviu Bob. 2022. "Are the Currently Available Elastography Methods Useful in the Assessment of Chronic Kidney Disease? A Systematic Review and a Meta-Analysis" Applied Sciences 12, no. 5: 2359. https://doi.org/10.3390/app12052359
APA StyleMaralescu, F.-M., Chiodan, M., Sircuta, A., Schiller, A., Petrica, L., & Bob, F. (2022). Are the Currently Available Elastography Methods Useful in the Assessment of Chronic Kidney Disease? A Systematic Review and a Meta-Analysis. Applied Sciences, 12(5), 2359. https://doi.org/10.3390/app12052359