
Does a Previous Segmentation Improve the Automatic Detection of Basal Cell Carcinoma Using Deep Neural Networks?


Abstract
:1. Introduction
2. Materials and Methods
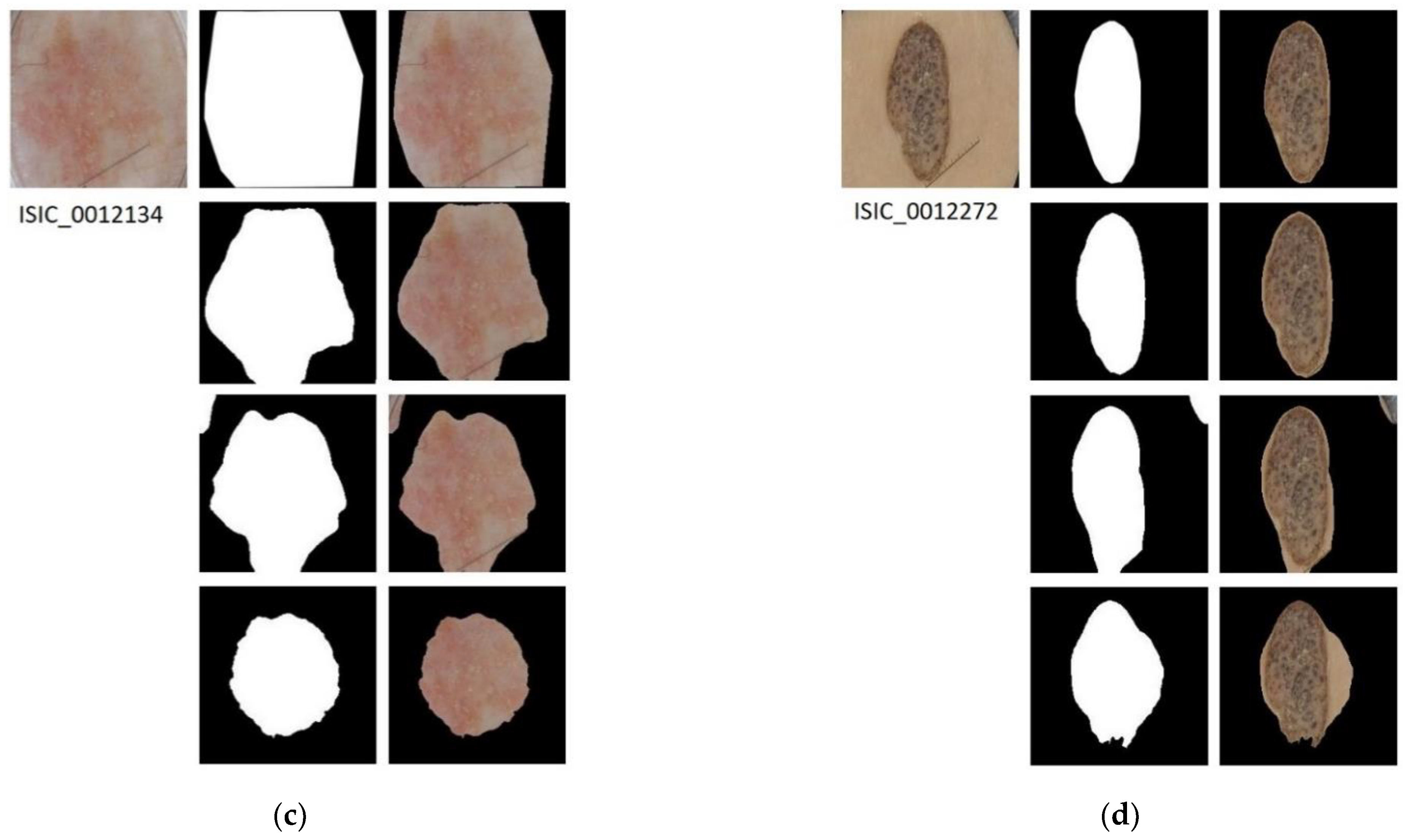
2.1. Lesion Segmentation
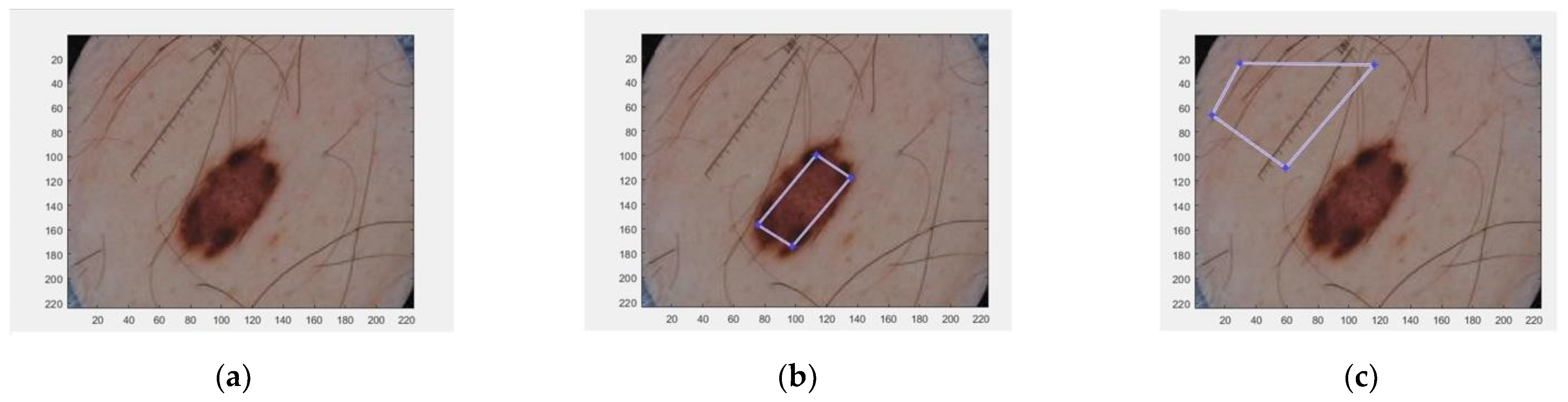
2.1.1. Unsupervised Method: Energy Minimization Based Algorithm
2.1.2. Supervised Methods
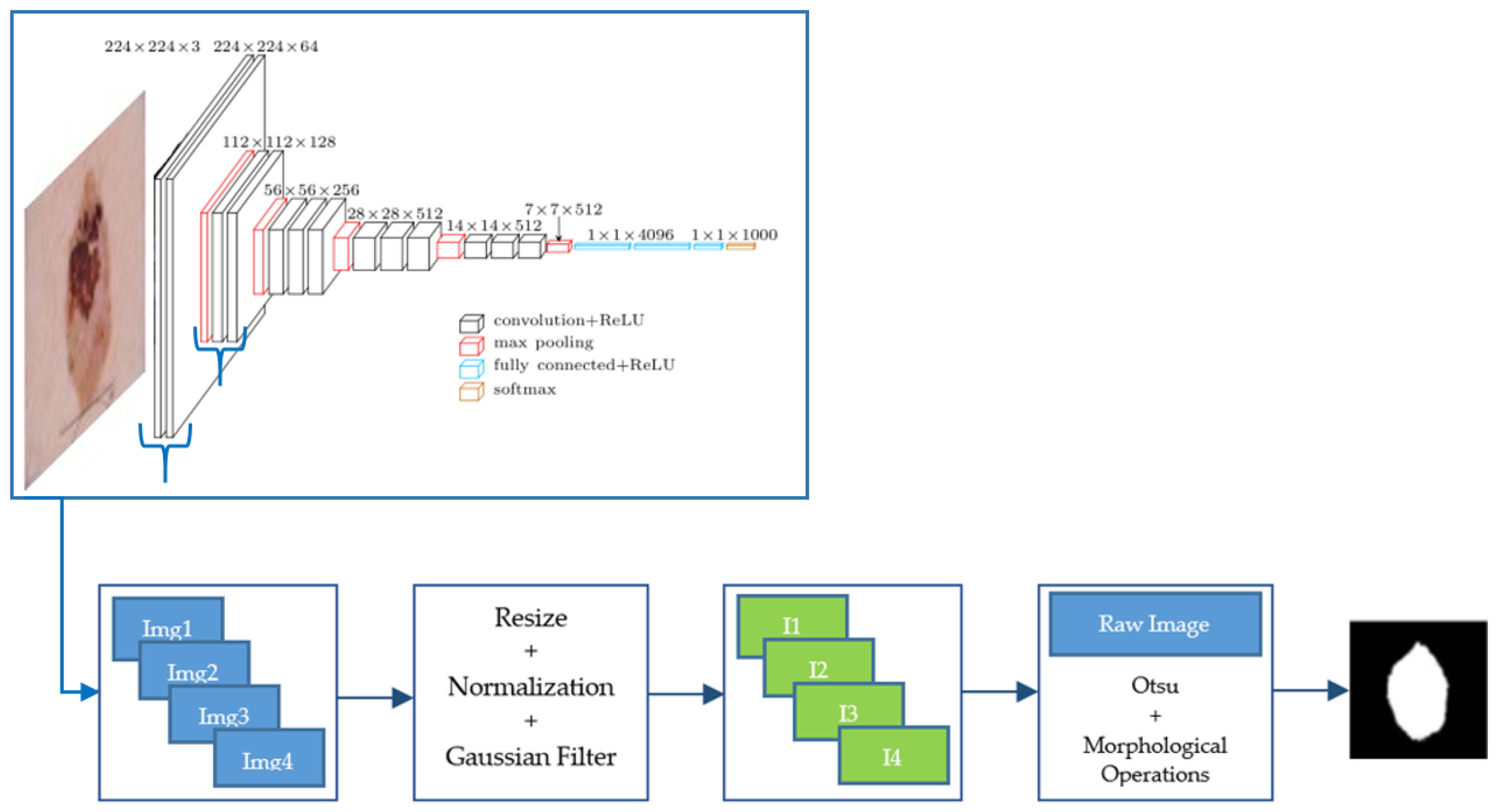
Segmentation from Feature Images of a CNN
Semantic Segmentation with SegNet Deep Neural Network
2.2. Lesion Classification
- BCC vs. Nevus;
- BCC vs. All, where the term “All” groups the following skin lesions: nevus, benign keratosis, dermatofibroma, melanoma, SCC, actinic keratosis and vascular lesion.
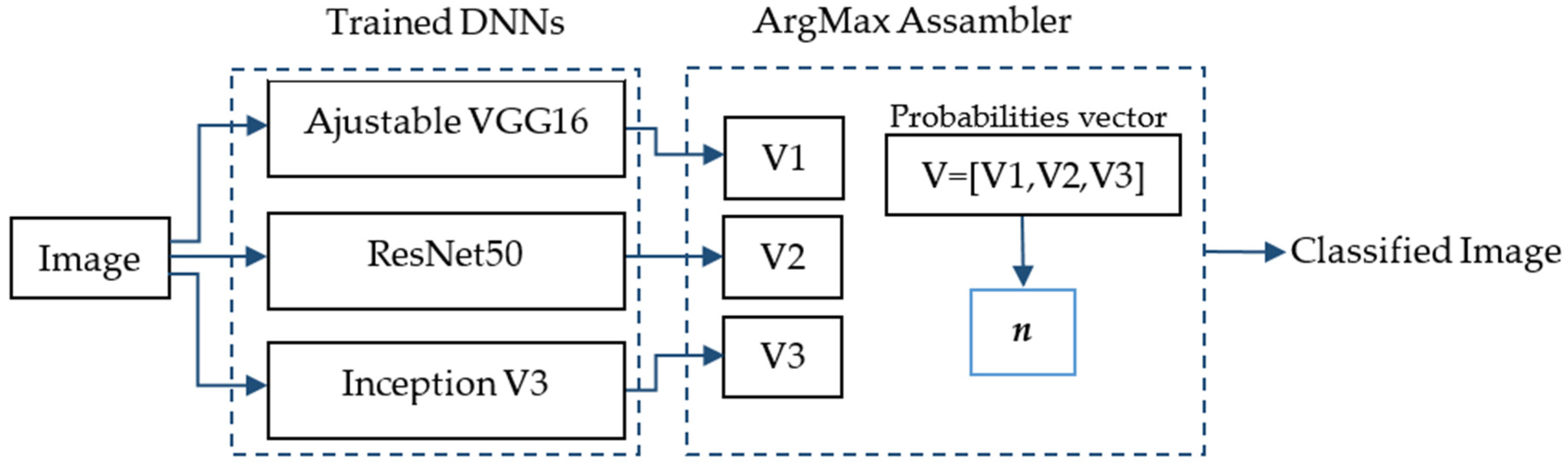
- The use of a VGG-16 neural network. VGG-16 consists of 16 convolutional layers and is very appealing because of its very uniform architecture [38].
- The use of a ResNet50 neural network. It is a convolutional neural network with 50 layers. It is a type of Residual Network and it first introduced the concept of skip connection [39].
- The use of an InceptionV3 neural network. InceptionV3 is another type of CNN developed by Google. It is 48 layers deep [40].
- The use of an ensemble of the three neural networks using the maximum argument. The ArgMax ensemble calculates, for each image, the probability of each class from each neural network, and it selects as the output class the one with highest probability among all the neural networks.
- The use of an ensemble of the three neural networks using the mean. In this case the average of the three probabilities for each class belonging to each neural network is calculated. The output class selected is the one with the maximum average value.
3. Results
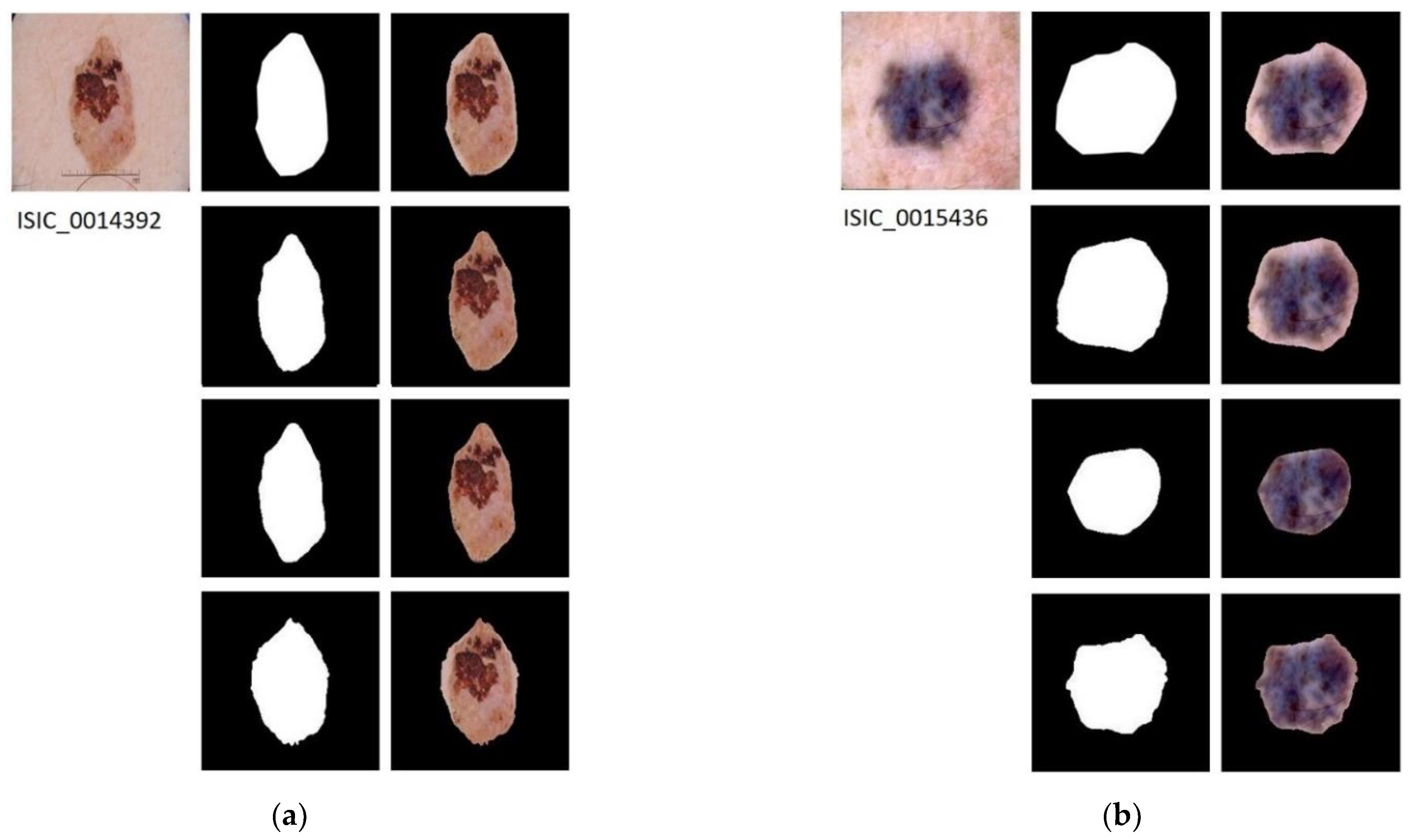
3.1. Segmentation Results
3.1.1. Database
3.1.2. Implementation Details
3.1.3. Results
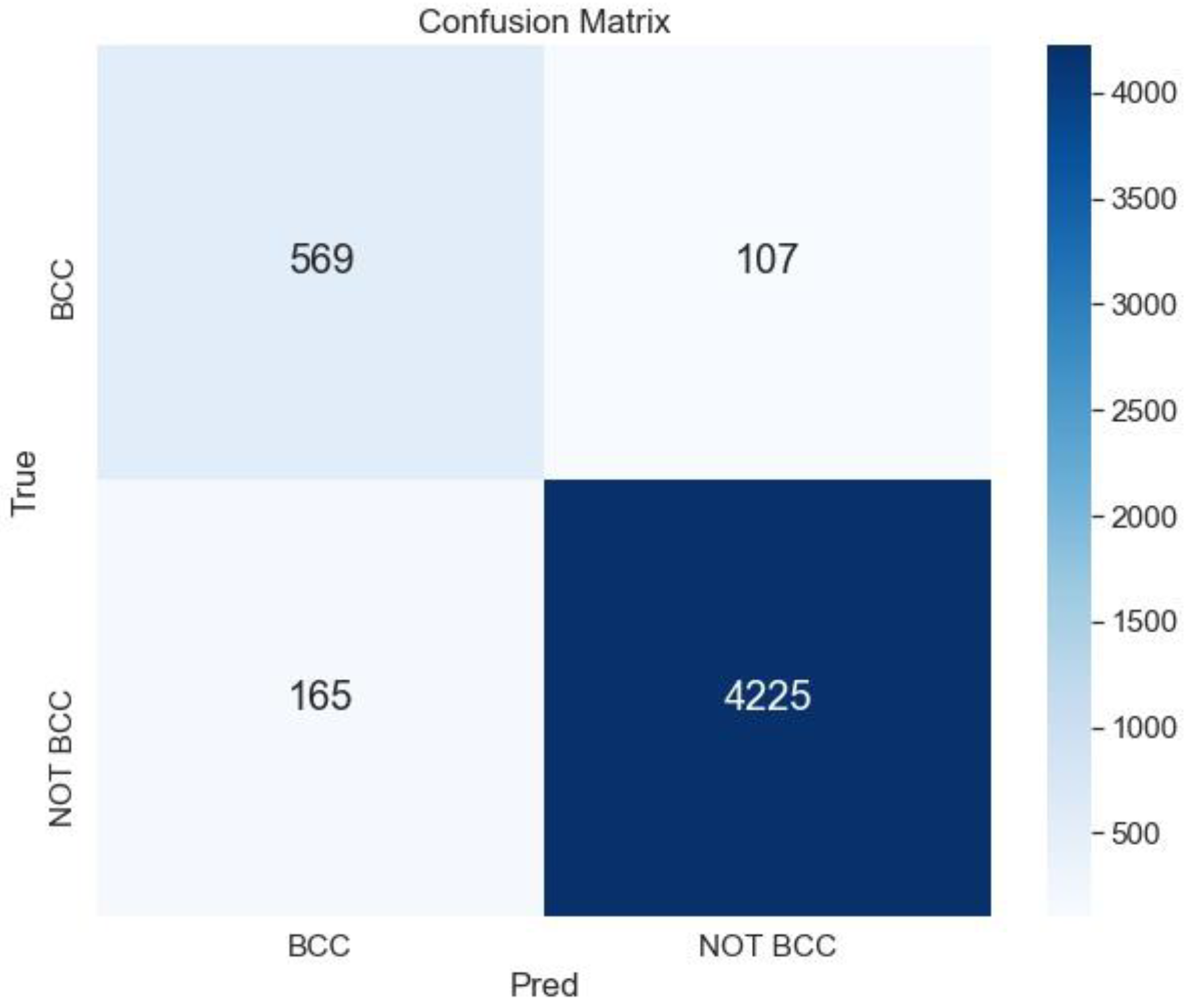
3.2. Classification Results
3.2.1. Database
3.2.2. Classification Results of BCC vs. Nevus
3.2.3. Classification Results of BCC vs. All Lesions
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviation
| Acc | Accuracy |
| AK | Actinic Keratosis |
| ANN | Artificial Neural Networks |
| AUROC | Area Under the Receiver Operating Characteristic |
| BCC | Basal Cell Carcinoma |
| BKL | Bening Keratosis |
| CAD | Computer Aid Diagnosis |
| CNN | Convolutional Neural Network |
| DF | Dermatofibroma |
| DICE | Dice Coefficient |
| DLBSM | Deep Learning-Based Segmentation Methods |
| DNN | Deep Neural Network |
| DT | Decision Trees |
| FCN | Fully Convolutional Network |
| FPR | False Positive Rate |
| ILSVRC | ImageNet Large Scale Visual Recognition Challenge |
| ISIC | International Skin Imaging Collaboration |
| JACC | Jaccard Index |
| MEL | Melanoma |
| ML | Machine Learning |
| NMSC | Non-Melanoma Skin Cancer |
| Pre | Precision |
| RAM | Random Access Memory |
| ResNet | Residual Networks |
| SCC | Squamous Cell Carcinoma |
| Se | Sensitivity |
| SegNet | Semantic Neural Network |
| SGDM | Stochastic Gradient Descent with Momentum |
| Sp | Specificity |
| SVM | Support Vector Machine |
| VASC | Vascular |
References
- Skin Cancer Foundation. Skin Cancer Facts and Statistics. Available online: https://www.skincancer.org/skin-cancer-information/skin-cancer-facts (accessed on 11 October 2021).
- Gillard, M.; Wang, T.S.; Johnson, T.M. Nonmelanoma cutaneous malignancies. In Oncology, An Evidence-Based Approach; Chang, A.E., Ganz, P.A., Hayes, D.F., Kinsella, T., Pass, H.I., Schiller, J.H., Stone, R.M., et al., Eds.; Springer: New York, NY, USA, 2006; pp. 1102–1118. [Google Scholar]
- Ciążyńska, M.; Narbutt, J.; Woźniacka, A.; Lesiak, A. Trends in basal cell carcinoma incidence rates: A 16-year retrospective study of a population in central Poland. Adv. Dermatol. Allergol. 2018, 35, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Peris, K.; Fargnoli, M.C.; Garbe, C.; Kaufman, R.; Bastholt, L.; Basset Seguin, N.; Bataille, V.; Del Marmol, V.; Dummer, R.; Harwood, C.A.; et al. Diagnosis and treatment of basal cell carcinoma: European consensus-based interdisciplinary guidelines. Eur. J. Cancer 2019, 118, 10–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breitbart, E.W.; Waldmann, A.; Nolte, S.; Capellaro, M.; Greinert, R.; Volkmer, B.; Katalinic, A. Systematic skin cancer screening in northern Germany. J. Am. Acad. Dermatol. 2012, 66, 201–211. [Google Scholar] [CrossRef] [PubMed]
- International Skin Imaging Collaboration. Available online: https://www.isic-archive.com (accessed on 26 October 2020).
- Kaymak, S.; Esmaili, P.; Serener, A. Deep Learning for Two-Step Classification of Malignant Pigmented Skin Lesions. In Proceedings of the 14th Symposium on Neural Networks and Applications (NEUREL 2018), Belgrade, Serbia, 20–21 November 2018. [Google Scholar] [CrossRef]
- Sultana, N.N.; Puhan, N.B. Recent Deep Learning Methods for Melanoma Detection: A Review. In Proceedings of the 4th International Conference Mathematics and Computing (ICMC 2018), Varanasi, India, 9–11 January 2018. [Google Scholar] [CrossRef]
- Marka, A.; Carter, J.B.; Toto, E.; Hassanpour, S. Automated detection of nonmelanoma skin cancer using digital images: A systematic review. BMC Med. Imaging 2019, 19, 21. [Google Scholar] [CrossRef]
- Wahba, M.A.; Ashour, A.S.; Napoleon, S.A.; Abd Elnaby, M.M.; Guo, Y. Combined empirical mode decomposition and texture features for skin lesion classification using quadratic support vector machine. Health Inf. Sci. Syst. 2017, 5, 10. [Google Scholar] [CrossRef]
- Wahba, M.A.; Ashour, A.S.; Guo, Y.; Napoleon, S.A.; Elnaby, M.M. A novel cumulative level difference mean based GLDM and modified ABCD features ranked using eigenvector centrality approach for four skin lesion types classification. Comput. Methods Programs Biomed. 2018, 165, 163–174. [Google Scholar] [CrossRef]
- Møllersen, K.; Kirchesch, H.; Zortea, M.; Schopf, T.R.; Hindberg, K.; Godtliebsen, F. Computer-aided decision support for melanoma detection applied on melanocytic and nonmelanocytic skin lesions: A comparison of two systems based on automatic analysis of Dermoscopic images. Biomed. Res. Int. 2015, 2015, 579282. [Google Scholar] [CrossRef] [Green Version]
- Sarkar, R.; Chatterjee, C.C.; Hazra, A. A novel approach for automatic diagnosis of skin carcinoma from dermoscopic images using parallel deep residual networks. In Proceedings of the Third International Conference on Advances in Computing and Data Sciences (ICACDS 2019), Ghaziabad, India, 12–13 April 2019. [Google Scholar] [CrossRef]
- Pangti, R.; Chouhan, V.; Mathur, J.; Kumar, S.; Dixit, A.; Gupta, S.; Mahajan, S.; Gupta, A.; Gupta, S. Performance of a deep learning-based application for the diagnosis of BCC in Indian patients as compared to dermatologists and nondermatologists. Int. J. Dermatol. 2020, 60, e51–e52. [Google Scholar] [CrossRef]
- Han, S.S.; Kim, M.S.; Lim, W.; Park, G.H.; Park, I.; Chang, S.E. Classification of the Clinical Images for Benign and Malignant Cutaneous Tumors Using a Deep Learning Algorithm. J. Investig. Dermatol. 2018, 138, 1529–1538. [Google Scholar] [CrossRef] [Green Version]
- Carcagni, P.; Leo, M.; Cuna, A.; Mazzeo, P.; Spagnolo, P.; Celeste, G.; Distante, C. Classification of Skin Lesions by Combining Multilevel Learnings in a DenseNet Architecture. In Proceedings of the 20th International Conference Image Analysis and Processing (ICIAP 2019), Trento, Italy, 9–13 September 2019. [Google Scholar] [CrossRef]
- Zhou, H.; Xie, F.; Jiang, Z.; Liu, J.; Wang, S.; Zhu, C. Multi-classification of skin diseases for dermoscopy images using deep learning. In Proceedings of the 2017 IEEE International Conference on Imaging Systems and Techniques (IST 2017), Beijing, China, 18–20 October 2017. [Google Scholar] [CrossRef]
- Sies, K.; Winkler, K.; Fink, C.; Bardehle, F.; Toberer, F.; Buhl, T.; Enk, A.; Blum, A.; Rosenberger, A.; Haenssle, H.A. Past and present of computer-assisted dermoscopic diagnosis: Performance of a conventional image analyser versus a convolutional neural network in a prospective data set of 1981 skin lesions. Eur. J. Cancer 2020, 135, 39–46. [Google Scholar] [CrossRef]
- Dorj, U.O.; Lee, K.K.; Choi, J.Y.; Lee, M. The skin cancer classification using deep convolutional neural network. Multimed. Tools Appl. 2018, 77, 9909–9924. [Google Scholar] [CrossRef]
- Cruz-Roa, A.A.; Arevalo Ovalle, J.E.; Madabhushi, A.; González Osorio, F.A. A Deep Learning Architecture for Image Representation, Visual Interpretability and Automated Basal-Cell Carcinoma Cancer Detection. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention MICCAI 2013, Nagoya, Japan, 22–26 September 2013. [Google Scholar] [CrossRef]
- Campanella, G.; Navarrete-Dechent, C.; Liopyris, K.; Monnier, J.; Aleissa, S.; Minhas, B.; Scope, A.; Longo, C.; Guitera, P.; Pellacani, G.; et al. Deep Learning for Basal Cell Carcinoma Detection for Reflectance Confocal Microscopy. J. Investig. Dermatol. 2022, 142, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Kimeswenger, S.; Tschandl, P.; Noack, P.; Hofmarcher, M.; Rumetshofer, E.; Kindermann, H.; Silye, R.; Hochreiter, S.; Kaltenbrunner, M.; Guenova, E.; et al. Artificial neural networks and pathologists recognize basal cell carcinomas based on different histological patterns. Mod. Pathol. 2011, 34, 895–903. [Google Scholar] [CrossRef] [PubMed]
- Pérez Malla, C.U.; Valdés Hernández, M.D.C.; Rachmadi, M.F.; Komura, T. Evaluation of enhanced learning techniques for segmenting ischaemic stroke lesions in brain magnetic resonance perfusion images using a convolutional neural network scheme. Front. Neuroinformatics 2019, 13. [Google Scholar] [CrossRef] [Green Version]
- Kaur, D.; Kaur, Y. Various image segmentation techniques: A review. Int. J. Comput. Sci. Mob. Comput. 2014, 3, 809–814. [Google Scholar] [CrossRef]
- Sreelatha, T.; Subramanyam, M.V.; Giri Prasad, M.N. Early Detection of Skin Cancer Using Melanoma Segmentation technique. J. Med. Syst. 2019, 43, 190. [Google Scholar] [CrossRef] [PubMed]
- Bi, L.; Jinman, K.; Ahn, E.; Kumar, A.; Feng, D.; Fulham, M. Step-wise integration of deep class-specific learning for dermoscopic image segmentation. Pattern Recognit. 2019, 85, 78–89. [Google Scholar] [CrossRef] [Green Version]
- Tang, P.; Liang, Q.; Yan, X.; Xiang, S.; Sun, W.; Zhang, D.; Coppola, G. Efficient skin lesion segmentation using separable-Unet with stochastic weight averaging. Comput. Methods Programs Biomed. 2019, 178, 289–301. [Google Scholar] [CrossRef]
- Codella, N.C.F.; Gutman, D.; Celebi, M.E.; Helba, B.; Marchetti, M.A.; Dusza, S.W.; Kalloo, A.; Liopyris, K.; Mishra, N.; Kittler, H.; et al. Skin lesion analysis toward melanoma detection. A challenge at the 2017 International symposium on biomedical imaging (ISBI), hosted by the international skin imaging collaboration (ISIC). In Proceedings of the IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018. [Google Scholar] [CrossRef] [Green Version]
- Punithakumar, K.; Yuan, J. A convex max-flow approach to distribution-based figure-ground separation. SIAM J. Imaging Sci. 2012, 5, 1333–1354. [Google Scholar] [CrossRef] [Green Version]
- Qiu, W.; Yuan, J.; Ukwatta, E.; Sun, Y.; Rajchl, M.; Fenster, A. Prostate segmentation: An efficient convex optimization approach with axial symmetry using 3-D TRUS and MR images. IEEE Trans. Med. Imaging 2014, 33, 947–960. [Google Scholar] [CrossRef]
- Pérez-Carrasco, J.A.; Acha, B.; Suárez-Mejías, C.; López-Guerra, J.L.; Serrano, C. Joint segmentation of bones and muscles using an intensity and histogram-based energy minimization approach. Comput. Methods Programs Biomed. 2018, 156, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Mejías, C.; Pérez-Carrasco, J.A.; Serrano, C.; López-Guerra, J.L.; Parra-Calderón, C.; Gómez-Cía, T.; Acha, B. Three-dimensional segmentation of retroperitoneal masses using continuous convex relaxation and accumulated gradient distance for radiotherapy planning. Med. Biol. Eng. Comput. 2017, 55, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Papadakis, N.; Rabin, J. Convex histogram-based joint image segmentation with regularized optimal transport cost. J. Math. Imaging Vis. 2017, 59, 161–186. [Google Scholar] [CrossRef] [Green Version]
- Al-masni, M.A.; Al-antari, M.A.; Choi, M.T.; Han, S.M.; Kim, T.S. Skin lesion segmentation in dermoscopy images via deep full resolution convolutional networks. Comput. Methods Programs Biomed. 2018, 162, 221–231. [Google Scholar] [CrossRef]
- Yu, L.; Chen, H.; Dou, Q.; Qin, J.; Heng, P. Automated melanoma recognition in dermoscopy images via very deep residual networks. IEEE Trans. Med. Imaging 2017, 36, 994–1004. [Google Scholar] [CrossRef]
- Kwasigroch, A.; Mikolajczyk, A.; Grochowski, M. Deep convolutional neural networks as a decision support tool in medical problems–malignant melanoma case study. In Proceedings of the 19th Polish Control Conference (KKA 2014), Kraków, Poland, 12–21 June 2017. [Google Scholar] [CrossRef]
- Badrinarayanan, V.; Kendall, A.; Cipolla, R. SegNet: A Deep Convolutional Encoder-Decoder Architecture for Image Segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 2481–2495. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. In Proceedings of the 3rd International Conference on Learning Representations (ICLR 2015), San Diego, CA, USA, 7–9 May 2015. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR 2016), Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar] [CrossRef] [Green Version]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J. Rethinking the Inception Architecture for Computer Vision. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR 2016), Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar] [CrossRef] [Green Version]
- Yuan, Y.; Chao, M.; Lo, Y.-C. Automatic skin lesion segmentation with fully convolutional deconvolutional networks. IEEE J. Biomed. Health Inform. 2018, 36, 1876–1886. [Google Scholar] [CrossRef] [Green Version]
- Tschandl, P.; Sinz, C.; Kittler, H. Domain-specific classification pre-trained fully convolutional network encoders for skin lesion segmentation. Comput. Biol. Med. 2019, 104, 111–116. [Google Scholar] [CrossRef]
- Sarker, M.K.; Rashwan, H.A.; Akram, F.; Singh, V.K.; Banu, S.F.; Chowdhury, F.U.H.; Choudhury, K.A.; Chambon, S.; Radeva, P.; Puig, D.; et al. SLSNet: Skin lesion segmentation using a lightweight generative adversarial network. Expert Syst. Appl. 2021, 183, 115433. [Google Scholar] [CrossRef]
- Tschandl, P.; Rosendahl, C.; Kittler, H. The HAM10000 dataset, a large collection of multi-source dermatoscopic images of common pigmented skin lesions. Sci. Data 2018, 5, 180161. [Google Scholar] [CrossRef]
- Combalia, M.; Codella, N.F.C.; Rotemberg, V.; Helba, B.; Vilaplana, V.; Reiter, O.; Halpern, A.C.; Puig, S.; Malvehy, J. BCN20000: Dermoscopic Lesions in the Wild. arXiv 2019, arXiv:1908.02288. [Google Scholar]
- Gessert, N.; Nielsen, M.; Shaikh, M.; Werner, R.; Schlaefer, A. Skin lesion classification using ensembles of multi-resolution EfficientNets with meta data. MethodsX 2020, 7, 100864. [Google Scholar] [CrossRef] [PubMed]
- Barata, C.; Celebi, M.E.; Marques, J.S. A survey of feature extraction in dermoscopy image analysis of skin cancer. IEEE J. Biomed. Health Inform. 2019, 23, 1096–1109. [Google Scholar] [CrossRef]
- Teixeira, L.O.; Pereira, R.M.; Bertolini, D.; Oliveira, L.S.; Nanni, L.; Cavalcanti, G.D.C.; Costa, M.G. Impact of lung segmentation on the diagnosis and explanation of COVID-19 in chest X-ray images. Sensors 2021, 21, 7116. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Methodology | DICE | JACC | Se | Sp | ACC |
|---|---|---|---|---|---|
| SegNet | 0.8548 | 0.7730 | 0.8533 | 0.9632 | 0.9357 |
| Energy minimization | 0.5937 | 0.4927 | 0.6020 | 0.9131 | 0.8647 |
| Feature images from VGG16 | 0.5853 | 0.4700 | 0.8627 | 0.8690 | 0.8170 |
| Ref. | Methodology | DICE | JACC | Se | Sp | ACC |
|---|---|---|---|---|---|---|
| [41] | FCDN- First Place at Challenge ISBI-2017 | 0.8490 | 0.7650 | 0.8250 | 0.9750 | 0.9340 |
| [27] | Separable-UNet model with stochastic weight averaging scheme | 0.8693 | 0.7926 | 0.8953 | 0.9632 | 0.9431 |
| [42] | LinkNet152 model | 0.8530 | 0.7700 | − | − | − |
| [43] | GAN-based model | 0.9063 | 0.8198 | 0.8781 | 0.9992 | 0.9761 |
| [26] | Deep class-specific learning | 0.8566 | 0.7773 | 0.8620 | 0.9671 | 0.9408 |
| SegNet | 0.8548 | 0.7730 | 0.8533 | 0.9632 | 0.9357 |
| Method | Se | Sp | Pre | FPR | Acc |
|---|---|---|---|---|---|
| VGG16 | 0.95 | 0.97 | 0.88 | 0.99 | 0.97 |
| ResNet50 | 0.95 | 0.97 | 0.88 | 0.99 | 0.96 |
| InceptionV3 | 0.95 | 0.97 | 0.87 | 0.96 | 0.94 |
| Ensemble ArgMax | 0.97 | 0.98 | 0.92 | 0.99 | 0.98 |
| Ensemble Mean | 0.97 | 0.97 | 0.90 | 0.99 | 0.97 |
| Method | Se | Sp | Pre | FPR | Acc |
|---|---|---|---|---|---|
| VGG16 | 0.87 | 0.97 | 0.87 | 0.97 | 0.95 |
| ResNet50 | 0.88 | 0.96 | 0.86 | 0.97 | 0.95 |
| InceptionV3 | 0.85 | 0.97 | 0.87 | 0.96 | 0.94 |
| Ensemble ArgMax | 0.90 | 0.97 | 0.88 | 0.97 | 0.95 |
| Ensemble Mean | 0.89 | 0.97 | 0.88 | 0.97 | 0.95 |
| Method | Se | Sp | Pre | FPR | Acc |
|---|---|---|---|---|---|
| VGG16 | 0.84 | 0.96 | 0.75 | 0.97 | 0.94 |
| ResNet50 | 0.81 | 0.95 | 0.72 | 0.97 | 0.93 |
| InceptionV3 | 0.78 | 0.95 | 0.70 | 0.97 | 0.93 |
| Ensemble ArgMax | 0.84 | 0.96 | 0.78 | 0.98 | 0.95 |
| Ensemble Mean | 0.83 | 0.96 | 0.78 | 0.97 | 0.95 |
| Method | Se | Sp | Pre | FPR | Acc |
|---|---|---|---|---|---|
| VGG16 | 0.68 | 0.96 | 0.74 | 0.95 | 0.94 |
| ResNet50 | 0.65 | 0.96 | 0.70 | 0.95 | 0.93 |
| InceptionV3 | 0.60 | 0.96 | 0.67 | 0.94 | 0.93 |
| Ensemble ArgMax | 0.68 | 0.97 | 0.77 | 0.95 | 0.95 |
| Ensemble Mean | 0.68 | 0.97 | 0.78 | 0.95 | 0.95 |
| Winner Challenge 2019 [46] | Proposed Method | ||||
|---|---|---|---|---|---|
| Se | Sp | Se | Sp | Acc | |
| AK | 0.48 | 0.97 | 0.48 | 1.00 | 0.96 |
| BCC | 0.72 | 0.94 | 0.83 | 0.98 | 0.96 |
| BKL | 0.39 | 0.99 | 0.50 | 0.99 | 0.94 |
| DF | 0.58 | 0.98 | 0.48 | 1.00 | 0.99 |
| MEL | 0.59 | 0.96 | 0.61 | 0.97 | 0.91 |
| NEVUS | 0.71 | 0.98 | 0.97 | 0.71 | 0.84 |
| SCC | 0.44 | 0.99 | 0.43 | 1.00 | 0.98 |
| VASC | 0.64 | 0.99 | 0.79 | 1.00 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vélez, P.; Miranda, M.; Serrano, C.; Acha, B. Does a Previous Segmentation Improve the Automatic Detection of Basal Cell Carcinoma Using Deep Neural Networks? Appl. Sci. 2022, 12, 2092. https://doi.org/10.3390/app12042092
Vélez P, Miranda M, Serrano C, Acha B. Does a Previous Segmentation Improve the Automatic Detection of Basal Cell Carcinoma Using Deep Neural Networks? Applied Sciences. 2022; 12(4):2092. https://doi.org/10.3390/app12042092
Chicago/Turabian StyleVélez, Paulina, Manuel Miranda, Carmen Serrano, and Begoña Acha. 2022. "Does a Previous Segmentation Improve the Automatic Detection of Basal Cell Carcinoma Using Deep Neural Networks?" Applied Sciences 12, no. 4: 2092. https://doi.org/10.3390/app12042092
APA StyleVélez, P., Miranda, M., Serrano, C., & Acha, B. (2022). Does a Previous Segmentation Improve the Automatic Detection of Basal Cell Carcinoma Using Deep Neural Networks? Applied Sciences, 12(4), 2092. https://doi.org/10.3390/app12042092