
Digital Photoelastic Analysis of TAD-Supported Maxillary Arch Distalization



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
Featured Application
Abstract
1. Introduction
2. Materials and Methods
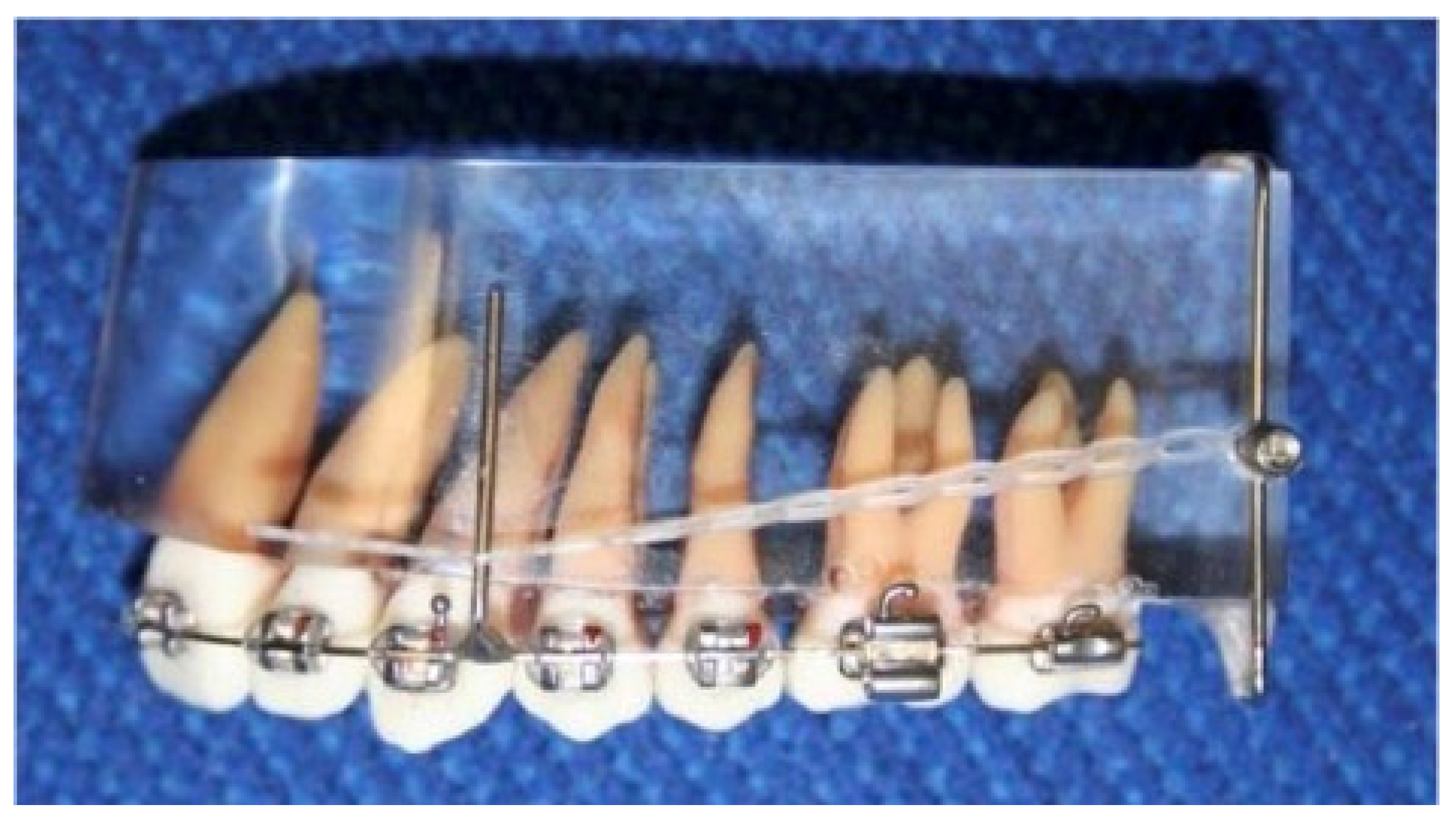
2.1. Photoelastic Model
2.2. Measurement System
2.3. Measurement Categories
2.3.1. Stress Distribution and Strength
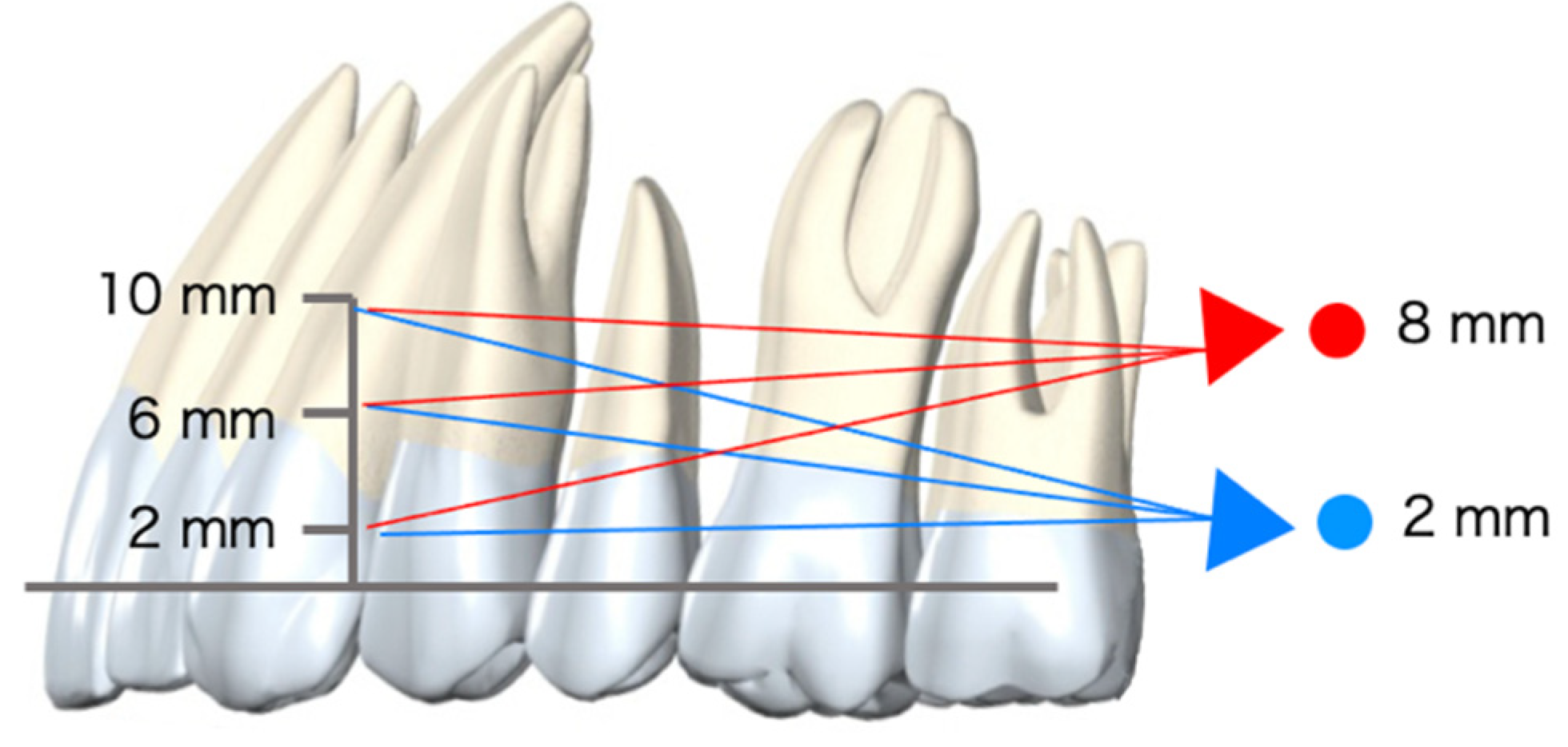
2.3.2. Stress Direction
3. Results
3.1. Stress Distribution and Strength (by Combinations)
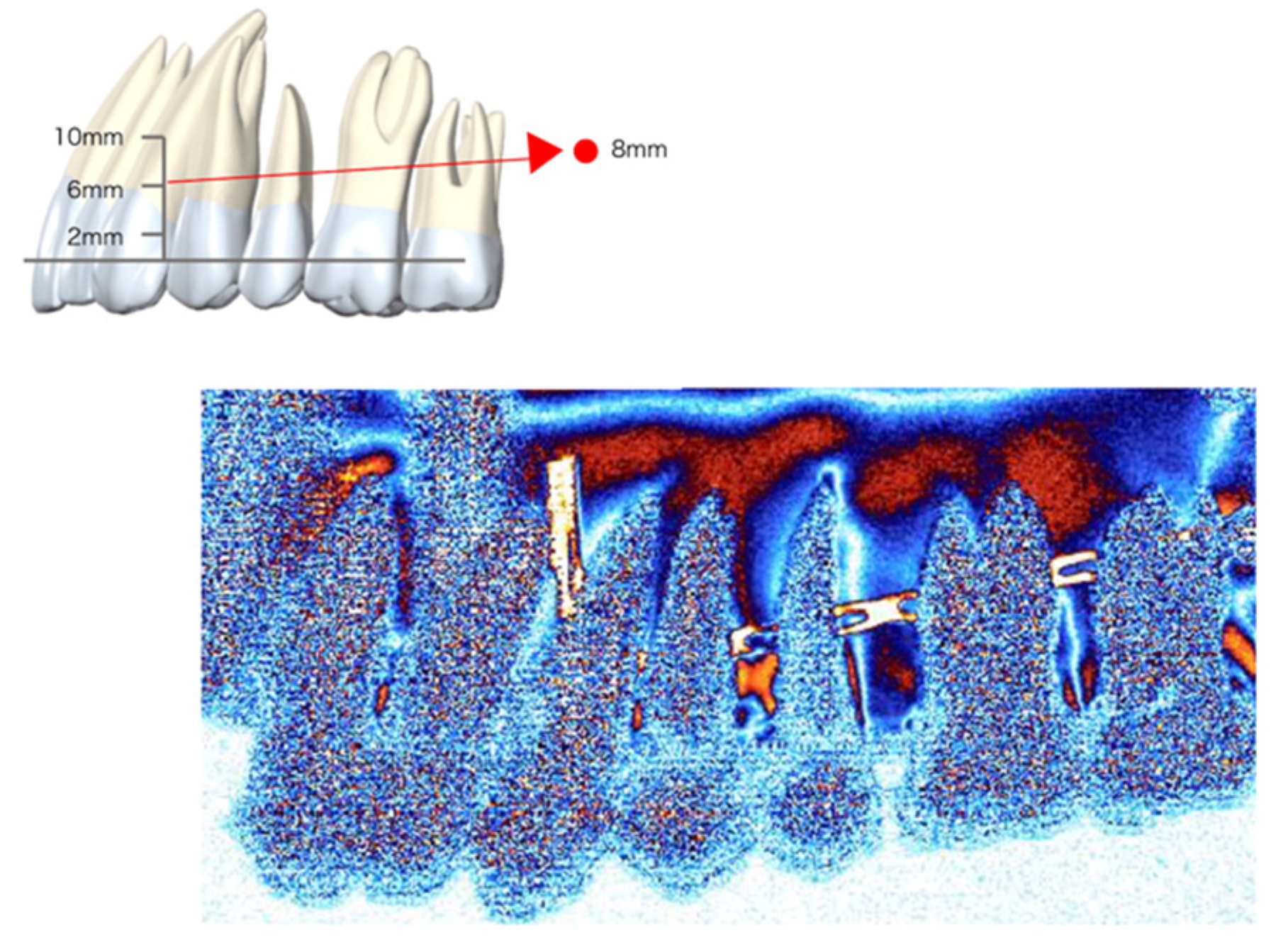
3.1.1. Two-Millimeter Anchor Model
- Two-millimeter-long retraction hook (Figure 5)
- Apical region: Compressive stress was detected around the root apex of the overall dentition. However, tensile stress was observed at the apex of the incisor;
- Center region: Compressive stress was observed in the cervical area of the distal root surface from the lateral incisor to the molars;
- Cervical region: Tensile stress was observed in the cervical third of the mesial root surface of the second premolars.
- Six-millimeter-long retraction hook (Figure 6)
- (a)
- Apical region: Similar tendencies to the 2 mm retraction hook were observed.
- (b)
- Center region
- (c)
- Cervical region
- Ten-millimeter-long retraction hook (Figure 7)
- (a)
- Apical region
- (b)
- Center region
- (c)
- Cervical region
3.1.2. Eight-Millimeter Anchor Model
- Two-millimeter-long retraction hook (Figure 8)
- (a)
- Apical region
- (b)
- Center region
- (c)
- Cervical region
- Six-millimeter-long retraction hook (Figure 9)
- (a)
- Apical region
- (b)
- Center region
- (c)
- Cervical region
- Ten-millimeter-long retraction hook (Figure 10)
- (a)
- Apical region
- (b)
- Center region
- (c)
- Cervical region
3.2. Stress Direction
4. Discussion
4.1. Overall Findings in the Context of the Experiment and Interpretation
4.2. Biomechanics of Dentition
4.3. Digital Photoelastic Method
4.4. Clinical Implications
- TAD positioned to retract from the cervical region
- 2.
- TAD positioned to retract from the apex
5. Conclusions
- Upward stress in molars and distal stress at the cervical region in the whole dentition were applied with a short hook regardless of the TAD position. This means that molar intrusion or posterior-superior occlusal plane rotation will occur.
- Downward stress in molars and distal stress at the apical third of the canine were applied with the TAD in the cervical position, especially with a long hook. This means that molar extrusion or posterior-inferior occlusal plane rotation will occur.
- Relatively uniform compressive stress was detected in the cervical position of TAD with a medium hook and apical position of TAD with a long hook. This means that the maxillary arch will be distalized parallelly to the occlusal plane.
- The digital photoelastic analysis method has great potential for evaluating orthodontic biomechanics.
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ghosh, J.N.R. Evaluation of an intraoral maxillary molar distalization technique. Am. J. Orthod. Dentofac. Orthop. 1996, 110, 639–946. [Google Scholar] [CrossRef]
- Kinzinger, G.S.M.; Eren, M.; Diedrich, P.R. Treatment effects of intraoral appliances with conventional anchorage designs for non-compliance maxillary molar distalization. A literature review. Eur. J. Orthod. 2008, 30, 558–571. [Google Scholar] [CrossRef] [PubMed]
- Antonarakis, G.S.; Kiliaridis, S. Maxillary molar distalization with noncompliance intramaxillary appliances in class II malocclusion: A systematic review. Angle Orthod. 2008, 78, 1133–1140. [Google Scholar] [CrossRef] [PubMed]
- Jambi, S.; Thiruvenkatachari, B.; O’Brien, K.D.; Walsh, T. Orthodontic treatment for distalising upper first molars in children and adolescents. Cochrane Database Syst. Rev. 2013, 2013, CD008375. [Google Scholar] [CrossRef]
- Al-Thomali, Y.; Basha, S.; Mohamed, R.N. Pendulum and modified pendulum appliances for maxillary molar distalization in Class II malocclusion—A systematic review. Acta Odontol. Scand. 2017, 75, 394–401. Available online: https://www.tandfonline.com/doi/full/10.1080/00016357.2017.1324636 (accessed on 15 December 2021). [CrossRef]
- Sugawara, J.; Kanzaki, R.; Takahashi, I.; Nagasaka, H.; Nanda, R. Distal movement of maxillary molars in nongrowing patients with the skeletal anchorage system. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 723–733. [Google Scholar] [CrossRef]
- Cornelis, M.A.; De Clerck, H.J. Maxillary molar distalization with miniplates assessed on digital models: A prospective clinical trial. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 373–377. [Google Scholar] [CrossRef]
- Papadopoulos, M.A.; Tarawneh, F. The use of miniscrew implants for temporary skeletal anchorage in orthodontics: A comprehensive review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 103, 6–15. [Google Scholar] [CrossRef]
- Fudalej, P.; Antoszewska, J. Are orthodontic distalizers reinforced with the temporary skeletal anchorage devices effective? Am. J. Orthod. Dentofac. Orthop. 2011, 139, 722–729. [Google Scholar] [CrossRef]
- Konno, M.; Uechi, J.; Tsuji, Y.; Shibata, T.; Mizoguchi, I. Three-dimensional Morphological Analysis of Dental Compensation in Facial Asymmetry Cases. Jpn. J. Jaw Deform 2014, 24, 37–45. Available online: http://jlc.jst.go.jp/DN/JST.JSTAGE/jjjd/24.37?lang=en&from=CrossRef&type=abstract (accessed on 15 December 2021). [CrossRef][Green Version]
- Ook, Y.-A.; Bayome, M.; Trang, V.T.T.; Kim, H.-J.; Park, J.H.; Kim, K.B.; Behrents, R.G. Treatment effects of a modified palatal anchorage plate for distalization evaluated with cone-beam computed tomography. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 47–54. [Google Scholar] [CrossRef]
- Roberts, W.E.; Viecilli, R.F.; Chang, C.; Katona, T.R.; Paydar, N.H. Biology of biomechanics: Finite element analysis of a statically determinate system to rotate the occlusal plane for correction of a skeletal Class III open-bite malocclusion. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 943–955. [Google Scholar] [CrossRef] [PubMed]
- Duran, G.S.; Görgülü, S.; Dindaroğlu, F. Three-dimensional analysis of tooth movements after palatal miniscrew-supported molar distalization. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Kawanabe, N.; Kataoka, T.; Murakami, T.; Yamashiro, T.; Kamioka, H. Comparative evaluation of treatment outcomes between temporary anchorage devices and Class III elastics in Class III malocclusions. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 1116–1124. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, A.; Teratani, T.; Itoh, H.; Sugawara, J.; Ishikawa, H. Photoelastic stress analysis of mandibular molars moved distally with the skeletal anchorage system. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 624–629. [Google Scholar] [CrossRef]
- Kojima, Y.; Kawamura, J.; Fukui, H. Finite element analysis of the effect of force directions on tooth movement in extraction space closure with miniscrew sliding mechanics. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 501–508. [Google Scholar] [CrossRef]
- Carvalho, L.; Roriz, P.; Simões, J.; Frazão, O. New Trends in Dental Biomechanics with Photonics Technologies. Appl. Sci. 2015, 5, 1350–1378. [Google Scholar] [CrossRef]
- Knop, L.; Gandini Jr, L.G.; Shintcovsk, R.L.; Gandini, M.R.E.A.S. Scientific use of the finite element method in Orthodontics. Dent. Press J. Orthod. 2015, 20, 119–125. Available online: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S2176-94512015000200119&lng=en&tlng=en (accessed on 15 December 2021). [CrossRef]
- Sakurai, Y.; Nishii, Y.; Kodaka, K.; Nojima, K.; Sueishi, K. Crown angulation measured by laser scanner. Orthod. Waves 2010, 69, 13–17. [Google Scholar] [CrossRef]
- Kodaka, K.; Nishii, Y.; Sakurai, Y.; Nojima, K.; Sueishi, K. Crown inclination measured by laser scanner. Orthod. Waves 2010, 69, 8–12. [Google Scholar] [CrossRef]
- Sugawara, J.; Daimaruya, T.; Umemori, M.; Nagasaka, H.; Takahashi, I.; Kawamura, H.; Mitani, H. Distal movement of mandibular molars in adult patients with the skeletal anchorage system. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Alsamak, S.; Gkantidis, N.; Bitsanis, E.; Christou, P. Assessment of Potential Orthodontic Mini-implant Insertion Sites Based on Anatomical Hard Tissue Parameters: A Systematic Review. Int. J. Oral Maxillofac. Implants 2012, 27, 875–887. [Google Scholar] [PubMed]
- Alsamak, S.; Psomiadis, S.; Gkantidis, N. Positional Guidelines for Orthodontic Mini-implant Placement in the Anterior Alveolar Region: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2013, 28, 470–479. Available online: http://www.quintpub.com/journals/omi/abstract.php?iss2_id=1108&article_id=13009&article=25&title=Positional Guidelines for Orthodontic Mini-implant Placement in the Anterior Alveolar Region: A Systematic Review (accessed on 15 December 2021). [CrossRef] [PubMed]
- Hamanaka, R.; Yamaoka, S.; Anh, T.N.; Tominaga, J.-Y.; Koga, Y.; Yoshida, N. Numeric simulation model for long-term orthodontic tooth movement with contact boundary conditions using the finite element method. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 601–612. [Google Scholar] [CrossRef]
- Alrbata, R.H.; Yu, W.; Kyung, H.-M. Biomechanical effectiveness of cortical bone thickness on orthodontic microimplant stability: An evaluation based on the load share between cortical and cancellous bone. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 175–182. [Google Scholar] [CrossRef]
- Tominaga, J.-Y.; Ozaki, H.; Chiang, P.-C.; Sumi, M.; Tanaka, M.; Koga, Y.; Bourauel, C.; Yoshida, N. Effect of bracket slot and archwire dimensions on anterior tooth movement during space closure in sliding mechanics: A 3-dimensional finite element study. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 166–174. [Google Scholar] [CrossRef]
- Pinit, P.; Umezaki, E. Full-Field Determination of Principal-Stress Directions Using Photoelasticity with Plane-Polarized RGB Lights. Opt. Rev. 2005, 12, 228–232. [Google Scholar] [CrossRef]
- Umezaki, E. Stress Distribution Measurement Techniques Using Photoelasticity: Current Status and Future Prospects. J. Jpn. Soc. Precis. Eng. 2013, 79, 607–611. [Google Scholar] [CrossRef][Green Version]
- Ueda, H.M.; Miyamoto, K.; Ishizuka, Y.; Tanne, K. Masticatory muscle activity in children and adults with different facial types. Am. J. Orthod. Dentofac. Orthop. 2000, 118, 63–68. [Google Scholar] [CrossRef]













Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishii, Y.; Sameshima, G.T.; Tachiki, C. Digital Photoelastic Analysis of TAD-Supported Maxillary Arch Distalization. Appl. Sci. 2022, 12, 1949. https://doi.org/10.3390/app12041949
Nishii Y, Sameshima GT, Tachiki C. Digital Photoelastic Analysis of TAD-Supported Maxillary Arch Distalization. Applied Sciences. 2022; 12(4):1949. https://doi.org/10.3390/app12041949
Chicago/Turabian StyleNishii, Yasushi, Glenn T. Sameshima, and Chie Tachiki. 2022. "Digital Photoelastic Analysis of TAD-Supported Maxillary Arch Distalization" Applied Sciences 12, no. 4: 1949. https://doi.org/10.3390/app12041949
APA StyleNishii, Y., Sameshima, G. T., & Tachiki, C. (2022). Digital Photoelastic Analysis of TAD-Supported Maxillary Arch Distalization. Applied Sciences, 12(4), 1949. https://doi.org/10.3390/app12041949