
A Blockchain-Applied Personal Health Record Application: Development and User Experience


Abstract
:1. Introduction
2. Materials and Methods
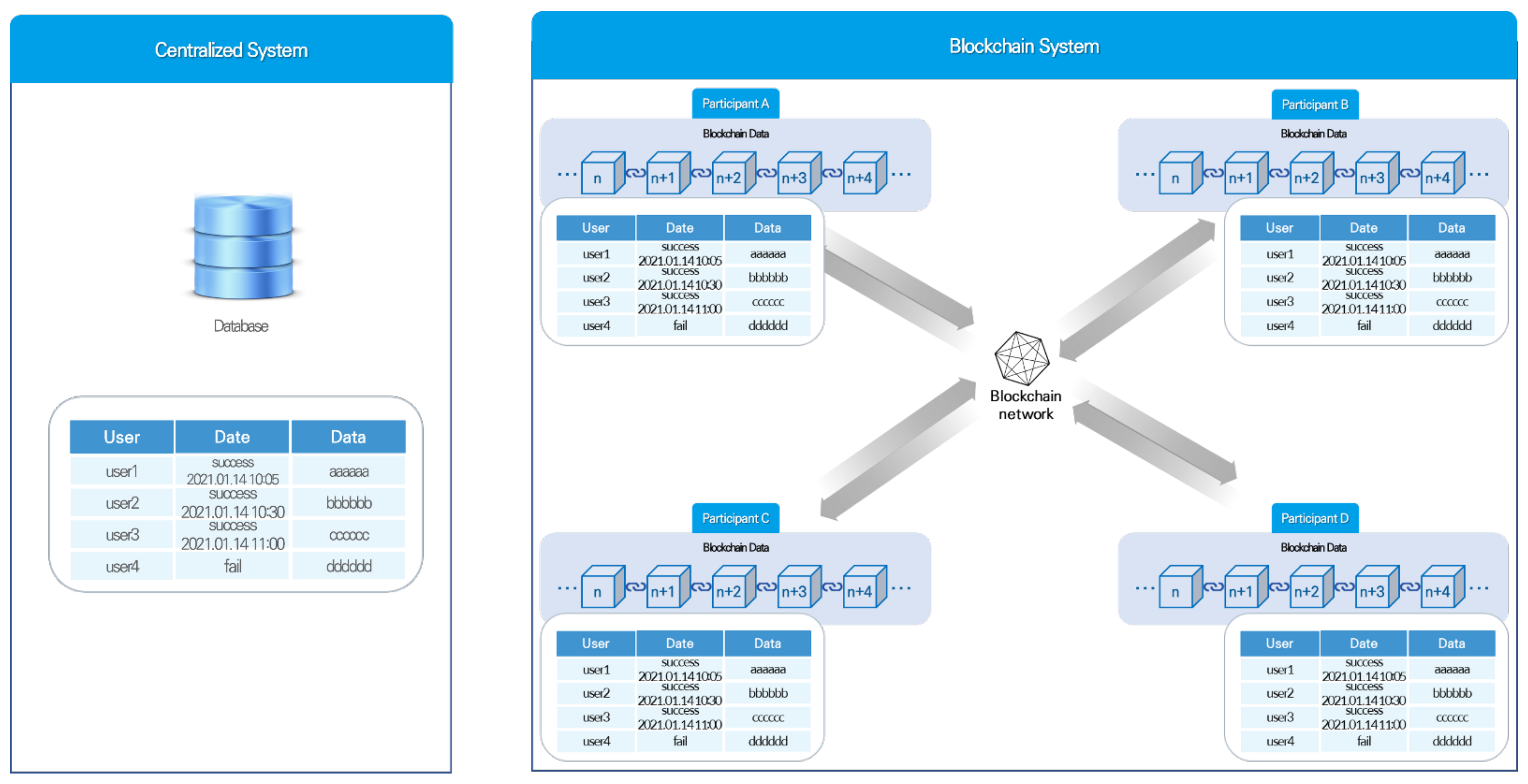
2.1. Blockchain Technology
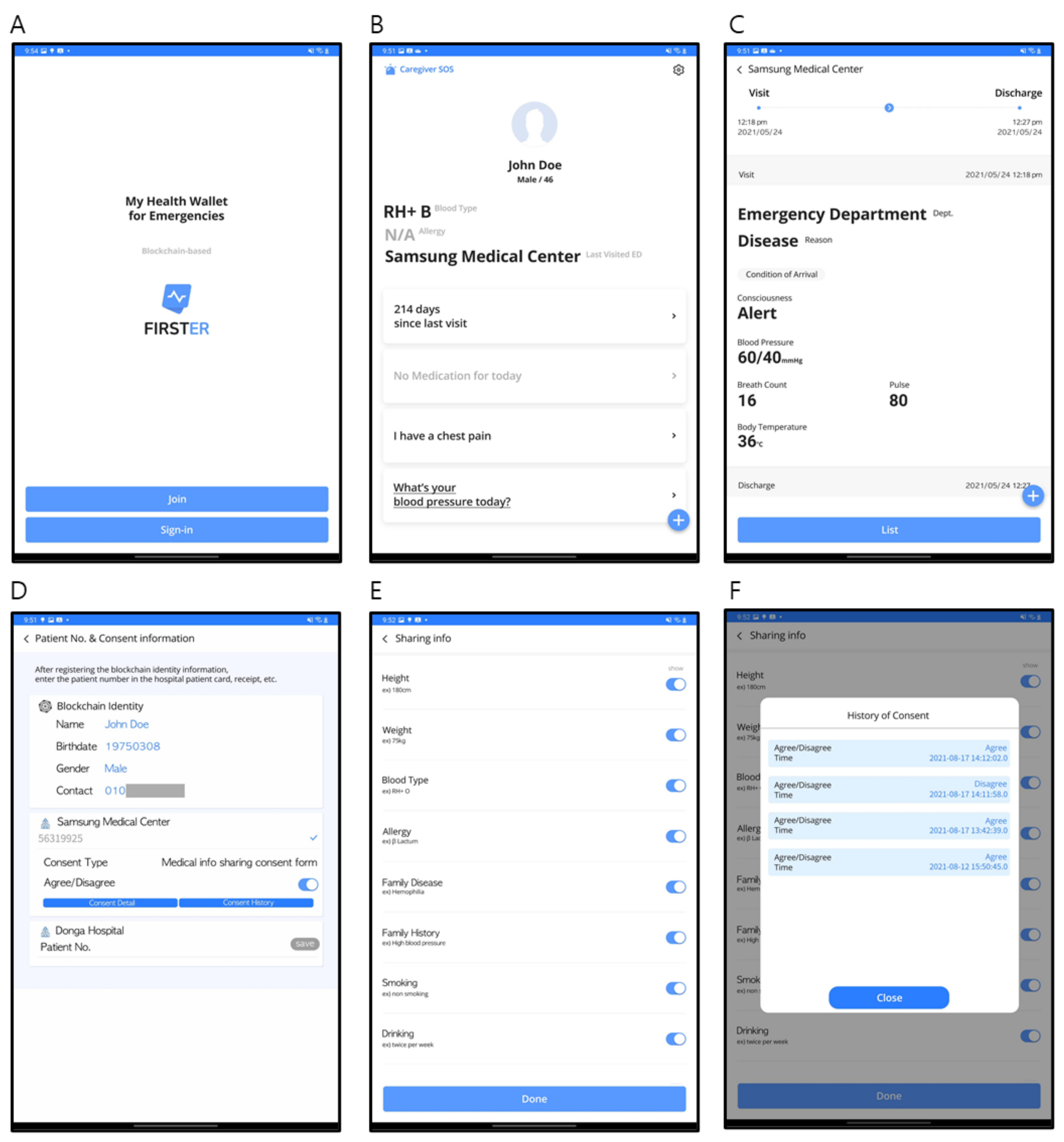
2.2. Structure of the Blockchain-Applied PHR
2.2.1. Main Function
2.2.2. Data Provided by Blockchain-Applied PHR
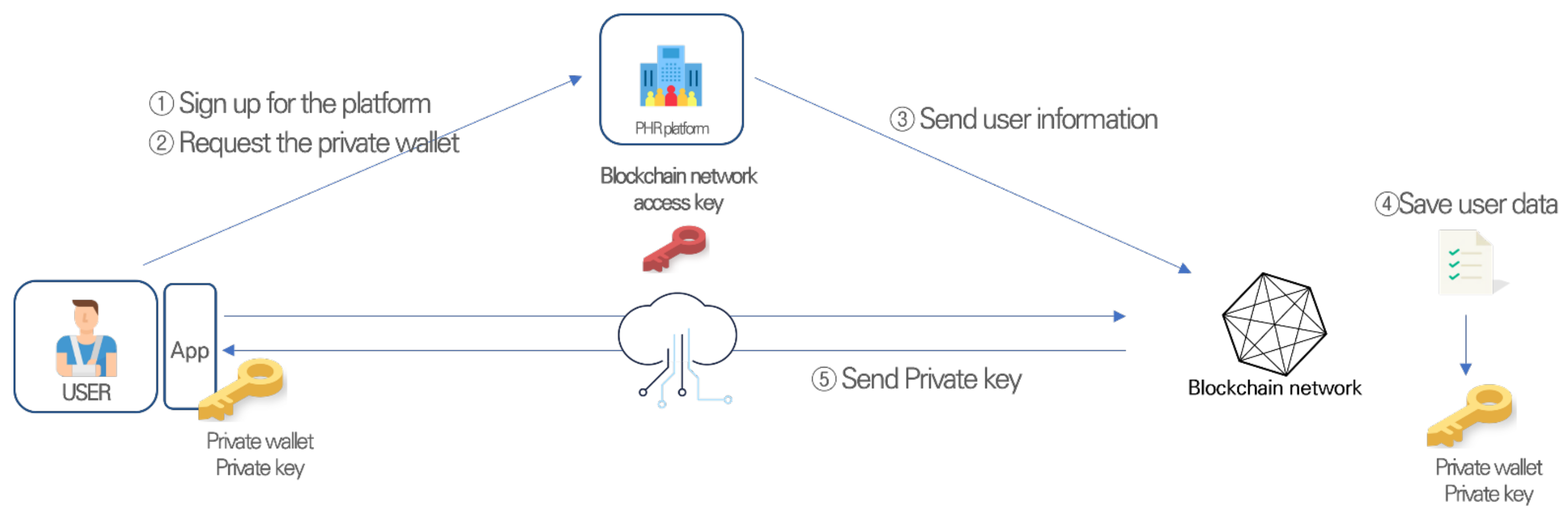
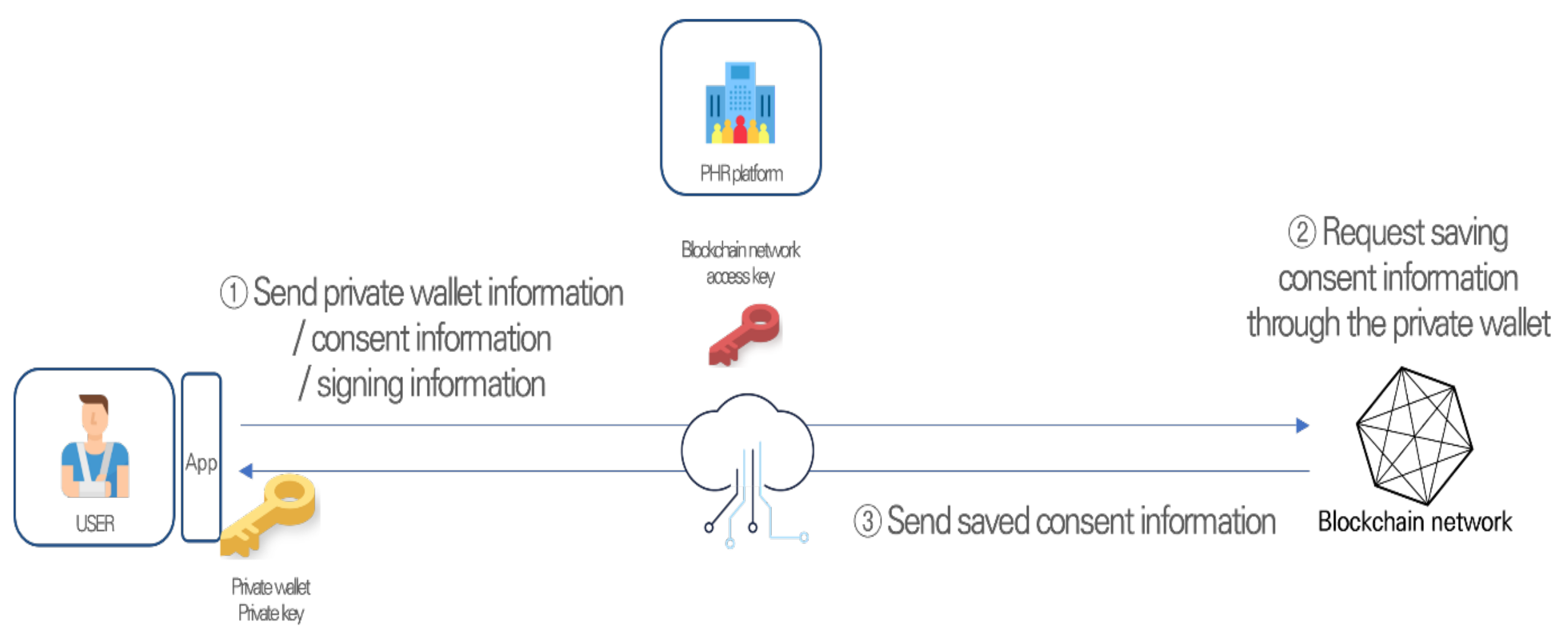
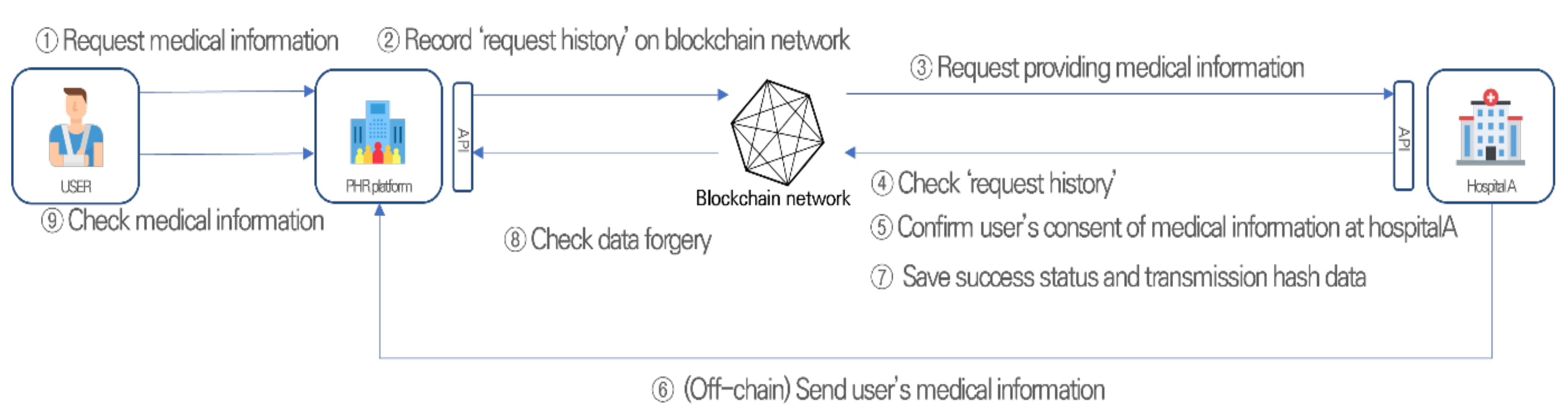
2.2.3. Flow of the Service
2.3. Study Design
2.3.1. Participants
2.3.2. Protocol
2.3.3. Questionnaire Study
2.3.4. In-Depth Interview
2.4. Data Analysis
3. Results
3.1. Demographics and SUS Score
3.2. Questionnaire Study
3.3. In-Depth Interviews
3.3.1. Intention of Use
“I like being able to check my records anywhere without having to go to the hospital.”[Study participant 30].
“By using the block chain [sic], the security is strengthened, and it seems to be reliable.”[Study participant 24].
“You can check it on the hospital app, too, so I don’t know much about the need.”[Study participant 10].
“I don’t know exactly what blockchain is, so I can’t say clearly, but honestly, I think that blockchain technology is really necessary? [sic].”[Study participant 29].
3.3.2. Acceptance of Technology
“I am only aware of the block chain [sic] technology that is applied to Bitcoin.”[Study participant 2].
“I don’t have to worry about how to use it because they gave me enough instructions.”[Study participant 3].
“It wasn’t difficult for me to understand, but I don’t know how adults will actually take it.”[Study participant 30].
3.3.3. Health Data Management and Sharing
“When I go to another hospital, I don’t have to explain my condition repeatedly, so I think sharing information will be helpful.”[Study participant 24].
“By using the blockchain, we feel that data is transmitted securely.”[Study participant 14].
3.3.4. Suggestions for Improvement
“If primary hospital, secondary hospital, tertiary hospital is linked, I am willing to use it.”[Study participant 10].
“If it is certified that there is no problem in security that blockchain technology has been applied through a government or institution, it is of course trustworthy.”[Study participant 28].
3.3.5. Summary of the In-Depth Interviews
4. Discussion
5. Limitations and Future Work
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Klini, S.; Markaki, A.; Kounalakis, D.; Emmanouil, K. Monitoring Reasons for Encounter via an Electronic Patient Record System: The Case of a Rural Practice Initiative. Int. J. Med. Sci. 2012, 9, 704–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abel, G.A.; Mendonca, S.C.; McPhail, S.; Zhou, Y.; Elliss-Brookes, L.; Lyratzopoulos, G. Emergency diagnosis of cancer and previous general practice consultations: Insights from linked patient survey data. Br. J. Gen. Pract. 2017, 67, e377–e387. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, J.S.; Kannry, J.; Lipton, M.; Goldberg, E.; Conocenti, P.; Stuard, S.; Wyatt, B.M.; Kuperman, G. Approaches to patient health information exchange and their impact on emergency medicine. Ann. Emerg. Med. 2006, 48, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Lee, S.-I.; Kim, Y.; Heo, E.-Y.; Lee, J.; Park, J.H.; Ha, K. Patients’ perceptions of a health information exchange: A pilot program in South Korea. Int. J. Med. Inform. 2013, 82, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Lee, S.-I.; Hwang, H.; Kim, Y.; Heo, E.-Y.; Kim, J.-W.; Ha, K. Can a health information exchange save healthcare costs? Evidence from a pilot program in South Korea. Int. J. Med. Inform. 2015, 84, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-I.; Park, H.; Kim, J.-W.; Hwang, H.; Cho, E.-Y.; Kim, Y.; Ha, K. Physicians’ Perceptions and Use of a Health Information Exchange: A Pilot Program in South Korea. Telemed. e-Health 2012, 18, 604–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.; Heo, E.; Lim, H.; Lee, J.Y.; Weon, S.; Chae, H.; Hwang, H.; Yoo, S. Developing a Common Health Information Exchange Platform to Implement a Nationwide Health Information Network in South Korea. Health Inform. Res. 2015, 21, 21–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brennan, P.F.; Kuang, Y.-S.; Volrathongchai, K. Patient-centered Information Systems. Yearb. Med. Inform. 2000, 1, 79–86. [Google Scholar] [CrossRef] [Green Version]
- Hussien, H.; Yasin, S.M.; Udzir, S.N.I.; Zaidan, A.A.; Zaidan, B.B. A Systematic Review for Enabling of Develop a Blockchain Technology in Healthcare Application: Taxonomy, Substantially Analysis, Motivations, Challenges, Recommendations and Future Direction. J. Med. Syst. 2019, 43, 320. [Google Scholar] [CrossRef]
- Roehrs, A.; da Costa, C.A.; Righi, R.D.R. OmniPHR: A distributed architecture model to integrate personal health records. J. Biomed. Inform. 2017, 71, 70–81. [Google Scholar] [CrossRef]
- Azaria, A.; Ekblaw, A.; Vieira, T.; Lippman, A. MedRec: Using Blockchain for Medical Data Access and Permission Management. In Proceedings of the 2016 2nd International Conference on Open and Big Data (OBD), Vienna, Austria, 22–24 August 2016; pp. 25–30. [Google Scholar] [CrossRef]
- Zhang, P.; White, J.; Schmidt, D.C.; Lenz, G.; Rosenbloom, S.T. FHIRChain: Applying Blockchain to Securely and Scalably Share Clinical Data. Comput. Struct. Biotechnol. J. 2018, 16, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Maslove, D.M.; Klein, J.; Brohman, K.; Martin, P. Using Blockchain Technology to Manage Clinical Trials Data: A Proof-of-Concept Study. JMIR Med. Inform. 2018, 6, e11949. [Google Scholar] [CrossRef]
- Wong, D.R.; Bhattacharya, S.; Butte, A.J. Prototype of running clinical trials in an untrustworthy environment using blockchain. Nat. Commun. 2019, 10, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clauson, K.A.; Breeden, E.A.; Davidson, C.; Mackey, T.K. Leveraging Blockchain Technology to Enhance Supply Chain Management in Healthcare. Blockchain Health Today 2018, 1, 1–12. [Google Scholar] [CrossRef]
- Castaldo, L.; Cinque, V. Blockchain-Based Logging for the Cross-Border Exchange of eHealth Data in Europe. In Informatics and Intelligent Applications; Springer: Cham, Switzerland, 2018; pp. 46–56. [Google Scholar]
- Patel, V. A framework for secure and decentralized sharing of medical imaging data via blockchain consensus. Health Inform. J. 2019, 25, 1398–1411. [Google Scholar] [CrossRef] [PubMed]
- Shen, B.; Guo, J.; Yang, Y. MedChain: Efficient Healthcare Data Sharing via Blockchain. Appl. Sci. 2019, 9, 1207. [Google Scholar] [CrossRef] [Green Version]
- Fan, K.; Wang, S.; Ren, Y.; Li, H.; Yang, Y. MedBlock: Efficient and Secure Medical Data Sharing Via Blockchain. J. Med. Syst. 2018, 42, 136. [Google Scholar] [CrossRef]
- Yang, J.; Onik, M.H.; Lee, N.-Y.; Ahmed, M.; Kim, C.-S. Proof-of-Familiarity: A Privacy-Preserved Blockchain Scheme for Collaborative Medical Decision-Making. Appl. Sci. 2019, 9, 1370. [Google Scholar] [CrossRef] [Green Version]
- Zhu, L.; Wu, Y.; Gai, K.; Choo, K.-K.R. Controllable and trustworthy blockchain-based cloud data management. Future Gener. Comput. Syst. 2019, 91, 527–535. [Google Scholar] [CrossRef]
- Genestier, P.; Zouarhi, S.; Limeux, P.; Excoffier, D.; Prola, A.; Sandon, S.; Temerson, J.M. Blockchain for consent management in the ehealth environment: A nugget for privacy and security challenges. J. Int. Soc. Telemed. eHealth 2017, 5, GKR-e24. [Google Scholar]
- Zhang, X.; Poslad, S. Blockchain Support for Flexible Queries with Granular Access Control to Electronic Medical Records (EMR). In Proceedings of the 2018 IEEE International Conference on Communications (ICC), Kansas City, MO, USA, 20–24 May 2018; pp. 1–6. [Google Scholar]
- Zhang, X.; Poslad, S.; Ma, Z. Block-Based Access Control for Blockchain-Based Electronic Medical Records (EMRs) Query in eHealth. In Proceedings of the 2018 IEEE Global Communications Conference (GLOBECOM), Abu Dhabi, UAE, 9–13 December 2018; pp. 1–7. [Google Scholar]
- Nakamoto, S. Bitcoin: A peer-to-peer electronic cash system. Decentralized Business Review (2008): 21260. Available online: https://bitcoin.org/bitcoin.pdf (accessed on 7 February 2022).
- Ali, S.I.M.; Farouk, H.; Sharaf, H. A blockchain-based models for student information systems. Egypt. Inform. J. 2021; in press. [Google Scholar] [CrossRef]
- Yadav, A.S.; Agrawal, S.; Kushwaha, D.S. Distributed Ledger Technology-based land transaction system with trusted nodes consensus mechanism. J. King Saud Univ.-Comput. Inf. Sci. 2021; in press. [Google Scholar] [CrossRef]
- Zhang, R.; Xue, R.; Liu, L. Security and Privacy on Blockchain. ACM Comput. Surv. 2020, 52, 1–34. [Google Scholar] [CrossRef] [Green Version]
- Ali, S.; Wang, G.; White, B.; Cottrell, R.L. A Blockchain-Based Decentralized Data Storage and Access Framework for PingER. In Proceedings of the 2018 17th IEEE International Conference on Trust, Security and Privacy in Computing and Communications/12th IEEE International Conference on Big Data Science and Engineering (TrustCom/BigDataSE), New York, NY, USA, 1–3 August 2018; pp. 1303–1308. [Google Scholar]
- Fouka, G.; Mantzorou, M. What are the major ethical issues in conducting research? Is there a conflict be-tween the research ethics and the nature of nursing? Health Sci. J. 2011, 5, 3. [Google Scholar]
- Hepp, T.; Sharinghousen, M.; Ehret, P.; Schoenhals, A.; Gipp, B. On-chain vs. off-chain storage for supply- and blockchain integration. It-Inf. Technol. 2018, 60, 283–291. [Google Scholar] [CrossRef]
- Dubovitskaya, A.; Baig, F.; Xu, Z.; Shukla, R.; Zambani, P.S.; Swaminathan, A.; Jahangir, M.; Chowdhry, K.; Lachhani, R.; Idnani, N.; et al. ACTION-EHR: Patient-Centric Blockchain-Based Electronic Health Record Data Management for Cancer Care. J. Med. Internet Res. 2020, 22, e13598. [Google Scholar] [CrossRef] [PubMed]
- Reijers, W.; Wuisman, I.; Mannan, M.; De Filippi, P.; Wray, C.; Rae-Looi, V.; Vélez, A.C.; Orgad, L. Now the Code Runs Itself: On-Chain and Off-Chain Governance of Blockchain Technologies. Topoi 2021, 40, 821–831. [Google Scholar] [CrossRef] [Green Version]
- Khatoon, A. A Blockchain-Based Smart Contract System for Healthcare Management. Electronics 2020, 9, 94. [Google Scholar] [CrossRef] [Green Version]
- Mackey, T.K.; Miyachi, K.; Fung, D.; Qian, S.; Short, J. Combating Health Care Fraud and Abuse: Conceptualization and Prototyping Study of a Blockchain Antifraud Framework. J. Med. Internet Res. 2020, 22, e18623. [Google Scholar] [CrossRef] [PubMed]
- Cagnazzo, M.; Hertlein, M.; Holz, T.; Pohlmann, N. Threat modeling for mobile health systems. In Proceedings of the 2018 IEEE Wireless Communications and Networking Conference Workshops (WCNCW), Barcelona, Spain, 15–18 April 2018; pp. 314–319. [Google Scholar]
- Oh, S.-R.; Seo, Y.-D.; Lee, E.; Kim, Y.-G. A Comprehensive Survey on Security and Privacy for Electronic Health Data. Int. J. Environ. Res. Public Health 2021, 18, 9668. [Google Scholar] [CrossRef] [PubMed]
- Namasudra, S.; Deka, G.C.; Johri, P.; Hosseinpour, M.; Gandomi, A.H. The Revolution of Blockchain: State-of-the-Art and Research Challenges. Arch. Comput. Methods Eng. 2021, 28, 1497–1515. [Google Scholar] [CrossRef]
- Mettler, M. Blockchain technology in healthcare: The revolution starts here. In Proceedings of the 2016 IEEE 18th International Conference on e-Health Networking, Applications and Services (Healthcom), Munich, Germany, 14–16 September 2016; pp. 1–3. [Google Scholar]
- Newton, E.H. Addressing overuse in emergency medicine: Evidence of a role for greater patient engagement. Clin. Exp. Emerg. Med. 2017, 4, 189–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gurley, K.; Onyeii, C.; Burstein, J.; Grossman, S. Management pathway for emergency department patients in the setting of the opioid epidemic and emergency department overcrowding. Clin. Exp. Emerg. Med. 2020, 7, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Van der Linden, H.; Kalra, D.; Hasman, A.; Talmon, J. Inter-organizational future proof EHR systems: A review of the security and privacy related issues. Int. J. Med. Inform. 2009, 78, 141–160. [Google Scholar] [CrossRef] [PubMed]
- Albanese, G.; Calbimonte, J.-P.; Schumacher, M.; Calvaresi, D. Dynamic consent management for clinical trials via private blockchain technology. J. Ambient Intell. Humaniz. Comput. 2020, 11, 4909–4926. [Google Scholar] [CrossRef]
- Saldamli, G.; Reddy, V.; Bojja, K.S.; Gururaja, M.K.; Doddaveerappa, Y.; Tawalbeh, L. Health Care Insurance Fraud Detection Using Blockchain. In Proceedings of the 2020 Seventh International Conference on Software Defined Systems (SDS), Paris, France, 20–23 April 2020; pp. 145–152. [Google Scholar]
- Kampik, T.; Najjar, A. Simulating, Off-Chain and On-Chain: Agent-Based Simulations in Cross-Organizational Business Processes. Information 2020, 11, 34. [Google Scholar] [CrossRef] [Green Version]
- Siyal, A.A.; Junejo, A.Z.; Zawish, M.; Ahmed, K.; Khalil, A.; Soursou, G. Applications of Blockchain Technology in Medicine and Healthcare: Challenges and Future Perspectives. Cryptography 2019, 3, 3. [Google Scholar] [CrossRef] [Green Version]
- Denzin, N.K.; Lincoln, Y.S.; Giardina, M.D. Disciplining qualitative research1. Int. J. Qual. Stud. Educ. 2006, 19, 769–782. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | % | ||
|---|---|---|---|
| Total | 30 | 100 | |
| Sex | Male | 15 | 50 |
| Female | 15 | 50 | |
| Age | 20’s | 11 | 36.7 |
| 30’s | 14 | 46.7 | |
| >40’s | 5 | 16.6 | |
| Reason for visit (Duplicate responses are possible) | Outpatient | 30 | 100 |
| Emergency | 4 | 13.3 |
| Category | Question | 1 | 2 | 3 | 4 | 5 | MODE |
|---|---|---|---|---|---|---|---|
| Understanding of blockchain technology | I have heard of blockchain. | 0 | 2 | 0 | 13 | 15 | 5 |
| I know how blockchain technology is applied. | 4 | 6 | 9 | 7 | 4 | 3 | |
| I considered using blockchain to manage my health information. | 5 | 13 | 2 | 5 | 5 | 2 | |
| Trust of blockchain technology | I trust blockchain technology. | 1 | 2 | 12 | 10 | 5 | 3 |
| I think blockchain technology protects my health information safely. | 0 | 6 | 7 | 13 | 4 | 4 | |
| I agree that the blockchain transmits data safely. | 2 | 2 | 8 | 14 | 4 | 4 | |
| I think blockchain technology is more reliable than conventional methods in transmitting health information. | 2 | 1 | 13 | 11 | 3 | 3 | |
| Familiarity of blockchain technology | I think blockchain technology has an advantage in accessing my health information. | 1 | 0 | 8 | 11 | 10 | 4 |
| I think I am familiar with blockchain technology. | 7 | 13 | 6 | 3 | 1 | 2 |
| Category | Question | 1 | 2 | 3 | 4 | 5 | MODE |
|---|---|---|---|---|---|---|---|
| Understanding of exchange health information | I have heard of a dynamic consent system. | 22 | 1 | 1 | 4 | 2 | 1 |
| I was able to actively participate in utilizing and exchanging my health information. | 1 | 1 | 1 | 17 | 10 | 4 | |
| I am interested in accessing my health information independently. | 0 | 0 | 1 | 12 | 17 | 5 | |
| Digital literacy | I use the Internet well. | 0 | 1 | 2 | 1 | 26 | 5 |
| I make good use of digital technology. | 0 | 2 | 2 | 8 | 18 | 5 | |
| I use the applications on my smartphone well. | 0 | 0 | 5 | 6 | 19 | 5 | |
| I can download and install applications well on my phone. | 0 | 1 | 1 | 1 | 27 | 5 | |
| I am active in learning digital technology. | 0 | 0 | 5 | 6 | 19 | 5 | |
| I feel scared when someone talks about digital technology. | 16 | 7 | 5 | 1 | 1 | 1 |
| Key Theme | Category | Pros | Cons |
|---|---|---|---|
| Intention of use | Blockchain | Blockchain is needed to protect patient data. Blockchain is needed because it is good in terms of system security. | Wondering if blockchain is the only way to protect patients’ information. |
| PHR | Exchanging patients’ health information is needed. Checking my health data anywhere and anytime is needed. | App provided by the hospital can also be used to check patient health data. | |
| Acceptance of technology | Blockchain | A basic understanding of blockchain technology. Users can have sovereignty over their own data. | Does not know about the technology. Heard of the technology but does not know about the mechanism. |
| PHR | No difficulty in using service. | A manual on how to use the service is needed. Application design needs to be a little more intuitive. | |
| Health data management and sharing | Blockchain | Health data could be systemically managed. Able to independently manage my own health data. | Negative opinion due to not knowing much about the technology. |
| PHR | Sharing information with medical staff has become easy. | Not very interested. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.W.; Kim, S.J.; Cha, W.C.; Kim, T. A Blockchain-Applied Personal Health Record Application: Development and User Experience. Appl. Sci. 2022, 12, 1847. https://doi.org/10.3390/app12041847
Kim JW, Kim SJ, Cha WC, Kim T. A Blockchain-Applied Personal Health Record Application: Development and User Experience. Applied Sciences. 2022; 12(4):1847. https://doi.org/10.3390/app12041847
Chicago/Turabian StyleKim, Ji Woong, Su Jin Kim, Won Chul Cha, and Taerim Kim. 2022. "A Blockchain-Applied Personal Health Record Application: Development and User Experience" Applied Sciences 12, no. 4: 1847. https://doi.org/10.3390/app12041847
APA StyleKim, J. W., Kim, S. J., Cha, W. C., & Kim, T. (2022). A Blockchain-Applied Personal Health Record Application: Development and User Experience. Applied Sciences, 12(4), 1847. https://doi.org/10.3390/app12041847