
Clinical Outcomes of the Double Lateral Sliding Bridge Flap Technique with Simultaneous Connective Tissue Graft in Sextant V Recessions: Three-Year Follow-Up Study

 ,
,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
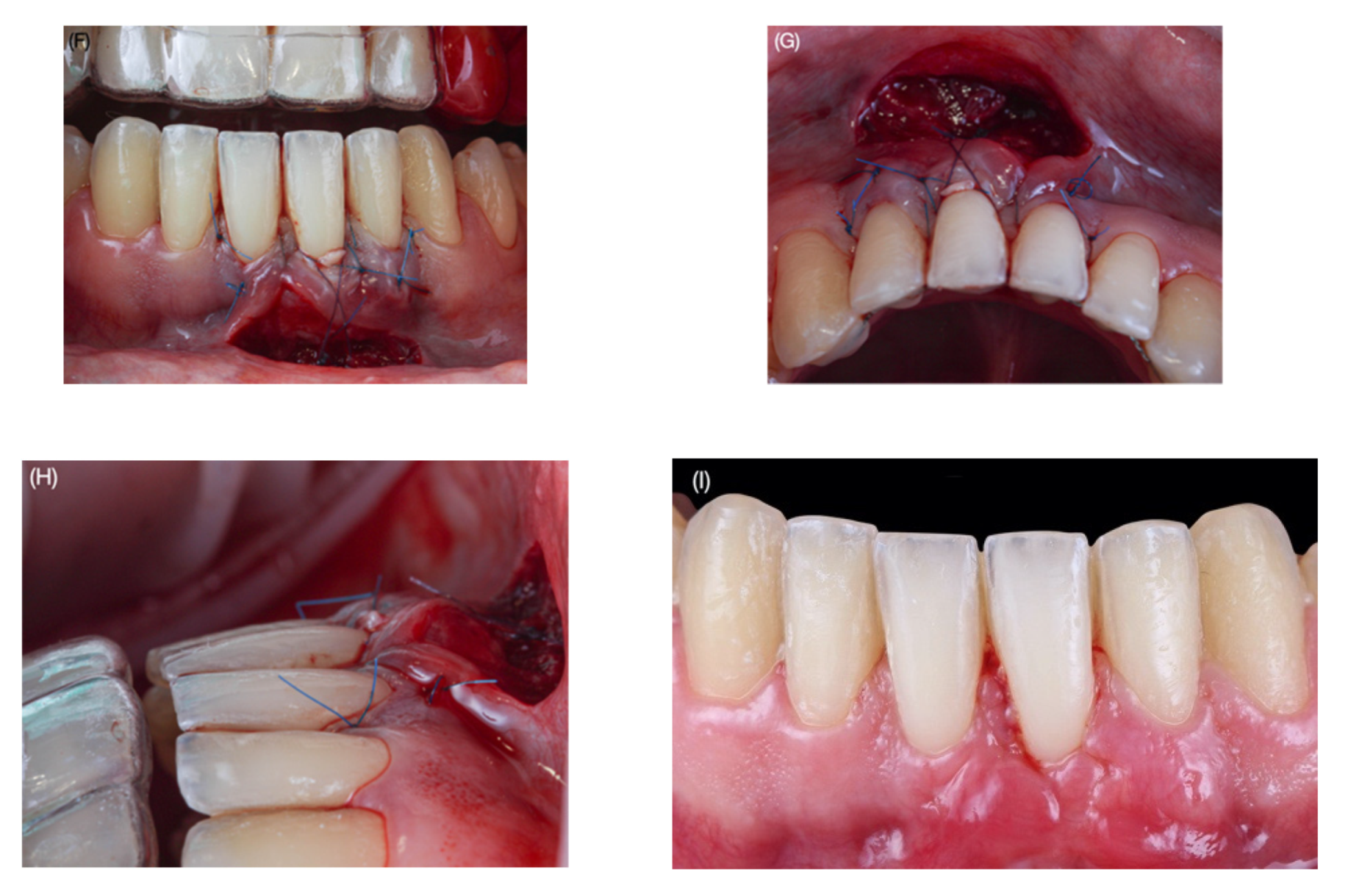
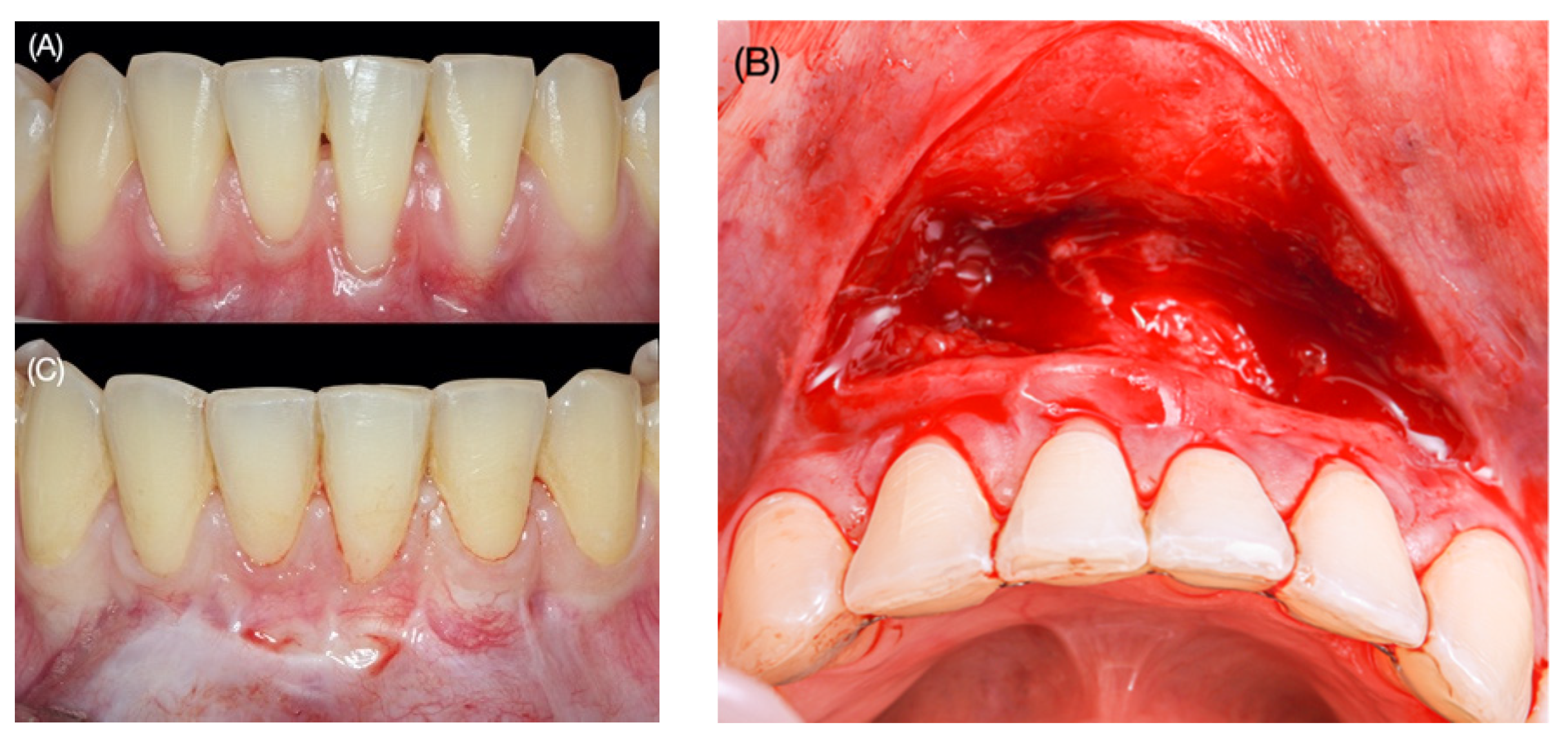
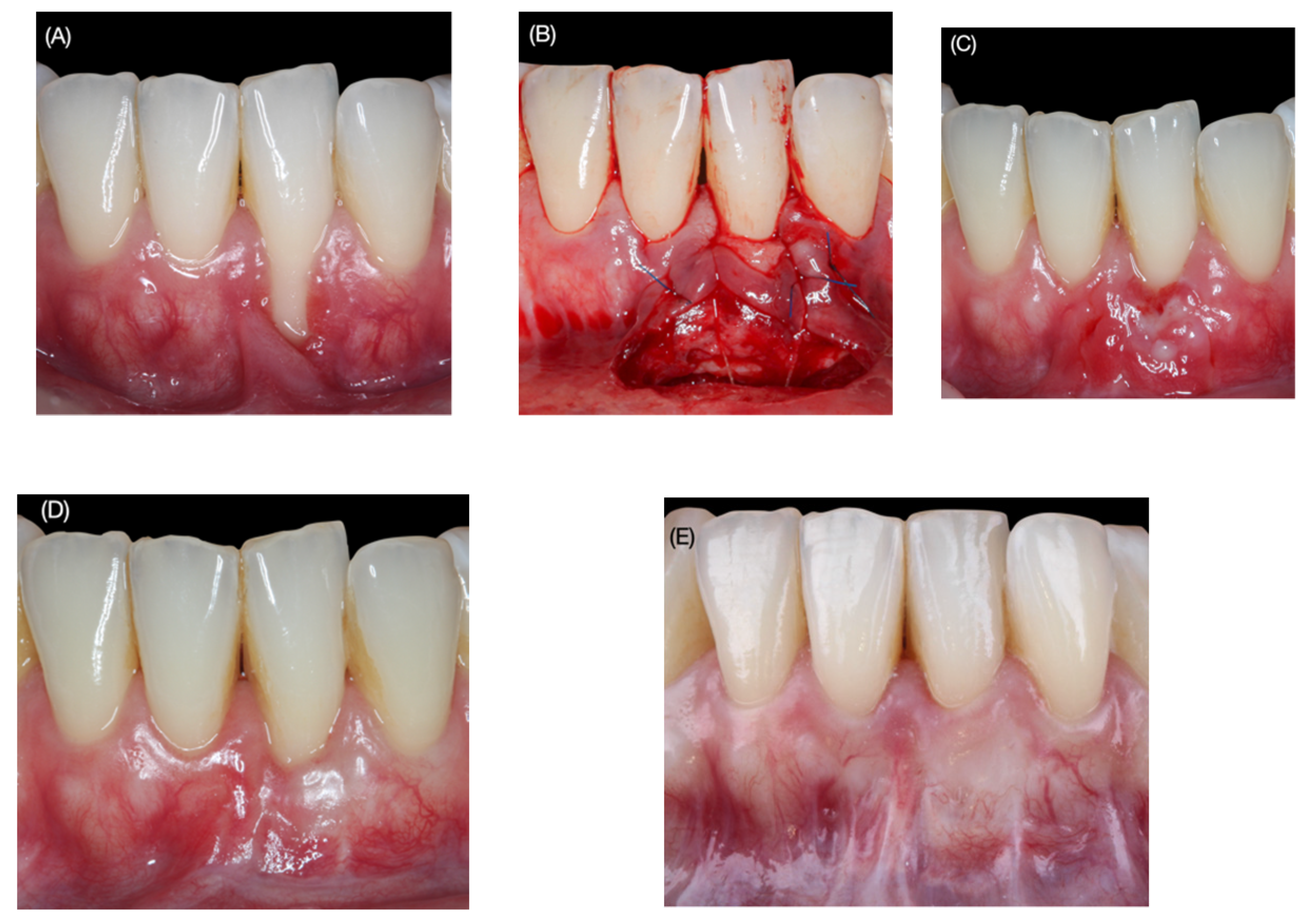
2.1. Surgical Protocol
2.2. Baseline Clinical Assessment
- Recession type (RT): the Miller [27] classification was used.
- Gingival recession depth (GRD), recorded in millimeters from the cementoenamel junction to the most apical point of the gingival margin.
- Probing depth (PD), recorded in millimeters from the gingival margin to the bottom of the gingival sulcus.
- Clinical attachment level (CAL): algebraic sum of the PD and GRD.
- Keratinized tissue width (KTW), measured in millimeters from the most apical point of the gingival margin to the mucogingival junction (MGJ).
- Gingival thickness (GT), measured in millimeters at 2 mm from the new gingival margin using a K#10 endodontic file with rubber stop (transgingival probing) [29].
- The percentage of root coverage (RC) was calculated according to the following formula: ([preoperative REC—postoperative REC]/preoperative REC) ×100.
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CEJ | cementoenamel junction |
| CTG | connective tissue graft |
| GR | gingival recession |
| RT | recession type |
| GRD | gingival recession depth |
| PD | probing depth |
| CAL | clinical attachment level |
| KTW | keratinized tissue width |
| GT | gingival thickness |
| MGJ | mucogingival junction |
| RC | root coverage |
| CRC | complete root coverage |
| CAF | coronally advanced flap |
References
- Cortellini, P.; Bissada, N.F. Mucogingival conditions in the natural dentition: Narrative review, case definitions, and diagnostic considerations. J. Periodontol. 2018, 89 (Suppl. 1), S204–S213. [Google Scholar] [CrossRef] [PubMed]
- Hugoson, A.; Sjödin, B.; Norderyd, O. Trends over 30 years, 1973–2003, in the prevalence and severity of periodontal disease. J. Clin. Periodontol. 2008, 35, 405–414. [Google Scholar] [CrossRef]
- Matas, F.; Sentís, J.; Mendieta, C. Ten-year longitudinal study of gingival recession in dentists. J. Clin. Periodontol. 2011, 38, 1091–1098. [Google Scholar] [CrossRef]
- Nieri, M.; Pini Prato, G.P.; Giani, M.; Magnani, N.; Pagliaro, U.; Rotundo, R. Patient perceptions of buccal gingival recessions and requests for treatment. J. Clin. Periodontol. 2013, 40, 707–712. [Google Scholar] [CrossRef]
- Douglas de Oliveira, D.W.; Oliveira-Ferreira, F.; Flecha, O.D.; Gonçalves, P.F. Is surgical root coverage effective for the treatment of cervical dentin hypersensitivity? A systematic review. J. Periodontol. 2013, 84, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Merijohn, G.K. Management and prevention of gingival recession. Periodontol. 2000 2016, 71, 228–242. [Google Scholar] [CrossRef]
- Cairo, F.; Pagliaro, U.; Nieri, M. Treatment of gingival recession with coronally advanced flap procedures: A systematic review. J. Clin. Periodontol. 2008, 35, 136–162. [Google Scholar] [CrossRef]
- Cairo, F.; Nieri, M.; Pagliaro, U. Efficacy of periodontal plastic surgery procedures in the treatment of localized facial gingival recessions. A systematic review. J. Clin. Periodontol. 2014, 41 (Suppl. 15), s44–s62. [Google Scholar] [CrossRef]
- Cairo, F.; Cortellini, P.; Tonetti, M.; Nieri, M.; Mervelt, J.; Cincinelli, S.; Pini-Prato, G. Coronally advanced flap with and without connective tissue graft for the treatment of single maxillary gingival recession with loss of inter-dental attachment. A randomized controlled clinical trial. J. Clin. Periodontol. 2012, 39, 760–768. [Google Scholar] [CrossRef]
- Graziani, F.; Gennai, S.; Roldan, S.; Discepoli, N.; Buti, J.; Madianos, P.; Herrera, D. Efficacy of periodontal plastic procedures in the treatment of multiple gingival recessions. J. Clin. Periodontol. 2014, 41, s63–s76. [Google Scholar] [CrossRef] [PubMed]
- Aroca, S.; Keglevich, T.; Nikolidakis, D.; Gera, I.; Nagy, K.; Azzi, R.; Etienne, D. Treatment of class III multiple gingival recessions: A randomized-clinical trial. J. Clin. Periodontol. 2010, 37, 88–97. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Jepsen, S.; Working Group 2 of the European Workshop on Periodontology. Clinical efficacy of periodontal plastic surgery procedures: Consensus report of Group 2 of the 10th European Workshop on Periodontology. J. Clin. Periodontol. 2014, 41 (Suppl. 15), S36–S43. [Google Scholar] [CrossRef] [PubMed]
- Müller, H.P.; Könönen, E. Variance components of gingival thickness. J. Periodontal. Res. 2005, 40, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Gebistorf, M.; Mijuskovic, M.; Pandis, N.; Fudalej, P.-S.; Katsaros, C. Gingival recession in orthodontic patients 10 to 15 years posttreatment: A retrospective cohort study. Am. J. Orthod. Dentofacial. Orthop. 2018, 153, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Kaitsas, R.; Kaitsas, F.; Paolone, G.; Paolone, M.-G. Ortho-Perio Risk Assessment and timing flowchart for lingual orthodontics in an interdisciplinary adult ortho-perio patient: A case report of “Perio-Guided” Orthodontic treatment. Int. Orthod. 2021, S1761–7227, 00143–1. [Google Scholar] [CrossRef]
- Cortellini, P.; Tonetti, M.; Prato, G.-P. The partly epithelialized free gingival graft (pe-fgg) at lower incisors. A pilot study with implications for alignment of the mucogingival junction. J. Clin. Periodontol. 2012, 39, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Nart, J.; Valles, C. Subepithelial Connective Tissue Graft in Combination with a Tunnel Technique for the Treatment of Miller Class II and III Gingival Recessions in Mandibular Incisors: Clinical and Esthetic Results. Int. J. Periodontics Restor. Dent. 2016, 36, 591–598. [Google Scholar] [CrossRef]
- Zucchelli, G.; Marzadori, M.; Mounssif, I.; Mazzotti, C.; Stefanini, M. Coronally advanced flap + connective tissue graft techniques for the treatment of deep gingival recession in the lower incisors. A controlled randomized clinical trial. J. Clin. Periodontol. 2014, 41, 806–813. [Google Scholar] [CrossRef]
- De Angelis, N.; Yumang, C.; Benedicenti, S. Efficacy of the lateral advanced flap in root-coverage procedures for mandibular central incisors: A 5-year clinical study. Int. J. Periodontics Restor. Dent. 2015, 35, e9–e13. [Google Scholar] [CrossRef]
- Harris, R.J. The connective tissue and partial thickness double pedicle graft: A predictable method of obtaining root coverage. J. Periodontol. 1992, 63, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Allen, E.-P. The Laterally Closed Tunnel for the Treatment of Deep Isolated Mandibular Recessions: Surgical Technique and a Report of 24 Cases. Int. J. Periodontics Restor. Dent. 2018, 38, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Zabalegui, I.; Sicilia, A.; Cambra, J.; Gil, J.; Sanz, M. Treatment of multiple adjacent gingival recessions with the tunnel subepithelial connective tissue graft: A clinical report. Int. J. Periodontics Restor. Dent. 1999, 19, 199–206. [Google Scholar]
- Stefanini, M.; Zucchelli, G.; Marzadori, M.; de Sanctis, M. Coronally Advanced Flap with Site-Specific Application of Connective Tissue Graft for the Treatment of Multiple Adjacent Gingival Recessions: A 3-Year Follow-Up Case Series. Int. J. Periodontics Restor. Dent. 2018, 38, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.J.; Miller, L.H.; Harris, C.R.; Miller, R.J. A comparison of three techniques to obtain root coverage on mandibular incisors. J. Periodontol. 2005, 76, 1758–1767. [Google Scholar] [CrossRef]
- Kerner, S.; Sarfati, A.; Katsahian, S.; Jaumet, V.; Micheau, C.; Mora, F.; Monnet-Corti, V.; Bouchard, P. Qualitative cosmetic evaluation after root-coverage procedures. J. Periodontol. 2009, 80, 41–47. [Google Scholar] [CrossRef]
- Cairo, F.; Nieri, M.; Cattabriga, M.; Cortellini, P.; De Paoli, S.; De Sanctis, M.; Fonzar, A.; Francetti, L.; Merli, M.; Rasperini, G.; et al. Root coverage esthetic score after treatment of gingival recession: An interrater agreement multicenter study. J. Periodontol. 2010, 81, 1752–1758. [Google Scholar] [CrossRef]
- Miller, P.D., Jr. A classification of marginal tissue recession. Int. J. Periodontics Restor. Dent. 1985, 5, 8–13. [Google Scholar]
- Romanos, G.E.; Bernimoulin, J.P.; Marggraf, E. The double lateral bridging flap for coverage of denuded root surface: Longitudinal study and clinical evaluation after 5 to 8 years. J. Periodontol. 1993, 64, 683–688. [Google Scholar] [CrossRef]
- Ronay, V.; Sahrmann, P.; Bindl, A.; Attin, T.; Schmidlin, P.-R. Current status and perspectives of mucogingival soft tissue measurement methods. J. Esthet. Restor. Dent. 2011, 23, 146–156. [Google Scholar] [CrossRef]
- Marggraf, E. A direct technique with a double lateral bridging flap for coverage of denuded root surface and gingiva extension. Clinical evaluation after 2 years. J. Clin. Periodontol. 1985, 12, 69–76. [Google Scholar] [CrossRef]
- Chambrone, L.; Sukekava, F.; Araújo, M.-G.; Pustiglioni, F.-E.; Chambrone, L.-A.; Lima, L.-A. Root-coverage procedures for the treatment of localized recession-type defects: A Cochrane systematic review. J Periodontol. 2010, 81, 452–478. [Google Scholar] [CrossRef]
- Tatakis, D.-N.; Chambrone, L.; Allen, E.-P.; Langer, B.; McGuire, M.-K.; Richardson, C. Periodontal soft tissue root coverage procedures: A consensus report from the AAP Regeneration Workshop. J. Periodontol. 2015, 86 (Suppl. S2), S52–S55. [Google Scholar] [CrossRef]
- Bethaz, N.; Romano, F.; Ferrarotti, F.; Mariani, G.-M.; Aimetti, M. A mucogingival technique for the treatment of multiple recession defects in the mandibular anterior region: A case series with a 2-year follow-up. Int. J. Periodontics Restor. Dent. 2014, 34, 345–352. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Edlan, A.; Mejchar, B. Plastic surgery of the vestibulum in periodontal therapy. Int. Dent. J. 1963, 13, 593–596. [Google Scholar]
- Azzi, R.; Etienne, D.; Sauvan, J.L.; Miller, P.D. Root coverage and papilla reconstruction in Class IV recession: A case report. Int. J. Periodontics Restor. Dent. 1999, 19, 449–455. [Google Scholar]
- Nart, J.; Valles, C.; Mareque, S.; Santos, A.; Sanz-Moliner, J.; Pascual, A. Subepithelial connective tissue graft in combination with a coronally advanced flap for the treatment of Miller Class II and III gingival recessions in mandibular incisors: A case series. Int. J. Periodontics Restor. Dent. 2012, 32, 647–654. [Google Scholar]
- Zucchelli, G.; Tavelli, L.; Ravidà, A.; Stefanini, M.; Suárez-López Del Amo, F.; Wang, H.-L. Influence of tooth location on coronally advanced flap procedures for root coverage. J. Periodontol. 2018, 89, 1428–1441. [Google Scholar] [CrossRef]
- Chambrone, L.; Chambrone, D.; Pustiglioni, F.-E.; Chambrone, L.-A.; Lima, L.-A. The influence of tobacco smoking on the outcomes achieved by root-coverage procedures: A systematic review. J. Am. Dent. Assoc. 2009, 140, 294–306. [Google Scholar] [CrossRef]
- Polizzi, E.; TetÃ, G.; Bova, F.; Pantaleo, G.; Gastaldi, G.; CapparÃ, P.; Gherlone, E. Antibacterial properties and side effects of chlorhexidine-based mouthwashes. A prospective, randomized clinical study. J. Osseointegr. 2019, 12, 2–7. [Google Scholar] [CrossRef]
- Parween, S.; George, J.-P.; Prabhuji, M. Treatment of Multiple Mandibular Gingival Recession Defects Using MCAT Technique and SCTG With and Without rhPDGF-BB: A Randomized Controlled Clinical Trial. Int. J. Periodontics Restor. Dent. 2020, 40, e43–e51. [Google Scholar] [CrossRef]
- Pini-Prato, G.; Cairo, F.; Nieri, M.; Rotundo, R.; Franceschi, D. Esthetic evaluation of root coverage outcomes: A case series study. Int. J. Periodontics Restor. Dent. 2011, 31, 603–610. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline | 3 Years | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient (n) | Age | Tooth (FDI) | RT (mm) | PD (mm) | GRD (mm) | CAL (mm) | KTW (mm) | CEJ (A/B) | Step (+/−) | PD (mm) | GRD (mm) | CAL Gain (mm) | KTW (mm) | GT (mm) |
| 1 | 29 | 31 | II | 2 | 3 | 5 | 0 | A | - | 4 | 0 | 4 | 3 | 1.1 |
| 2 | 27 | 41 | II | 1.5 | 2.5 | 4 | 0.5 | A | - | 2 | 0 | 2 | 3 | 1 |
| 3 | 41 | 41 | III | 2 | 6 | 8 | 0.5 | A | - | 5 | 1.5 | 6.5 | 5 | 1.7 |
| 4 | 37 | 41 | III | 2 | 1.5 | 3.5 | 4 | A | - | 2.5 | 0.5 | 3 | 4 | 1.7 |
| 37 | 31 | III | 2 | 3.5 | 5.5 | 1 | A | - | 2 | 0.5 | 2.5 | 5 | 1.2 | |
| 5 | 38 | 31 | III | 1 | 6 | 7 | 0 | A | - | 3 | 0 | 3 | 5 | 1.3 |
| 6 | 31 | 31 | II | 2 | 4 | 6 | 1 | A | - | 2 | 0.5 | 2.5 | 3 | 1.1 |
| 7 | 22 | 42 | III | 2 | 1.5 | 3.5 | 0 | A | - | 2 | 0 | 2 | 1 | 1 |
| 22 | 41 | III | 2 | 1 | 3 | 0.5 | A | - | 4 | 0 | 4 | 1 | 1.5 | |
| 22 | 31 | III | 1 | 4 | 5 | 0 | A | - | 1.5 | 1 | 2.5 | 1 | 1.1 | |
| 22 | 32 | III | 2 | 2 | 4 | 0 | A | - | 2.5 | 0 | 2.5 | 2 | 1.1 | |
| 8 | 28 | 31 | III | 2 | 4 | 6 | 0 | A | - | 3 | 2.5 | 5.5 | 1 | 1.5 |
| 9 | 38 | 41 | III | 1 | 3 | 4 | 1 | A | - | 3 | 1 | 4 | 1 | 1.4 |
| 38 | 31 | III | 1 | 3 | 4 | 1 | A | - | 2 | 2 | 4 | 1.5 | 2 | |
| Baseline and 36-Month Follow-Up | ||||
|---|---|---|---|---|
| Parameters | N | Mean ± SD | Range | p |
| GRD (mm) | 14 | |||
| Baseline | 14 | 3.2 ± 1.5 | 1–6 | |
| 36 months | 14 | 0.7 ± 0.8 | 0–2.5 | |
| Difference | 14 | 2.5 ± 1.5 | 1–6 | <0.01 |
| PD (mm) | 14 | |||
| Baseline | 14 | 1.7 ± 0.5 | 1–2 | |
| 36 months | 14 | 2.7 ± 1 | 1.5–5 | |
| Difference | 14 | 1.1 ± 1.0 | 0–6 | <0.01 |
| CAL (mm) | 14 | |||
| Baseline | 14 | 4.9 ± 1.5 | 3–8 | |
| 36 months | 14 | 3.4 ± 1.3 | 2.0–6.5 | |
| Difference | 14 | 1.5 ±1.4 | (−1)–4 | <0.01 |
| KTW (mm) | 14 | |||
| Baseline | 14 | 0.7 ± 1 | 0–4 | |
| 36 months | 14 | 2.6 ± 1.6 | 1–5 | |
| Difference | 14 | 1.9 ±1.7 | 0–5 | <0.01 |
| GT (mm) | 14 | |||
| Baseline | 14 | 0.0± 0.0 | 0–0 | |
| 36 months | 14 | 1.3 ± 0.3 | 1–2 | |
| Difference | 14 | 1.3 ± 0.3 | 1–2 | <0.01 |
| RES Score | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Parameter | Level of Gingival Margin * | Marginal Tissue Contour ** | Soft Tissue Texture *** | Mucogingival Junction **** | Gingival Color ***** | ||||||
| TF | |||||||||||
| Score | 0 | 3 | 6 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 1 |
| n. (%) | 1 | 4 | 9 | 4 | 10 | 8 | 6 | 4 | 10 | 3 | 11 |
| (7.1) | (28.6) | (64.3) | (28.6) | (71.4) | (57.1) | (42.9) | (28.6) | (71.4) | (21.4) | (78.6) | |
| Total Score Average Mean (SD) | 7.4 (2.7) | ||||||||||
| Median (IQR) | 8.5 (4) | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quispe-López, N.; Castaño-Séiquer, A.; Pardal-Peláez, B.; Garrido-Martínez, P.; Gómez-Polo, C.; Mena-Álvarez, J.; Montero-Martín, J. Clinical Outcomes of the Double Lateral Sliding Bridge Flap Technique with Simultaneous Connective Tissue Graft in Sextant V Recessions: Three-Year Follow-Up Study. Appl. Sci. 2022, 12, 1038. https://doi.org/10.3390/app12031038
Quispe-López N, Castaño-Séiquer A, Pardal-Peláez B, Garrido-Martínez P, Gómez-Polo C, Mena-Álvarez J, Montero-Martín J. Clinical Outcomes of the Double Lateral Sliding Bridge Flap Technique with Simultaneous Connective Tissue Graft in Sextant V Recessions: Three-Year Follow-Up Study. Applied Sciences. 2022; 12(3):1038. https://doi.org/10.3390/app12031038
Chicago/Turabian StyleQuispe-López, Norberto, Antonio Castaño-Séiquer, Beatriz Pardal-Peláez, Pablo Garrido-Martínez, Cristina Gómez-Polo, Jesús Mena-Álvarez, and Javier Montero-Martín. 2022. "Clinical Outcomes of the Double Lateral Sliding Bridge Flap Technique with Simultaneous Connective Tissue Graft in Sextant V Recessions: Three-Year Follow-Up Study" Applied Sciences 12, no. 3: 1038. https://doi.org/10.3390/app12031038
APA StyleQuispe-López, N., Castaño-Séiquer, A., Pardal-Peláez, B., Garrido-Martínez, P., Gómez-Polo, C., Mena-Álvarez, J., & Montero-Martín, J. (2022). Clinical Outcomes of the Double Lateral Sliding Bridge Flap Technique with Simultaneous Connective Tissue Graft in Sextant V Recessions: Three-Year Follow-Up Study. Applied Sciences, 12(3), 1038. https://doi.org/10.3390/app12031038