
A Comparison of Hip Muscle Mass, Muscle Power, and Clinical Outcomes with Long-Term Follow-Up in Patients with Metal-on-Metal Hip Arthroplasty Compared to Metal-on-Polyethylene Hip Arthroplasty
 ,
, 
Abstract
1. Introduction
2. Materials and Methods
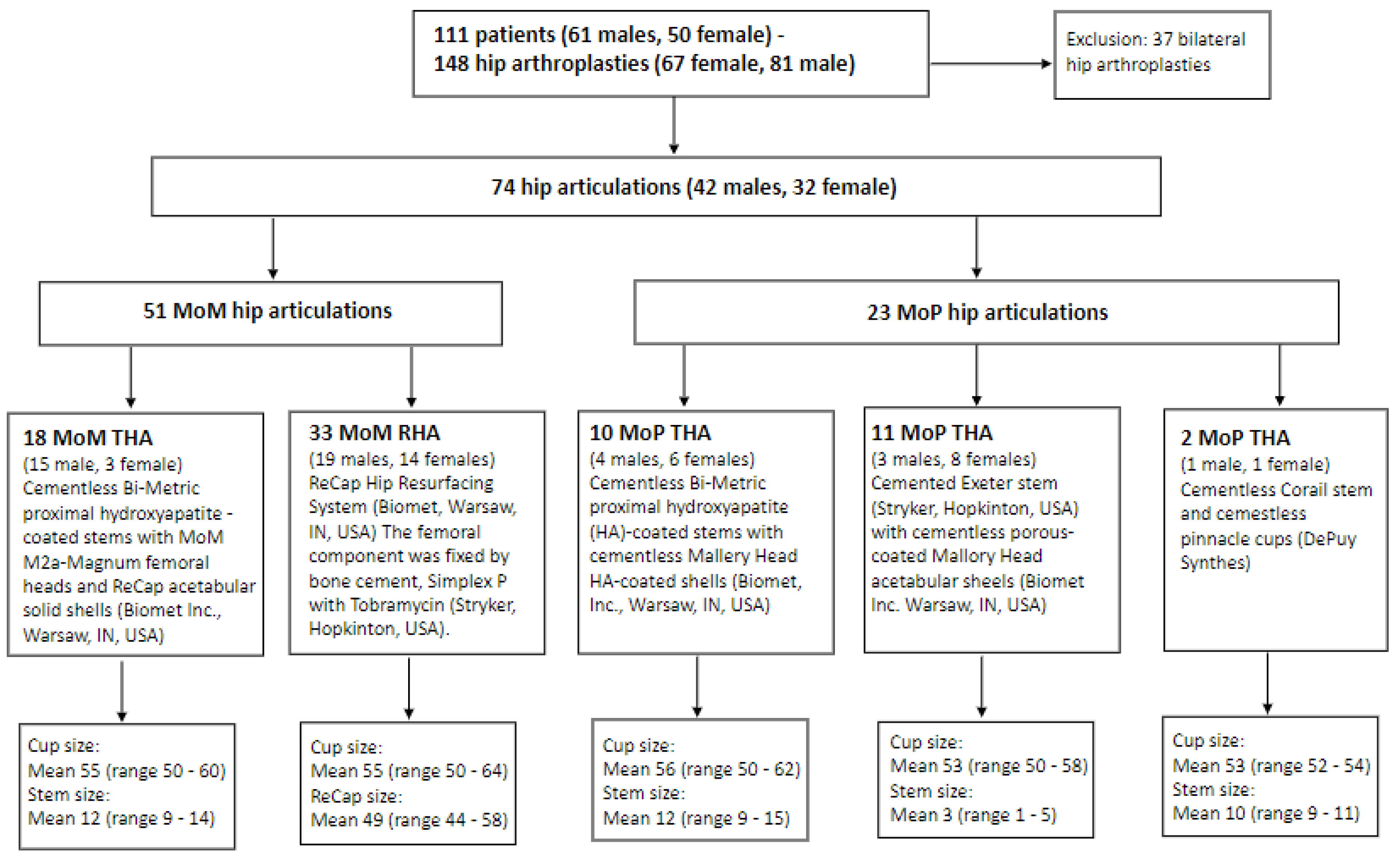
2.1. Patients and Articulations
2.2. Dual-Energy X-ray Absorptiometry (DXA) Scans
2.3. Leg Extensor Power Rig (LEPR)
2.4. Inertial Measurement Unit (IMU)
2.5. Step Test
2.6. Harris Hip Score (HHS) and the Copenhagen Hip and Groin Outcome Score (HAGOS)
2.7. Statistical Analysis
3. Results
3.1. Dual-Energy X-ray Absorptiometry (DXA) Scans
3.2. Leg Extensor Power Rig (LEPR)
3.3. Step Test
3.4. The Harris Hip Score (HHS) and the Copenhagen Hip and Groin Outcome Score (HAGOS) and Correlations
3.5. Sub-Analysis Comparing Males to Males, Females to Females
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wylde, V.; Blom, A.W. Assessment of outcomes after hip arthroplasty. Hip Int. 2009, 19, 1–7. [Google Scholar] [CrossRef]
- Jinks, C.; Lewis, M.; Croft, P. Health status after hip or knee arthroplasty. Ann. Rheum. Dis. 2003, 62, 700–701. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.A.; Voaklander, D.C.; Johnston, D.W.; Suarez-Almazor, M.E. Health related quality of life outcomes after total hip and knee arthroplasties in a community based population. J. Rheumatol. 2000, 27, 1745–1752. [Google Scholar] [PubMed]
- Wilkinson, J.M.; Hamer, A.J.; Stockley, I.; Eastell, R. Polyethylene wear rate and osteolysis: Critical threshold versus continuous dose-response relationship. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2005, 23, 520–525. [Google Scholar] [CrossRef]
- Dumbleton, J.H.; Manley, M.T.; Edidin, A.A. A literature review of the association between wear rate and osteolysis in total hip arthroplasty. J. Arthroplast. 2002, 17, 649–661. [Google Scholar] [CrossRef] [PubMed]
- Numair, J.; Joshi, A.B.; Murphy, J.C.; Porter, M.L.; Hardinge, K. Total hip arthroplasty for congenital dysplasia or dislocation of the hip. Survivorship analysis and long-term results. J. Bone Jt. Surg. Am. Vol. 1997, 79, 1352–1360. [Google Scholar] [CrossRef] [PubMed]
- Varnum, C.; Pedersen, A.B.; Kjærsgaard-Andersen, P.; Overgaard, S. Comparison of the risk of revision in cementless total hip arthroplasty with ceramic-on-ceramic and metal-on-polyethylene bearings: Data on 11,096 patients from the Danish Hip Arthroplasty Registry. Acta Orthop. 2015, 86, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Cuckler, J.M.; Moore, K.D.; Lombardi, A.V.; Jr McPherson, E.; Emerson, R. Large versus small femoral heads in metal-on-metal total hip arthroplasty. J. Arthroplast. 2004, 19, 41–44. [Google Scholar] [CrossRef]
- Drummond, J.; Tran, P.; Fary, C. Metal-on-Metal Hip Arthroplasty: A Review of Adverse Reactions and Patient Management. J. Funct. Biomater. 2015, 6, 486–499. [Google Scholar] [CrossRef]
- Silverman, E.J.; Ashley, B.; Sheth, N.P. Metal-on-metal total hip arthroplasty: Is there still a role in 2016? Curr. Rev. Musculoskelet. Med. 2016, 9, 93–96. [Google Scholar] [CrossRef]
- Pijls, B.G.; Meessen, J.; Schoones, J.W.; Fiocco, M.; van der Heide, H.J.L.; Sedrakyan, A.; Nelissen, R. Increased mortality in metal-on-metal versus non-metal-on-metal primary total hip arthroplasty at 10 years and longer follow-up: A systematic review and meta-analysis. Ned. Tijdschr. Geneeskd. 2017, 161, D1162. [Google Scholar] [CrossRef] [PubMed]
- Tsikandylakis, G.; Mohaddes, M.; Cnudde, P.; Eskelinen, A.; Kärrholm, J.; Rolfson, O. Head size in primary total hip arthroplasty. EFORT Open Rev. 2018, 3, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Holappa, E.; Kettunen, J.; Miettinen, H.; Kröger, H.; Miettinen, S. Long-term survival analysis of cementless large-diameter head metal-on-metal total hip arthroplasty. Arch. Orthop. Trauma Surg. 2022. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Bitar, C.; Moberg, I.; Krupic, F.; Wretenberg, P.; Otten, V.; Crnalic, S. 11-Year outcomes in patients with metal-on-metal ASR hip arthroplasty. J. Orthop. 2022, 32, 98–103. [Google Scholar] [CrossRef]
- Clough, E.J.; Clough, T.M. Metal on metal hip resurfacing arthroplasty: Where are we now? J. Orthop. 2021, 23, 123–127. [Google Scholar] [CrossRef]
- Jensen, C.; Aagaard, P.; Overgaard, S. Recovery in mechanical muscle strength following resurfacing vs standard total hip arthroplasty—A randomised clinical trial. Osteoarthr. Cartil. 2011, 19, 1108–1116. [Google Scholar] [CrossRef]
- Lavigne, M.; Therrien, M.; Nantel, J.; Roy, A.; Prince, F.; Vendittoli, P.A. The John Charnley Award: The functional outcome of hip resurfacing and large-head THA is the same: A randomized, double-blind study. Clin. Orthop. Relat. Res. 2010, 468, 326–336. [Google Scholar] [CrossRef]
- Mont, M.A.; Seyler, T.M.; Ragland, P.S.; Starr, R.; Erhart, J.; Bhave, A. Gait analysis of patients with resurfacing hip arthroplasty compared with hip osteoarthritis and standard total hip arthroplasty 231. J. Arthroplast. 2007, 22, 100–108. [Google Scholar] [CrossRef]
- Nantel, J.; Termoz, N.; Vendittoli, P.A.; Lavigne, M.; Prince, F. Gait patterns after total hip arthroplasty and surface replacement arthroplasty. Arch. Phys. Med. Rehabil. 2009, 90, 463–469. [Google Scholar] [CrossRef]
- Nantel, J.; Termoz, N.; Centomo, H.; Lavigne, M.; Vendittoli, P.A.; Prince, F. Postural balance during quiet standing in patients with total hip arthroplasty and surface replacement arthroplasty. Clin. Biomech. 2008, 23, 402–407. [Google Scholar] [CrossRef]
- Gerhardt, D.M.J.M.; Mors, T.G.T.; Hannink, G.; Van Susante, J.L.C. Resurfacing hip arthroplasty better preserves a normal gait pattern at increasing walking speeds compared to total hip arthroplasty. Acta Orthop. 2019, 90, 231–236. [Google Scholar] [CrossRef]
- Hjorth, M.H.; Stilling, M.; Lorenzen, N.D.; Jakobsen, S.S.; Soballe, K.; Mechlenburg, I. Block-step asymmetry 5 years after large-head metal-on-metal total hip arthroplasty is related to lower muscle mass and leg power on the implant side. Clin. Biomech. 2014, 29, 684–690. [Google Scholar] [CrossRef]
- World Medical Association. Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Elia, M.; Fuller, N.J.; Hardingham, C.R.; Graves, M.; Screaton, N.; Dixon, A.K.; Ward, L.C. Modeling leg sections by bioelectrical impedance analysis, dual-energy X-ray absorptiometry, and anthropometry: Assessing segmental muscle volume using magnetic resonance imaging as a reference 25. Ann. N. Y. Acad Sci. 2000, 904, 298–305. [Google Scholar] [CrossRef]
- Fuller, N.J.; Hardingham, C.R.; Graves, M.; Screaton, N.; Dixon, A.K.; Ward, L.C.; Elia, M. Assessment of limb muscle and adipose tissue by dual-energy X-ray absorptiometry using magnetic resonance imaging for comparison 28. Int. J. Obes. Relat. Metab. Disord. 1999, 23, 1295–1302. [Google Scholar] [CrossRef][Green Version]
- Villadsen, A.; Roos, E.M.; Overgaard, S.; Holsgaard-Larsen, A. Agreement and reliability of functional performance and muscle power in patients with advanced osteoarthritis of the hip or knee 2. Am. J. Phys. Med. Rehabil. 2012, 91, 401–410. [Google Scholar] [CrossRef]
- Mikkelsen, L.R.; Mikkelsen, S.; Søballe, K.; Mechlenburg, I.; Petersen, A.K. A study of the inter-rater reliability of a test battery for use in patients after total hip replacement. Clin. Rehabil. 2015, 29, 165–174. [Google Scholar] [CrossRef]
- Toft Nielsen, E.; Jørgensen, P.B.; Mechlenburg, I.; Sørensen, H. Validation of an inertial measurement unit to determine countermovement jump height. Asia-Pac. J. Sport. Med. Arthrosc. Rehabil. Technol. 2019, 16, 8–13. [Google Scholar] [CrossRef]
- Luinge, H.J.; Veltink, P.H. Measuring orientation of human body segments using miniature gyroscopes and accelerometers. Med. Biol. Eng. Comput. 2005, 43, 273–282. [Google Scholar] [CrossRef]
- Zijlstra, W.; Hof, A.L. Assessment of spatio-temporal gait parameters from trunk accelerations during human walking. Gait Posture 2003, 18, 1–10. [Google Scholar] [CrossRef]
- Bolink, S.A.; van Laarhoven, S.N.; Lipperts, M.; Heyligers, I.C.; Grimm, B. Inertial sensor motion analysis of gait, sit-stand transfers and step-up transfers: Differentiating knee patients from healthy controls 2. Physiol. Meas. 2012, 33, 1947–1958. [Google Scholar] [CrossRef]
- van den Akker-Scheek, I.; Stevens, M.; Bulstra, S.K.; Groothoff, J.W.; van Horn, J.R.; Zijlstra, W. Recovery of gait after short-stay total hip arthroplasty. Arch. Phys. Med. Rehabil. 2007, 88, 361–367. [Google Scholar] [CrossRef]
- Senden, R.; Grimm, B.; Heyligers, I.C.; Savelberg, H.H.; Meijer, K. Acceleration-based gait test for healthy subjects: Reliability and reference data. Gait Posture 2009, 30, 192–196. [Google Scholar] [CrossRef]
- Senden, R.; Heyligers, I.C.; Meijer, K.; Savelberg, H.; Grimm, B. Acceleration-based motion analysis as a tool for rehabilitation: Exploration in simulated functional knee limited walking conditions. Am. J. Phys. Med. Rehabil. 2011, 90, 226–232. [Google Scholar] [CrossRef]
- Jorgensen, P.B.; Bogh, S.B.; Kierkegaard, S.; Sorensen, H.; Odgaard, A.; Soballe, K.; Mechlenburg, I. The efficacy of early initiated, supervised, progressive resistance training compared to unsupervised, home-based exercise after unicompartmental knee arthroplasty: A single-blinded randomized controlled trial. Clin. Rehabil. 2017, 31, 61–70. [Google Scholar] [CrossRef]
- Kierkegaard, S.; Jorgensen, P.B.; Dalgas, U.; Soballe, K.; Mechlenburg, I. Pelvic movement strategies and leg extension power in patients with end-stage medial compartment knee osteoarthritis: A cross-sectional study. Arch. Orthop. Trauma Surg. 2015, 135, 1217–1226. [Google Scholar] [CrossRef]
- Harris, W.H. Traumatic Arthritis of the Hip after Dislocation and Acetabular Fractures: Treatment by Mold Arthroplasty: An End-Result Study Using a New Method of Result Evaluation. J. Bone Jt. Surg. Am. Vol. 1969, 51, 737–755. [Google Scholar] [CrossRef]
- Thorborg, K.; Holmich, P.; Christensen, R.; Petersen, J.; Roos, E.M. The Copenhagen Hip and Groin Outcome Score (HAGOS): Development and validation according to the COSMIN checklist. Br. J. Sport. Med. 2011, 45, 478–491. [Google Scholar] [CrossRef]
- Nilsdotter, A.; Bremander, A. Measures of hip function and symptoms: Harris Hip Score (HHS), Hip Disability and Osteoarthritis Outcome Score (HOOS), Oxford Hip Score (OHS), Lequesne Index of Severity for Osteoarthritis of the Hip (LISOH), and American Academy of Orthopedic Surgeons (AAOS) Hip and Knee Questionnaire. Arthritis Care Res. 2011, 63 (Suppl. S11), S200–S207. [Google Scholar]
- Altman, D.G. Practical Statistics for Medical Research; Chapman & Hall: London, UK, 2009. [Google Scholar]
- Loureiro, A.; Mills, P.M.; Barrett, R.S. Muscle weakness in hip osteoarthritis: A systematic review. Arthritis Care Res. 2013, 65, 340–352. [Google Scholar] [CrossRef]
- Skelton, D.A.; Greig, C.A.; Davies, J.M.; Young, A. Strength, power and related functional ability of healthy people aged 65–89 years 12. Age Ageing 1994, 23, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Marsh, A.P.; Miller, M.E.; Rejeski, W.J.; Hutton, S.L.; Kritchevsky, S.B. Lower extremity muscle function after strength or power training in older adults. J. Aging Phys. Act. 2009, 17, 416–443. [Google Scholar] [CrossRef] [PubMed]
- Pandit, H.; Glyn-Jones, S.; McLardy-Smith, P.; Gundle, R.; Whitwell, D.; Gibbons, C.L.; Ostlere, S.; Athanasou, N.; Gill, H.S.; Murray, D.W. Pseudotumours associated with metal-on-metal hip resurfacings. J. Bone Jt. Surg. Br. Vol. 2008, 90, 847–851. [Google Scholar] [CrossRef] [PubMed]
- Berber, R.; Khoo, M.; Cook, E.; Guppy, A.; Hua, J.; Miles, J.; Carrington, R.; Skinner, J.; Hart, A. Muscle atrophy and metal-on-metal hip implants: A serial MRI study of 74 hips. Acta Orthop. 2015, 86, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Parsons, T.M.; Satchithananda, K.; Berbe, R.; Siddiqui, I.A.; Robinson, E.; Hart, A.J. MRI investigations in patients with problems due to metal-on-metal implants. Orthopade 2013, 42, 629–636. [Google Scholar]
- Hayter, C.L.; Gold, S.L.; Koff, M.F.; Perino, G.; Nawabi, D.H.; Miller, T.T.; Potter, H.G. MRI findings in painful metal-on-metal hip arthroplasty. AJR Am. J. Roentgenol. 2012, 199, 884–893. [Google Scholar] [CrossRef]
- Toms, A.P.; Marshall, T.J.; Cahir, J.; Darrah, C.; Nolan, J.; Donell, S.T.; Barker, T.; Tucker, J.K. MRI of early symptomatic metal-on-metal total hip arthroplasty: A retrospective review of radiological findings in 20 hips. Clin. Radiol. 2008, 63, 49–58. [Google Scholar] [CrossRef]
- Rasch, A.; Byström, A.H.; Dalén, N.; Martinez-Carranza, N.; Berg, H.E. Persisting muscle atrophy two years after replacement of the hip. J. Bone Jt. Surg. Br. Vol. 2009, 91-B, 583–588. [Google Scholar] [CrossRef]
- Foucher, K.C.; Hurwitz, D.E.; Wimmer, M.A. Do gait adaptations during stair climbing result in changes in implant forces in subjects with total hip replacements compared to normal subjects? Clin. Biomech. 2008, 23, 754–761. [Google Scholar] [CrossRef]
- Varnum, C.; Pedersen, A.B.; Kjærsgaard-Andersen, P.; Overgaard, S. Do different types of bearings and noise from total hip arthroplasty influence hip-related pain, function, and quality of life postoperatively?: A cross-sectional study from the Danish Hip Arthroplasty Registry. Acta Orthop. 2016, 87, 567–574. [Google Scholar] [CrossRef]
- Kasper, J.D.; Chan, K.S.; Freedman, V.A. Measuring Physical Capacity. J. Aging Health 2017, 29, 289–309. [Google Scholar] [CrossRef]
- Dempsey, K.; Collins, J.; Ghazinouri, R.; Alcantara, L.; Thornhill, T.; Katz, J. Associations between preoperative functional status and functional outcomes of total joint replacement in the Dominican Republic. Rheumatology 2013, 52, 1802–1808. [Google Scholar] [CrossRef]
- Raad, M.; Amin, R.M.; El Abiad, J.M.; Puvanesarajah, V.; Best, M.J.; Oni, J.K. Preoperative Patient Functional Status Is an Independent Predictor of Outcomes After Primary Total Hip Arthroplasty. Orthopedics 2019, 42, e326–e330. [Google Scholar] [CrossRef]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; et al. Pitfalls in the measurement of muscle mass: A need for a reference standard. J. Cachexia Sarcopenia Muscle 2018, 9, 269–278. [Google Scholar] [CrossRef]
- Kovalak, E.; Özdemir, H.; Ermutlu, C.; Obut, A. Assessment of hip abductors by MRI after total hip arthroplasty and effect of fatty atrophy on functional outcome. Acta Orthop. Traumatol. Turc. 2018, 52, 196–200. [Google Scholar] [CrossRef]
- Vadalà, A.P.; Mazza, D.; Desideri, D.; Iorio, R.; Fedeli, G.; Scrivano, M.; Serlorenzi, P.; Ferretti, A. Could the tendon degeneration and the fatty infiltration of the gluteus medius affect clinical outcome in total hip arthroplasty? Int. Orthop. 2020, 44, 275–282. [Google Scholar] [CrossRef]
- Klemt, C.; Simeone, F.J.; Melnic, C.M.; Tirumala, V.; Xiong, L.; Kwon, Y.-M. MARS MRI assessment of fatty degeneration of the gluteal muscles in patients with THA: Reliability and accuracy of commonly used classification systems. Skeletal Radiol. 2021, 50, 665–672. [Google Scholar] [CrossRef]
- Petis, S.; Howard, J.L.; Lanting, B.L.; Vasarhelyi, E.M. Surgical approach in primary total hip arthroplasty: Anatomy, technique and clinical outcomes. Can. J. Surg. J. Can. Chir. 2015, 58, 128–139. [Google Scholar] [CrossRef]
- Winther, S.B.; Husby, V.S.; Foss, O.A.; Wik, T.S.; Svenningsen, S.; Engdal, M.; Haugan, K.; Husby, O.S. Muscular strength after total hip arthroplasty. A prospective comparison of 3 surgical approaches. Acta Orthop. 2016, 87, 22–28. [Google Scholar] [CrossRef]
- Palan, J.; Beard, D.J.; Murray, D.W.; Andrew, J.G.; Nolan, J. Which approach for total hip arthroplasty: Anterolateral or posterior? Clin. Orthop. Relat. Res. 2009, 467, 473–477. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Articulation | MoM THA/HRA | MoP THA | p-Value a |
|---|---|---|---|
| Number of patients | 51 | 23 | - |
| Sex (male/female) | 33/18 | 8/15 | 0.02 |
| Age at follow-up, mean (range) | 56 (30–71) | 67 (45–77) | 0.00 |
| Years since operation, mean (range) | 5.8 (2.4–9.0) | 8.5 (6–12.5) | 0.00 |
| BMI (kg/m2) (range) | 23.7 (17–34) | 22.6 (16–30) | 0.20 |
| Implant side, right/left | 31/20 | 11/12 | 0.30 |
| Region of Interest (ROI) | MoM THA/HRA | MoP THA | p-Value |
|---|---|---|---|
| Hip area (g/cm2) | |||
| Implant side | 9.44 (1.50) | 8.98 (1.59) | 0.24 b |
| Non-implant side | 10.63 (1.57) | 9.78 (1.55) | 0.04 b |
| Inter-limb difference | 1.28 (0.71) | 0.92 (0.47) | 0.02 a |
| Thigh area (g/cm2) | |||
| Implant side | 6.96 (1.19) | 5.83 (1.28) | 0.0004 b |
| Non-implant side | 7.13 (1.26) | 6.04 (1.22) | 0.0008 b |
| Inter-limb difference | 0.38 (0.33) | 0.41 (0.40) | 0.71 a |
| Hip and thigh area (g/cm2) | |||
| Implant side | 7.88 (1.15) | 6.71 (1.39) | 0.0003 b |
| Non-implant side | s8.35 (1.18) | 7.20 (1.58) | 0.0008 b |
| Inter-limb difference | 0.51 (0.34) | 0.54 (0.37) | 0.76 a |
| Calf area (g/cm2) | |||
| Implant side | 3.63 (0.53) | 3.35 (1.01) | 0.0038 b |
| Non-implant side | 3.69 (0.49) | 3.47 (1.07) | 0.0097 b |
| Inter-limb difference | 0.29 (0.21) | 0.18 (0.12) | 0.06 a |
| MoM THA/RHA | MoP THA | p-Value a | |
|---|---|---|---|
| Power (W/kg) | |||
| Implant side | 1.98 (0.67) | 1.29 (0.50) | 0.000 |
| Non-implant side | 2.02 (0.69) | 1.50 (0.50) | 0.002 |
| Inter-limb difference | 0.24 (0.18) | 0.23 (0.18) | 0.87 |
| Power (W) | |||
| Implant side | 164.06 (61.55) | 100.96 (45.19) | 0.000 |
| Non-implant side | 168.08 (62.41) | 115.78 (43.71) | 0.0003 |
| Inter-limb difference | 19.18 (14.47) | 17.35 (11.79) | 0.75 |
| HHS | |||
| Score | 97.7 (4.2) | 96.6 (5.2) | 0.26 |
| HAGOS | |||
| Symptoms | 90.5 (13.0) | 84.8 (16.9) | 0.18 |
| Pain | 93.9 (10.2) | 85.3 (21.9) | 0.07 |
| Function in Daily Living | 91.7 (15.6) | 85.9 (18.7) | 0.08 |
| Sport and recreation | 83.8 (20.5) | 72.9 (27.1) | 0.08 |
| Physical Activities | 78.9 (29.4) | 79.4 (26.6) | 0.99 |
| Hip related Quality of Life | 81.8 (21.3) | 77.4 (26.5) | 0.68 |
| IMU Parameters | MoM THA/HRA | MoP THA | p-Value a |
|---|---|---|---|
| Step test rotation asymmetry | |||
| Sagital plane descending (%) | 15.93 (14.86) | 19.24 (11.64) | 0.17 |
| Sagital plane ascending (%) | 19.98 (16.08) | 19.12 (14.74) | 0.95 |
| Frontal plane descending (%) | 17.30 (13.37) | 14.68 (13.34) | 0.39 |
| Frontal plane ascending (%) | 13.78 (11.29) | 15.24 (12.49) | 0.65 |
| Step test time asymmetry | |||
| Ascending (%) | 11.60 (8.53) | 20.60 (16.29) | 0.03 |
| Descending (%) | 13.13 (10.61) | 18.81 (14.72) | 0.19 |
| Step test acceleration asymmetry | |||
| Vertical plane ascending (%) | 12.97 (11.38) | 16.64 (15.13) | 0.46 |
| Sagital plane ascending (%) | 17.29 (14.36) | 18.30 (20.39) | 0.56 |
| Frontal plane ascending (%) | 18.07 (13.04) | 21.68 (12.91) | 0.32 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hjorth, M.H.; Mechlenburg, I.; Foldager, F.N.; Tjur, M.; Stilling, M. A Comparison of Hip Muscle Mass, Muscle Power, and Clinical Outcomes with Long-Term Follow-Up in Patients with Metal-on-Metal Hip Arthroplasty Compared to Metal-on-Polyethylene Hip Arthroplasty. Appl. Sci. 2022, 12, 12772. https://doi.org/10.3390/app122412772
Hjorth MH, Mechlenburg I, Foldager FN, Tjur M, Stilling M. A Comparison of Hip Muscle Mass, Muscle Power, and Clinical Outcomes with Long-Term Follow-Up in Patients with Metal-on-Metal Hip Arthroplasty Compared to Metal-on-Polyethylene Hip Arthroplasty. Applied Sciences. 2022; 12(24):12772. https://doi.org/10.3390/app122412772
Chicago/Turabian StyleHjorth, Mette Holm, Inger Mechlenburg, Frederik Nicolai Foldager, Marianne Tjur, and Maiken Stilling. 2022. "A Comparison of Hip Muscle Mass, Muscle Power, and Clinical Outcomes with Long-Term Follow-Up in Patients with Metal-on-Metal Hip Arthroplasty Compared to Metal-on-Polyethylene Hip Arthroplasty" Applied Sciences 12, no. 24: 12772. https://doi.org/10.3390/app122412772
APA StyleHjorth, M. H., Mechlenburg, I., Foldager, F. N., Tjur, M., & Stilling, M. (2022). A Comparison of Hip Muscle Mass, Muscle Power, and Clinical Outcomes with Long-Term Follow-Up in Patients with Metal-on-Metal Hip Arthroplasty Compared to Metal-on-Polyethylene Hip Arthroplasty. Applied Sciences, 12(24), 12772. https://doi.org/10.3390/app122412772