
A Workflow for Dosimetry of 90Y Radioembolization Based on Quantitative 99mTc-MAA SPECT/CT Imaging and a 3D-Printed Phantom

 , , , and
, , , and
Abstract
1. Introduction
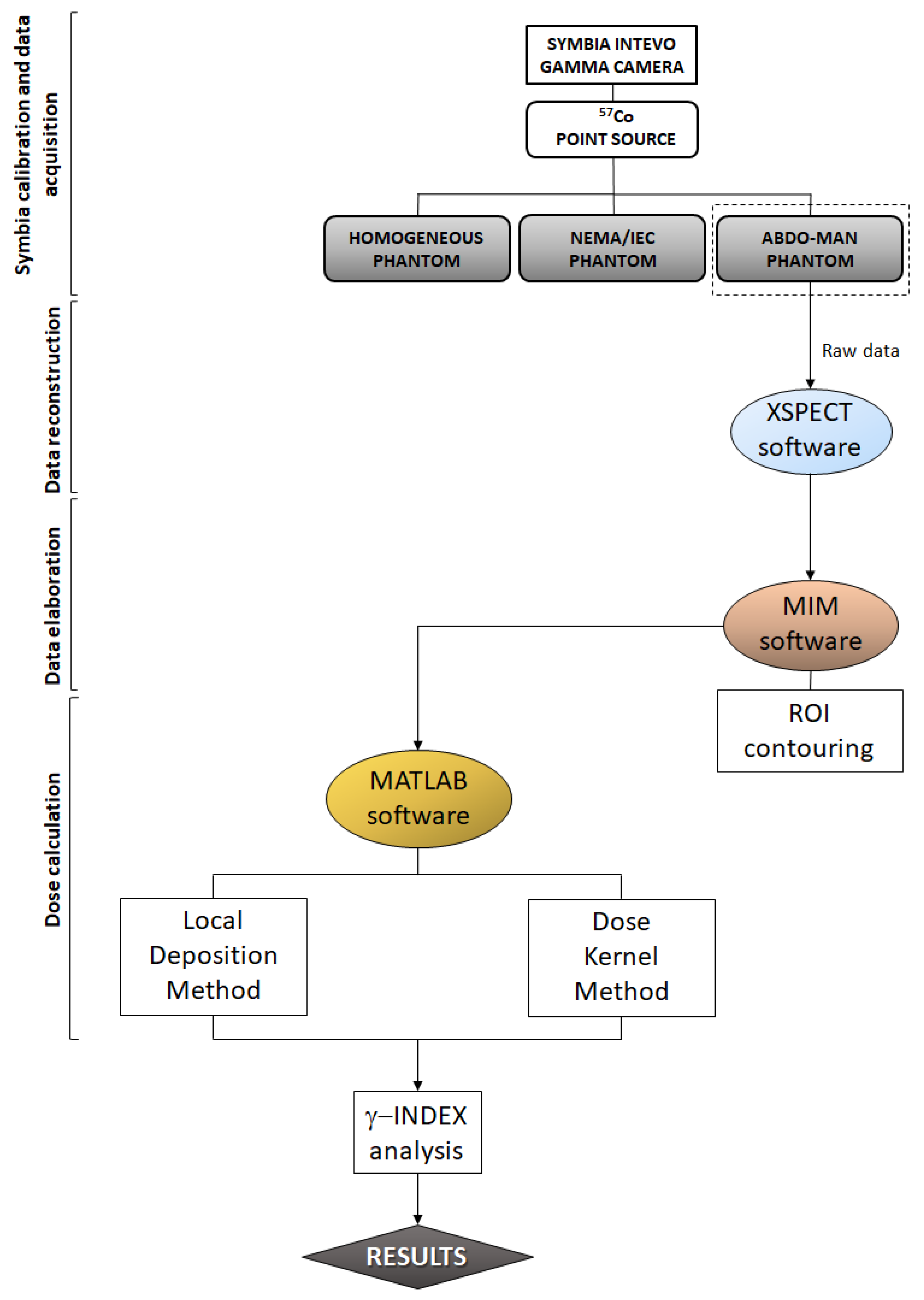
2. Materials and Methods
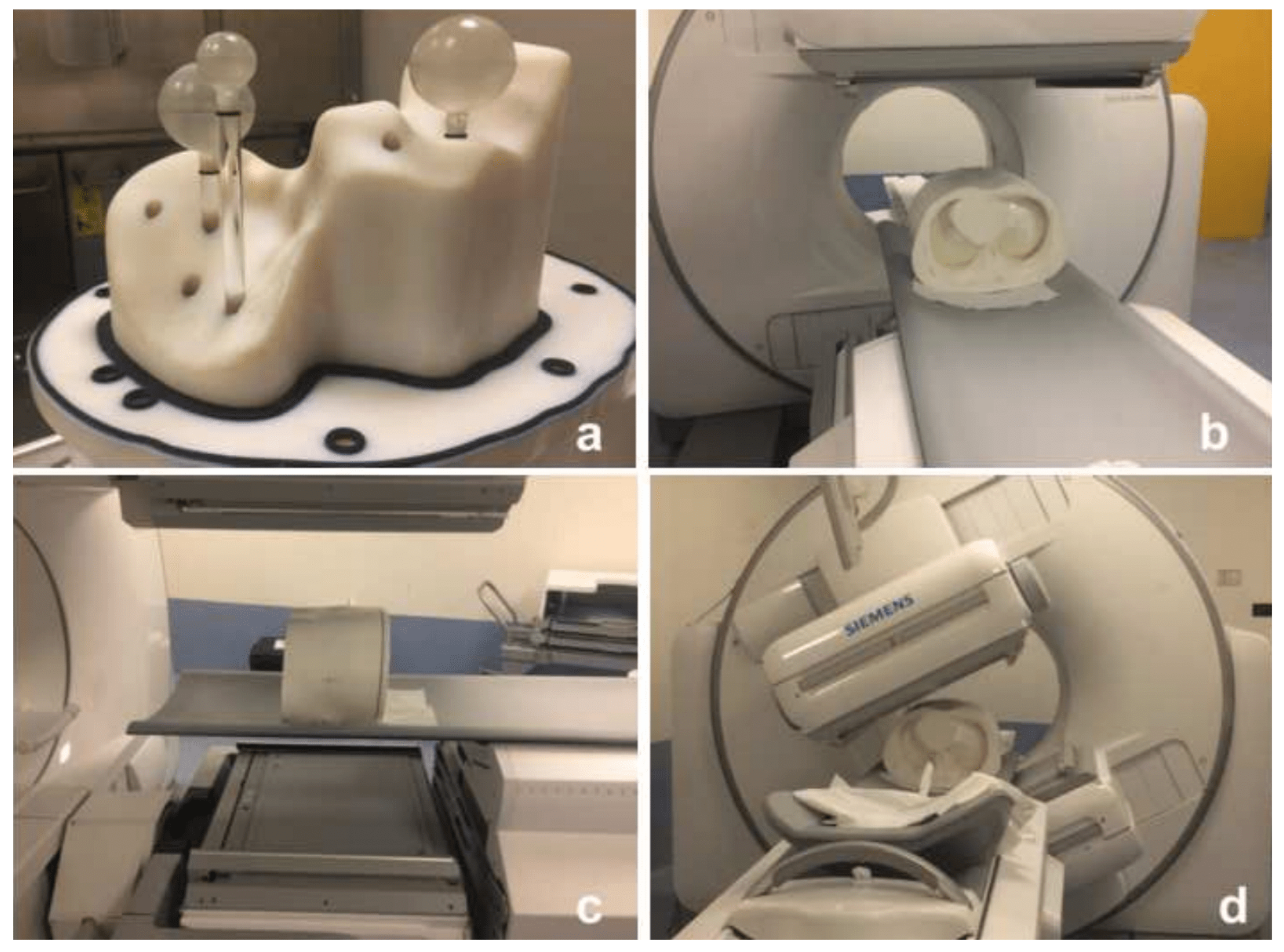
2.1. Data Acquisition and Reconstruction
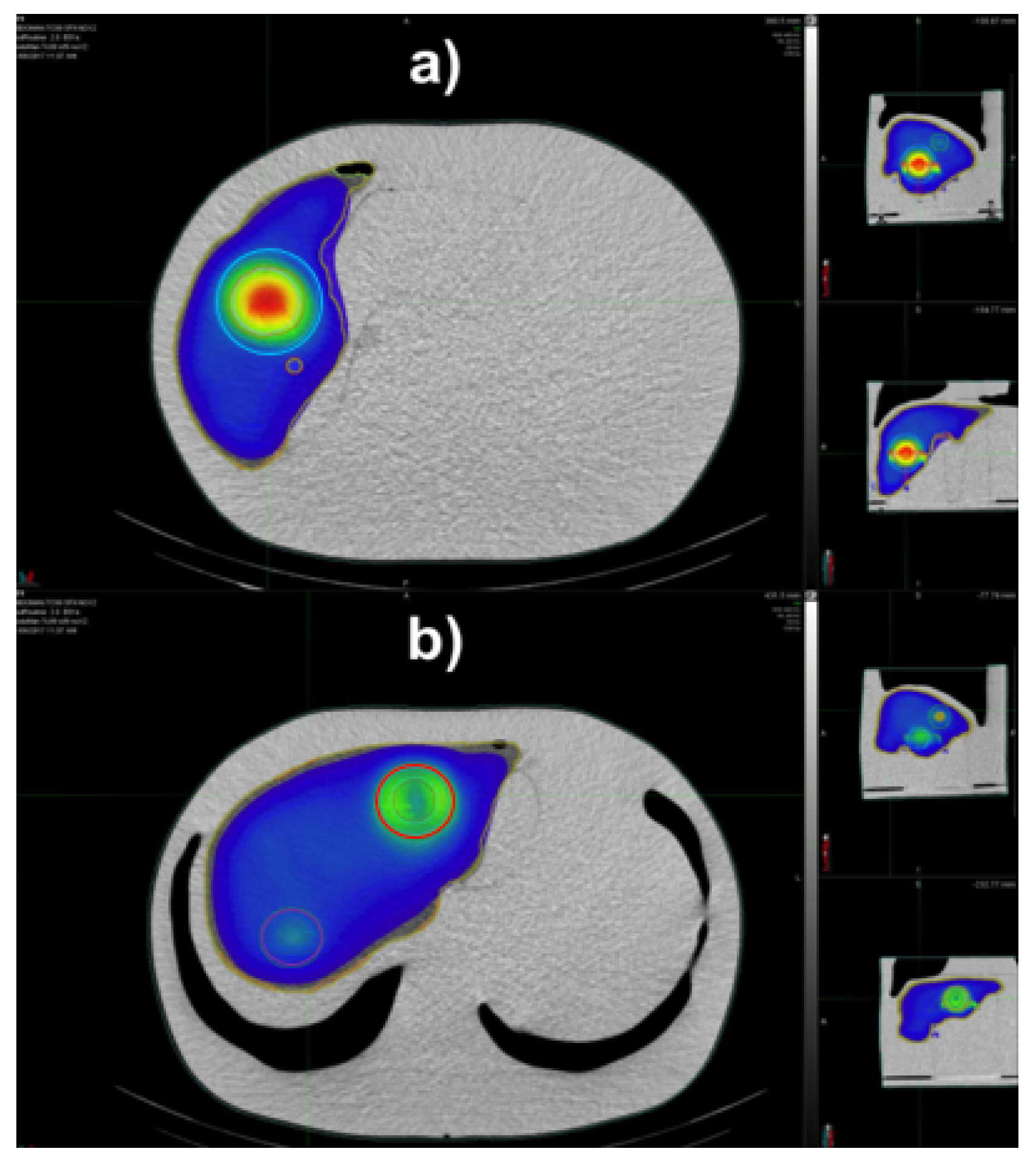
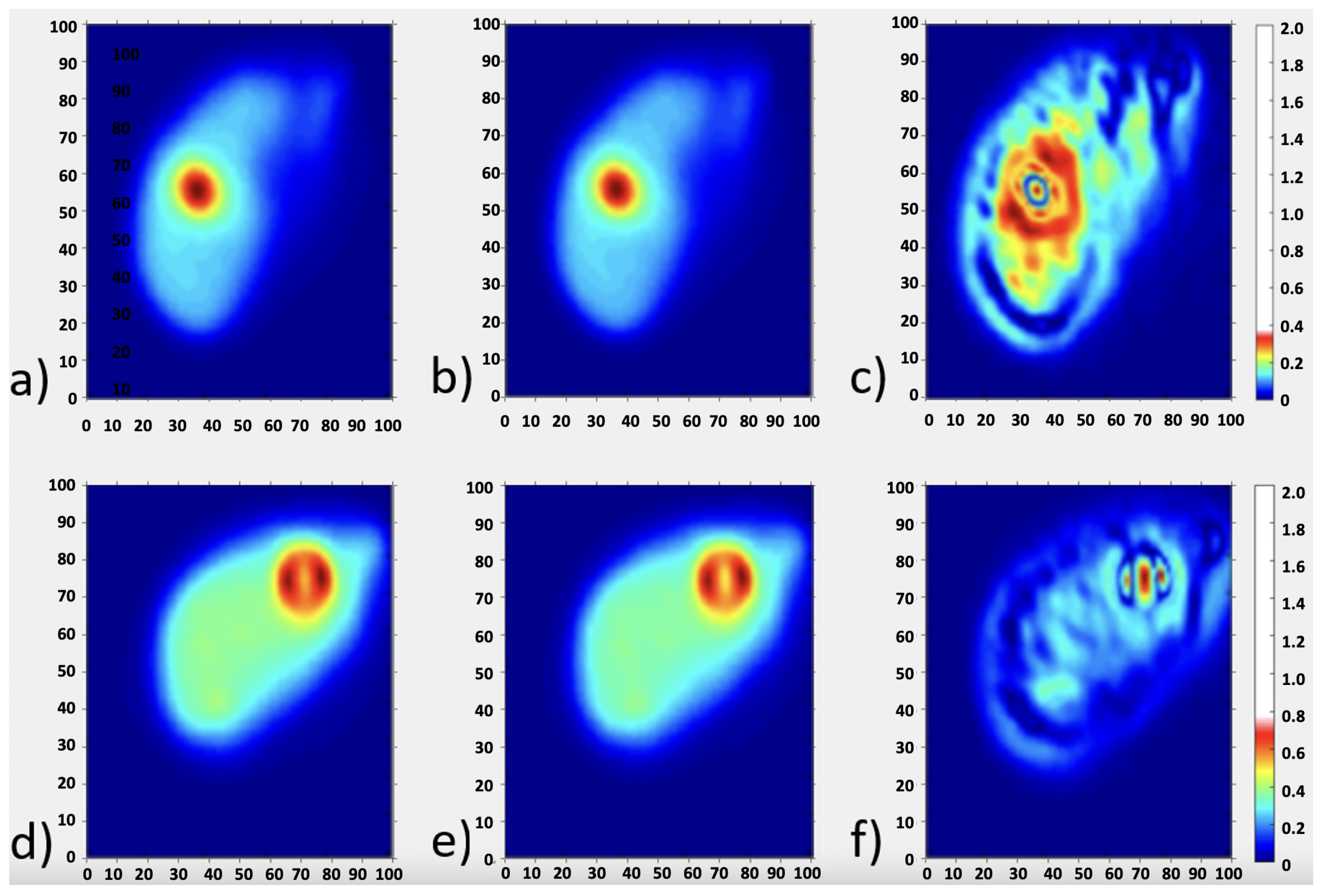
2.2. Image Segmentation, Dose Calculation and Data Comparison
3. Results
4. Discussion
4.1. Role of Predictive Dosimetry with 99mTc-MAA SPECT
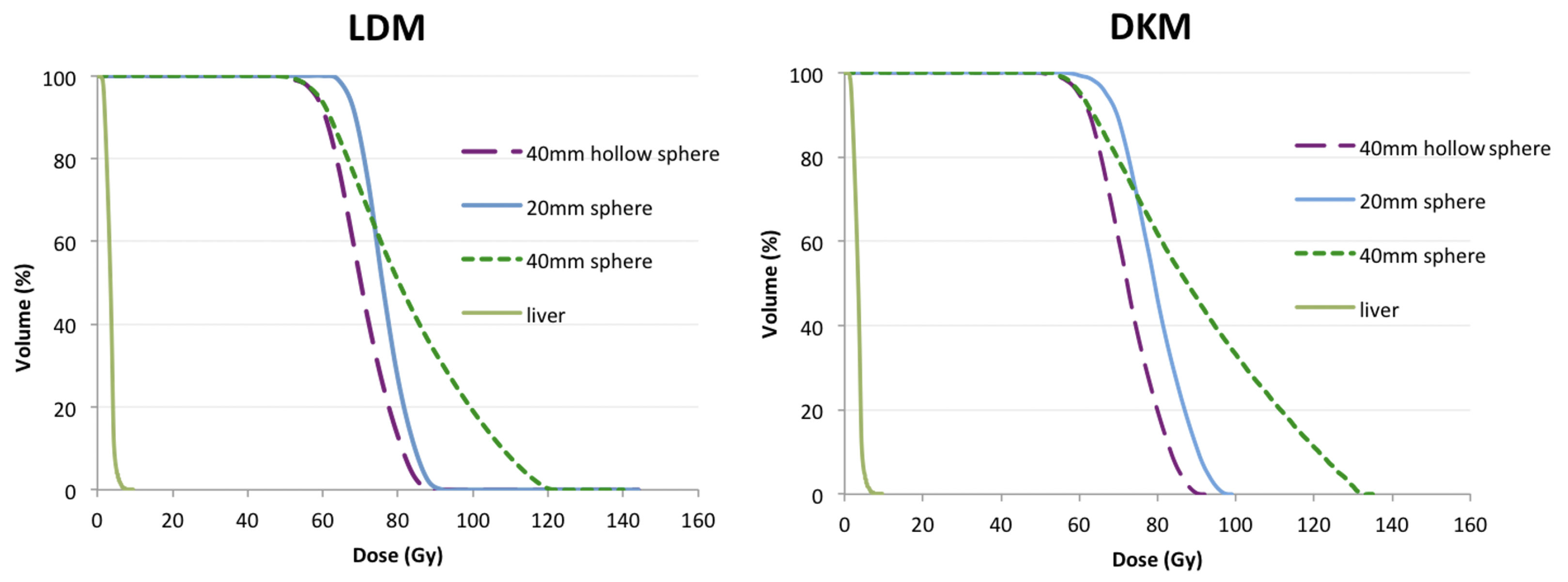
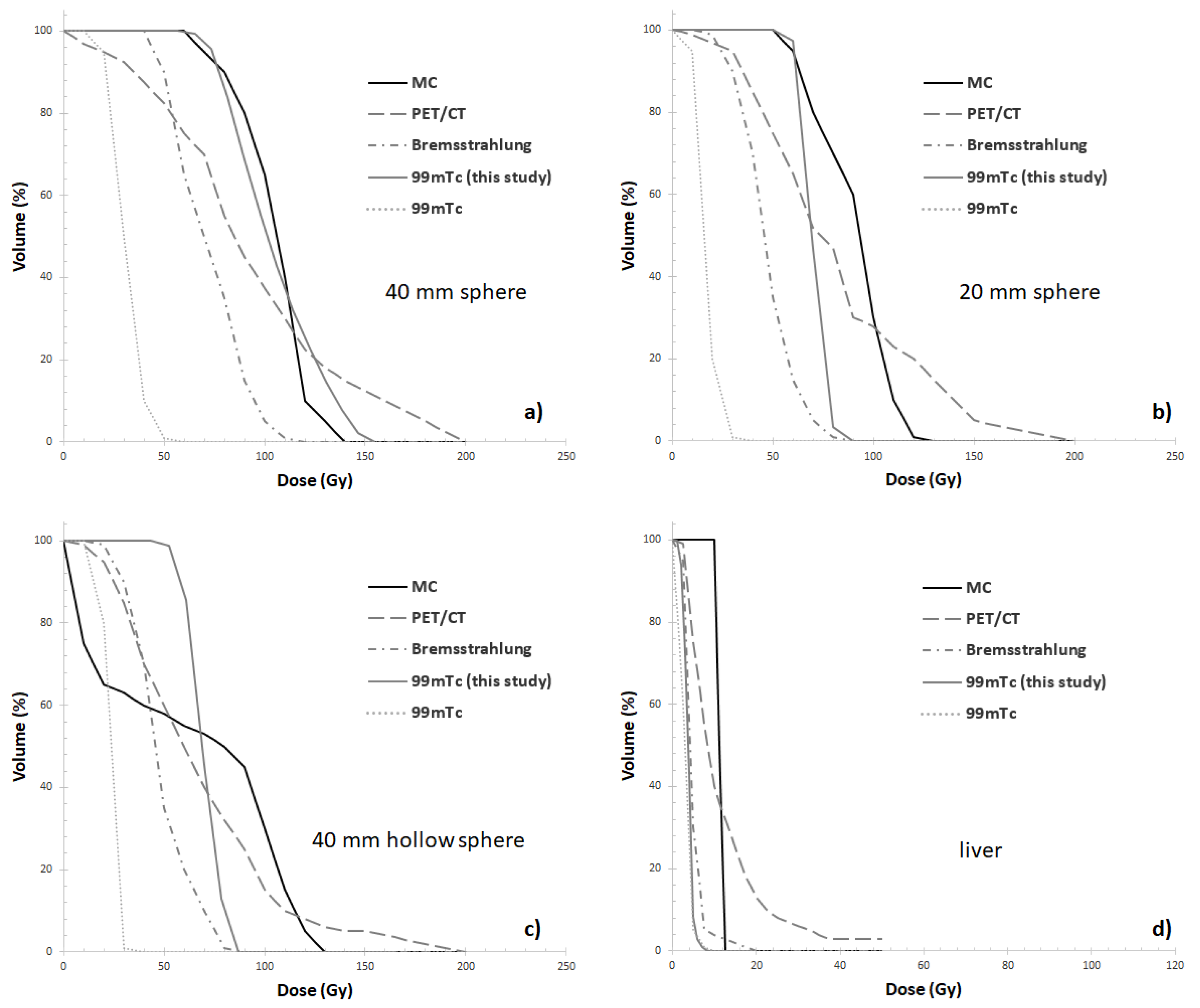
4.2. DVH Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| RE | Radioembolization |
| SPECT | Single Photon Emission Computed Tomography |
| OSEM | Ordered Subset Expectation Maximization |
| CT | Computed Tomography |
| VOI | Volume of Interest |
| PET | Positron Emission Tomography |
| MAA | Macroaggregated Albumin |
| DKM | dose kernel method |
| LDM | local energy deposition method |
| DVHs | dose volume histograms |
| s | microspheres |
| EBRT | External Beam Radiotherapy |
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in globocan 2012. Int. J. Cancer 2015, 5, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ren, J.S.; Masuyer, E.; Ferlay, J. Estimates of global cancer prevalence for 27 sites in the adult population in 2008. Int. J. Cancer 2013, 132, 1133–1145. [Google Scholar] [CrossRef] [PubMed]
- Altekruse, S.F.; McGlynn, K.A.; Reichman, M.E. Hepatocellular carcinoma (hcc) incidence, mortality, and survival trends in the united states from 1975 to 2005. J. Clin. Oncol. 2009, 27, 1485–1491. [Google Scholar] [CrossRef] [PubMed]
- Zurkiya, O.; Ganguli, S. Beyond hepatocellular carcinoma and colorectal metastasis: The expanding applications of radioembolization. Front. Oncol. 2014, 150, 2850. [Google Scholar] [CrossRef]
- Sato, K.T.; Lewandowski, R.J.; Mulcahy, M.F.; Atassi, B.; Ryu, R.K.; Gates, V.L.; Nemcek, A.A.; Barajat, O.; Benson, A.; Mandal, R.; et al. Unresectable chemorefractory liver metastases: Radioembolization with 90Y microspheressafety, efficacy, and survival. Radiology 2008, 247, 507–515. [Google Scholar] [CrossRef]
- Cutsem, E.V.; Cervantes, A.; Adam, R.; Sobrero, A.; Krieken, J.H.V.; Aderka, D.; Aguilar, E.A.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. Esmo consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef]
- Ahmadzadehfar, H.; Sabet, A.; Biermann, K.; Muckle, M.; Brockmann, H.; Kuhl, C.; Wilhelm, K.; Biersack, H.-J.; Ezzidin, S. The significance of 99mTc SPECT/CT liver perfusion imaging in treatment planning for 90Y-microsphere selective internal radiation treatment. J. Nucl. Med. 2009, 51, 1206–1212. [Google Scholar] [CrossRef]
- Sato, K.; Lewandowski, R.J.; Bui, J.T.; Omary, R.; Hunter, R.D.; Kulik, L.; Mulcahy, M.; Chrisman, H.; Nemcek, A.A.; Vogelzang, R.; et al. Treatment of unresectable primary andmetastatic liver cancer with yttrium-90 microspheres (TheraSphere): Assessment of hepatic arterial embolization. Cardiovasc. Intervent. Radiol. 2006, 29, 522–529. [Google Scholar] [CrossRef]
- Lam, M.G.; Goris, M.L.; Iagaru, A.H.; Mittra, E.S.; Louie, J.D.; Sze, D.Y. Prognostic utility of 90Y radioembolization dosimetry based on fusion 99mTc macroaggregated albumin-99mTc-sulfur colloid spect. J. Nucl. Med. 2013, 12, 2055–2061. [Google Scholar] [CrossRef]
- Garin, E.; Rolland, Y.; Lenoir, L. Utility of quantitative 99mTc SPECT/CT for yttrium labelled microsphere treatment planning: Calculating vascularized hepatic volume and dosimetric approach. Int. J. Mol. Imaging 2011, 2011, 51. [Google Scholar] [CrossRef]
- Hamami, M.E.; Poeppel, T.D.; Muller, S.; Heusner, T.; Bockisch, A.; Hilgard, P.; Antoch, G. Spect/ct with 99mTc-MAA in radioembolization with 90y microspheres in patients with hepatocellular cancer. J. Nucl. Med. 2009, 50, 688–692. [Google Scholar] [CrossRef] [PubMed]
- Srinivas, S.; Shrikanthan, S.; Yu, N.; Kost, S.; Gurajala, R.; Karuppasamy, K. Treatment Planning Part Thesis Ii: Procedure Simulation And Prognostication. In Handbook of Radioembolization: Physics, Biology, Nuclear Medicine, and Imaging; Pasciak, A., McKinney, J., Bradleyed, Y., Eds.; CRC Press/Taylor & Francis: Boca Raton, CA, USA, 2017; p. 70. [Google Scholar]
- Kao, Y.H.; Tan, A.E.H.; Burgmans, M.C.; Irani, F.G.; Khoo, L.S.; Lo, R.H.G.; Tay, K.H.; Tan, B.S.; Chow, P.K.; Eng, D.C.; et al. Image-guided personalized predictive dosimetry by artery-specific SPECT/CT partition modeling for safe and effective 90Y radioembolization. J. Nucl. Med. 2012, 53, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Strigari, L.; Sciuto, R.; Rea, S.; Carpanese, L.; Pizzi, G.; Soriani, A.; Iaccarino, G.; Benassi, M.; Ettorre, G.M.; Maini, C.L. Efficacy and toxicity related to treatment of hepatocellular carcinoma with 90y-sir spheres: Radiobiologic considerations. J. Nucl. Med. 2010, 9, 1377–1385. [Google Scholar] [CrossRef]
- European Council. Directive 2013/59/Euratom on basic safety standards for protection against the dangers arising from exposure to ionizing radiation and repealing Directives 89/618/Euratom, 90/641/Euratom, 96/29/Euratom, 97/43/Euratom and2003/122/Euratom. Off. J. Eur. Union 2013, L13, 1–73. Available online: http://data.europa.eu/eli/dir/2013/59/oj (accessed on 21 September 2021).
- Dewaraja, Y.K.; Frey, E.C.; Sgouros, G.; Brill, A.B.; Roberson, P.; Zanzonico, P.B.; Ljunberg, M. MIRD pamphlet no. 23: Quantitative spect for patient-specific 3-dimensional dosimetry in internal radionuclide therapy. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2012, 8, 1310–1325. [Google Scholar] [CrossRef]
- Pasciak, A.S.; Bourgeois, A.C.; Bradley, Y.C. A comparison of techniques for 90Y PET/CT image-based dosimetry following radioembolization with resin microspheres. Front. Oncol. 2014, 4, 121. [Google Scholar] [CrossRef]
- Ljungberg, M.; Gleisner, K.S. Personalized dosimetry for radionuclide therapy using molecular imaging tools. Biomedicines 2016, 4, 25. [Google Scholar] [CrossRef]
- Ljungberg, M.; Sjogreen-Gleisner, K. The accuracy of absorbed dose estimates in tumours determined by quantitative spect: A monte carlo study. Acta Oncol. 2011, 6, 981–989. [Google Scholar] [CrossRef] [PubMed]
- Garin, E.; Rolland, Y.; Ladffont, S.; Edelin, J. Clinical impact of 99mTc-MAA SPECT/CT-based dosimetry in the radioembolization of liver malignancies with 90Y-loaded microsphere. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 559–575. [Google Scholar] [CrossRef]
- Veenstra, E.B.; Ruiter, S.J.S.; de Haas, R.J.; Bokkers, R.P.H.; Jong, K.P.D.; Noordzij, W. Post-treatment three-dimensional voxel-based dosimetry after Yttrium-90 resin microsphere radioembolization in HCC. Eur. J. Nucl. Med. Mol. Imaging 2022, 12, 9. [Google Scholar] [CrossRef]
- Gear, J.; Cummings, C.; Craig, A.J.; Divoli, A.; Long, C.D.C.; Tapner, M.; Flux, G.D. Abdoman: A 3D-printed anthropomorphic phantom for validating quantitative SIRT. EJNMMI Phys. 2016, 3, 17. [Google Scholar] [CrossRef] [PubMed]
- American Association of Physicists in Medicine. The Selection, Use, Calibration, and Quality Assurance of Radionuclide Calibrators Used in Nuclear Medicine; Report of AAPM Task Group 181; American Association of Physicists in Medicine: College Park, MD, USA, 2012. [Google Scholar]
- D’Arienzo, M.; Cox, M. Uncertainty Analysis in the Calibration of an Emission Tomography System for Quantitative Imaging. Comput. Math. Methods Med. 2017, 9, 9830386. [Google Scholar] [CrossRef] [PubMed]
- D’Arienzo, M.; Cazzato, M.; Cozzella, M.L.; Cox, M.; Ungania, S.; Fazio, A.; Fenwick, A.; Iaccarino, G.; Johansson, L.; Strigari, L.; et al. Gamma camera calibration and validation for quantitative spect imaging with (177)lu. Appl. Radiat. Isotop. 2016, 112, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Ungania, S.; Nocentini, S.; Iaccarino, G.; D’Andrea, M.; D’Arienzo, M.; Cacciatore, A.; Sciuto, R.; Vallati, G.E.; Pizzi, G.; Strigari, L.; et al. [OA165] Optimization of quantitative 99MTC-MAA SPECT/CT imaging for 90Y radioembolization: A 3D-printed phantom study. Phys. Med. 2018, 52, 10022. [Google Scholar] [CrossRef]
- Strigari, L.; Menghi, E.; D’Andrea, M.; Benassi, M. Monte Carlo dose voxel kernel calculations of beta-emitting and Auger-emitting radionuclides for internal dosimetry: A comparison between EGSnrcMP and EGS4. Med. Phys. 2006, 33, 3383–3389. [Google Scholar] [CrossRef]
- D’Arienzo, M.; Pimpinella, M.; Capogni, M.; Coste, V.D.; Filippi, L.; Spezi, E.; Patterson, N.; Mariotti, F.; Ferrari, P.; Chiaramida, P.; et al. Phantom validation of quantitative Y-90 PET/CT-based dosimetry in liver radioembolization. EJNMMI Res. 2017, 7, 1. [Google Scholar] [CrossRef]
- Low, D.A.; Dempsey, J.F. Evaluation of the gamma dose distribution comparison method. Med. Phys. 2003, 30, 156–164. [Google Scholar] [CrossRef]
- Maughan, N.M.; Garcia-Ramirez, J.; Arpidone, M.; Swallen, A.; Laforest, R.; Goddu, S.M.; Parikh, P.J.; Zoberi, J.E. Validation of Post-Treatment PET-Based Dosimetry Software for Hepatic Radioembolization of Yttrium-90 Microspheres. Med Phys. 2019, 46, 2394–2402. [Google Scholar] [CrossRef]
- D’Arienzo, M.; Filippi, L.; Chiaramida, P.; Cianni, R.; Salvatori, R.; Scopinaro, F.; Bagni, O. Absorbed dose to lesion and clinical outcome after liver radioembolization with 90Y microspheres: A case report of PET-based dosimetry. Ann. Nucl. Med. 2013, 27, 676–680. [Google Scholar] [CrossRef]
- D’Arienzo, M. Dosimetry by 90Y internal pair production PET imaging after liver radioembolization: How well can we quantify the absorbed dose to lesions? Nuov. Cim. 2017, 40C, 97. [Google Scholar]
- Chiesa, C.; Sjogreen-Gleisner, K.; Walrand, S.; Strigari, L.; Flux, G.; Gear, J.; Stokke, C.; Gabina, M.; Bernhardt, P.; Konijnenberg, M. EANM dosimetry committee series on standard operational procedures: A unified methodology for 99mTc-MAA pre- and 90Y peri-therapy dosimetry in liver radioembolization with 90Y microspheres. EJNMMI Phys. 2021, 8, 394. [Google Scholar] [CrossRef] [PubMed]
- Läppchen, T.; Meier, L.; Fürstner, M.; Prenosil, G.; Krause, T.; Rominger, A.; Klaeser, B.; Hentschel, M. 3D printing of radioactive phantoms for nuclear medicine imaging. EJNMMI Phys. 2020, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Tran-Gia, J.; Schlögl, S.; Lassmann, M. Design and Fabrication of Kidney Phantoms for Internal Radiation Dosimetry Using 3D Printing Technology. J. Nucl. Med. 2016, 57, 1998–2005. [Google Scholar] [CrossRef] [PubMed]
- Green, S.; Grice, J. Technical note: 3D-printed phantom for dedicated cardiac protocols and geometries in nuclear medicine. Med. Phys. 2021, 49, 943–951. [Google Scholar] [CrossRef] [PubMed]
- Okkalidis, N. 3D printing methods for radiological anthropomorphic phantoms. Phys. Med. Biol. 2022, 67, 15TR04. [Google Scholar] [CrossRef]
- Tino, R.; Yeo, A.; Leary, M.; Brandt, M.; Kron, T. A Systematic Review on 3D-Printed Imaging and Dosimetry Phantoms in Radiation Therapy. Technol. Cancer Res. Treat. 2019, 18, 153303381987020. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Abdoman | (MBq/mL) | (MBq/mL) | |
|---|---|---|---|
| 20 mm sphere | 0.530 | 0.510 | −3.8% |
| 40 mm sphere | 0.530 | 0.540 | +1.9% |
| 40 mm hollow sphere | 0.530 | 0.390 | −26.4% |
| Liver compartment | 0.103 | 0.104 | +1.0% |
| AbdoMan | D-LDM | D-KDM | (%) |
|---|---|---|---|
| Liver | 4 Gy | 4 Gy | 0% |
| 40 mm sphere | 80 Gy | 87 Gy | 8.7% |
| 20 mm sphere | 76 Gy | 79 Gy | 4% |
| 40 mm hollow sphere | 70 Gy | 72 Gy | 2.4% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ungania, S.; D’Arienzo, M.; Mezzenga, E.; Pizzi, G.; Vallati, G.; Ianiro, A.; Rea, S.; Sciuto, R.; Soriani, A.; Strigari, L. A Workflow for Dosimetry of 90Y Radioembolization Based on Quantitative 99mTc-MAA SPECT/CT Imaging and a 3D-Printed Phantom. Appl. Sci. 2022, 12, 10541. https://doi.org/10.3390/app122010541
Ungania S, D’Arienzo M, Mezzenga E, Pizzi G, Vallati G, Ianiro A, Rea S, Sciuto R, Soriani A, Strigari L. A Workflow for Dosimetry of 90Y Radioembolization Based on Quantitative 99mTc-MAA SPECT/CT Imaging and a 3D-Printed Phantom. Applied Sciences. 2022; 12(20):10541. https://doi.org/10.3390/app122010541
Chicago/Turabian StyleUngania, Sara, Marco D’Arienzo, Emilio Mezzenga, Giuseppe Pizzi, Giulio Vallati, Anna Ianiro, Sandra Rea, Rosa Sciuto, Antonella Soriani, and Lidia Strigari. 2022. "A Workflow for Dosimetry of 90Y Radioembolization Based on Quantitative 99mTc-MAA SPECT/CT Imaging and a 3D-Printed Phantom" Applied Sciences 12, no. 20: 10541. https://doi.org/10.3390/app122010541
APA StyleUngania, S., D’Arienzo, M., Mezzenga, E., Pizzi, G., Vallati, G., Ianiro, A., Rea, S., Sciuto, R., Soriani, A., & Strigari, L. (2022). A Workflow for Dosimetry of 90Y Radioembolization Based on Quantitative 99mTc-MAA SPECT/CT Imaging and a 3D-Printed Phantom. Applied Sciences, 12(20), 10541. https://doi.org/10.3390/app122010541