1. Introduction
Virtual reality is well known for its applications in the entertainment industry, specifically for gaming purposes. Nowadays, the application of virtual reality has been extended into various fields such as tourism, engineering and education. Marketing and promotion strategy, heritage preservation, product design visualisation and practical sessions for technical skills are some of the purposes of virtual reality that serves the mentioned field.
In recent years, the interest in virtual reality applications has leaned towards the medical field. This trend is apparent in a number of published articles reviewing the effectiveness, potential, benefits and current issues of using virtual reality in the medical field. Among the recent topics discussed in the studies include the use of virtual reality as an alternative treatment for rehabilitation [
1,
2,
3] and therapies for psychological illness [
4,
5,
6]. In the field of psychology, virtual reality has been used as an alternative tool in therapy sessions to treat various psychological disorders such as anxiety disorders [
4,
7,
8], post-traumatic stress disorder (PTSD) [
6,
9,
10] and depression [
6,
9,
11,
12,
13]. The studies showed encouraging results where the usage of virtual reality as a therapy tool was found to benefit the patients in reducing and controlling their illnesses. The positive results have encouraged the researchers to further expand the application of virtual reality for therapy purposes to reduce psychological stress and promote relaxation.
A stress therapy technique that uses virtual reality as an alternative tool to reduce stress is referred to as virtual reality-based stress therapy. Many studies have been conducted to identify the effectiveness of virtual reality-based stress therapy in reducing stress. The studies demonstrated positive findings where virtual reality was found to be effective to be used as an alternative tool for the stress reduction process [
6,
11,
12,
14]. However, despite the promising findings, the studies only focused on the efficacy aspect of the system in reducing stress without presenting a detailed discussion of how the virtual environments used were designed. Based on the available studies, it was acknowledged that virtual reality-based stress therapy was effective in reducing stress. However, it remains unclear how the virtual environments should be designed to aid the stress reduction process.
Given the above situation, it is imperative to have a design framework that can serve as a guideline for designing a virtual environment that effectively reduces stress. This paper therefore presents a conceptual framework for designing a virtual environment for stress therapy purposes. The framework serves as a guideline for designing an effective virtual environment that aids the stress reduction process.
2. Review on Existing Virtual Reality-Based Stress Therapy Studies
Virtual reality-based stress therapy has been proven to be effective in relieving stress and inducing relaxation. A number of studies have been conducted that have yielded promising results where the usage of virtual reality as a stress therapy tool has benefited the users.
A study by Straßmann et al. [
15] on the development progress of a virtual reality relaxation application has attained a positive finding. The result of a preliminary study conducted showed that participants had lower negative effects of stress after a relaxation process using virtual reality.
Lin et al. [
16], in a study on virtual reality-based musical therapy for mental health management, also obtained a positive finding. The result of the analysis showed that the participants had lower overall stress levels after using the system.
Apart from this, studies by Ahmaniemi et al. [
17], Thoondee and Oikonomou [
18], Taneja et al. [
19] and Andersen et al. [
20] on the application of virtual reality for stress therapy and relaxation also presented positive findings. The findings of these studies showed that virtual reality-based stress therapy was effective in reducing stress.
Despite the reported positive results for the application of virtual reality as a stress therapy tool, there were still concerns to be highlighted when it came to designing the virtual environment for stress therapy. The majority of the existing studies on virtual reality for stress therapy reviewed only presented the results on the effectiveness of the application without discussing in detail the design of the virtual environments used. The discussion on the design of the virtual environments needs to be emphasized, as the information presented can serve as a guideline for designing an effective virtual environment which aids in the stress-reduction process. The guideline is essential as it will outline the directions for the design process, which helps in decision making. In addition, the guideline may also serve as a reference to check for necessary design requirements to be included in an effective virtual environment for stress therapy. Apart from that, the guideline is also important as the recommendation is designed from a combination of psychology and information technology knowledge. Without an appropriate guideline, unsuitable design elements may be incorporated into the virtual environment, resulting in the development of a system with ineffective therapy outcomes.
3. Review on Available Frameworks for Designing Purposes
Based on the available literature, existing frameworks for designing purposes were discussed from two perspectives; (i) psychological knowledge and (ii) information technology knowledge.
From a perspective of psychological knowledge, there were some frameworks available for designing technologies for positive change or mental well-being such as positive technologies [
21], positive computing [
22] and positive design [
23]. Positive technologies, proposed by [
21], categorised technologies according to how technology supports psychological changes in users. Meanwhile, positive computing, proposed by [
22], highlighted the wellbeing-supportive design to be used in all technologies by targeting the necessary well-being determinants such as gratitude, motivation and self-awareness. Finally, positive design, proposed by [
23], focuses on how technology can be designed to foster flourishing.
From a perspective of information technology, there are also several existing design frameworks for a virtual environment, as outlined by Blom and Beckhaus [
24], Chen and Bowman [
25] and Essabbah et al. [
26]. The framework proposed in [
24] focuses on the design space for dynamic interactive virtual environments. Meanwhile, [
25] proposed a general approach for designing a virtual environment by describing three architectures, which were (i) application, (ii) domain and (iii) generic interactive features. Lastly, [
26] highlighted the various methods of implementing user control, interactions and constraints on objects’ behaviour included in the virtual environment.
Although the existing frameworks mentioned above were available as a guideline, it was found that such frameworks focus on discussing the design information from either a psychological or an information technology perspective, respectively. It was also noted that, from a psychological knowledge perspective, the proposed frameworks only provide a general guideline on how to design technologies for mental well-being and do not particularly focus on immersive interactive technologies such as virtual reality. Meanwhile, from an information technology point of view, the frameworks mostly highlighted the functionality and system architecture of the virtual environment but not on the design of the virtual environment itself.
In general, the frameworks from both perspectives were found to provide general guidelines highlighting either the nature of systems that would have positive treatment outcomes, or on the systems of architectural and technical design that were not specified for stress therapy purposes. The gaps identified from the existing design frameworks have caused unclear understanding of how virtual environments for stress therapy should be designed and how the knowledge from both psychological and information technology perspectives should be implemented into the design process to facilitate stress reduction. Therefore, a framework is required to provide the necessary information on the requirements to design an effective virtual environment to reduce stress. In addition, the framework was also needed to provide a guideline on the actionable design practices to implement the requirements from the psychological and information technology points of view to facilitate the stress reduction process.
To address the identified issues, a framework for designing virtual environments for stress therapy was developed, highlighting the design elements from both psychological and information technology perspectives. The design elements proposed in the framework specifically focus on the design requirements for designing a virtual environment that is capable of reducing stress.
4. Proposed Framework
The development of the proposed framework involved four studies: (i) user requirements, (ii) an existing system review, where the discussion was presented in [
27], (iii) user evaluation, where the study information was presented in [
28], and (iv) an expert review, where the discussion was presented in [
29].
The result of the studies was a framework for designing virtual environments for stress therapy that can successfully contribute to stress reduction. The proposed framework, as shown in
Table 1, lists five factors and 14 design elements. Meanwhile, the descriptions for the design elements are as presented in
Table 2.
As the framework for designing virtual environments for stress therapy has been proposed, thus the next section presents the methodology for evaluating the framework.
5. Methodology
5.1. Participants
Participation in this study was based on a voluntary basis. Only interested participants were invited to experience the virtual environments and then interviewed. Eligible participants were healthy adults between the ages of 18 and 60 years who could understand the study procedure and had no physical disabilities.
A total of 55 participants took part in this study. The participants were required to take a screening session to determine their suitability for the experiment. The screening process involved the participants answering questions related to their stress condition. Only participants with a Depression Anxiety Stress Scale (DASS) score of higher than 14 proceeded with the experiment. Those participants with a total DASS score of below 14, but a stress intensity of four or higher, were included in the experiment. Inclusion was based on a stress intensity scale of four and higher, which demonstrated that the participants experienced some levels of stress.
As a result of the screening process, 40 out of 55 participants were eligible for the experiment. Ten of the participants were male and thirty were female.
5.2. Data Collection
Four methods were used to collect the required data; (i) questionnaire, (ii) physiological measures, (iii) experiment and (iv) interview.
5.2.1. Questionnaire
Nine types of questions were used with the following objectives:
To identify the participant’s perceived stress condition;
To identify the restorative outcome of the participants;
To identify the perceived usability of the system that implemented the design elements proposed in the framework in reducing stress;
To identify the perceived usefulness and ease of use of the system that implemented the design elements proposed in the framework in reducing stress;
To identify the perceived effectiveness of the system that implemented the design elements proposed in the framework in reducing stress;
To identify the usefulness of the design proposed in reducing stress.
- (i)
To identify the participant’s perceived stress condition
Three questions were used to identify the perceived stress conditions of the participants before and after the therapy session. The questions used were (i) the Depression Anxiety Stress Scale (DASS), (ii) a stress intensity scale and (iii) an emotional intensity scale.
Depression Anxiety Stress Scale (DASS). The Depression Anxiety Stress Scale (DASS) is a well-established self-reporting tool to assess the participant’s mental health before experiencing a therapy session. The DASS consists of 42 items, including three emotional states, namely (i) depression, (ii) anxiety and (iii) stress. The questions required the participants to rate their feelings and thoughts during the past week on a 4-point Likert scale (from 0 = ‘did not apply to me’ to 3 = ‘applied to me very much, or most of the time’). As this study focused on psychological stress, only 14 questions measuring the symptoms of stress were used.
Stress intensity scale. In addition to the DASS question, this question was also used to measure the stress level of the participants. The question requested the participants to rate their current stress intensity level based on a 10-point Likert scale (from 1 = ‘not at all stress’ to 10 = ‘maximally stressed’). The participants were asked to rate their stress intensity level twice, before and after the therapy session.
Emotional intensity scale. A question on current emotional state was also included to measure the participants’ psychological disturbance. Six emotional states: (i) angry, (ii) worried, (iii) sad, (iv) tense, (v) exhausted, and (vi) restless were listed to be selected by the participants. These six emotions have been validated by a clinical psychologist as common words used in everyday conversations to represent a person’s psychological state of stress. The participants were asked to choose an emotion that best described their current feeling and to rate the intensity of the selected emotion based on a 10-point Likert scale (from 1 = ‘low’ to 10 = ‘high’). The intensity of the chosen emotion was rated twice, before and after the therapy session.
- (ii)
To identify the restorative outcome of the participants
Restoration outcome scale (ROS) statements, proposed in [
30], were utilised to measure the restorative state of the participants. The ROS consists of six statements to be rated by the participants using a 7-point Likert scale (from 1 = ‘extremely disagree’ to 7 = ‘extremely agree’). The participants were requested to rate the ROS statements twice, before and after the therapy session.
- (iii)
To identify the perceived usability of the system that implemented the design elements proposed in the framework in reducing stress
The system usability scale (SUS) is one of the most widely used standardised questions for the assessment of perceived usability [
31,
32]. The SUS consists of 10 items, for which the participants had to rate each one based on a five-point Likert scale (from 0 = ‘strongly disagree’ to 4 = ‘strongly agree’). The participants were asked to rate the SUS once after the therapy session. For this study, the positive version of the SUS proposed by [
33] was used to reduce the likelihood of response and scoring errors, misinterpretation and miscoding, due to the mixed-tone statement used in the original version of the SUS.
- (iv)
To identify the perceived usefulness and ease of use of the system that implemented the design elements proposed in the framework in reducing stress
Two questions were used to identify the perceived usefulness of the system in reducing stress; (i) the technology acceptance model (TAM) and (ii) a perceived usefulness scale. Meanwhile, only the TAM was used to identify the ease of use of the system as a stress therapy tool.
Technology Acceptance Model (TAM). The technology acceptance model (TAM) questionnaire, proposed by Davis [
34], was utilised to measure the perceived usefulness and perceived ease of use of the system. The TAM was considered as one of the most-used tools utilised to identify the perceived usefulness and ease of use of technology adoption [
35,
36]. This tool consisted of 12 items; six were used to assess the perceived usefulness and the other six aimed to assess the perceived ease of use of the developed system. The participants were required to rate each of the items based on a 7-point Likert scale (from 1 = ‘extremely disagree’ to 7 = ‘extremely agree’). The TAM was only required to be rated once, after the therapy session.
Perceived usefulness scale. In addition to TAM, a general question was included on the perceived usefulness of the system as a stress therapy tool. For this question, the participants were asked to rate the usefulness based on a 10-point Likert scale (from 1 = ‘not useful at all’ to 10 = ‘very useful’).
- (v)
To identify the perceived effectiveness of the system that implemented the design elements proposed in the framework in reducing stress
For the purpose of identifying the effectiveness of the system in reducing stress, similar questions of (i) a stress intensity scale, (ii) an emotional intensity scale and (iii) a restorative outcome scale (ROS) were used.
In addition to the three questions, a general question on the perceived effectiveness of the system was included. For this question, the participants were asked to rate the effectiveness based on a 10-point Likert scale (from 1 = ‘not effective at all’ to 10 = ‘very effective’).
- (vi)
To identify the usefulness of the design proposed in reducing stress
In order to identify the usefulness of the design elements proposed, a set of questions regarding the 14 design elements proposed in the framework was constructed. For each of the design elements, the participants were requested to rate the usefulness of the design element in aiding them to reduce stress based on a 4-point Likert scale (from 1 = ‘not helpful at all’ to 4 = ‘very helpful’).
5.2.2. Physiological Measures
Stress responses can be measured with psychological changes assessed through questionnaires and physiological changes [
37]. Therefore, in addition to the questionnaire, physiological measures were also used to collect the required data. Stress can cause one’s arousal to increase, which leads to physical changes such as in pulse rate, blood pressure and galvanic skin reading [
14]. Blood pressure and pulse readings, especially with regard to the differences between the pre-test and post-test, are the most commonly used parameters to measure physiological changes caused by stress [
38]. Similar methods of using blood pressure and pulse reading changes to measure stress were found in studies of virtual reality and stress by [
14,
17,
38].
In addition, physiological measures were included in the study to strengthen the results obtained for the effectiveness of the system in reducing stress. Measuring the stress-reduction effects experienced by the participants through both psychological changes and physiological changes provided more reliable results to be presented, as the results were not reported from only one point of view.
Considering the benefits of including the physiological measures, this study hence included blood pressure and pulse rate as data to be collected. The blood pressure (both systolic and diastolic) and pulse rate of the participants were measured with a sphygmomanometer. Both readings were recorded before and immediately after the participants experienced the therapy session.
5.2.3. Experiment
The experiment stage involved participants experiencing the virtual environments in a single session for each participant. The objective of the experiment was to provide the participants with the opportunity to experience the virtual environment. A prototype implementing the proposed frameworks was used as an experimental tool.
Figure 1 shows the images of the virtual environments.
5.2.4. Interview
An interview was conducted face-to-face with each of the participants. The session was conducted after the participants had completed the therapy session and answered the post-test questionnaire. The questions asked during this session were based on the feedback written on the questionnaire. This step was taken to obtain a further explanation of the feedback received. The interview session aided the researcher in better understanding the feedback received and ensuring that the feedback is correctly interpreted.
5.3. Experimental Procedure
The experiment process consisted of eight steps.
Step 1: Research background explanation. The first step was to explain the research background, including the objectives and participants’ contributions to the research. This step aimed to give brief ideas to the participants about this research and why it was conducted. Additionally, this step also included an explanation of the objective of the study and the procedure of the experiment.
Step 2: Filling in the pre-test questionnaire. Once the participants understood the research background and the procedure, they were asked to fill in pre-test questions. The questions included were DASS, stress intensity, emotional intensity and ROS.
Step 3: Pre-test physiological measures. The pre-test blood pressure and pulse rate readings of the participants were recorded.
Step 4: System demonstration. Next, the system was then demonstrated to the participants. For this step, a prototype was used as the evaluation system. The flow of the system, the usage of the controllers, the instructions for activities provided, the features available, the options for interaction, and the options for audio were explained to the participants. A live demonstration of how to use the controller was provided to ensure the participants understood how to operate them.
Step 5: System exploration. The participants were invited to experience the system. As they explored the virtual environment, the researcher observed their spontaneous reactions and noted them down for analysis and discussion purposes. If the participants encountered any difficulties, such as having problems with the controller, the researcher would assist them until they understood the concept.
Step 6: Post-test physiological measures. The post-test blood pressure and pulse rate readings of the participants were recorded.
Step 7: Filling in the post-test questionnaire. The participants were requested to complete the post-test questionnaire. The questions included were stress intensity, emotional intensity, ROS, SUS, TAM, and questions on perceived usefulness and effectiveness of the system, as well as questions on the usefulness of the design elements proposed in reducing stress.
Step 8: Interview session. Upon completing the questionnaire, the participants were interviewed. The interview aimed to help the researcher to better understand the feedback received in terms of reasons for the rating given and some explanation on the suggestions given. The whole interview sessions were audio-recorded for analysis purposes.
5.4. Data Analysis
For the analysis, the feedback from the questionnaire was tabulated according to sections. Meanwhile, the recorded audio was transcribed word-for-word and reviewed three times for clarity and understanding purposes. The prepared data were then analysed using three methods, namely, (i) descriptive statistical analysis, (ii) inferential statistical analysis, and (iii) content analysis.
The descriptive statistical and inferential statistical analysis methods were used to analyse feedback for the quantitative data. The statistical analysis was performed using the software SPSS 26.0 and Microsoft Excel 2021. The data were checked for normality distribution using the value of skewness and the detrended normal Q-Q plot. The results of the normality test indicated that the data were approximately normally distributed. Hence, the relevant sample t-test to determine the significance of pre–post test values and mean value compared to the general population was appropriate to be conducted.
Meanwhile, content analysis was used to analyse responses received from the qualitative data. The analysis was carried out by using ATLAS.ti version 9.
6. Results
The results of the experiment were analysed and presented based on the participants’ stress level and the effectiveness, usability, usefulness and ease of use of the virtual reality-based system in reducing stress, as well as the usefulness of the design elements proposed in the framework for assisting participants in the stress reduction process.
6.1. Participants’ Stress Level
Based on the scoring scheme of the Depression Anxiety Stress Scale (DASS), the participants’ distress levels were divided into five levels as shown in
Table 3.
The DASS is intended as a screening instrument to assess the severity of negative symptoms commonly associated with depression, anxiety and chronic stress, and not as a diagnostic tool to diagnose a psychological disorder [
39,
40,
41] -. Therefore, the total score as presented in
Table 3 describes the severity of distress, with a higher DASS score indicating a more severe experience of negative psychological disturbances by an individual [
39,
41,
42]. Apart from this, the score also describes whether the negative symptoms experienced should be a concern and require further assessment by the clinical personnel [
39]. The score has no direct impact on the assignment of individuals to any psychological disorder categories such as depression and anxiety disorders [
40]. A high DASS score may indicate the possibility of having psychological disorders. However, a person with a high DASS score cannot be classified as having a mental disorder until they have undergone comprehensive clinical interviewing and diagnosis to identify a possible mental disorder [
41].
For the purpose of a clearer analysis, this study has further grouped the standard distress levels in
Table 3 into two levels as shown in
Table 4. The grouping of the participants into the normal and high distress levels was performed based on DASS total score. The participants with DASS scores of 14 and below were classified as having normal distress and those participants with a score of 15 and above were considered to experience high distress [
19,
43].
Based on the interpretive distress level as shown in
Figure 2, the results show that 13 out of 40 participants (32.50%) experienced a normal distress level. Twenty-seven out of 40 participants (67.50%) experienced a high distress level.
Although there were 13 participants with a normal distress level, which could indicate less negative psychological disturbance experienced, they were still included in the study because the result of the second stage of screening, based on stress intensity level, showed that the 13 participants had a high perceived stress intensity of four and above. Thus, the DASS score results from
Figure 2 demonstrated that all participants experienced either moderate to high stress intensity (represented by the 13 participants) or high distress level (represented by the 27 participants), which were indicative of negative psychological disturbance.
6.2. The Effectiveness of Virtual Reality-Based Therapy System in Reducing Stress
The effectiveness of a virtual-reality based therapy system in reducing stress was determined through two measures: psychological measures and physiological measures. The psychological measures included a stress intensity score, emotional intensity changes value, ROS and perceived effectiveness rating, while the physiological measures were identified through blood pressure and pulse rate readings.
- (i)
The effectiveness measured by stress intensity
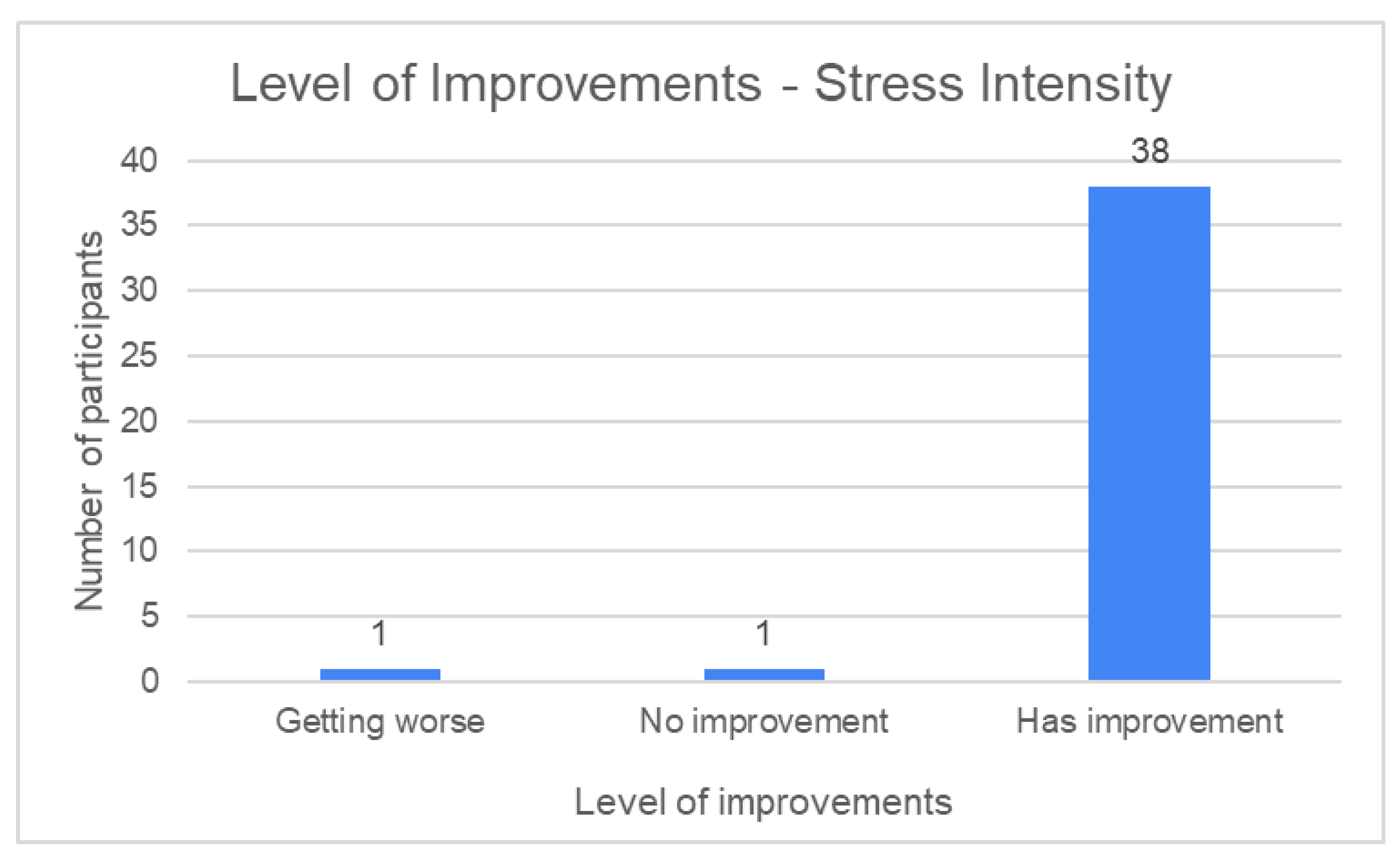
Comparison of the stress intensity score before and after the therapy session showed that the majority of the participants experienced stress reduction after the therapy session. Thirty-eight participants (95.00%) reported to have a stress level improvement by experiencing a lower stress intensity level after the therapy session. One participant (2.50%) was found to have a similar level of stress intensity before and after the therapy session and one participant (2.50%) was reported to feel worse after the therapy session.
Figure 3 shows the level of stress intensity improvement after the therapy sessions.
The mean comparison for the stress intensity score showed significant difference before and after the therapy sessions. The mean value of stress intensity after the therapy session (M = 2.05, SD = 0.89) was significantly lower than before the therapy session (M = 3.9, SD = 2.05); t(39) = 13.774, p = 0.001.
- (ii)
The effectiveness measured by emotional intensity changes value
The emotional intensity values of the participants before and after therapy were compared. The results of the emotional changes values were divided into three levels. The three levels of emotional changes were (i) getting worse, (ii) no improvement and (iii) had improvement.
Table 5 shows the level of emotional changes and the conditions to classify the value of emotional changes resulting from the comparison process.
The system was considered effective if the participants experienced positive emotional improvement. Based on
Table 5, emotional improvement was considered to happen if the participants’ emotional intensity values after the therapy session were lower than before the therapy session.
Based on the analysis performed, 30 participants (75.50%) showed some emotional improvements after the therapy sessions. Seven participants (17.50%) reported experiencing no emotional improvement and three participants (7.50%) reported emotional worsening after the therapy session.
Figure 4 shows the participants’ level of emotional changes after experiencing the therapy sessions.
A paired-samples t-test result shows a significant difference between the mean value of emotional intensity before and after the therapy session. The mean value for after the therapy session (M = 3.60, SD = 1.77) was significantly lower than before the therapy session (M = 5.48, SD = 1.71); t(39) = 6.807, p = 0.001.
- (iii)
The effectiveness measured by ROS
The mean ROS values before and after the therapy session were compared. The result yielded a significant difference, where the mean value for ROS after the therapy session (M = 33.90, SD = 6.30) was higher than before the therapy session (M = 27.70, SD = 7.02); t(39) = 20.479, p = 0.001.
- (iv)
The effectiveness measured by perceived effectiveness rating
For analysis purposes, the scores of the effectiveness of the system were grouped into four levels, which were (i) not effective, (ii) somewhat effective, (iii) effective and (iv) very effective. The rescaling of the 10-point scale to 4-point scale feedback was performed based on an approach proposed by Dawes [
44].
Table 6 shows the scoring level used to determine the effectiveness of the system.
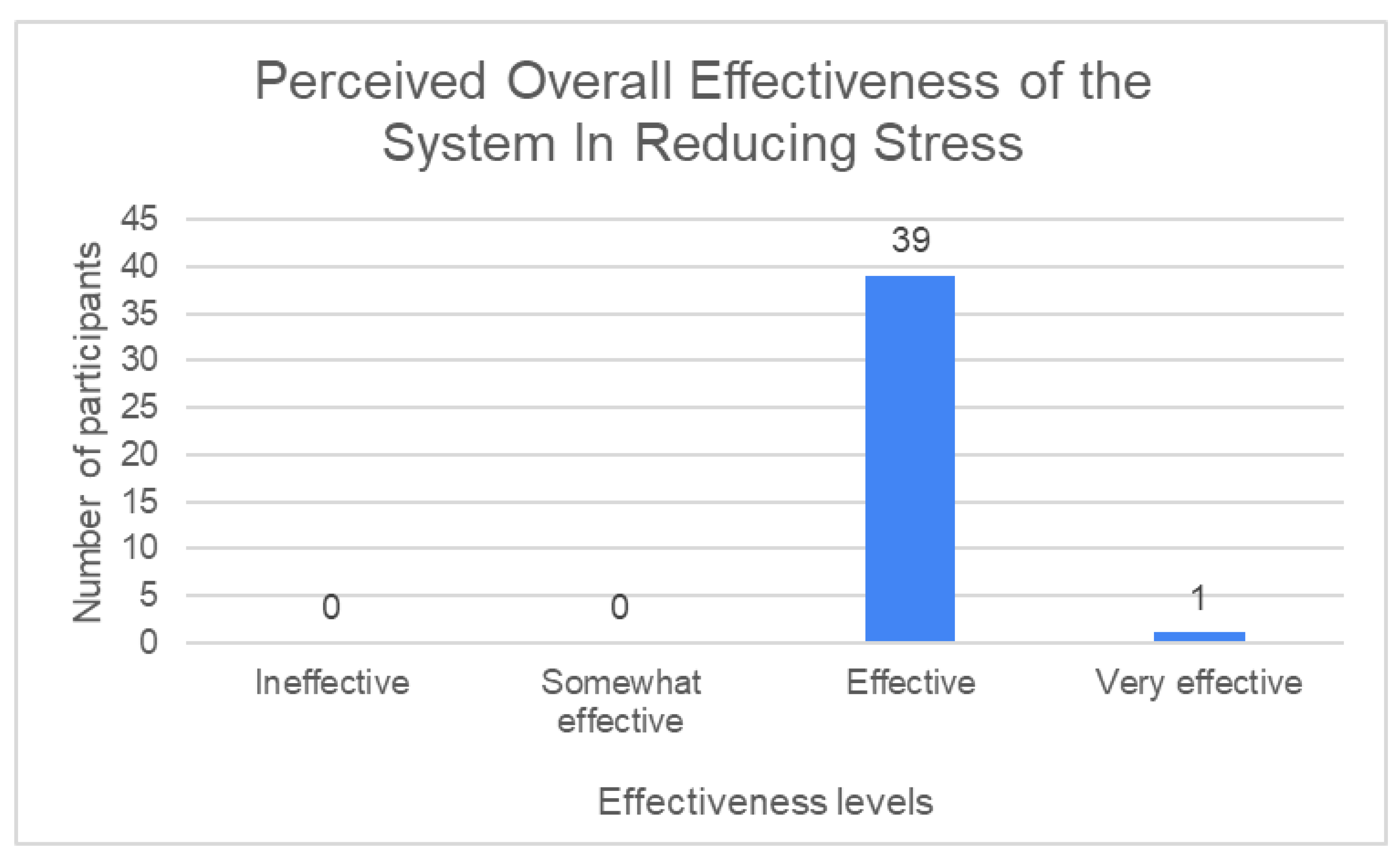
Based on the analysis done, the result show that all participants agreed that the virtual reality-based stress therapy system was effective in reducing stress. All 40 participants (100%) rated the system as effective (with the feedback of effective and very effective). None of the participants rated the system as somewhat effective nor not effective as a stress-reduction tool.
Figure 5 shows the graph of the perceived effectiveness of the system in reducing stress.
A one-sample t-test that was conducted revealed a positive result, where the mean value of the perceived effectiveness of the system implementing the proposed framework in reducing stress (M = 7.85, SD =1.027) was significantly higher than the mean of the scale which was 5.5; t(39) = 17.478, p = 0.000 < 0.05.
- (v)
The effectiveness measured by physiological measures
The mean participants’ blood pressure and pulse rate were compared before and after the therapy session. The results of the comparison showed no significant differences in systolic blood pressure, diastolic blood pressure and pulse rate as presented in
Table 7.
6.3. Usability, Usefulness and Ease of Use of Virtual Reality-Based System in Reducing Stress
- (i)
The usability of the virtual reality-based therapy system.
The usability of the system was measured by SUS items. Analysis performed resulted in the SUS average score of 78.1. According to Bangor et al. [
45], a SUS score of 78.1 was interpreted as “good” with acceptable acceptability ranges. Meanwhile, when the score was interpreted according to a curved grading scale by Sauro and Lewis [
46], the usability score fell into the A-category.
- (ii)
The usefulness and ease of use of the virtual reality-based therapy system.
The usefulness and ease of use of the system were determined based on the score of TAM. As for the usefulness, the mean score recorded was 5.71. One sample t-test conducted resulted in a significant difference from the usefulness mean value as compared to the mean of the scale. The result of the t-test indicated that the mean value of the perceived usefulness of the system (M = 5.71, SD = 0.78) was significantly higher than the mean of the scale used of 4; t(39) = 13.920, p = 0.000 < 0.05.
In addition to the usefulness result obtained from the TAM instrument, this study also evaluated the usefulness of the system based on a perceived usefulness rating. The scores of the usefulness were grouped into four categories, which were (i) useless, (ii) somewhat useful, (iii) useful and (iv) very useful. The rescaling of the 10-point scale to 4-point scale feedback was performed based on an approach proposed by Dawes [
44].
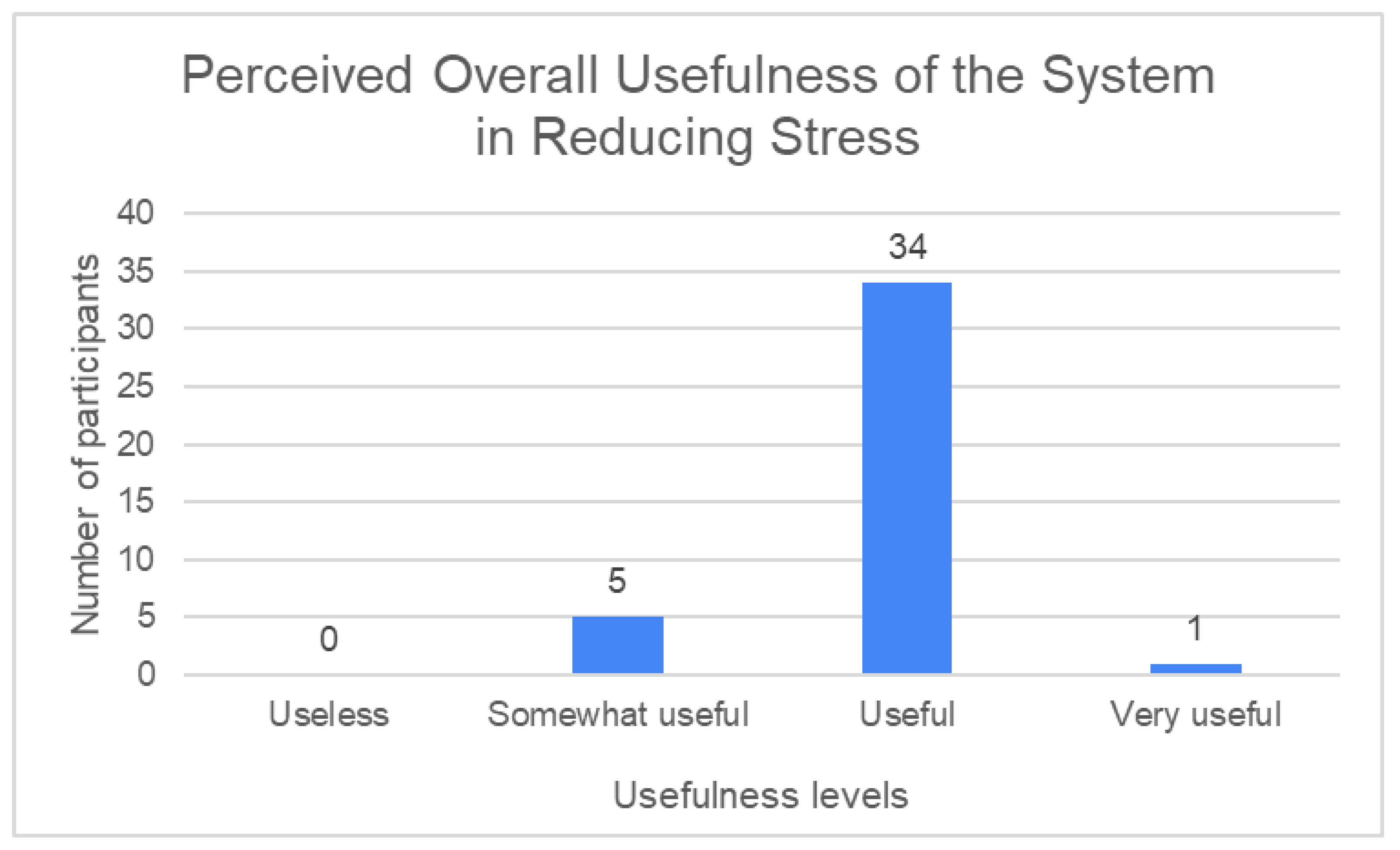
The results of the analysis revealed that the majority of the participants rated the system as useful in reducing stress. Thirty-five participants (87.50%) agreed that the system was useful (with feedback of useful and very useful). Five participants (12.50%) rated the system as somewhat useful in reducing stress. None of the participants rated the system as useless in reducing stress.
Figure 6 shows the graph of the perceived usefulness of the system in reducing stress.
The one-sample t-test performed returned an encouraging result where the mean value of perceived usefulness of the system in reducing stress (M = 7.630, SD =1.409) was significantly higher than the mean of the scale of 5.5; t(39) = 9.542, p = 0.000 < 0.05.
Meanwhile, the ease-of-use items recorded a mean value of 6.07. The result of the one-sample t-test conducted showed a significant difference between the ease-of-use mean value, as compared to the mean of the scale, which was 4. The mean value of perceived ease of use of the system that implemented the proposed framework (M = 6.071, SD = 0.751) was significantly higher than the mean of the scale of 4; t(39) = 17.440, p = 0.000 < 0.05.
6.4. The Usefulness of the Design Element Proposed in Assisting Users to Reduce Their Stress
The usefulness of the design elements in reducing stress was determined through two measures: helpfulness frequency and helpfulness mean.
- (i)
The usefulness of the design elements measured by helpfulness frequency
The usefulness of the design elements proposed was evaluated based on the rating of their helpfulness in assisting users to reduce stress. The participants were requested to rate the helpfulness of the design elements proposed based on a 5-point Likert scale (from 1 = ‘not helpful at all’ to 4 = ‘very helpful’ and 5 = ‘no opinion’).
For analysis purposes, the helpfulness scores were grouped into four categories which were (i) helpful, (ii) not helping much, (iii) not helpful at all and (iv) no opinion.
Table 8 shows the scoring level used to determine the helpfulness of the design elements proposed.
The results of the analysis show the majority of the participants agreed that most of the design elements proposed were helpful (with scores of very helpful and helpful) in reducing stress.
Table 9 shows the results of the helpfulness of the design elements proposed.
Based on
Table 9, it can be seen that 12 of the 14 design elements proposed received most of the scores in the ‘helpful’ category, while the scores of the remaining two design elements were mostly tabulated between the ‘Helpful’ and the ‘Not helping much’ category.
- (ii)
The usefulness of the design elements measured by helpfulness mean
The usefulness of the design elements was also analysed through the helpfulness mean values. To determine the usefulness, the helpfulness mean values for each of the design elements were calculated. Next, the results obtained were rearranged according to the mean value, from highest to lowest, as shown in
Table 10.
Based on
Table 10, it can be seen that 13 design elements proposed, except for the pre-defined path, have a mean value of 2.6 and above, which surpassed the mean scale value of 2.5. Meanwhile, the mean value for the pre-defined path design element fell slightly below the mean scale value of 2.5.
7. Discussion
The results of this study showed that the virtual reality-based stress therapy system developed based on the framework proposed was effective, usable, useful and easy to be used in reducing stress.
Based on the results of the psychological measures, it was found that the system implementing the concept of the framework proposed was effective in reducing stress. The effectiveness was demonstrated by the significant reduction in stress intensity after the therapy session. Apart from this, the result of the emotional intensity changes also showed that the majority of the participants experienced positive emotional improvements after the therapy sessions. The positive results indicate that the virtual reality-based stress therapy system was effective in reducing stress. The result of the restorative outcome scale (ROS) also demonstrated a significant increase in mean value after the therapy session, suggesting that the system was effective in restoring the mental state of the participants. In addition, the results of the perceived overall effectiveness of the system also showed that the majority of the participants agreed that the system was effective at aiding them in reducing stress. Thus, this reflects the effectiveness of the system in reducing stress.
In terms of physiological measures, the mean blood pressure, both systolic and diastolic readings, as well as pulse rate before and after the therapy sessions, recorded no significant differences. The results could be caused by the inclusion of the active interaction design element that required the participants to perform some physical movements in order to complete the relaxation activities. The physical movements performed could result in unchanged, or in the case of some participants, increase in blood pressure and pulse rate readings. A study by Fernandes et al. [
47] on the determination of stress using blood pressure and galvanic skin response revealed that 80 percent of participants recorded higher blood pressure levels after performing some physical activities. The findings of the study indicated that the increase in blood pressure experienced by the majority of the participants was due to physical stress resulting from the physical activities and was not due to psychological stress [
47]. Aside from including the active interaction, the insignificant differences recorded for the blood pressure and pulse rate reading might also be caused by the excitement in using the system or focused attention on fascination stimuli included in the virtual environment. Crosswell and Lockwood [
48], in an article on best practices for stress measurement, highlighted that biological changes, such as increases in blood pressure and pulse rate, are not only evoked by psychological stress but can also be triggered by non-psychological stress situations such as feeling excited, focusing attention on stimuli or exercising. The findings reported by [
47,
48] underlined an important point that physiological changes are not only triggered by increases in psychological stress but may also be contributed to by other factors. The insignificant differences recorded for the psychological measures were not a novel situation. Similar findings were reported in [
17,
37,
38,
49] in the studies of stress reduction and psychological restoration.
For the usability aspect, the result obtained demonstrated that the system implementing the concept of the proposed framework was usable for reducing stress. The mean value recorded for the usability of the system revealed that the system was at the ‘good’ level of usability acceptance as well as interpreted to be in the ‘A-’ usability category.
For the usefulness of the system in reducing stress, the results indicated that the system was useful. The usefulness was demonstrated by the high mean value of perceived usefulness based on TAM items. The recorded mean value was higher than 5, which surpass the scale’s mean of 4. Similarly, the result on the perceived usefulness of the system based on a general scale also indicated that the system was opined to be useful in assisting the users in reducing stress. The mean recorded for the perceived usefulness based on the general scale was greater than 7, which also exceeded the scale’s mean of 5.5.
In terms of ease of use, the system was agreed to be easy to be used. The mean value recorded for the perceived ease-of-use items adapted from TAM was 6.071, which surpassed the scale’s mean of 4. The result indicated that the system was easy to be used.
As presented, the results for the effectiveness, usability, usefulness and ease-of-use of the system, which demonstrated the concept of the framework proposed, returned positive findings. These encouraging findings indicated that the design elements included in the virtual environment somehow contributed to the stress reduction process. As the results presented were encouraging, therefore, it was appropriate to investigate in detail which of the design elements proposed contributed to this effect.
Based on
Table 9, all 14 design elements proposed obtained a higher score in the ‘helpful’ feedback. Despite the positive result, two of the design elements, which were (i) passive interaction and (ii) the pre-defined path, recorded most of their scores in the percentage of ‘helpful’ and ‘not helping much’ feedback. A detailed analysis of the interview transcripts revealed that the higher ‘not helping much’ feedback recorded by these two design elements compared to the other design elements was due to issues in the implementation strategies of these two design elements in the prototype. Therefore, the existing implementation strategies should be improved to better present the design elements, thus enhancing the helpfulness value.
For passive interaction, the participants suggested including more fascinating stimuli objects or features to distract the users’ minds. With passive interaction, the users were given the opportunity to sit back and enjoy the surrounding view without having to engage in physical activities. As no activities were available, the participants suggested adding more visually visible fascination stimuli to address the need for mental distraction, which in active interaction is fulfilled by the physical activities offered. The various fascination stimuli will help to distract the users’ minds for a longer period of time. According to feedback from the participants, the current prototype has only limited fascination stimuli to look at. Therefore, proposing to include more of the fascination stimuli objects or features may enhance the passive interaction design element implemented in the existing prototype.
Meanwhile, for the pre-defined path, the participants suggested revising the implementation of the design element in the current prototype. In the prototype used for the experiment, the pre-defined path was implemented by the flight-based technique, where the users were taken along a path simulating as if they were on a sightseeing train. Based on the feedback received, the pre-defined path implemented in the existing prototype did not provide the users with the opportunity to control the movement, such as to start and stop the simulation, or to adjust the speed of the movement according to the users’ preferences. The mentioned drawbacks caused dizziness and discomfort among the participants. Therefore, the participants recommended adding two features that would allow the users to control the movement, i.e., the start and stop functions, and to have the ability to control the speed of the movement based on users’ preferences.
For the helpfulness of the design elements based on the mean values, the presented results indicated the usefulness of the design elements in reducing stress. The usefulness was demonstrated by the mean value for each of the design elements that surpassed the mean value of the scale used.
In addition, the sorted tabulated mean value also provided insight into which of the design elements had higher contributions to stress reduction. Based on the presented result, design elements at the top list of the ranking indicated higher contribution to the stress reduction process. From
Table 10, it can be seen that active interaction was the design element with the highest contribution to stress reduction. The second and third highly contributed design elements were the nature-based theme, followed by fascination stimuli. Meanwhile, the design element that contributed the least to reducing stress was the pre-defined path.
Overall, the results on the helpfulness of the design elements showed that all 14 design elements proposed were useful in reducing stress, demonstrating the suitability of the design elements for implementation in a virtual environment designed for stress therapy.
8. Conclusions
In this article, a framework for designing a virtual environment for stress therapy has been developed as a guideline to refer to when designing a virtual environment for stress therapy. There are five factors, namely (i) attention attraction, (ii) environment setting, (iii) environment exploration, (iv) interaction and (v) user comfort laid out in the framework. Each factor listed design elements that aid the stress reduction process. A total of 14 design elements are proposed, including (i) fascination stimuli, (ii) nature-based theme, (iii) supporting audio, (iv) daylight lighting, (v) realism, (vi) free exploration, (vii) pre-defined viewpoints, (viii) pre-defined path, (ix) passive interaction, (x) active interaction, (xi) safety features, (xii) mind preparation, (xiii) social support and (xiv) visual clarity.
The results of the evaluation conducted showed that the virtual reality-based stress therapy system incorporating all the design elements suggested by the framework was effective, usable, useful and easy to be used in reducing stress. Therefore, the design elements proposed in the framework were found to be useful and appropriate to be included in the virtual environment for stress therapy purposes.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}