
Enhanced Osteoblast Adhesion and Proliferation on Vacuum Plasma-Treated Implant Surface


Abstract
:1. Introduction
2. Materials and Methods
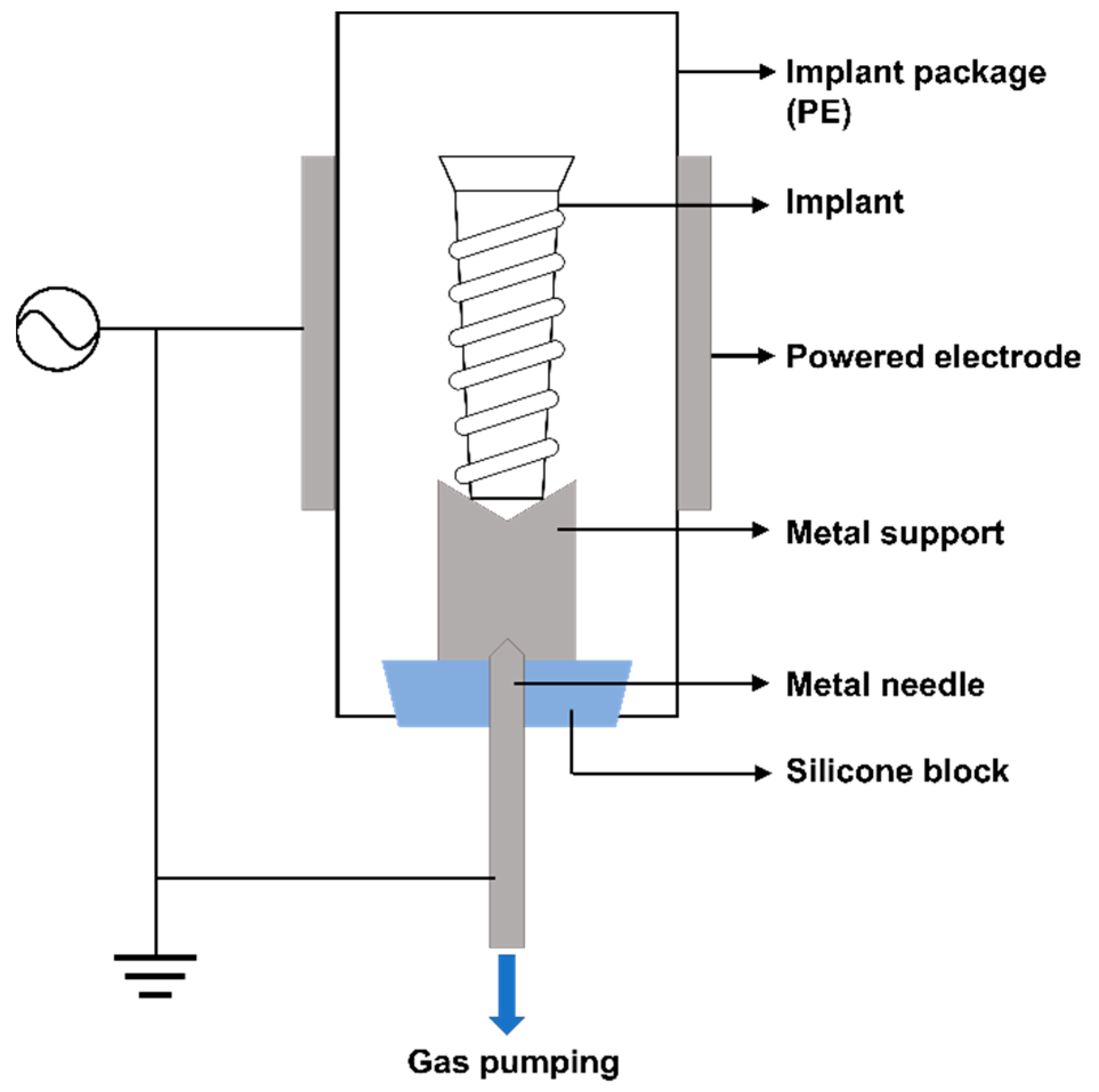
2.1. Plasma Device
2.2. Implant Treatment Process
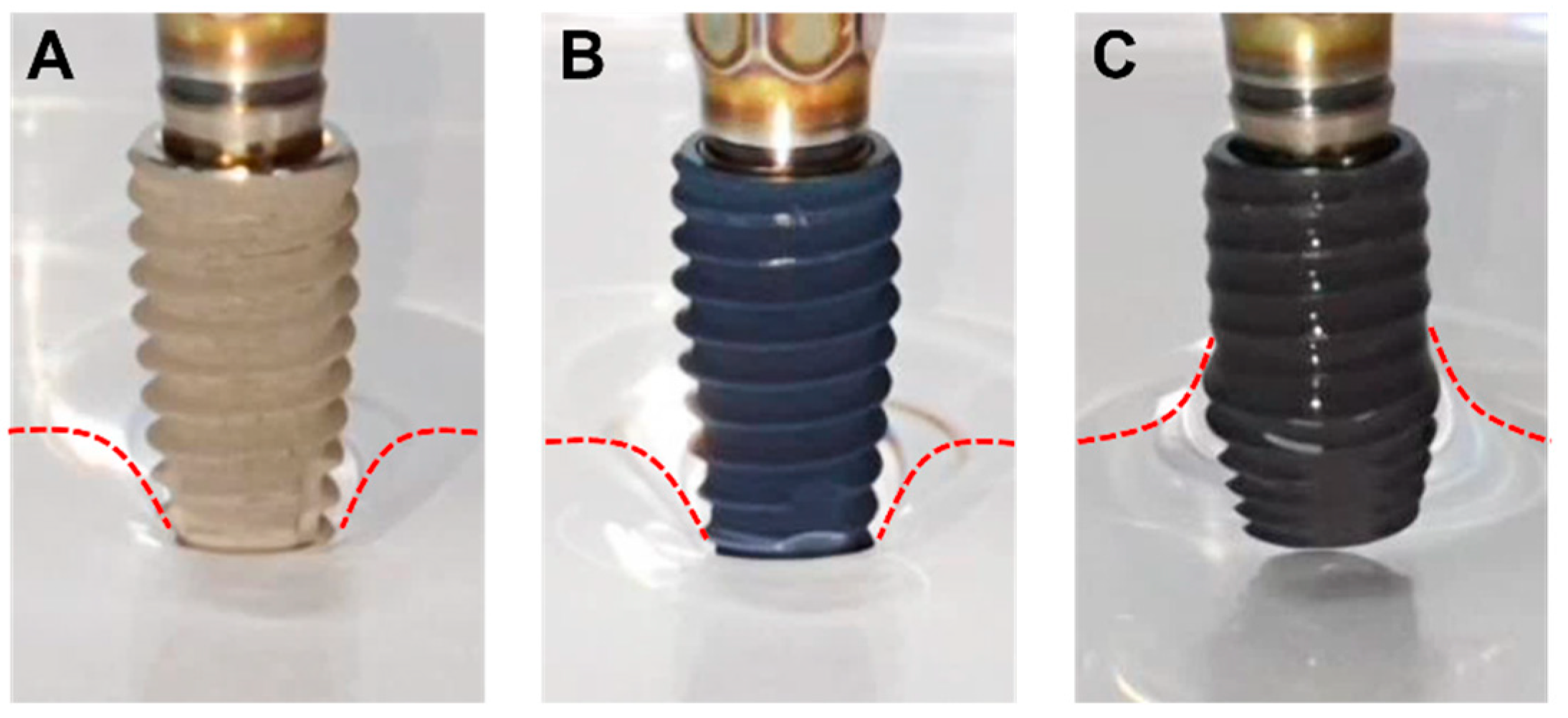
2.3. Hydrophilicity Test of Implant Surface
2.4. Assessing Characteristics of Implant Surface Using SEM and EDS
2.5. Protein Adsorbtion Experiment
2.6. Quantification of Osteoblast Adhesion and Proliferation
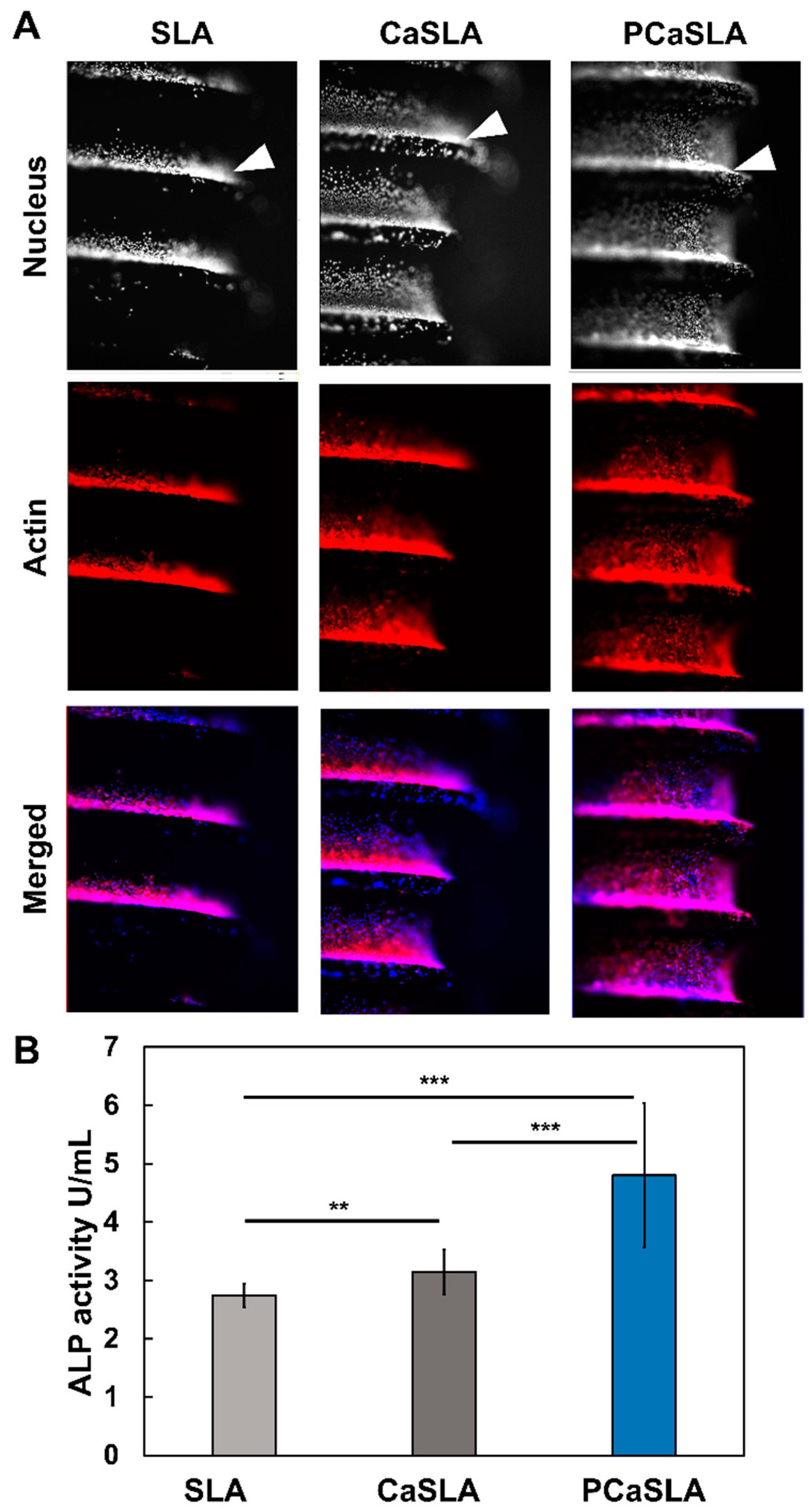
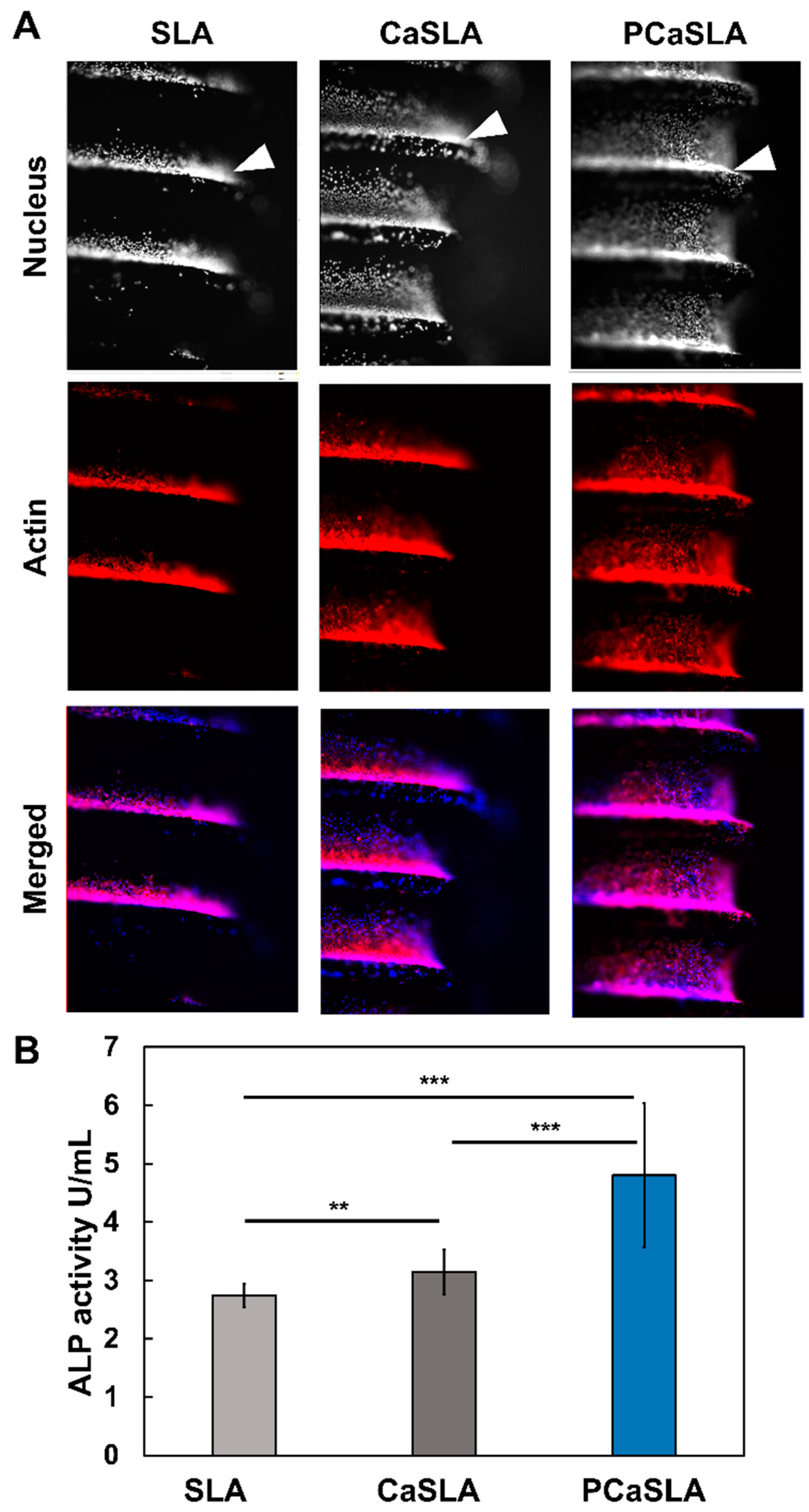
2.7. Quantification of Osteoblast Differentiation
2.8. Staining and Imaging Cells on Implant Surface
2.9. Statistical Analysis
3. Results
3.1. Hydrophilicity of Implant Surface before and after Plasma Treatment
3.2. Surface Characteristics of Implant before and after Plasma Treatment
3.3. Enhancement of Protein Adsorption by Plasma Treatment
3.4. Improvement of Cell Adhesion and Proliferation by Plasma Treatment
3.5. Distribution of Cells on Implant Surface
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aparicio, C.; Javier Gil, F.; Fonseca, C.; Barbosa, M.; Planell, J.A. Corrosion behaviour of commercially pure titanium shot blasted with different materials and sizes of shot particles for dental implant applications. Biomaterials 2003, 24, 263–273. [Google Scholar] [CrossRef]
- Sanchez-Perez, A.; Nicolas-Silvente, A.I.; Sanchez-Matas, C.; Muñoz-Guzon, F.; Navarro-Cuellar, C.; Romanos, G.E. Influence on Bone-to-Implant Contact of Non-Thermal Low-Pressure Argon Plasma: An Experimental Study in Rats. Appl. Sci. 2020, 10, 3069. [Google Scholar] [CrossRef]
- Schuler, M.; Trentin, D.; Textor, M.; Tosatti, S.G. Biomedical interfaces: Titanium surface technology for implants and cell carriers. Nanomedicine 2006, 1, 449–463. [Google Scholar] [CrossRef]
- Textor, M.; Sittig, C.; Frauchiger, V.; Tosatti, S.; Brunette, D.M. Properties and Biological Significance of Natural Oxide Films on Titanium and Its Alloys. In Titanium in Medicine: Material Science, Surface Science, Engineering, Biological Responses and Medical Applications; Brunette, D.M., Tengvall, P., Textor, M., Thomsen, P., Eds.; Springer: Berlin/Heidelberg, Germany, 2001; pp. 171–230. [Google Scholar] [CrossRef]
- Jansen, J.A.; Vonrecum, A.F.; Vanderwaerden, J.P.C.M.; Degroot, K. Soft-Tissue Response to Different Types of Sintered Metal Fiber-Web Materials. Biomaterials 1992, 13, 959–968. [Google Scholar] [CrossRef]
- McCracken, M. Dental Implant Materials: Commercially Pure Titanium and Titanium Alloys. J. Prosthodont. 1999, 8, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Verardi, S.; Swoboda, J.; Rebaudi, F.; Rebaudi, A. Osteointegration of Tissue-Level Implants with Very Low Insertion Torque in Soft Bone: A Clinical Study on SLA Surface Treatment. Implant Dent. 2018, 27, 5–9. [Google Scholar] [CrossRef]
- Gianfreda, F.; Raffone, C.; Antonacci, D.; Mussano, F.; Genova, T.; Chinigò, G.; Canullo, L.; Bollero, P. Early Biological Response of an Ultra-Hydrophilic Implant Surface Activated by Salts and Dry Technology: An In-Vitro Study. Appl. Sci. 2021, 11, 6120. [Google Scholar] [CrossRef]
- Hou, P.-J.; Syam, S.; Lan, W.-C.; Ou, K.-L.; Huang, B.-H.; Chan, K.-C.; Tsai, C.-H.; Saito, T.; Liu, C.-M.; Chou, H.-H.; et al. Development of a Surface-Functionalized Titanium Implant for Promoting Osseointegration: Surface Characteristics, Hemocompatibility, and In Vivo Evaluation. Appl. Sci. 2020, 10, 8582. [Google Scholar] [CrossRef]
- Zuanazzi, D.; Xiao, Y.; Siqueira, W.L. Evaluating protein binding specificity of titanium surfaces through mass spectrometry–based proteomics. Clin. Oral Investig. 2021, 25, 2281–2296. [Google Scholar] [CrossRef]
- de Avila, E.; Lima, B.; Sekiya, T.; Torii, Y.; Ogawa, T.; Shi, W.; Lux, R. Effect of UV-photofunctionalization on oral bacterial attachment and biofilm formation to titanium implant material. Biomaterials 2015, 67, 84–92. [Google Scholar] [CrossRef]
- Att, W.; Hori, N.; Iwasa, F.; Yamada, M.; Ueno, T.; Ogawa, T. The effect of UV-photofunctionalization on the time-related bioactivity of titanium and chromium–cobalt alloys. Biomaterials 2009, 30, 4268–4276. [Google Scholar] [CrossRef] [PubMed]
- Kilpadi, D.V.; E Lemons, J.; Liu, J.; Raikar, G.N.; Weimer, J.J.; Vohra, Y. Cleaning and heat-treatment effects on unalloyed titanium implant surfaces. Int. J. Oral Maxillofac. Implants 2000, 15, 219–230. [Google Scholar] [PubMed]
- Aita, H.; Hori, N.; Takeuchi, M.; Suzuki, T.; Yamada, M.; Anpo, M.; Ogawa, T. The effect of ultraviolet functionalization of titanium on integration with bone. Biomaterials 2009, 30, 1015–1025. [Google Scholar] [CrossRef]
- Iwasa, F.; Hori, N.; Ueno, T.; Minamikawa, H.; Yamada, M.; Ogawa, T. Enhancement of osteoblast adhesion to UV-photofunctionalized titanium via an electrostatic mechanism. Biomaterials 2010, 31, 2717–2727. [Google Scholar] [CrossRef]
- Danna, N.R.; Beutel, B.G.; Tovar, N.; Witek, L.; Marin, C.; Bonfante, E.A.; Granato, R.; Suzuki, M.; Coelho, P.G. Assessment of Atmospheric Pressure Plasma Treatment for Implant Osseointegration. BioMed Res. Int. 2015, 2015, 761718. [Google Scholar] [CrossRef] [PubMed]
- Guastaldi, F.P.S.; Yoo, D.; Marin, C.; Jimbo, R.; Tovar, N.; Zanetta-Barbosa, D.; Coelho, P.G. Plasma Treatment Maintains Surface Energy of the Implant Surface and Enhances Osseointegration. Int. J. Biomater. 2013, 2013, 354125. [Google Scholar] [CrossRef] [PubMed]
- Hui, W.L.; Perrotti, V.; Iaculli, F.; Piattelli, A.; Quaranta, A. The Emerging Role of Cold Atmospheric Plasma in Implantology: A Review of the Literature. Nanomaterials 2020, 10, 1505. [Google Scholar] [CrossRef] [PubMed]
- Henningsen, A.; Smeets, R.; Heuberger, R.; Jung, O.T.; Hanken, H.; Heiland, M.; Cacaci, C.; Precht, C. Changes in surface characteristics of titanium and zirconia after surface treatment with ultraviolet light or non-thermal plasma. Eur. J. Oral Sci. 2018, 126, 126–134. [Google Scholar] [CrossRef]
- Yang, Y.; Zheng, M.; Liao, Y.; Zhou, J.; Li, H.; Tan, J. Different behavior of human gingival fibroblasts on surface modified zirconia: A comparison between ultraviolet (UV) light and plasma. Dent. Mater. J. 2019, 38, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Tashiro, Y.; Komasa, S.; Miyake, A.; Komasa, Y.; Okazaki, J. Effects of Surface Modification on Adsorption Behavior of Cell and Protein on Titanium Surface by Using Quartz Crystal Microbalance System. Materials 2021, 14, 97. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, K.; Kumar, S.; Bremmell, K.; Griesser, H. Molecular-level removal of proteinaceous contamination from model surfaces and biomedical device materials by air plasma treatment. J. Hosp. Infect. 2010, 76, 234–242. [Google Scholar] [CrossRef]
- Gong, X.; Lin, Y.; Li, X.; Wu, A.; Zhang, H.; Yan, J.; Du, C. Decomposition of volatile organic compounds using gliding arc discharge plasma. J. Air Waste Manag. Assoc. 2020, 70, 138–157. [Google Scholar] [CrossRef] [PubMed]
- Gruchmann, T. The impact of usability on patient safety. Biomed. Insa. Technol. 2005, 39, 462–465. [Google Scholar]
- Zhang, J.; Johnson, T.; Patel, V.L.; Paige, D.L.; Kubose, T. Using usability heuristics to evaluate patient safety of medical devices. J. Biomed. Inform. 2003, 36, 23–30. [Google Scholar] [CrossRef]
- Cai, S.; Wu, C.; Yang, W.; Liang, W.; Yu, H.; Liu, L. Recent advance in surface modification for regulating cell adhesion and behaviors. Nanotechnol. Rev. 2020, 9, 971–989. [Google Scholar] [CrossRef]
- Guo, S.; Zhu, X.; Li, M.; Shi, L.; Ong, J.L.T.; Jańczewski, D.; Neoh, K.G. Parallel Control over Surface Charge and Wettability Using Polyelectrolyte Architecture: Effect on Protein Adsorption and Cell Adhesion. ACS Appl. Mater. Interfaces 2016, 8, 30552–30563. [Google Scholar] [CrossRef]
- Ayala, R.; Zhang, C.; Yang, D.; Hwang, Y.; Aung, A.; Shroff, S.S.; Arce, F.T.; Lal, R.; Arya, G.; Varghese, S. Engineering the cell-material interface for controlling stem cell adhesion, migration, and differentiation. Biomaterials 2011, 32, 3700–3711. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, T. Ultraviolet Photofunctionalization of Titanium Implants. Int. J. Oral Maxillofac. Implants 2014, 29, e95–e102. [Google Scholar] [CrossRef]
- Razali, M.; Ngeow, W.C.; Omar, R.A.; Chai, W.L. An Integrated Overview of Ultraviolet Technology for Reversing Titanium Dental Implant Degradation: Mechanism of Reaction and Effectivity. Appl. Sci. 2020, 10, 1654. [Google Scholar] [CrossRef]
- Soltanzadeh, P.; Ghassemi, A.; Ishijima, M.; Tanaka, M.; Park, W.; Iwasaki, C.; Hirota, M.; Ogawa, T. Success rate and strength of osseointegration of immediately loaded UV-photofunctionalized implants in a rat model. J. Prosthet. Dent. 2017, 118, 357–362. [Google Scholar] [CrossRef]
- Kim, H.S.; Lee, J.I.; Yang, S.S.; Kim, B.S.; Kim, B.C.; Lee, J. The effect of alendronate soaking and ultraviolet treatment on bone-implant interface. Clin. Oral Implants Res. 2017, 28, 1164–1172. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Hashimoto, K.; Fujishima, A.; Chikuni, M.; Kojima, E.; Kitamura, A.; Shimohigoshi, M.; Watanabe, T. Light-induced amphiphilic surfaces. Nature 1997, 388, 431–432. [Google Scholar] [CrossRef]
- Liu, X.; Hua, R.; Niu, J.; Zhang, Z.; Zhang, J. N2 plasma treatment TiO2 nanosheets for enhanced visible light-driven photocatalysis. J. Alloys Compd. 2021, 881, 160509. [Google Scholar] [CrossRef]
- Kim, W.J.; Kim, S.; Lee, B.S.; Kim, A.; Ah, C.S.; Huh, C.; Sung, G.Y.; Yun, W.S. Enhanced protein immobilization effi-ciency on a TiO2 surface modified with a hydroxyl functional group. Langmuir 2009, 25, 11692–11697. [Google Scholar] [CrossRef] [PubMed]
- Ujino, D.; Nishizaki, H.; Higuchi, S.; Komasa, S.; Okazaki, J. Effect of plasma treatment of titanium surface on biocom-patibility. Appl. Sci. 2019, 9, 2257. [Google Scholar] [CrossRef]
- Volkov, A.G.; Xu, K.G.; Kolobov, V.I. Plasma-generated reactive oxygen and nitrogen species can lead to closure, locking and constriction of the Dionaea muscipula Ellis trap. J. R. Soc. Interface 2019, 16, 20180713. [Google Scholar] [CrossRef]
- Nastuta, A.V.; Gerling, T. Cold Atmospheric Pressure Plasma Jet Operated in Ar and He: From Basic Plasma Properties to Vacuum Ultraviolet, Electric Field and Safety Thresholds Measurements in Plasma Medicine. Appl. Sci. 2022, 12, 644. [Google Scholar] [CrossRef]
- Dukes, C.A.; Baragiola, R.A. Compact plasma source for removal of hydrocarbons for surface analysis. Surf. Interface Anal. 2010, 42, 40–44. [Google Scholar] [CrossRef]
- Sasmazel, H.T.; Alazzawi, M.; Alsahib, N.K.A. Atmospheric Pressure Plasma Surface Treatment of Polymers and Influence on Cell Cultivation. Molecules 2021, 26, 1665. [Google Scholar] [CrossRef] [PubMed]
- Graves, D.B. Reactive Species from Cold Atmospheric Plasma: Implications for Cancer Therapy. Plasma Process. Polym. 2014, 11, 1120–1127. [Google Scholar] [CrossRef]
- Feng, B.; Weng, J.; Yang, B.; Qu, S.; Zhang, X. Characterization of titanium surfaces with calcium and phosphate and osteoblast adhesion. Biomaterials 2004, 25, 3421–3428. [Google Scholar] [CrossRef]
- Park, J.W.; Kim, H.K.; Kim, Y.J.; An, C.H.; Hanawa, T. Enhanced osteoconductivity of micro-structured titanium implants (XiVE S CELLplus((TM))) by addition of surface calcium chemistry: A histomorphometric study in the rabbit femur. Clin. Oral Implants Res. 2009, 20, 684–690. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EDS Image Number | Carbon Reduction Rate (%) |
|---|---|
| #1 | 35.80886586 |
| #2 | 25.75539568 |
| #3 | 12.45318352 |
| #4 | 17.42268041 |
| #5 | 23.06220096 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, H.J.; Jung, A.; Kim, H.J.; Seo, J.S.; Kim, J.Y.; Yum, M.S.; Gweon, B.; Lim, Y. Enhanced Osteoblast Adhesion and Proliferation on Vacuum Plasma-Treated Implant Surface. Appl. Sci. 2022, 12, 9884. https://doi.org/10.3390/app12199884
Jeon HJ, Jung A, Kim HJ, Seo JS, Kim JY, Yum MS, Gweon B, Lim Y. Enhanced Osteoblast Adhesion and Proliferation on Vacuum Plasma-Treated Implant Surface. Applied Sciences. 2022; 12(19):9884. https://doi.org/10.3390/app12199884
Chicago/Turabian StyleJeon, Hyun Jeong, Ara Jung, Hee Jin Kim, Jeong San Seo, Jun Young Kim, Moon Seop Yum, Bomi Gweon, and Youbong Lim. 2022. "Enhanced Osteoblast Adhesion and Proliferation on Vacuum Plasma-Treated Implant Surface" Applied Sciences 12, no. 19: 9884. https://doi.org/10.3390/app12199884
APA StyleJeon, H. J., Jung, A., Kim, H. J., Seo, J. S., Kim, J. Y., Yum, M. S., Gweon, B., & Lim, Y. (2022). Enhanced Osteoblast Adhesion and Proliferation on Vacuum Plasma-Treated Implant Surface. Applied Sciences, 12(19), 9884. https://doi.org/10.3390/app12199884