
IoT Fog-Enabled Multi-Node Centralized Ecosystem for Real Time Screening and Monitoring of Health Information

 , , ,
, , ,  , and
, and 
Abstract
:1. Introduction
- Design of the IoT-Fog Computing-Based Multi-Node (FCMN) Architectural Framework for Real Time Health Monitoring;
- Real-time analysis of the proposed FCMN-based real time health monitoring framework;
- Statistical analysis for the validation of the proposed health monitoring framework.
2. Related Study and General Methodology
3. Proposed System
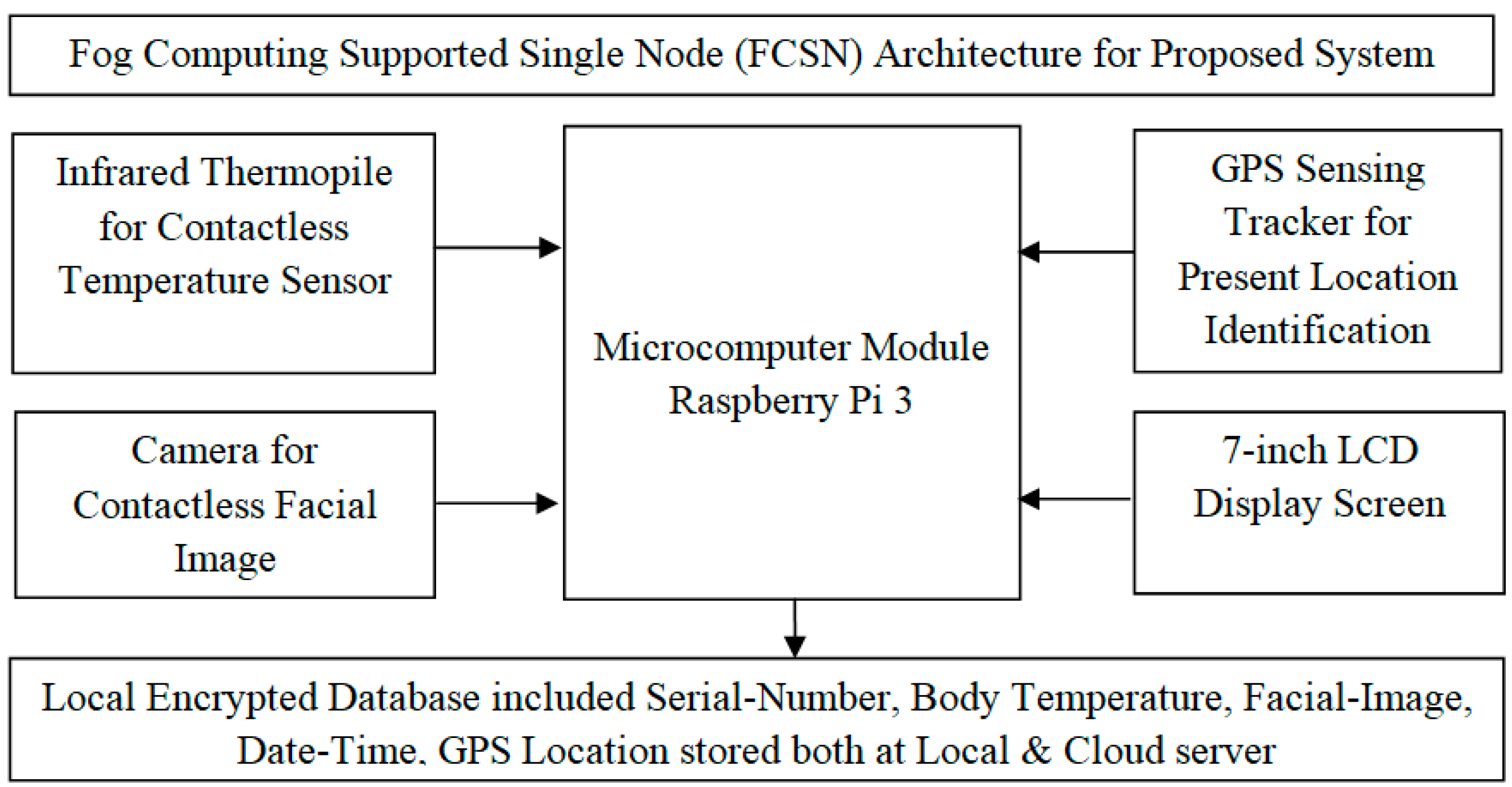
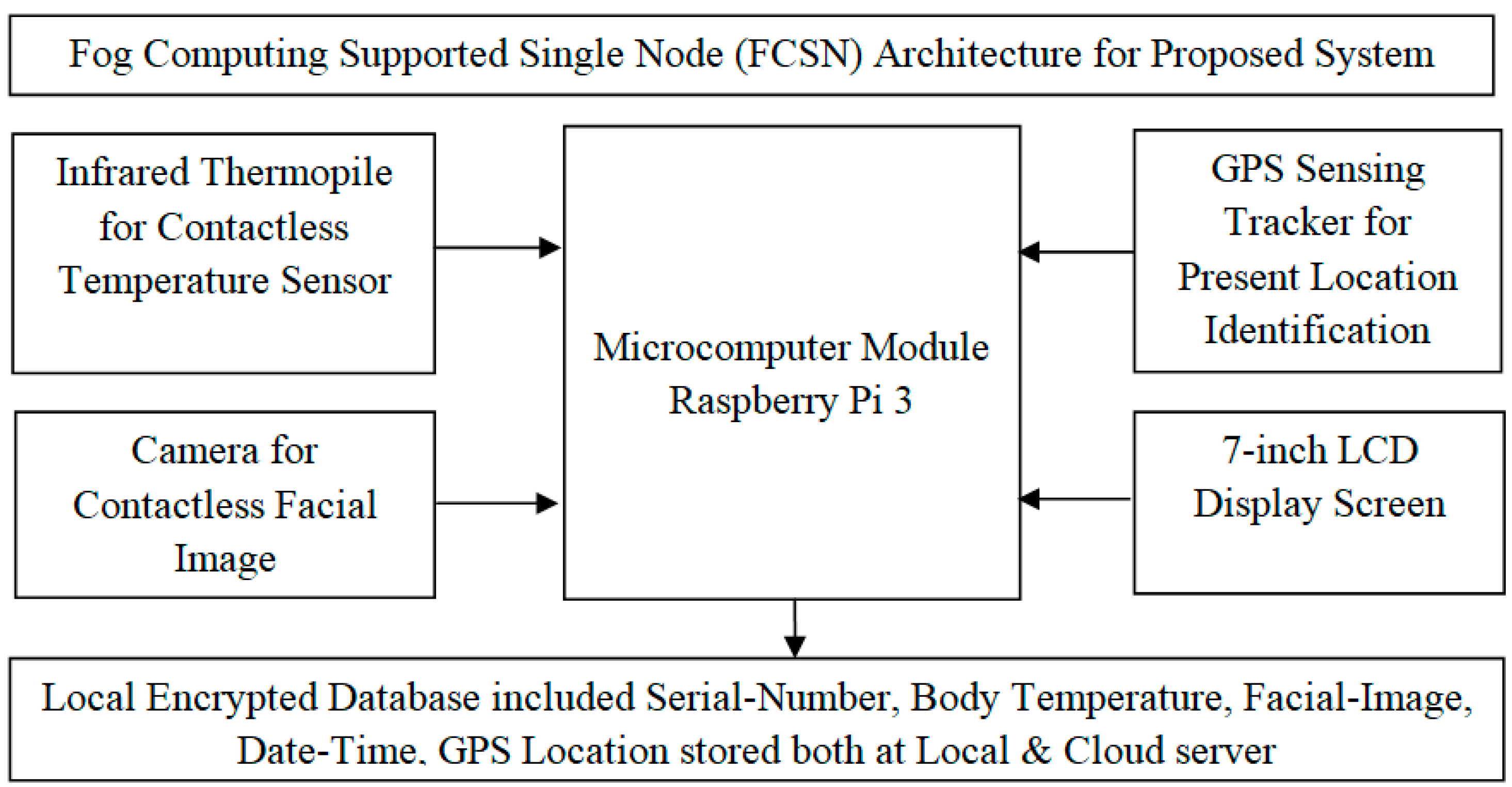
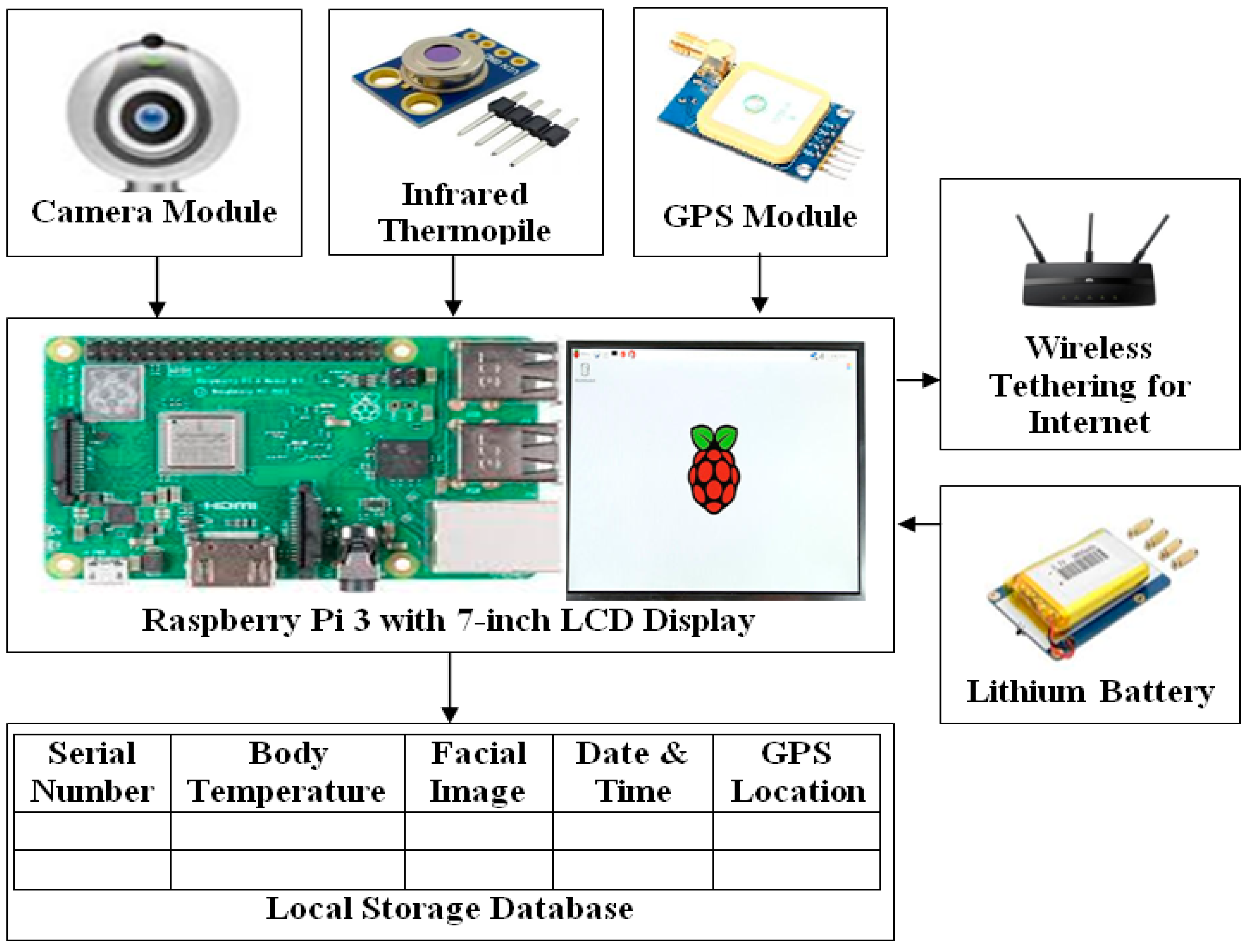
3.1. Fog Computing-Based Single Node (FCSN) Architecture
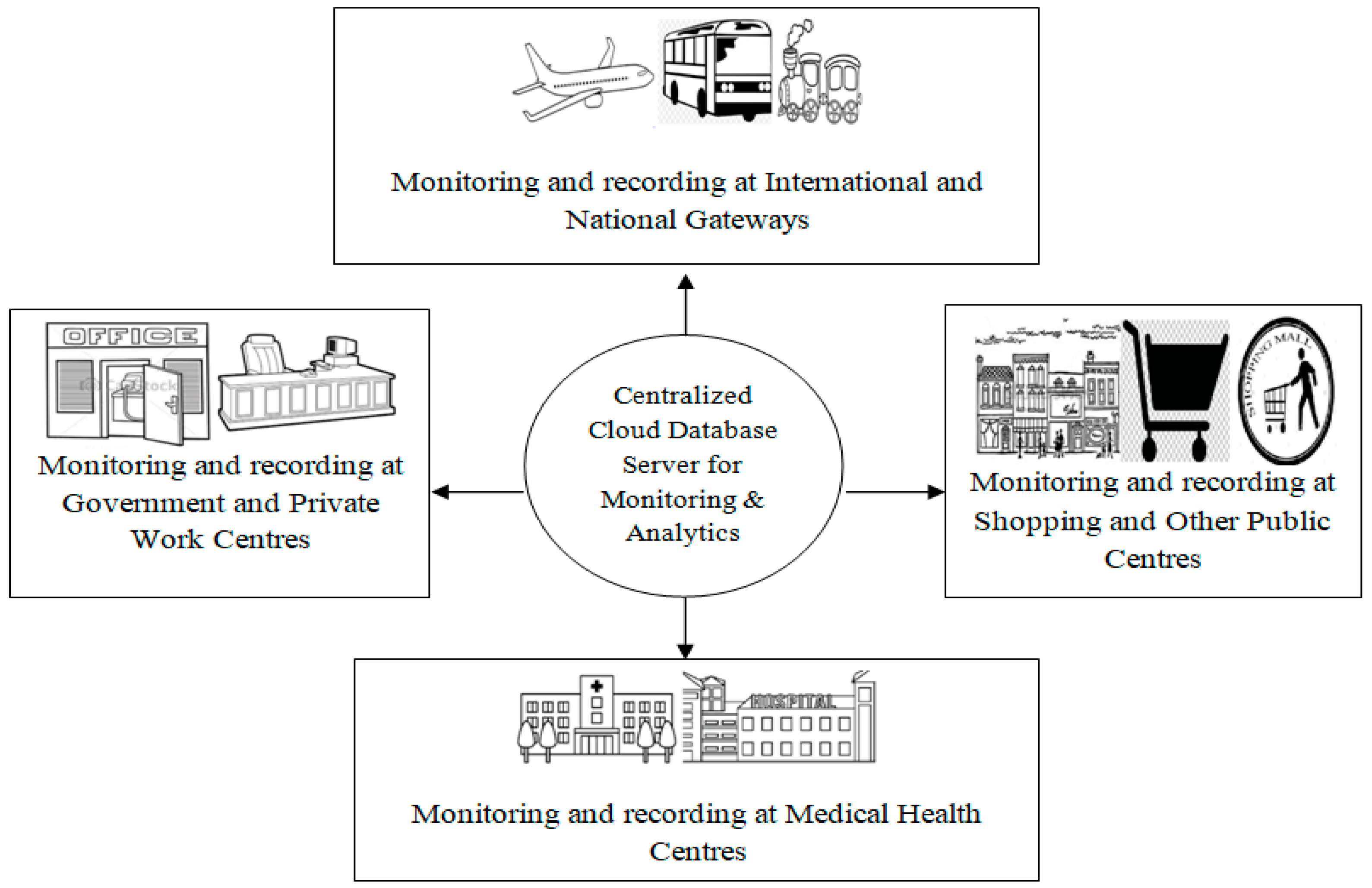
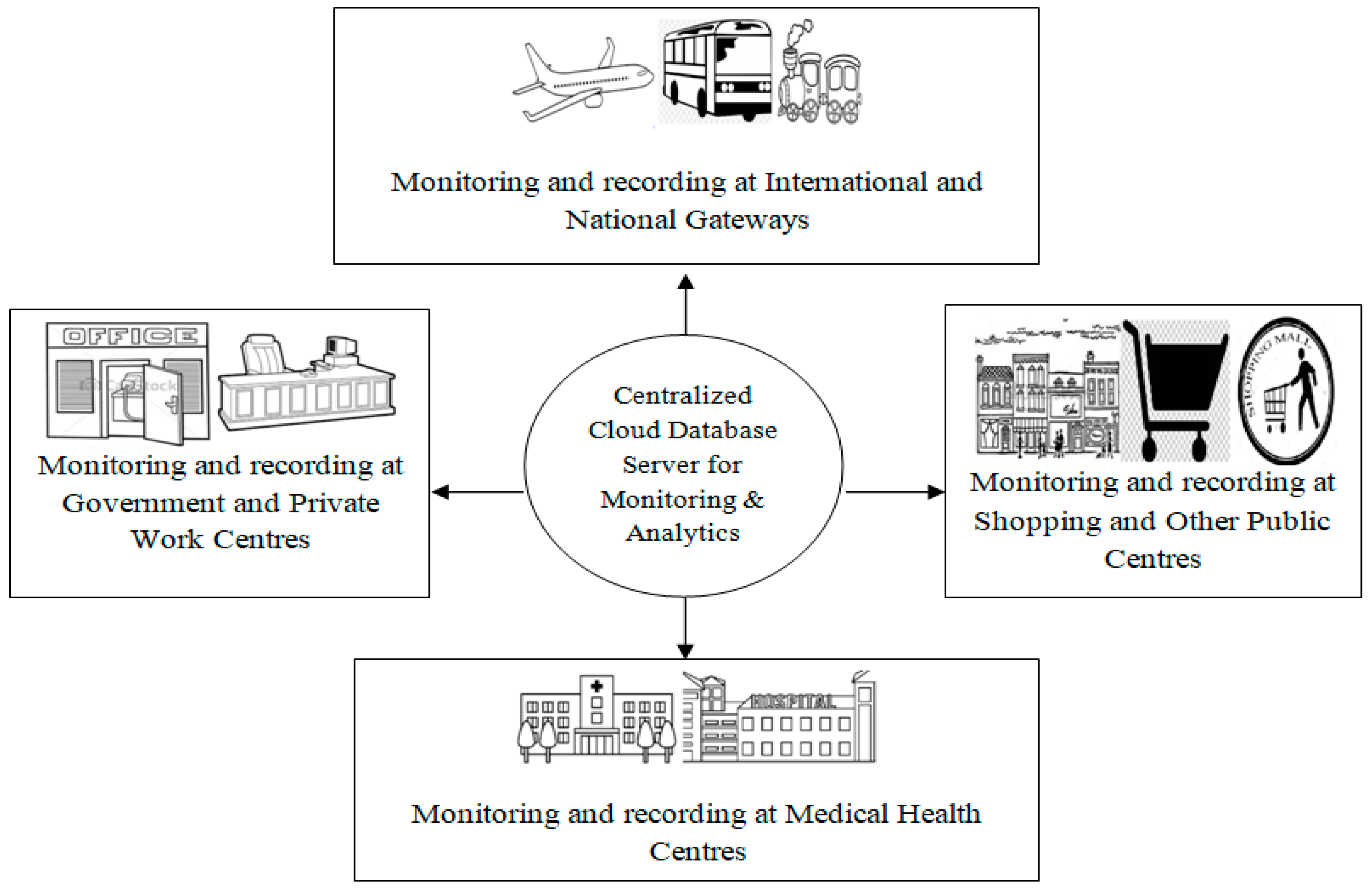
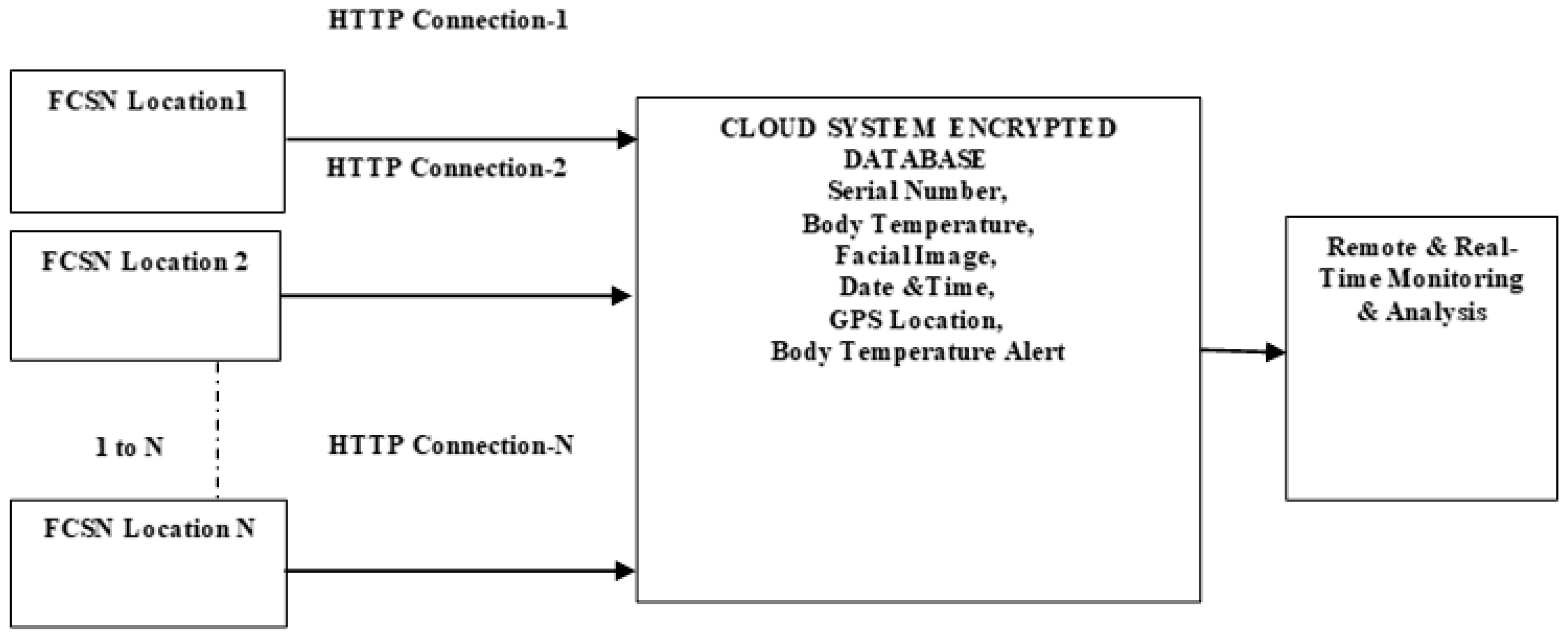
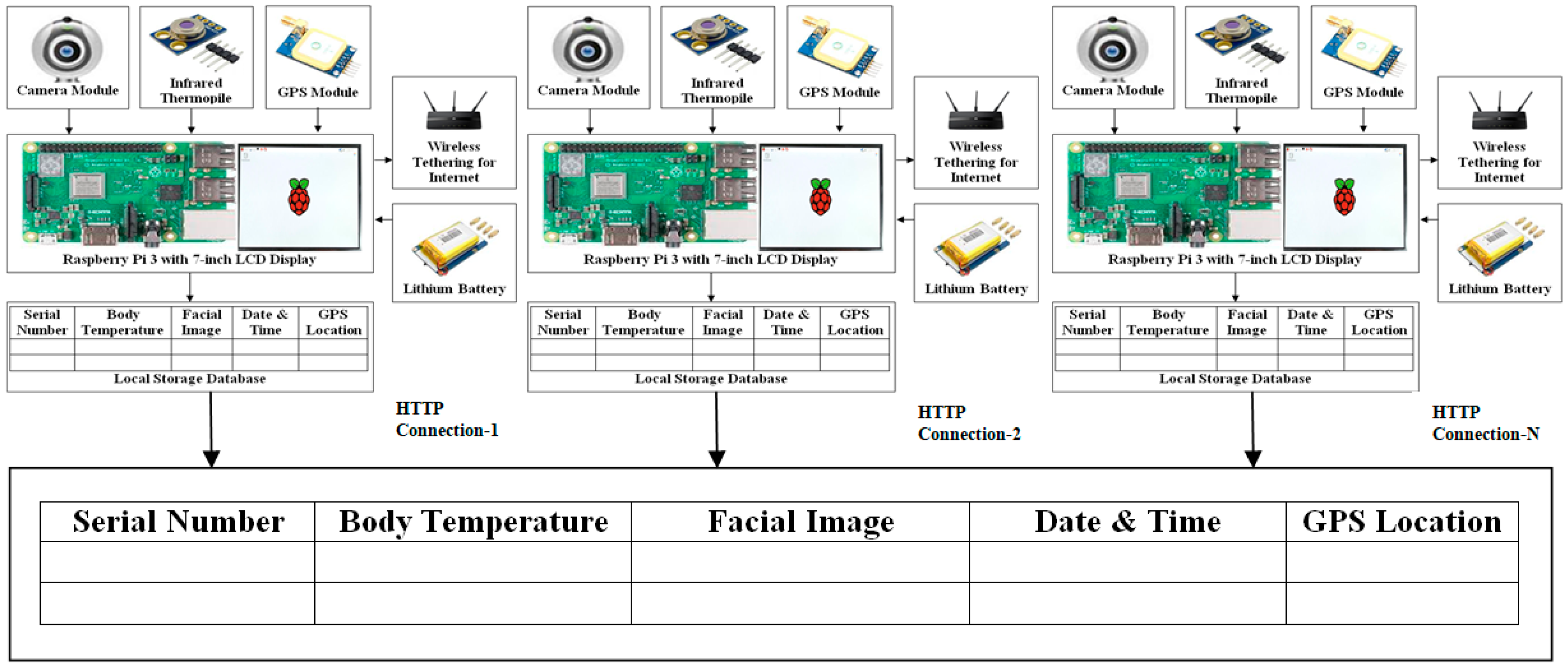
3.2. IoT-Fog Computing Supported Multi-Node (FCMN) Architecture
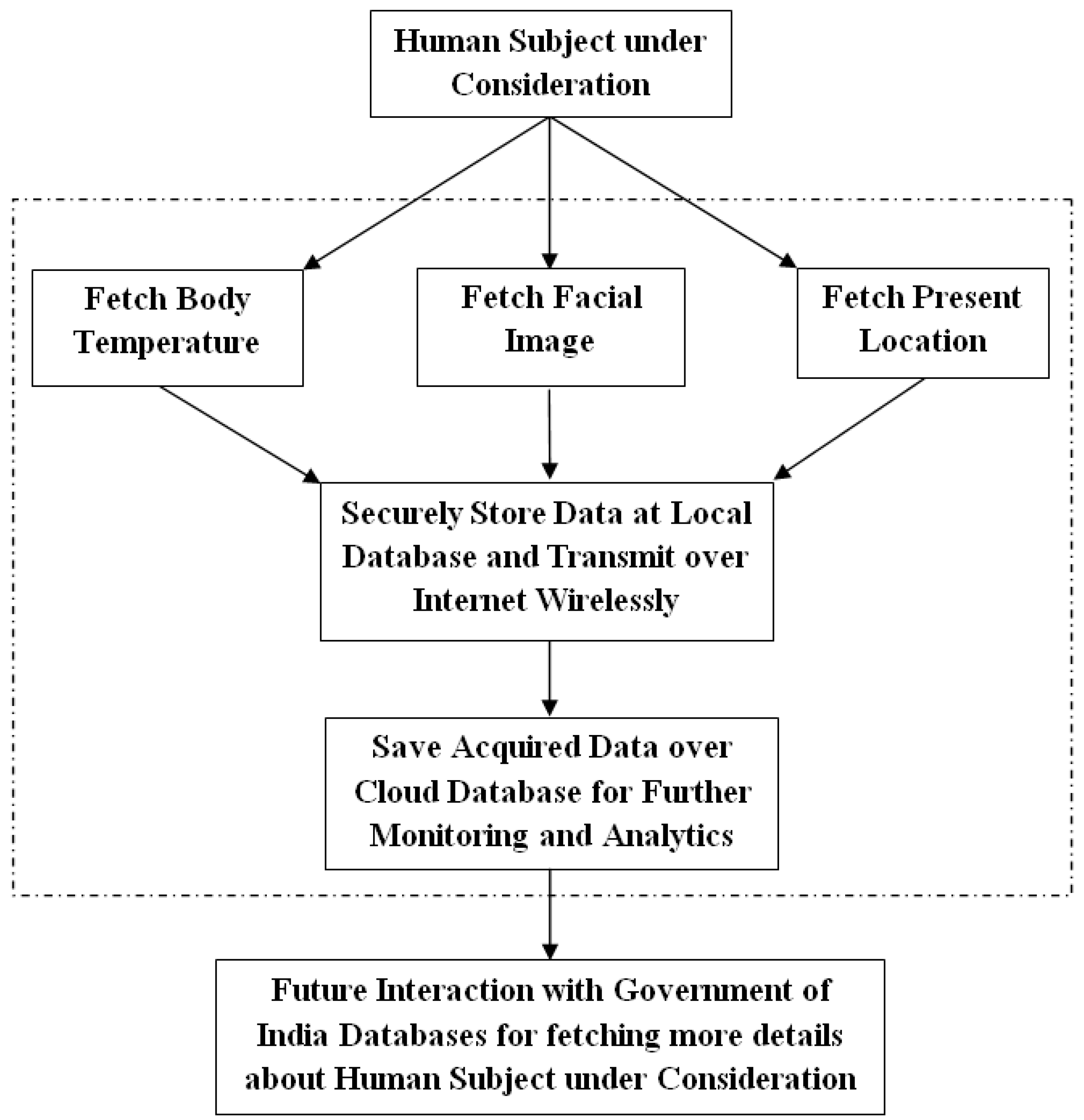
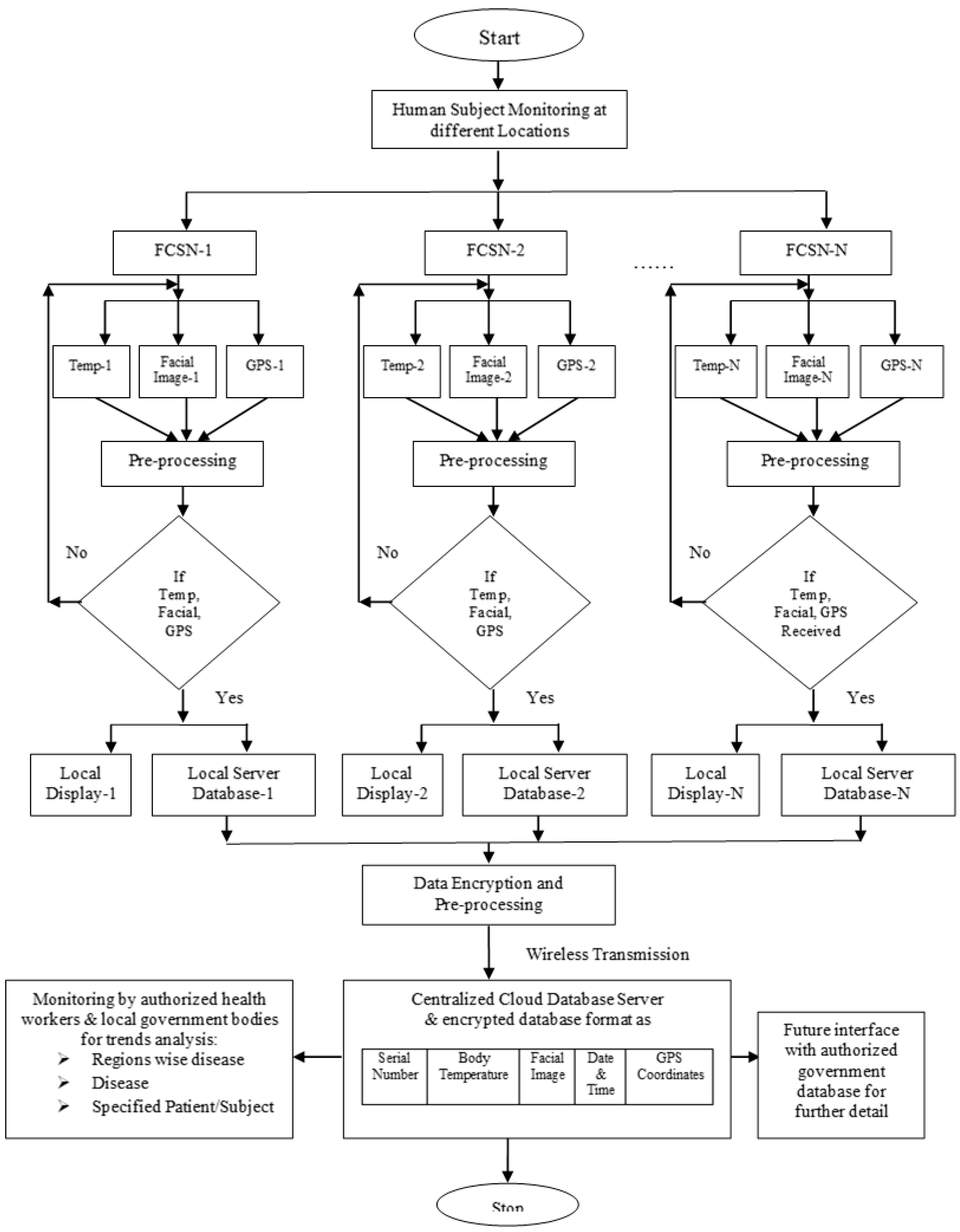
3.3. Working Methodology
- Step 1
- Installation of N-FCSN system nodes at N-locations
- Step 2
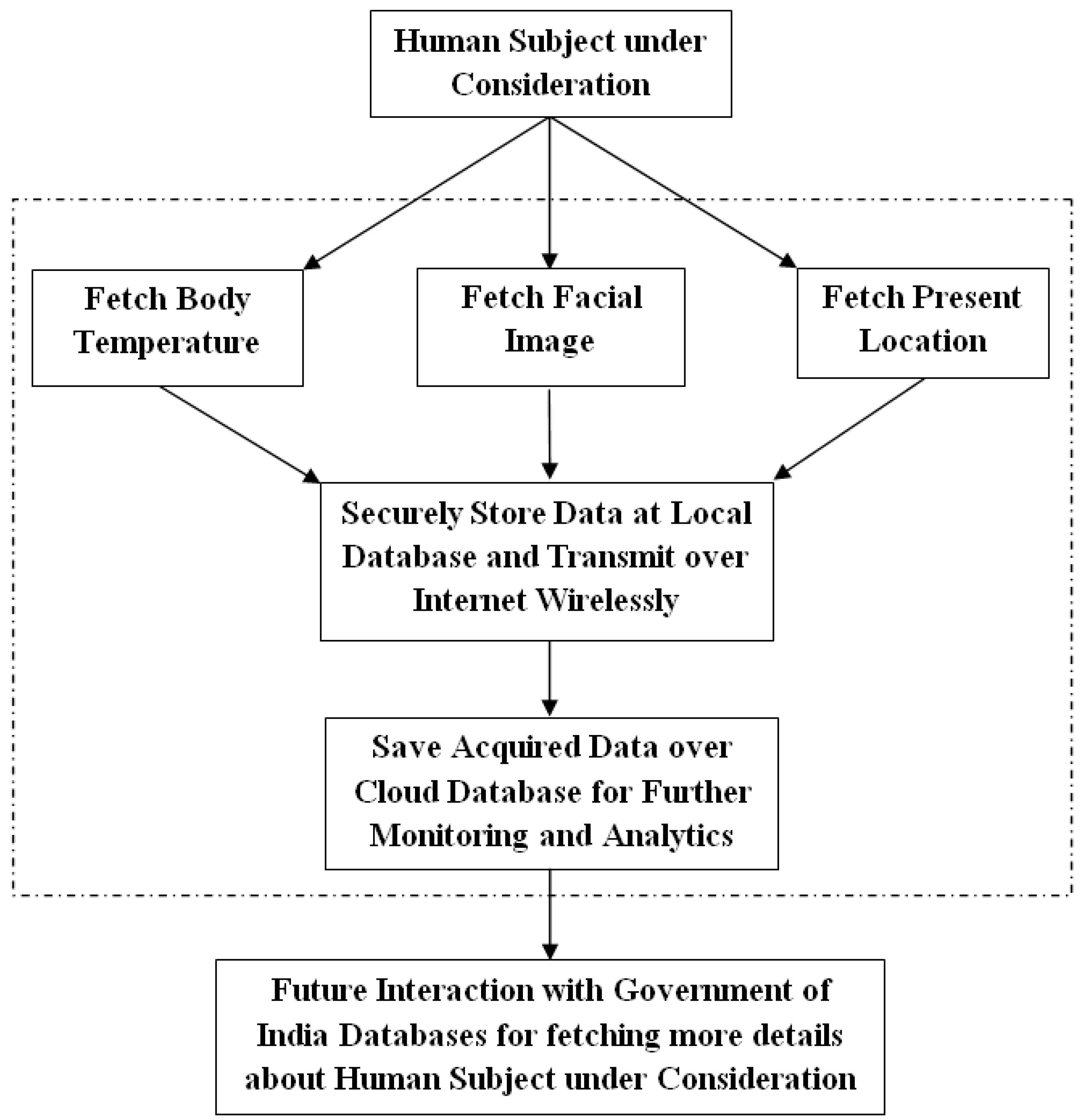
- At different locations, health and social data is fetched by each FCSN system node with click buttons provided such as:
- Fetch social data as a facial image by contactless means through the attached camera with FCSN.
- Fetch human body temperature by contactless means using an infrared thermopile attached with FCSN.
- Fetch present location of screening using GPS locating sensor attached with FCSN where facial image and temperature were fetched.
- Step 3
- Thereceived data is pre-processed and if the proper data cannot be fetched at a particular FCSN node location, then Step-2 is repeated at the respective location.
- Step 4
- The fetched data is displayed on the local display screen with each FCSN and also stored on the local database server in the prescribed format.
- Step 5
- The received data is then encrypted to secure transmission and pre-processing is performed to remove any redundancy.
- Step 6
- Transmission of encrypted data from FCSNs deployed at different locations to cloud databases using a wireless internet connection.
- Step 7
- At the centralized cloud database server, the social facial image, health data and location of capture are stored for run time monitoring and analysis by the authorized health worker and local government officials.
4. Results Analysis
4.1. Data Collection and Analysis
4.2. Statistical Analysis of User Satisfaction
4.3. Discussion
5. Conclusions and Future Work
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sr No | Symbol or Notation | Detail |
|---|---|---|
| 1 | IoT | Internet of Things |
| 2 | SARS | Severe Acute Respiratory Syndrome |
| 3 | FCMN | Fog Computing Based Multi Node |
| 4 | NICU | Neonatal Intensive Care Unit |
| 5 | GPS | Global Positioning Satellite |
| 6 | FCSN | Fog Computing based Single Node |
| 7 | PD | Proposed Device |
| 8 | SD | Standard Device |
| 9 | ABS | Absolute |
| 10 | G(T) | Graduates (Technical) |
| 11 | G(NT) | Graduates (Non-Technical) |
| 12 | UG(T) | Under Graduates (Technical) |
| 13 | UG (NT) | Under Graduates (Non-Technical) |
| 14 | CG | Caregiver Group |
| 15 | TM | Temperature Measurement |
| 16 | HE | Handling Easiness |
| 17 | LI | Location Identification |
| 18 | FIU | Facial Image Utilization |
| 19 | DR | Data Recording |
| 20 | DV | Data Visualization |
| 21 | SD | Standard Deviation |
References
- Adhikari, S.P.; Meng, S.; Wu, Y.-J.; Mao, Y.-P.; Ye, R.-X.; Wang, Q.-Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Wu, T.; Liu, Q.; Yang, Z. The SARS-CoV-2 outbreak: What we know. Int. J. Infect. Dis. 2020, 94, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Anzai, A.; Kobayashi, T.; Linton, N.M.; Kinoshita, R.; Hayashi, K.; Suzuki, A.; Yang, Y.; Jung, S.-M.; Miyama, T.; Akhmetzhanov, A.R.; et al. Assessing the Impact of Reduced Travel on Exportation Dynamics of Novel Coronavirus Infection (COVID-19). J. Clin. Med. 2020, 9, 601. [Google Scholar] [CrossRef] [PubMed]
- Aiyegbusi, O.L.; Hughes, S.E.; Turner, G.; Rivera, S.C.; McMullan, C.; Chandan, J.S.; Haroon, S.; Price, G.; Davies, E.H.; Nirantharakumar, K.; et al. Symptoms, complications and management of long COVID: A review. J. R. Soc. Med. 2021, 114, 428–442. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-2019) Situation Reports. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 5 May 2022).
- Government of India. COVID-19 Tracker INDIA. Available online: https://www.mygov.in/covid-19 (accessed on 10 May 2022).
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Diseases 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Durankuş, F.; Aksu, E. Effects of the COVID-19 pandemic on anxiety and depressive symptoms in pregnant women: A preliminary study. J. Matern. Neonatal Med. 2020, 35, 205–211. [Google Scholar] [CrossRef]
- Kwon, J.; Azad, A. More than 140 seemingly recovered patients have retested positive for Covid-19, says South Korea. CNN Health News, 16 April 2020. [Google Scholar]
- Liu, S.; Yang, L.; Zhang, C.; Xiang, Y.-T.; Liu, Z.; Hu, S.; Zhang, B. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, E17–E18. [Google Scholar] [CrossRef]
- Polas, M.R.H.; Raju, V. Technology and Entrepreneurial Marketing Decisions During COVID-19. Glob. J. Flex. Syst. Manag. 2020, 22, 95–112. [Google Scholar] [CrossRef]
- Intawong, K.; Olson, D.; Chariyalertsak, S. Application technology to fight the COVID-19 pandemic: Lessons learned in Thailand. Biochem. Biophys. Res. Commun. 2021, 534, 830–836. [Google Scholar] [CrossRef]
- Menni, C.; Valdes, A.M.; Freidin, M.B.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Ganesh, S.; Varsavsky, T.; Cardoso, M.J.; El-Sayed Moustafa, J.S.; et al. Real-time tracking of self-reported symptoms to predict potential COVID-19. Nat. Med. 2020, 26, 1037–1040. [Google Scholar] [CrossRef]
- He, W.; Zhang, Z.; Li, W. Information technology solutions, challenges, and suggestions for tackling the COVID-19 pandemic. Int. J. Inf. Manag. 2021, 57, 102287. [Google Scholar] [CrossRef] [PubMed]
- Vargo, D.; Zhu, L.; Benwell, B.; Yan, Z. Digital technology use during COVID-19 pandemic: A rapid review. Hum. Behav. Emerg. Technol. 2021, 3, 13–24. [Google Scholar] [CrossRef]
- Ranjha, A.; Kaddoum, G. URLLC-Enabled by Laser Powered UAV Relay: A Quasi-Optimal Design of Resource Allocation, Trajectory Planning and Energy Harvesting. IEEE Trans. Veh. Technol. 2022, 71, 753–765. [Google Scholar] [CrossRef]
- Epstein, Y.; Moran, D.S. Extremes of temperature and hydration. In Travel Medicine, 4th ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Noyes, F.R.; Barber-Westin, S.D. Diagnosis and treatment of complex regional pain syndrome. In Noyes’ Knee Disorders: Surgery, Rehabilitation, Clinical Outcomes, 2nd ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Beyala, L. Comprehensive risk analysis process. In Connected Objects in Health; Elsevier Inc.: Amsterdam, The Netherlands, 2017; pp. 23–51. [Google Scholar]
- Hu, P.; Ning, H.; Qiu, T.; Zhang, Y.; Luo, X. Fog Computing Based Face Identification and Resolution Scheme in Internet of Things. IEEE Trans. Ind. Inform. 2017, 13, 1910–1920. [Google Scholar] [CrossRef]
- Kumar, P.M.; Gandhi, U.; Varatharajan, R.; Manogaran, G.R.; Vadivel, T. Intelligent face recognition and navigation system using neural learning for smart security in Internet of Things. Clust. Comput. 2019, 22, 7733–7744. [Google Scholar] [CrossRef]
- Kaur, H.; Sood, S.K. Fog-assisted IoT-enabled scalable network infrastructure for wildfire surveillance. J. Netw. Comput. Appl. 2019, 144, 171–183. [Google Scholar] [CrossRef]
- Kaur, H.; Sood, S.K. Cloud-Fog based framework for drought prediction and forecasting using artificial neural network and genetic algorithm. J. Exp. Theor. Artif. Intell. 2020, 32, 273–289. [Google Scholar] [CrossRef]
- Javed, S.; Ghazala, S.; Faseeha, U. Perspectives perspectives of heat stroke shield: An iot based solution for the detection and preliminary treatment of heat stroke. Eng. Technol. Appl. Sci. Res. 2020, 10, 5576–5580. [Google Scholar] [CrossRef]
- Kumar, A.; Sharma, S.; Goyal, N.; Singh, A.; Cheng, X.; Singh, P. Secure and energy-efficient smart building architecture with emerging technology IoT. Comput. Commun. 2021, 176, 207–217. [Google Scholar] [CrossRef]
- Dave, M.; Rastogi, V.; Miglani, M.; Saharan, P.; Goyal, N. Smart Fog-Based Video Surveillance with Privacy Preservation based on Blockchain. Wirel. Pers. Commun. 2022, 124, 1677–1694. [Google Scholar] [CrossRef]
- Kshirsgar, P.; More, V.; Hendre, V.; Chippalkatti, P.; Paliwal, K. IOT Based Baby Incubator for Clinic; Lecture Notes in Electrical Engineering; Springer: Berlin/Heidelberg, Germany, 2020; Volume 570, pp. 349–355. [Google Scholar]
- Wijaya, N.H.; Fauzi, F.A.T.; Helmy, E.; Nguyen, P.T.; Atmoko, R.A. The design of heart rate detector and body temperature measurement device using ATMega16. J. Robot. Control. 2020, 1, 40–43. [Google Scholar] [CrossRef]
- Ranjha, A.; Nguyen, T.N.; Javed, M.A. AECT: Accurate Energy Efficient Contact Tracing Using Smart Phones for Infectious Disease Detection. ACM Trans. Sens. Netw. 2022, 1–13. [Google Scholar] [CrossRef]
- Zhang, J.; Xiao, W.; Li, Y. Data and Knowledge Twin Driven Integration for Large-Scale Device-Free Localization. IEEE Internet Things 2021, 8, 320–331. [Google Scholar] [CrossRef]
- Khullar, V.; Singh, H.P.; Bala, M. Intelligent Handheld Expert System (HES) for Diagnosis of Autism Spectrum Disorder and its Severity Level. ASEAN J. Psychiatry 2018, 19, 12–26. [Google Scholar]
- Khullar, V.; Singh, H.P.; Bala, M. Deep Neural Network-based Handheld Diagnosis System for Autism Spectrum Disorder. Neurol. India 2019, 69, 66. [Google Scholar] [CrossRef]
- Tableau. Available online: https://www.tableau.com/support/releases/desktop/2020.1 (accessed on 5 May 2022).
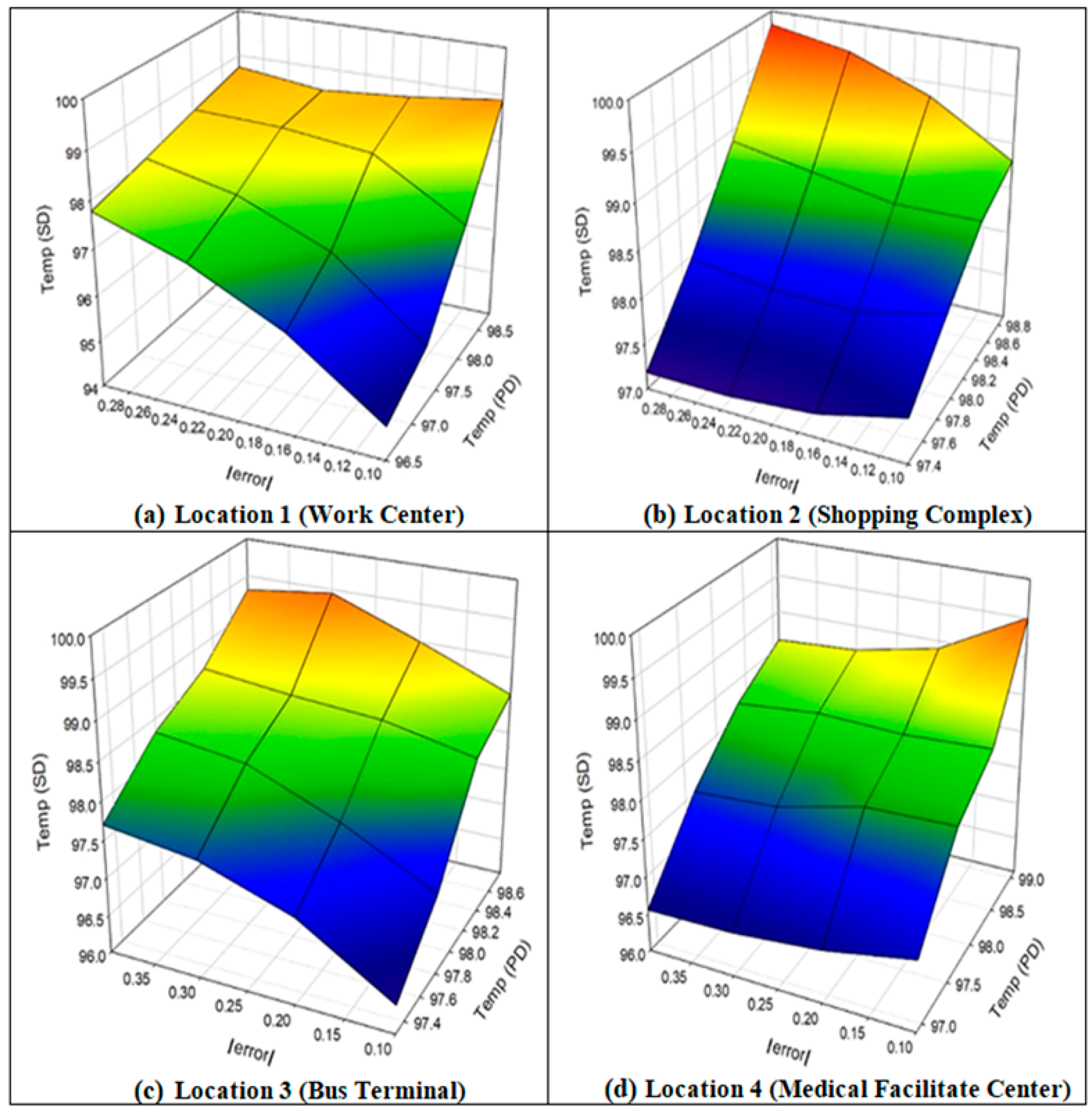
| Test Number | Body Temperature (Measured in Degrees Fahrenheit) | |||||||
|---|---|---|---|---|---|---|---|---|
| Location 1 (Work Center) | Location 2 (Shopping Complex) | Location 3 (Bus Terminal) | Location 4 (Medical Center) | |||||
| Proposed Device (PD) | Standard Device (SD) | Proposed Device (PD) | Standard Device (SD) | Proposed Device (PD) | Standard Device (SD) | Proposed Device (PD) | Standard Device (SD) | |
| 1 | 98.3 | 98.5 | 98.1 | 98.2 | 97.3 | 97.7 | 98.1 | 98.2 |
| 2 | 98.7 | 98.6 | 98.3 | 98.5 | 98.7 | 98.5 | 96.9 | 96.7 |
| 3 | 98.4 | 98.3 | 98.2 | 98.5 | 98.6 | 98.7 | 97.9 | 98.1 |
| 4 | 98.2 | 98.5 | 97.6 | 97.4 | 98.5 | 98.7 | 98.6 | 98.5 |
| 5 | 98.5 | 98.6 | 98.9 | 98.8 | 98.2 | 98.5 | 98.7 | 98.8 |
| 6 | 96.5 | 96.7 | 98.3 | 98.4 | 98.8 | 99.0 | 99.1 | 98.9 |
| 7 | 98.6 | 98.5 | 97.4 | 97.2 | 98.4 | 98.6 | 98.6 | 98.4 |
| 8 | 98.8 | 98.9 | 98.6 | 98.5 | 97.5 | 97.8 | 98.7 | 98.5 |
| 9 | 97.2 | 97.4 | 98.3 | 98.4 | 98.7 | 98.6 | 98.9 | 98.5 |
| 10 | 98.7 | 98.5 | 98.5 | 98.6 | 98.3 | 98.2 | 98.6 | 98.7 |
| Mean Error in Temperature Measurement between Proposed and Standard Devices Mean Error (in Degrees Fahrenheit) | GPS Location Fetched | Facial Image Fetched | Data Received by Server | |
|---|---|---|---|---|
| Location 1 (Work centre) | 0.016 | Yes | Yes | Yes |
| Location 2 (Shopping complex) | 0.015 | Yes | Yes | Yes |
| Location 3 (Bus terminal) | 0.021 | Yes | Yes | Yes |
| Location4 (Medical centre) | 0.018 | Yes | Yes | Yes |
| Average error | 0.07 | No failure identified | ||
| Gender | Total Number of Participants (Age from 18 to 40 Years) | Education Bifurcation of Participants G(T):G(NT):UG (T):UG(NT) |
|---|---|---|
| Male | 15 | 11:5:6:3 |
| Female | 10 |
| CG | TM | HE | LI | FIU | DR | DV | Average |
|---|---|---|---|---|---|---|---|
| 1-G(T) | 7 | 6.5 | 7 | 7 | 8 | 6.5 | 7.0 |
| 2-G(T) | 7 | 7 | 8 | 6 | 5.5 | 6 | 6.6 |
| 3-G(T) | 6 | 6.5 | 5 | 7 | 6 | 5.5 | 6.0 |
| 4-G(T) | 4 | 4.5 | 5 | 4 | 3.5 | 4.5 | 4.3 |
| 5-G(T) | 6.5 | 8 | 5.5 | 5.5 | 6 | 8 | 6.6 |
| 6-G(T) | 6 | 7 | 6 | 6.5 | 8 | 6 | 6.6 |
| 7-G(T) | 8 | 6.5 | 7 | 8 | 8 | 6 | 7.3 |
| 8-G(T) | 9 | 8.5 | 8 | 7 | 7.5 | 8 | 8.0 |
| 9-G(T) | 6 | 8 | 6 | 7 | 7 | 4.5 | 6.4 |
| 10-G(T) | 5 | 7 | 8 | 7 | 8 | 8 | 7.2 |
| 11-G(T) | 8 | 5 | 5 | 5 | 6 | 4 | 5.5 |
| 12-G(NT) | 5 | 6.5 | 6 | 8 | 6 | 6.5 | 6.3 |
| 13-G(NT) | 8 | 6 | 8 | 4 | 8 | 6.5 | 6.8 |
| 14-G(NT) | 6 | 6 | 8 | 6 | 5.5 | 6 | 6.3 |
| 15-G(NT) | 7 | 6 | 6 | 6.5 | 5 | 8 | 6.4 |
| 16-G(NT) | 7 | 5 | 4 | 4.5 | 4 | 4 | 4.8 |
| 17-UG(T) | 8 | 7 | 8.5 | 8 | 8.5 | 8 | 8.0 |
| 18-UG(T) | 7 | 6.5 | 8 | 5 | 6 | 6.5 | 6.5 |
| 19-UG(T) | 8 | 4 | 5 | 5 | 5.5 | 8 | 5.9 |
| 20-UG(T) | 4 | 7 | 7 | 8 | 4 | 7 | 6.2 |
| 21-UG(T) | 8 | 5 | 8 | 4.5 | 7 | 6 | 6.4 |
| 22-UG(T) | 7 | 5.5 | 6 | 6 | 8 | 5 | 6.3 |
| 23-UG(NT) | 6 | 8 | 6 | 6 | 8 | 7 | 6.8 |
| 24-UG(NT) | 6 | 6 | 7 | 6 | 7 | 8 | 6.7 |
| 25-UG(NT) | 7 | 6 | 7.5 | 6.5 | 7 | 6.5 | 6.8 |
| Statistical Parameter | TM | HE | LI | FIU | DR | DV | Overall Average |
|---|---|---|---|---|---|---|---|
| Mean | 6.66 | 6.36 | 6.62 | 6.16 | 6.52 | 6.40 | 6.47 |
| SD | 1.28 | 1.13 | 1.28 | 1.24 | 1.44 | 1.31 | 0.81 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khullar, V.; Singh, H.P.; Miro, Y.; Anand, D.; Mohamed, H.G.; Gupta, D.; Kumar, N.; Goyal, N. IoT Fog-Enabled Multi-Node Centralized Ecosystem for Real Time Screening and Monitoring of Health Information. Appl. Sci. 2022, 12, 9845. https://doi.org/10.3390/app12199845
Khullar V, Singh HP, Miro Y, Anand D, Mohamed HG, Gupta D, Kumar N, Goyal N. IoT Fog-Enabled Multi-Node Centralized Ecosystem for Real Time Screening and Monitoring of Health Information. Applied Sciences. 2022; 12(19):9845. https://doi.org/10.3390/app12199845
Chicago/Turabian StyleKhullar, Vikas, Harjit Pal Singh, Yini Miro, Divya Anand, Heba G. Mohamed, Deepali Gupta, Navdeep Kumar, and Nitin Goyal. 2022. "IoT Fog-Enabled Multi-Node Centralized Ecosystem for Real Time Screening and Monitoring of Health Information" Applied Sciences 12, no. 19: 9845. https://doi.org/10.3390/app12199845
APA StyleKhullar, V., Singh, H. P., Miro, Y., Anand, D., Mohamed, H. G., Gupta, D., Kumar, N., & Goyal, N. (2022). IoT Fog-Enabled Multi-Node Centralized Ecosystem for Real Time Screening and Monitoring of Health Information. Applied Sciences, 12(19), 9845. https://doi.org/10.3390/app12199845