

Adult Asthma Management in the Emergency Department during COVID-19 Pandemic: An Expert Opinion Survey

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
- The “COVID-19 path” for asthma patients in the ED;
- Management of the adult patients with asthma in the ED at the time of the COVID-19 pandemic;
- The role of innovative respiratory hubs and telemedicine in the follow-up of adult patients with severe asthma after discharge from the ED.
3. Results of the Survey
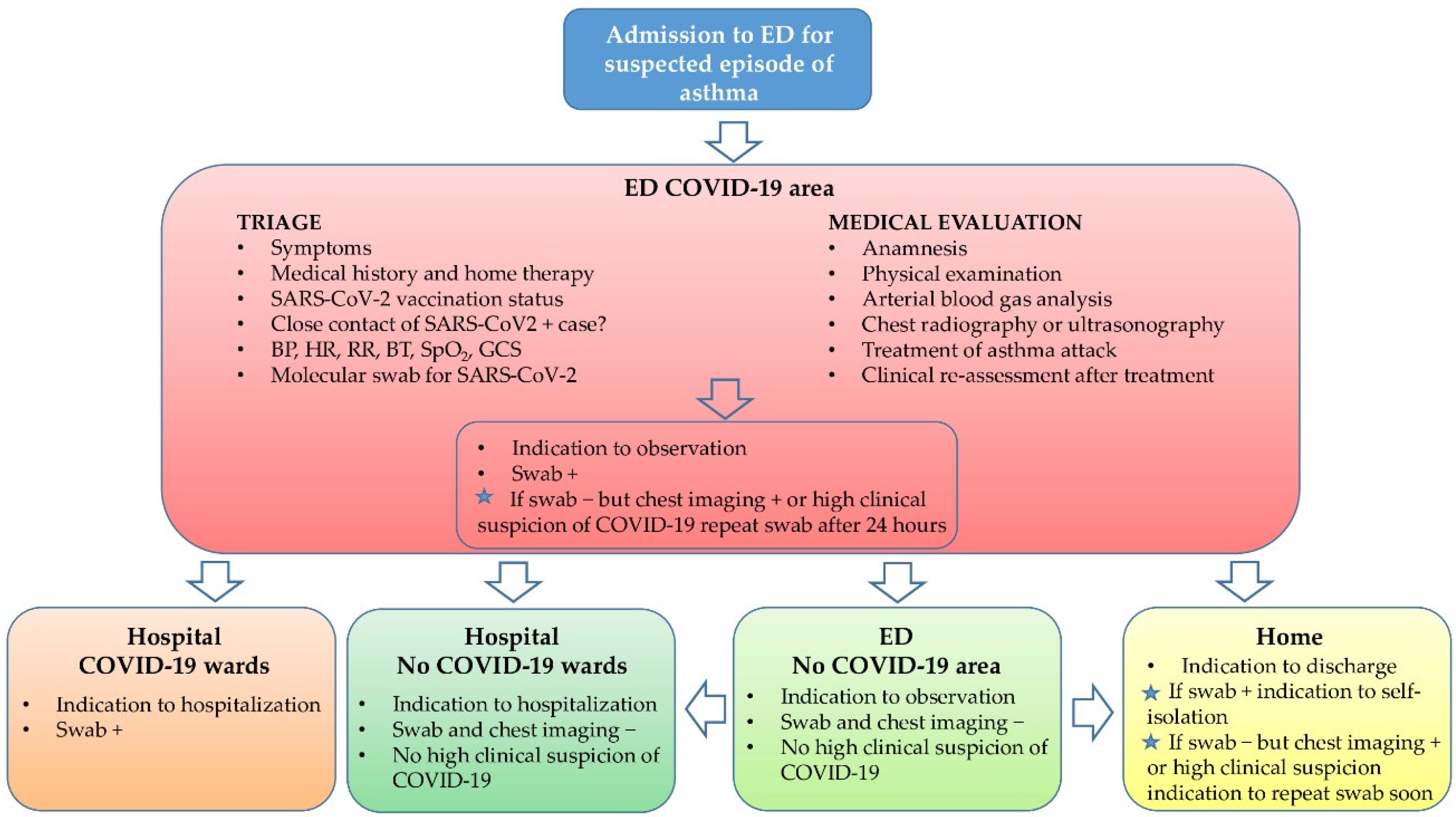
3.1. The “COVID-19 Path” for Asthma Patients in the ED
3.2. Management of Adult Patients with Asthma in the ED at the Time of COVID-19 Pandemic
3.2.1. Assessing Patients’ Symptoms
3.2.2. Asthma and COVID-19: What We Know Today
3.2.3. Medical Treatment of Severe Asthma Exacerbations in the COVID-19 Era in the Emergency Department
3.2.4. Hospitalization and Discharge of Asthmatic Patients during COVID-19 Disease
- (1)
- Respiratory failure, severe respiratory distress, cyanosis, use of accessory muscles and altered mental status with impaired consciousness, after treatment and reassessment;
- (2)
- Hypoxia with SpO2 < 92% after treatment and elevated PCO2 > 45 mmHg; near fatal asthma; presence of complications (e.g., pneumothorax, pneumomediastinum, atelectasis, arrhythmia);
- (3)
- History of previous severe asthma attacks (e.g., >3 ED visits or >2 hospitalizations in the past 12 months or previous intubation or management in ICU for asthma);
- (4)
- Poor family support or difficulty in reaching the hospital in case of further deterioration;
- (5)
- Significant medical comorbidities; psychological problems with concerns about compliance;
- (6)
- Recent steroid use;
- (1)
- With stable vital signs, partial response to therapy (beta-2 agonists plus steroids in the ED), with clinical improvement but still presence of wheezing;
- (2)
- Who need medical reassessment because they do not improve adequately with the initial therapy;
- (3)
- Whose discharge is unsafe because of concerns about therapy compliance or follow-up.
3.3. The Role of Innovative Respiratory Hubs and Telemedicine in the Follow-Up of Adult Patients with Severe Asthma after Discharge from the ED
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Holgate, S.T.; Wenzel, S.; Postma, D.S.; Weiss, S.T.; Renz, H.; Sly, P.D. Asthma. Nat. Rev. Dis. Primers 2015, 1, 15025. [Google Scholar] [CrossRef] [PubMed]
- McCracken, J.L.; Veeranki, S.P.; Ameredes, B.T.; Calhoun, W.J. Diagnosis and Management of Asthma in Adults: A Review. JAMA 2017, 318, 279–290. [Google Scholar] [CrossRef]
- Reddel, H.K.; Bacharier, L.B.; Bateman, E.D.; Brightling, C.E.; Brusselle, G.G.; Buhl, R.; Cruz, A.A.; Duijts, L.; Drazen, J.M.; FitzGerald, J.M.; et al. Global Initiative for Asthma Strategy 2021: Executive summary and rationale for key changes. Eur. Respir. J. 2022, 59, S1–S18. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur. Respir. J. 2014, 43, 343–373. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, F.R.; Guglielmelli, E.; Angelini, D.; Cicchini, C.; Castaldo, E.; Di Girolamo, F.; Fedeli, A.; Ronzoni, D.; Rumi, F.; Franceschi, F. Pharmacoeconomic management of patient with severe asthma in the Emergency Department: Retrospective multicentric and cost of illness study. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 11729–11739. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Long, B.; Carius, B.M.; Chavez, S.; Liang, S.Y.; Brady, W.J.; Koyfman, A.; Gottlieb, M. Clinical update on COVID-19 for the emergency clinician: Presentation and evaluation. Am. J. Emerg. Med. 2022, 54, 46–57. [Google Scholar] [CrossRef]
- Grasselli, G.; Tonetti, T.; Protti, A.; Langer, T.; Girardis, M.; Bellani, G.; Laffey, J.; Carrafiello, G.; Carsana, L.; Rizzuto, C.; et al. Pathophysiology of COVID-19-associated acute respiratory distress syndrome: A multicentre prospective observational study. Lancet Respir. Med. 2020, 8, 1201–1208. [Google Scholar] [CrossRef]
- Mantica, G.; Riccardi, N.; Terrone, C.; Gratarola, A. Non-COVID-19 admissions to the emergency department during the pandemic second wave in Italy: What is changed from the first wave? Am. J. Emerg. Med. 2021, 45, 625–626. [Google Scholar] [CrossRef]
- Busse, W.W.; Lemanske, R.F., Jr.; Gern, J.E. Role of viral respiratory infections in asthma and asthma exacerbations. Lancet 2010, 376, 826–834. [Google Scholar] [CrossRef]
- Yin, Y.; Wunderink, R.G. MERS, SARS and other coronaviruses as causes of pneumonia. Respirology 2018, 23, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Gabrielli, M.; Pignataro, G.; Candelli, M.; Sacco Fernandez, M.; Bizzarri, M.; Esperide, A.; Franceschi, F.; Gemelli Against, C. Asthma in patients admitted to emergency department for COVID-19: Prevalence and risk of hospitalization. Intern. Emerg. Med. 2022, 17, 917–920. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Yu, P.; Li, Y.; Wang, J.; Li, Z.; Qiu, J.; Cui, L.; Mou, Y.; Sun, Y. Asthma does not influence the severity of COVID-19: A meta-analysis. J. Asthma 2021, 59, 1188–1194. [Google Scholar] [CrossRef] [PubMed]
- McMillan, S.S.; King, M.; Tully, M.P. How to use the nominal group and Delphi techniques. Int. J. Clin. Pharm. 2016, 38, 655–662. [Google Scholar] [CrossRef]
- Möckel, M.; Corman, V.M.; Stegemann, M.S.; Hofmann, J.; Stein, A.; Jones, T.C.; Gastmeier, P.; Seybold, J.; Offermann, R.; Bachmann, U.; et al. SARS-CoV-2 antigen rapid immunoassay for diagnosis of COVID-19 in the emergency department. Biomarkers 2021, 26, 213–220. [Google Scholar] [CrossRef]
- Hanson, K.E.; Altayar, O.; Caliendo, A.M.; Arias, C.A.; Englund, J.A.; Hayden, M.K.; Lee, M.J.; Loeb, M.; Patel, R.; El Alayli, A.; et al. The Infectious Diseases Society of America Guidelines on the Diagnosis of COVID-19: Antigen Testing. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Cloutier, M.M.; Dixon, A.E.; Krishnan, J.A.; Lemanske, R.F., Jr.; Pace, W.; Schatz, M. Managing Asthma in Adolescents and Adults: 2020 Asthma Guideline Update From the National Asthma Education and Prevention Program. JAMA 2020, 324, 2301–2317. [Google Scholar] [CrossRef]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef]
- Lee, E.Y.P.; Ng, M.Y.; Khong, P.L. COVID-19 pneumonia: What has CT taught us? Lancet Infect. Dis. 2020, 20, 384–385. [Google Scholar] [CrossRef]
- Jacobi, A.; Chung, M.; Bernheim, A.; Eber, C. Portable chest X-ray in coronavirus disease-19 (COVID-19): A pictorial review. Clin. Imaging 2020, 64, 35–42. [Google Scholar] [CrossRef]
- Islam, N.; Ebrahimzadeh, S.; Salameh, J.P.; Kazi, S.; Fabiano, N.; Treanor, L.; Absi, M.; Hallgrimson, Z.; Leeflang, M.M.; Hooft, L.; et al. Thoracic imaging tests for the diagnosis of COVID-19. Cochrane Database Syst. Rev. 2021, 3, Cd013639. [Google Scholar] [CrossRef] [PubMed]
- Beasley, R.; Hills, T.; Kearns, N. Asthma and COVID-19: Preconceptions about Predisposition. Am. J. Respir. Crit. Care Med. 2021, 203, 799–801. [Google Scholar] [CrossRef] [PubMed]
- Beaney, T.; Salman, D.; Samee, T.; Mak, V. Assessment and management of adults with asthma during the covid-19 pandemic. BMJ 2020, 369, m2092. [Google Scholar] [CrossRef] [PubMed]
- Alberca, R.W.; Yendo, T.; Aoki, V.; Sato, M.N. Asthmatic patients and COVID-19: Different disease course? Allergy 2021, 76, 963–965. [Google Scholar] [CrossRef]
- Mendes, N.F.; Jara, C.P.; Mansour, E.; Araújo, E.P.; Velloso, L.A. Asthma and COVID-19: A systematic review. Allergy Asthma Clin. Immunol. 2021, 17, 5. [Google Scholar] [CrossRef]
- Mikhail, I.; Grayson, M.H. Asthma and viral infections: An intricate relationship. Ann. Allergy Asthma Immunol. 2019, 123, 352–358. [Google Scholar] [CrossRef]
- Mauer, Y.; Taliercio, R.M. Managing adult asthma: The 2019 GINA guidelines. Clevel. Clin. J. Med. 2020, 87, 569–575. [Google Scholar] [CrossRef]
- Saglani, S.; Menzie-Gow, A.N. Approaches to Asthma Diagnosis in Children and Adults. Front. Pediatr. 2019, 7, 148. [Google Scholar] [CrossRef]
- Drake, S.M.; Simpson, A.; Fowler, S.J. Asthma Diagnosis: The Changing Face of Guidelines. Pulm. Ther. 2019, 5, 103–115. [Google Scholar] [CrossRef]
- Ish, P.; Malhotra, N.; Gupta, N. GINA 2020: What’s new and why? J. Asthma 2021, 58, 1273–1277. [Google Scholar] [CrossRef]
- Boulet, L.P.; Reddel, H.K.; Bateman, E.; Pedersen, S.; FitzGerald, J.M.; O’Byrne, P.M. The Global Initiative for Asthma (GINA): 25 years later. Eur. Respir. J. 2019, 54, 1900598. [Google Scholar] [CrossRef] [PubMed]
- Bonser, L.R.; Eckalbar, W.L.; Rodriguez, L.; Shen, J.; Koh, K.D.; Ghias, K.; Zlock, L.T.; Christenson, S.; Woodruff, P.G.; Finkbeiner, W.E.; et al. The Type 2 Asthma Mediator IL-13 Inhibits Severe Acute Respiratory Syndrome Coronavirus 2 Infection of Bronchial Epithelium. Am. J. Respir. Cell Mol. Biol. 2022, 66, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.B.; Wang, L.; Fu, X.; Wallace, Z.S.; Long, A.A.; Zhang, Y.; Camargo, C.A., Jr.; Blumenthal, K.G. COVID-19 severity in asthma patients: A multi-center matched cohort study. J. Asthma 2022, 59, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Lee, S.; Krings, J.G.; Rauseo, A.M.; Reynolds, D.; Presti, R.; Goss, C.; Mudd, P.A.; O’Halloran, J.A.; Wang, L. Asthma in patients with suspected and diagnosed coronavirus disease 2019. Ann. Allergy Asthma Immunol. 2021, 126, 535–541.e2. [Google Scholar] [CrossRef]
- Sunjaya, A.P.; Allida, S.M.; Di Tanna, G.L.; Jenkins, C. Asthma and risk of infection, hospitalization, ICU admission and mortality from COVID-19: Systematic review and meta-analysis. J. Asthma 2022, 59, 866–879. [Google Scholar] [CrossRef]
- Liu, S.; Cao, Y.; Du, T.; Zhi, Y. Prevalence of Comorbid Asthma and Related Outcomes in COVID-19: A Systematic Review and Meta-Analysis. J. Allergy Clin. Immunol. Pract. 2021, 9, 693–701. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, J.; Chen, W.; Liu, L.; Dong, M.; Ji, J.; Hu, D.; Zhang, N. Does Asthma Increase the Mortality of Patients with COVID-19?: A Systematic Review and Meta-Analysis. Int. Arch. Allergy Immunol. 2021, 182, 76–82. [Google Scholar] [CrossRef]
- Garcia-Pachon, E.; Grau-Delgado, J.; Soler-Sempere, M.J.; Zamora-Molina, L.; Baeza-Martinez, C.; Ruiz-Alcaraz, S.; Padilla-Navas, I. Low prevalence of post-COVID-19 syndrome in patients with asthma. J. Infect. 2021, 82, 276–316. [Google Scholar] [CrossRef]
- Skene, I.P.; Pfeffer, P.E. Improved asthma control during the COVID-19 pandemic: Are there lessons to be learnt? Thorax 2021, 76, 852–853. [Google Scholar] [CrossRef]
- Kannan, S.; Shaik Syed Ali Pakeer, P.; Sheeza Ali, A.; Hemalatha, K. Reply Letter—COVID-19 (Novel Coronavirus 2019)—Recent trends. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 6482–6483. [Google Scholar] [CrossRef]
- Eguiluz-Gracia, I.; van den Berge, M.; Boccabella, C.; Bonini, M.; Caruso, C.; Couto, M.; Erkekol, F.; Rukhadze, M.; Sanchez-Garcia, S.; Del Giacco, S.; et al. Real-life impact of COVID-19 pandemic lockdown on the management of pediatric and adult asthma: A survey by the EAACI Asthma Section. Allergy 2021, 76, 2776–2784. [Google Scholar] [CrossRef]
- Wang, L.; Wang, Y.; Ye, D.; Liu, Q. Review of the 2019 novel coronavirus (SARS-CoV-2) based on current evidence. Int. J. Antimicrob. Agents 2020, 55, 105948. [Google Scholar] [CrossRef]
- Wu, D.; Wu, T.; Liu, Q.; Yang, Z. The SARS-CoV-2 outbreak: What we know. Int. J. Infect. Dis. 2020, 94, 44–48. [Google Scholar] [CrossRef]
- Singhal, T. A Review of Coronavirus Disease-2019 (COVID-19). Indian J. Pediatr. 2020, 87, 281–286. [Google Scholar] [CrossRef]
- Ashour, H.M.; Elkhatib, W.F.; Rahman, M.M.; Elshabrawy, H.A. Insights into the Recent 2019 Novel Coronavirus (SARS-CoV-2) in Light of Past Human Coronavirus Outbreaks. Pathogens 2020, 9, 186. [Google Scholar] [CrossRef]
- Ferastraoaru, D.; Hudes, G.; Jerschow, E.; Jariwala, S.; Karagic, M.; de Vos, G.; Rosenstreich, D.; Ramesh, M. Eosinophilia in Asthma Patients Is Protective Against Severe COVID-19 Illness. J. Allergy Clin. Immunol. Pract. 2021, 9, 1152–1162.e1153. [Google Scholar] [CrossRef]
- Lafaurie, M.; Martin-Blondel, G.; Delobel, P.; Kamar, N.; Charpentier, S.; Sommet, A.; Moulis, G. Impact of previous exposure to systemic corticosteroids on unfavorable outcome in patients hospitalized for COVID-19. BMC Pharmacol. Toxicol. 2021, 22, 14. [Google Scholar] [CrossRef]
- Halpin, D.M.G.; Singh, D.; Hadfield, R.M. Inhaled corticosteroids and COVID-19: A systematic review and clinical perspective. Eur. Respir. J. 2020, 55, 2001009. [Google Scholar] [CrossRef]
- Choi, J.C.; Jung, S.Y.; Yoon, U.A.; You, S.H.; Kim, M.S.; Baek, M.S.; Jung, J.W.; Kim, W.Y. Inhaled Corticosteroids and COVID-19 Risk and Mortality: A Nationwide Cohort Study. J. Clin. Med. 2020, 9, 3406. [Google Scholar] [CrossRef]
- Adir, Y.; Humbert, M.; Saliba, W. COVID-19 risk and outcomes in adult asthmatic patients treated with biologics or systemic corticosteroids: Nationwide real-world evidence. J. Allergy Clin. Immunol. 2021, 148, 361–367.e13. [Google Scholar] [CrossRef]
- Griesel, M.; Wagner, C.; Mikolajewska, A.; Stegemann, M.; Fichtner, F.; Metzendorf, M.I.; Nair, A.A.; Daniel, J.; Fischer, A.L.; Skoetz, N. Inhaled corticosteroids for the treatment of COVID-19. Cochrane Database Syst. Rev. 2022, 3, Cd015125. [Google Scholar] [CrossRef] [PubMed]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Shi, L.; Xu, J.; Xiao, W.; Wang, Y.; Jin, Y.; Chen, S.; Duan, G.; Yang, H. Asthma in patients with coronavirus disease 2019: A systematic review and meta-analysis. Ann. Allergy Asthma Immunol. 2021, 126, 524–534. [Google Scholar] [CrossRef]
- Busse, W.W.; Fang, J.; Marvel, J.; Tian, H.; Altman, P.; Cao, H. Uncontrolled asthma across GINA treatment steps 2 - 5 in a large US patient cohort. J. Asthma 2022, 59, 1051–1062. [Google Scholar] [CrossRef]
- Kuprys-Lipinska, I.; Kolacinska-Flont, M.; Kuna, P. New approach to intermittent and mild asthma therapy: Evolution or revolution in the GINA guidelines? Clin. Transl. Allergy 2020, 10, 19. [Google Scholar] [CrossRef]
- Motta, L.P.; Silva, P.; Borguezan, B.M.; Amaral, J.; Milagres, L.G.; Bóia, M.N.; Ferraz, M.R.; Mogami, R.; Nunes, R.A.; Melo, P.L. An emergency system for monitoring pulse oximetry, peak expiratory flow, and body temperature of patients with COVID-19 at home: Development and preliminary application. PLoS ONE 2021, 16, e0247635. [Google Scholar] [CrossRef]
- Levin, M.; Ansotegui, I.J.; Bernstein, J.; Chang, Y.S.; Chikhladze, M.; Ebisawa, M.; Fiocchi, A.; Heffler, E.; Martin, B.; Morais-Almeida, M.; et al. Acute asthma management during SARS-CoV2-pandemic 2020. World Allergy Organ J. 2020, 13, 100125. [Google Scholar] [CrossRef] [PubMed]
- Koh, H.P.; Shamsudin, N.S.; Tan, M.M.Y.; Mohd Pauzi, Z. The outcomes and acceptance of pressurized metered-dose inhaler bronchodilators with venturi mask modified spacer in the outpatient emergency department during the COVID-19 pandemic. J. Clin. Pharm. Ther. 2021, 46, 1129–1138. [Google Scholar] [CrossRef]
- Goldstein, K.M.; Ghadimi, K.; Mystakelis, H.; Kong, Y.; Meng, T.; Cantrell, S.; Von Isenburg, M.; Gordon, A.; Ear, B.; Gierisch, J.M.; et al. Risk of Transmitting Coronavirus Disease 2019 During Nebulizer Treatment: A Systematic Review. J. Aerosol. Med. Pulm. Drug Deliv. 2021, 34, 155–170. [Google Scholar] [CrossRef]
- Tran, K.; Cimon, K.; Severn, M.; Pessoa-Silva, C.L.; Conly, J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: A systematic review. PLoS ONE 2012, 7, e35797. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, J.A.; Davis, S.Q.; Naureckas, E.T.; Gibson, P.; Rowe, B.H. An umbrella review: Corticosteroid therapy for adults with acute asthma. Am. J. Med. 2009, 122, 977–991. [Google Scholar] [CrossRef] [PubMed]
- Rowe, B.H.; Spooner, C.H.; Ducharme, F.M.; Bretzlaff, J.A.; Bota, G.W. Corticosteroids for preventing relapse following acute exacerbations of asthma. Cochrane Database Syst. Rev. 2001, 1, Cd000195. [Google Scholar] [CrossRef]
- Rowe, B.H.; Spooner, C.; Ducharme, F.M.; Bretzlaff, J.A.; Bota, G.W. Early emergency department treatment of acute asthma with systemic corticosteroids. Cochrane Database Syst. Rev. 2001, 1, Cd002178. [Google Scholar] [CrossRef] [PubMed]
- Rowe, B.H.; Camargo, C.A., Jr. The role of magnesium sulfate in the acute and chronic management of asthma. Curr. Opin. Pulm. Med. 2008, 14, 70–76. [Google Scholar] [CrossRef]
- Calzetta, L.; Matera, M.G.; Coppola, A.; Rogliani, P. Prospects for severe asthma treatment. Curr. Opin. Pharmacol. 2021, 56, 52–60. [Google Scholar] [CrossRef]
- Papiris, S.A.; Manali, E.D.; Kolilekas, L.; Triantafillidou, C.; Tsangaris, I. Acute severe asthma: New approaches to assessment and treatment. Drugs 2009, 69, 2363–2391. [Google Scholar] [CrossRef]
- Normansell, R.; Sayer, B.; Waterson, S.; Dennett, E.J.; Del Forno, M.; Dunleavy, A. Antibiotics for exacerbations of asthma. Cochrane Database Syst. Rev. 2018, 6, Cd002741. [Google Scholar] [CrossRef]
- Papaioannou, A.I.; Kostikas, K.; Zervas, E.; Kolilekas, L.; Papiris, S.; Gaga, M. Control of asthma in real life: Still a valuable goal? Eur. Respir. Rev. 2015, 24, 361–369. [Google Scholar] [CrossRef]
- Papiris, S.; Kotanidou, A.; Malagari, K.; Roussos, C. Clinical review: Severe asthma. Crit. Care 2002, 6, 30–44. [Google Scholar] [CrossRef]
- Caruso, C.; Colantuono, S.; Urbani, S.; Heffler, E.; Canonica, G.W.; Andriollo, G.; Di Michele, L.; Scarlata, S.; Zennaro, D.; Rigon, A.; et al. Real-life survey on severe asthma patients during COVID-19 lockdown in Italy. Expert Rev. Respir. Med. 2021, 15, 1057–1060. [Google Scholar] [CrossRef]
- Heffler, E.; Detoraki, A.; Contoli, M.; Papi, A.; Paoletti, G.; Malipiero, G.; Brussino, L.; Crimi, C.; Morrone, D.; Padovani, M.; et al. COVID-19 in Severe Asthma Network in Italy (SANI) patients: Clinical features, impact of comorbidities and treatments. Allergy 2021, 76, 887–892. [Google Scholar] [CrossRef]
- Calmes, D.; Graff, S.; Maes, N.; Frix, A.N.; Thys, M.; Bonhomme, O.; Berg, J.; Debruche, M.; Gester, F.; Henket, M.; et al. Asthma and COPD Are Not Risk Factors for ICU Stay and Death in Case of SARS-CoV2 Infection. J. Allergy Clin. Immunol. Pract. 2021, 9, 160–169. [Google Scholar] [CrossRef]
- Toungoussova, O.; Foschino Barbaro, M.P.; Esposito, L.M.; Carpagnano, G.E.; Salerno, F.G.; Dal Negro, R.W.; Spanevello, A. Brittle asthma. Monaldi Arch. Chest Dis. 2007, 67, 102–105. [Google Scholar] [CrossRef]
- Skevaki, C.; Karsonova, A.; Karaulov, A.; Fomina, D.; Xie, M.; Chinthrajah, S.; Nadeau, K.C.; Renz, H. SARS-CoV-2 infection and COVID-19 in asthmatics: A complex relationship. Nat. Rev. Immunol. 2021, 21, 202–203. [Google Scholar] [CrossRef]
- Li, X.; Xu, S.; Yu, M.; Wang, K.; Tao, Y.; Zhou, Y.; Shi, J.; Zhou, M.; Wu, B.; Yang, Z.; et al. Risk factors for severity and mortality in adult COVID-19 inpatients in Wuhan. J. Allergy Clin. Immunol. 2020, 146, 110–118. [Google Scholar] [CrossRef]
- Lu, X.; Chen, T.; Wang, Y.; Wang, J.; Yan, F. Adjuvant corticosteroid therapy for critically ill patients with COVID-19. Crit. Care 2020, 24, 241. [Google Scholar] [CrossRef]
- Lei, Z.; Luo, Q.; Yang, W.; Su, Q.; Zuo, Y. Meta-analysis of competitive antagonists in asthma treatment. Ann. Palliat. Med. 2021, 10, 3235–3246. [Google Scholar] [CrossRef]
- Rogliani, P.; Ritondo, B.L.; Calzetta, L. Triple therapy in uncontrolled asthma: A network meta-analysis of phase III studies. Eur. Respir. J. 2021, 58, 2004233. [Google Scholar] [CrossRef]
- Eggert, L.E.; He, Z.; Collins, W.; Lee, A.S.; Dhondalay, G.; Jiang, S.Y.; Fitzpatrick, J.; Snow, T.T.; Pinsky, B.A.; Artandi, M.; et al. Asthma phenotypes, associated comorbidities, and long-term symptoms in COVID-19. Allergy 2022, 77, 173–185. [Google Scholar] [CrossRef]
- Pérez de Llano, L.; Dacal Rivas, D.; Blanco Cid, N.; Martin Robles, I. Phenotype-Guided Asthma Therapy: An Alternative Approach to Guidelines. J. Asthma Allergy 2021, 14, 207–217. [Google Scholar] [CrossRef]
- Pena, M.E.; Kazan, V.M.; Helmreich, M.N.; Mace, S.E. Care of Respiratory Conditions in an Observation Unit. Emerg. Med. Clin. N. Am. 2017, 35, 625–645. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.; Jit, M.; Warren-Gash, C.; Guthrie, B.; Wang, H.H.X.; Mercer, S.W.; Sanderson, C.; McKee, M.; Troeger, C.; Ong, K.L.; et al. Global, regional, and national estimates of the population at increased risk of severe COVID-19 due to underlying health conditions in 2020: A modelling study. Lancet Glob. Health 2020, 8, e1003–e1017. [Google Scholar] [CrossRef]
- Schatz, M.; Rachelefsky, G.; Krishnan, J.A. Follow-up after acute asthma episodes: What improves future outcomes? J. Emerg. Med. 2009, 37 (Suppl. 2), S42–S50. [Google Scholar] [CrossRef]
- Munoz-Cano, R.; Torrego, A.; Bartra, J.; Sanchez-Lopez, J.; Palomino, R.; Picado, C.; Valero, A. Follow-up of patients with uncontrolled asthma: Clinical features of asthma patients according to the level of control achieved (the COAS study). Eur. Respir. J. 2017, 49, 1501885. [Google Scholar] [CrossRef]
- Bajowala, S.; Shih, J.; Varshney, P.; Elliott, T. The Future of Telehealth for Allergic Disease. J. Allergy Clin. Immunol. Pract. 2022. [Google Scholar] [CrossRef]
- Lin, C.H.; Cerrone, D.A. Shifts in Asthma Evaluation and Management During COVID-19. Curr. Treat. Options Allergy 2022, 9, 42–51. [Google Scholar] [CrossRef]
- Kannan, S.; Shaik Syed Ali, P.; Sheeza, A.; Hemalatha, K. COVID-19 (Novel Coronavirus 2019)—Recent trends. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 2006–2011. [Google Scholar] [CrossRef]
- Bousquet, J.; Jutel, M.; Akdis, C.A.; Klimek, L.; Pfaar, O.; Nadeau, K.C.; Eiwegger, T.; Bedbrook, A.; Ansotegui, I.J.; Anto, J.M.; et al. ARIA-EAACI statement on asthma and COVID-19 (June 2, 2020). Allergy 2021, 76, 689–697. [Google Scholar] [CrossRef]
- Assaf, S.M.; Tarasevych, S.P.; Diamant, Z.; Hanania, N.A. Asthma and severe acute respiratory syndrome coronavirus 2019: Current evidence and knowledge gaps. Curr. Opin. Pulm. Med. 2021, 27, 45–53. [Google Scholar] [CrossRef]
- Adir, Y.; Saliba, W.; Beurnier, A.; Humbert, M. Asthma and COVID-19: An update. Eur. Respir. Rev. 2021, 30, 210152. [Google Scholar] [CrossRef]
- Ong, K.Y.; Tan, T.L.; Chan, A.K.W.; Tan, K.L.L.; Koh, M.S. Managing asthma in the COVID-19 pandemic and current recommendations from professional bodies: A review. J. Asthma 2021, 58, 1536–1543. [Google Scholar] [CrossRef]
- Taillé, C.; Chenivesse, C.; Devouassoux, G.; Bourdin, A.; Garcia, G. Management of asthma during the Coronavirus disease 2019 outbreak. Respir. Med. Res. 2020, 78, 100762. [Google Scholar] [CrossRef]
- British Toracic Society. Advice for Healthcare Professionals Treating People with Asthma (Adults) in Relation to COVID-19. 2020. Available online: https://www.brit-thoracic.org.uk/document-library/quality-improvement/covid-19/bts-advice-for-healthcare-professionals-treating-patients-with-asthma/ (accessed on 18 July 2022).
- GINA Scientific Committee. Global Strategy for Asthma Management and Prevention Updated 2022. 2022. Available online: https://ginasthma.org/wp-content/uploads/2022/07/GINA-Main-Report-2022-FINAL-22-07-01-WMS.pdf (accessed on 18 July 2022).
- National Asthma Council Australia. Australian Asthma Handbook—Managing Asthma during the COVID-19 (SARS-CoV-2) Pandemic 2020. 2021. Available online: https://www.asthmahandbook.org.au/clinical-issues/covid-19 (accessed on 18 July 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]


{kind=link}
| Before COVID-19 Pandemic | During COVID-19 Pandemic | |
|---|---|---|
| First-line chest imaging is indicated in all patients admitted to the ED for symptoms consistent with acute asthma. |  |  |
| PEF measurement is indicated to stratify asthma severity in the ED. | | |
| In adult patients admitted to the ED for asthma, inhaled bronchodilators should be administered as soon as possible, with preference given to pressurized MDI via a spacer. | | |
| Oxygen supplementation is indicated SpO2 is <90%. | | |
| Systemic corticosteroids should be administered as soon as possible in patients with severe asthma exacerbation admitted to the ED. | | |
| Antibiotics per se are not indicated in patients with asthma exacerbations, unless there is clear evidence of bacterial infection/superinfection. | | |
|
Reddel [3] |
|
Sunjaya [35] |
|
|
|
Beaney [23] |
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gabrielli, M.; Saviano, A.; Bonini, M.; Boccabella, C.; Caruso, C.; Ruggieri, M.P.; Bianconi, S.; Fuso, L.; Capuzi, P.; De Marco, F.; et al. Adult Asthma Management in the Emergency Department during COVID-19 Pandemic: An Expert Opinion Survey. Appl. Sci. 2022, 12, 9460. https://doi.org/10.3390/app12199460
Gabrielli M, Saviano A, Bonini M, Boccabella C, Caruso C, Ruggieri MP, Bianconi S, Fuso L, Capuzi P, De Marco F, et al. Adult Asthma Management in the Emergency Department during COVID-19 Pandemic: An Expert Opinion Survey. Applied Sciences. 2022; 12(19):9460. https://doi.org/10.3390/app12199460
Chicago/Turabian StyleGabrielli, Maurizio, Angela Saviano, Matteo Bonini, Cristina Boccabella, Cristiano Caruso, Maria Pia Ruggieri, Simone Bianconi, Leonello Fuso, Pietro Capuzi, Francesca De Marco, and et al. 2022. "Adult Asthma Management in the Emergency Department during COVID-19 Pandemic: An Expert Opinion Survey" Applied Sciences 12, no. 19: 9460. https://doi.org/10.3390/app12199460
APA StyleGabrielli, M., Saviano, A., Bonini, M., Boccabella, C., Caruso, C., Ruggieri, M. P., Bianconi, S., Fuso, L., Capuzi, P., De Marco, F., Franza, L., & Franceschi, F. (2022). Adult Asthma Management in the Emergency Department during COVID-19 Pandemic: An Expert Opinion Survey. Applied Sciences, 12(19), 9460. https://doi.org/10.3390/app12199460