
Long-Term Prosthetic Aftercare of Mandibular Implant-Supported Overdenture

 ,
,  ,
,  , , and
, , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
- Addresses the Oral Rehabilitation Department, School of Dentistry, Tel-Aviv University;
- MISOD treatment;
- Reduced stability and insufficient retention of their former traditional mandibular complete denture;
- Edentulous period concurrent with standard mandibular complete dentures of at least 12 months;
- Classes III–VI resorption of the mandible according to Cawood and Howell (1988, [20]);
- Presence of keratinized mucosa at the future implantation sites.
2.2. Exclusion Criteria
- Stable mandibular denture without patient complaint;
- Lack of available data;
- Edentulous period <12 months;
- Classes I–II resorption of the mandible according to Cawood and Howell (1988, [20]);
- Absence of keratinized mucosa at the future implantation sites.
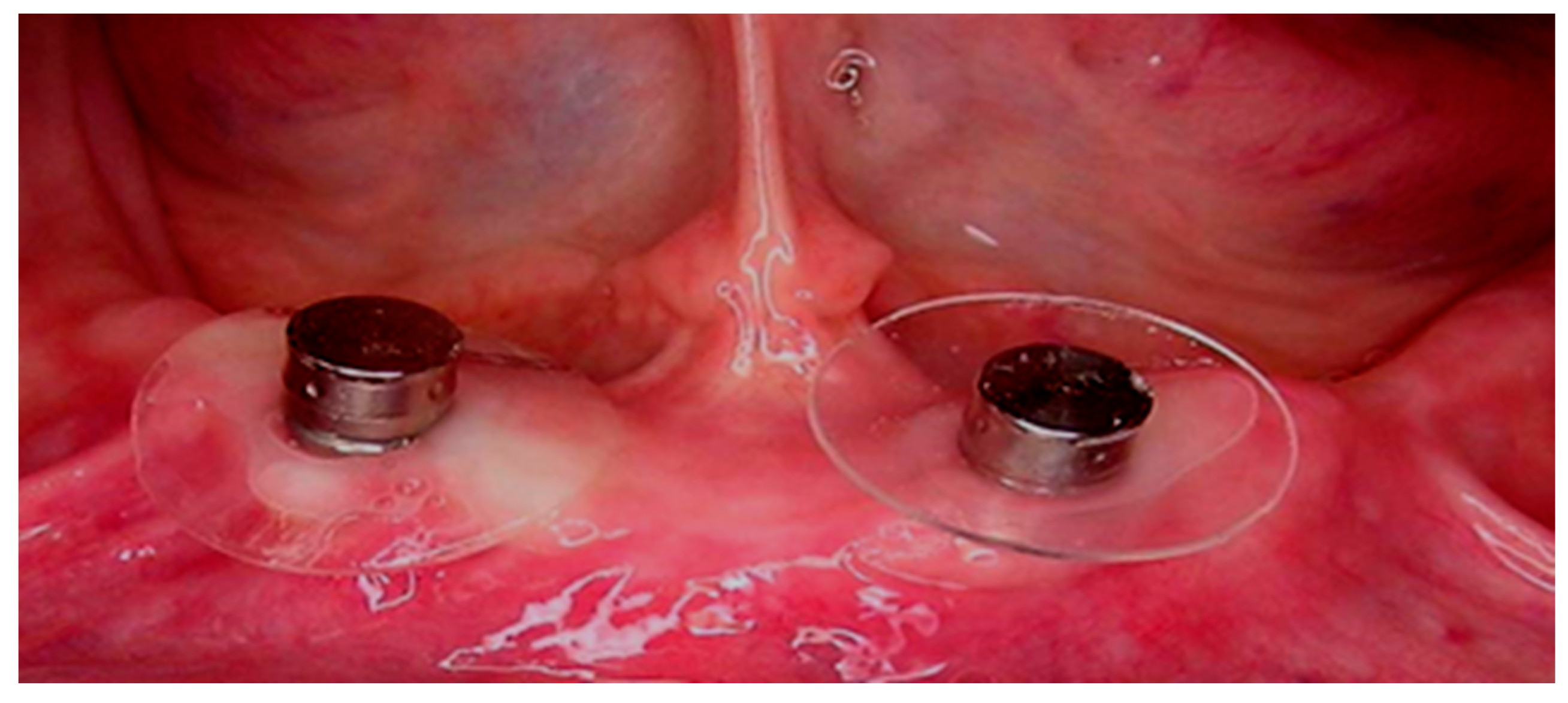
2.3. Surgical Treatment
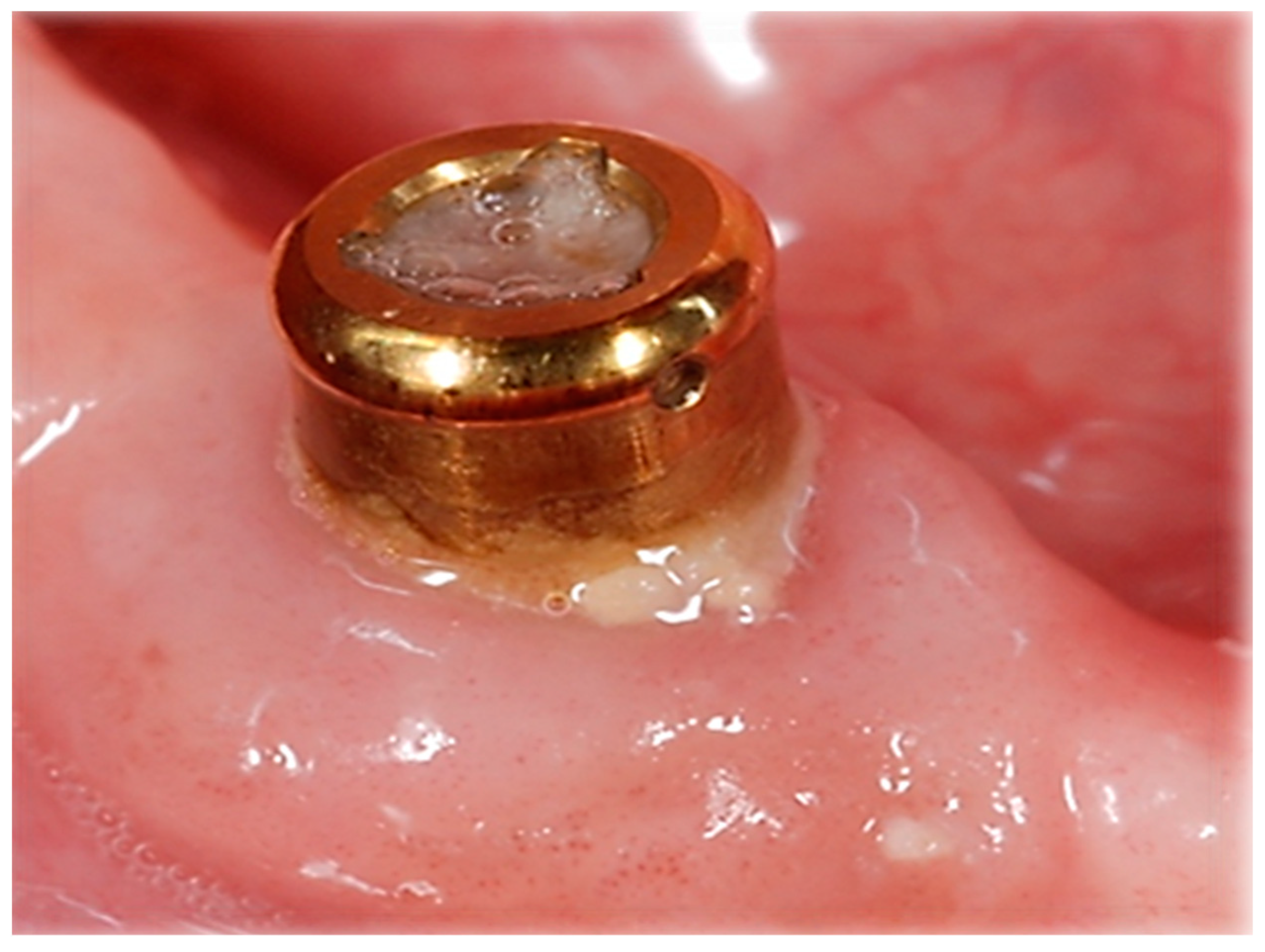
2.4. Prosthetic Treatment
2.5. Follow-Up and Data Collection
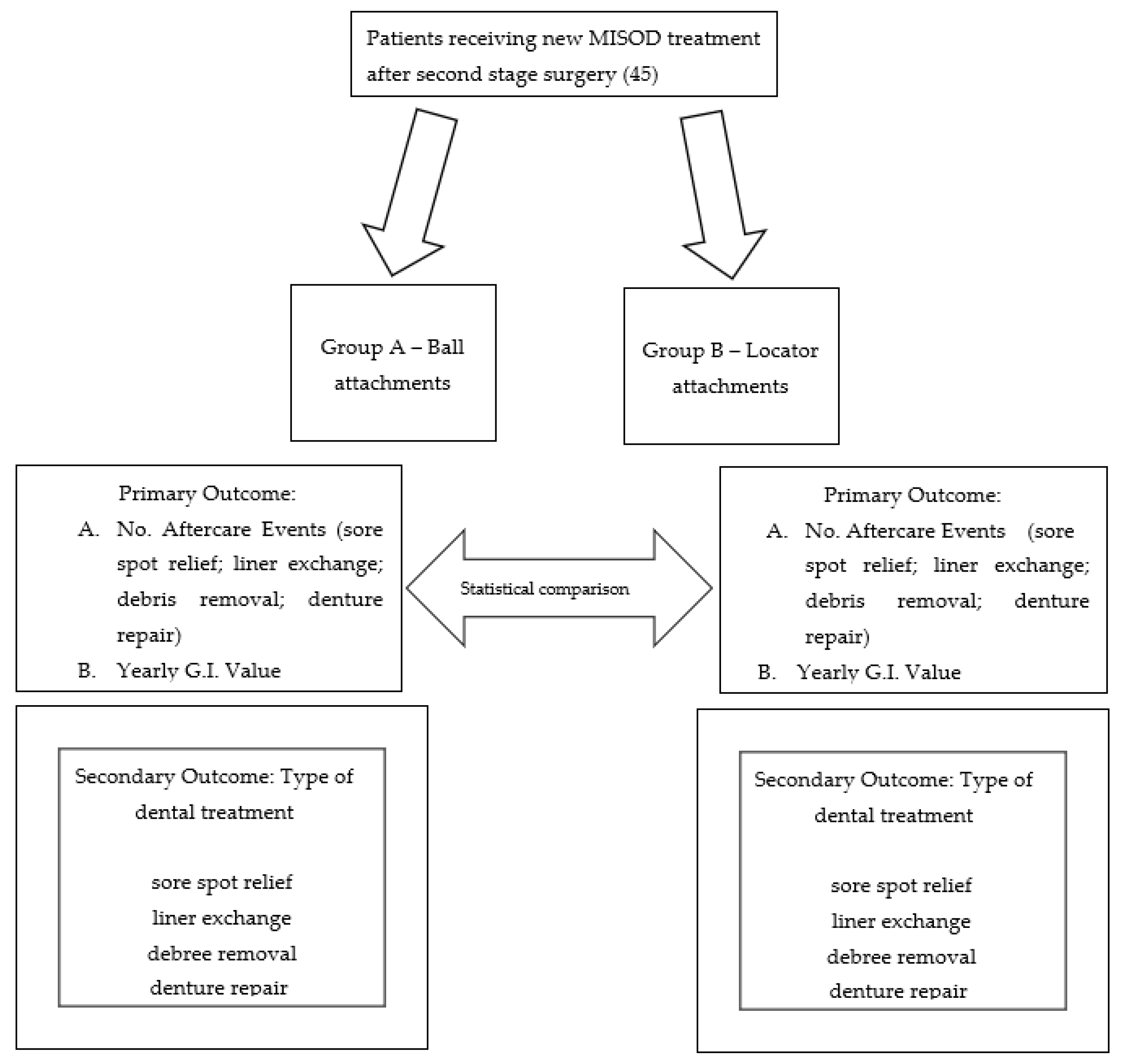
2.6. Outcome Parameters
- Number of aftercare visits—primary outcome parameter;
- Dental treatment received— secondary outcome parameters:
- Pressure sores relief;
- Liner (silicone insert) exchanges due to loss of retention;
- Cleaning debris accumulation after loss of retention;
- Denture repair;
- Oral hygiene (gingival index 0–3 according to Loe and Silness [21])—primary outcome parameter.
2.7. Statistical Analysis
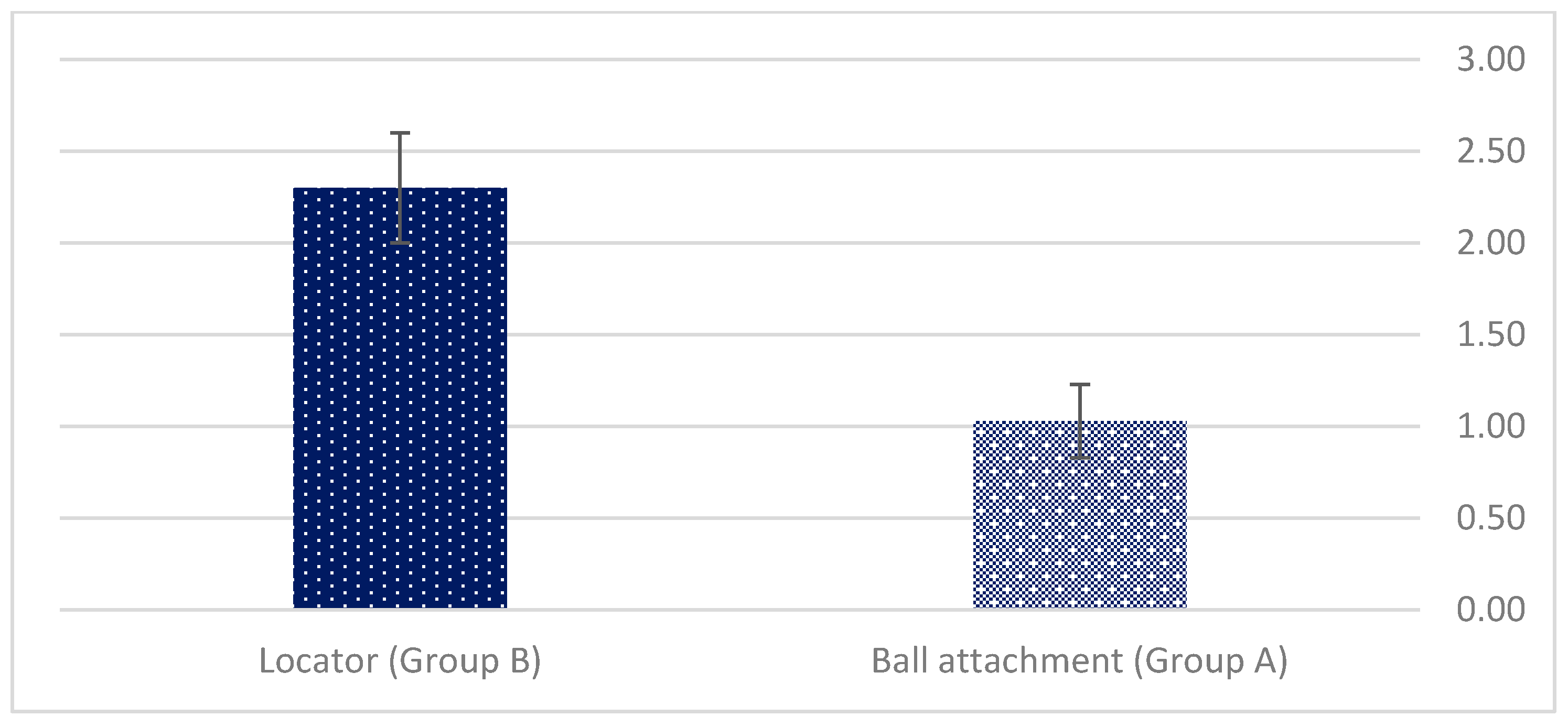
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tyrovolas, S.; Koyanagi, A.; Panagiotakos, D.B.; Haro, J.M.; Kassebaum, N.J.; Chrepa, V.; Kotsakis, G.A. Population prevalence of edentulism and its association with depression and self-rated health. Sci. Rep. 2016, 6, 37083. [Google Scholar] [PubMed]
- Allen, P.F.; McMillian, A. Food selections and perceptions of chewing ability following provision of implant and conventional prostheses to complete denture wearers. Clin. Oral Implant. Res. 2002, 12, 320–326. [Google Scholar]
- Feine, J.S.; Carlsson, G.E.; Awad, M.A.; Chehade, A.; Duncan, W.J.; Gizani, S.; Head, T.; Lund, J.P.; MacEntee, M.; Mericske-Stern, R.; et al. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Montreal, Quebec, May 24–25, 2002. Int. J. Oral Maxillofac. Implant. 2002, 17, 601–602. [Google Scholar]
- Engquist, B.; Bergendal, T.; Kallus, T.; Linden, U. A retrospective multicenter evaluation of osseointegrated implants supporting overdentures. Int. J. Oral Maxillofac. Implant. 1988, 3, 129–134. [Google Scholar]
- Rentsch Kollar, A.; Huber, S.; Mericske Stern, R. Mandibular implant overdentures followed for over 10 years: Patient compliance and prosthetic maintenance. Int. J. Prosthodont. 2010, 23, 91–98. [Google Scholar] [PubMed]
- Assaf, A.; Daas, M.; Boittin, A.; Eid, N.; Postaire, M. Prosthetic maintenance of different mandibular implant overdentures: A systematic review. J. Prosthet. Dent. 2017, 118, 144–152. [Google Scholar]
- Payne, A.G.; Alsabeeha, N.H.; Atieh, M.A.; Esposito, M.; Ma, S.; Anas El-Wegoud, M.A. Interventions for replacing missing teeth: Attachment systems for implant overdentures in edentulous jaws. Cochrane Database Syst. Rev. 2018, 10, CD008001. [Google Scholar]
- Payne, G.T.; Zarb, G. (Eds.) Prosthodontic Treatment for Edentulous Patients: Complete Dentures and Implant-Supported Prostheses; Elsevier: St Louis, MA, USA, 2013; p. 334. [Google Scholar]
- Naert, I.; Gizani, S.; Vuylsteke, M.; Van Steenberghe, D. A 5-year prospective randomized clinical trial on the influence of splinted and unsplinted oral implants retaining a mandibular overdenture: Prosthetic aspects and patient satisfaction. J. Oral Rehabil. 1999, 26, 195–202. [Google Scholar]
- Cune, M.; Burgers, M.; van Kampen, F.M.; de Putter, C.; Van der Bilt, A. Mandibular overdentures retained by two implants. 10 year results from a cross-over trial comparing ball- socket and clip-attachments. Int. J. Prosthodont. 2010, 23, 310–317. [Google Scholar]
- Cehreli, M.C.; Uysal, S.; Akca, K. Marginal Bone Level Changes and Prosthetic Maintenance of Mandibular Overdentures Supported by 2 Implants: A 5-Year Randomized Clinical Trial. Clin. Implant Dent. Relat. Res. 2010, 12, 114–121. [Google Scholar]
- Leão, R.S.; Moraes, S.L.D.; Vasconcelos, B.C.E.; Lemos, C.A.A.; Pellizzer, E.P. Splinted and unsplinted overdenture attachment systems: A systematic review and meta-analysis. J. Oral Rehabil. 2018, 45, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Cai, H.; Zhang, J.; Wang, J.; Sui, L. Effects of immediate and delayed loading protocols on marginal bone loss around implants in unsplinted mandibular implant-retained overdentures: A systematic review and meta-analysis. BMC Oral Health 2021, 21, 122. [Google Scholar] [CrossRef] [PubMed]
- Krennmair, G.; Seemann, R.; Fazekas, A.; Ewers, R.; Piehslinger, E. Patient preference and satisfaction with implant-supported mandibular overdentures retained with ball or locator attachments: A crossover clinical trial. Int. J. Oral Maxillofac. Implant. 2012, 27, 1560–1568. [Google Scholar]
- Mackie, A.; Lyons, K.; Thomson, W.M.; Payne, A.G.T. Mandibular two implant overdentures: Three years prosthodontic maintenance using the locator attachment system. Int. J. Prosthodont. 2011, 21, 328–331. [Google Scholar]
- Matthys, C.; Vervaeke, S.; Besseler, J.; Doornewaard, R.; Dierens, M.; De Bruyn, H. Five years follow-up of mandibular 2-implant overdentures on locator or ball abutments: Implant results, patient-related outcome, and prosthetic aftercare. Clin. Implant Dent. Relat. Res. 2019, 21, 835–844. [Google Scholar] [CrossRef]
- Cristache, C.M.; Muntianu, L.A.S.; Burlibasa, M.; Didilescu, A.C. Five-year clinical trial using three attachment systems for implant overdentures. Clin. Oral Implant. Res. 2014, 28, 171–178. [Google Scholar] [CrossRef]
- Brandt, S.; Lauer, H.-C.; Fehrenz, M.; Güth, J.-F.; Romanos, G.; Winter, A. Ball versus locator attachments: A retrospective study on prosthetic maintenance and effect on oral-health- related quality of life. Materials 2021, 14, 1051. [Google Scholar] [CrossRef]
- Di Spirito, F.; Toti, P.; Brevi, B.; Martuscelli, R.; Sbordone, L.; Sbordone, C. Computed tomography evaluation of jaw atrophies before and after surgical bone augmentation. Int. J. Clin. Dent. 2019, 12, 259–270. [Google Scholar]
- Cawood, J.I.; Howell, R.A. A classification of the edentulous jaws. Int. J. Oral Maxillofac. Surg. 1988, 17, 232–236. [Google Scholar]
- Loe, H.; Silness, J. Periodontal disease in pregnancy. I. Prevalence and severity. Acta Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef]
- Nagy, U.; Guédat, C.; Giannopoulou, C.; Schimmel, M.; Müller, F.; Srinivasan, M. Microbiological evaluation of Locator® legacy attachments: A cross-sectional clinical study. Clin. Exp. Dent. Res. 2019, 5, 476–484. [Google Scholar] [CrossRef] [PubMed]
- Sultana, N.; Bartlett, D.W.; Suleiman, M. Retention of implant supported overdentures at different implant angulations: Comparing locator and ball attachments. Clin. Oral Implant. Res. 2017, 28, 1406–1410. [Google Scholar] [CrossRef] [PubMed]
- Matthys, C.; Vervaeke, S.; Besseler, J.; De Bruyn, H. Five-year study of mandibular overdentures on Stud abutments: Clinical outcome, patient satisfaction and prosthetic maintenance—Influence of bone resorption and implant position. Clin. Oral Implant. Res. 2019, 30, 940–951. [Google Scholar] [CrossRef] [PubMed]
- Nissan, J.; Oz-Ari, B.; Gross, O.; Ghelfan, O.; Chaushu, G. Long-term prosthetic aftercare of direct vs. indirect attachment incorporation techniques to mandibular implant-supported overdenture. Clin. Oral Implant. Res. 2011, 22, 627–630. [Google Scholar] [CrossRef] [PubMed]
- Marinis, A.; Afshari, F.S.; Chia-Chun Yuan, J.; Lee, D.J.; Syros, G.; Knoernschild, K.L.; Campbell, S.D.; Sukotjo, C. Retrospective analysis of implant overdenture treatment in the advanced prosthodontic clinic at the university of illinois at chicago. J. Oral Implantol. 2016, 27, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Rosner, O.; Zenziper, E.; Heller, H.; Nissan, J.; Matalon, S.; Melamed, G.; Har-Ness, S.; Glickman, A. Long-Term Prosthetic Aftercare of Two-Vs. Four-Ball Attachment Implant-Supported Mandibular Overdentures. Appl. Sci. 2021, 11, 8974. [Google Scholar] [CrossRef]
- Sato, H.; Kobayashi, T.; Nomura, T.; Tanabe, N.; Tagafuji, K.; Kihara, H.; Kondo, H. Oral mucosa pressure caused by mandibular implant overdenture with different types of attachments. J. Prosthodont. Res. 2019, 30, 301–307. [Google Scholar] [CrossRef]
- Di Spirito, F.; Schiavo, L.; Pilone, V.; Lanza, A.; Sbordone, L.; D’Ambrosio, F. Periodontal and peri-implant diseases and systemically administered statins: A systematic review. Dent. J. 2021, 9, 100. [Google Scholar] [CrossRef]
- Di Spirito, F.; Sbordone, L.; Pilone, V.; D’Ambrosio, F. Obesity and periodontal disease: A narrative review on current evidence and putative molecular links. Open Dent. J. 2019, 13, 526–536. [Google Scholar] [CrossRef]
- Di Spirito, F.; Iacono, V.J.; Alfredo, I.; Alessandra, A.; Sbordone, L.; Lanza, A.T. Evidence-based recommendations on periodontal practice and the management of periodontal patients during and after the COVID-19 era: Challenging infectious diseases spread by airborne transmission. Open Dent. J. 2021, 15, 325–336. [Google Scholar] [CrossRef]
- Speranza, A.; Massafra, C.; Pecchia, S.; Di Niccolo, R.; Iorio, R.; Ferretti, A. Metallic versus Non-Metallic Cerclage Cables System in Periprosthetic Hip Fracture Treatment: Single-Institution Experience at a Minimum 1-Year Follow-Up. J. Clin. Med. 2022, 11, 1608. [Google Scholar] [CrossRef] [PubMed]
- Bülhoff, M.; Zeifang, F.; Welters, C.; Renkawitz, T.; Schiltenwolf, M.; Tross, A.-K. Medium- to Long-Term Outcomes after Reverse Total Shoulder Arthroplasty with a Standard Long Stem. J. Clin. Med. 2022, 11, 2274. [Google Scholar] [CrossRef] [PubMed]
- Solarino, G.; Carlet, A.; Moretti, L.; Miolla, M.P.; Ottaviani, G.; Moretti, B. Clinical Results in Posterior-Stabilized Total Knee Arthroplasty with Cementless Tibial Component in Porous Tantalum: Comparison between Monoblock and Two Pegs vs. Modular and Three Pegs. Prosthesis 2022, 4, 160–168. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zenziper, E.; Rosner, O.; Ghelfan, O.; Nissan, J.; Blumer, S.; Ben-Izhack, G.; Slutzky, H.; Meinster, I.; Chaushu, L.; Naishlos, S. Long-Term Prosthetic Aftercare of Mandibular Implant-Supported Overdenture. Appl. Sci. 2022, 12, 8673. https://doi.org/10.3390/app12178673
Zenziper E, Rosner O, Ghelfan O, Nissan J, Blumer S, Ben-Izhack G, Slutzky H, Meinster I, Chaushu L, Naishlos S. Long-Term Prosthetic Aftercare of Mandibular Implant-Supported Overdenture. Applied Sciences. 2022; 12(17):8673. https://doi.org/10.3390/app12178673
Chicago/Turabian StyleZenziper, Eran, Ofir Rosner, Oded Ghelfan, Joseph Nissan, Sigalit Blumer, Gil Ben-Izhack, Hagay Slutzky, Isabelle Meinster, Liat Chaushu, and Sarit Naishlos. 2022. "Long-Term Prosthetic Aftercare of Mandibular Implant-Supported Overdenture" Applied Sciences 12, no. 17: 8673. https://doi.org/10.3390/app12178673
APA StyleZenziper, E., Rosner, O., Ghelfan, O., Nissan, J., Blumer, S., Ben-Izhack, G., Slutzky, H., Meinster, I., Chaushu, L., & Naishlos, S. (2022). Long-Term Prosthetic Aftercare of Mandibular Implant-Supported Overdenture. Applied Sciences, 12(17), 8673. https://doi.org/10.3390/app12178673