
Skeletal Muscles of Patients Infected with SARS-CoV-2 Develop Severe Myofiber Damage upon One Week of Admission on the Intensive Care Unit

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Muscle Analyses
2.3. Statistics
3. Results
3.1. Patients’ Characteristics
3.2. Immunofluorescent Analysis
3.3. Muscle Fiber Type Composition and Size
3.4. Myonuclear Content
3.5. Muscle Fiber Capillarization
3.6. Histology
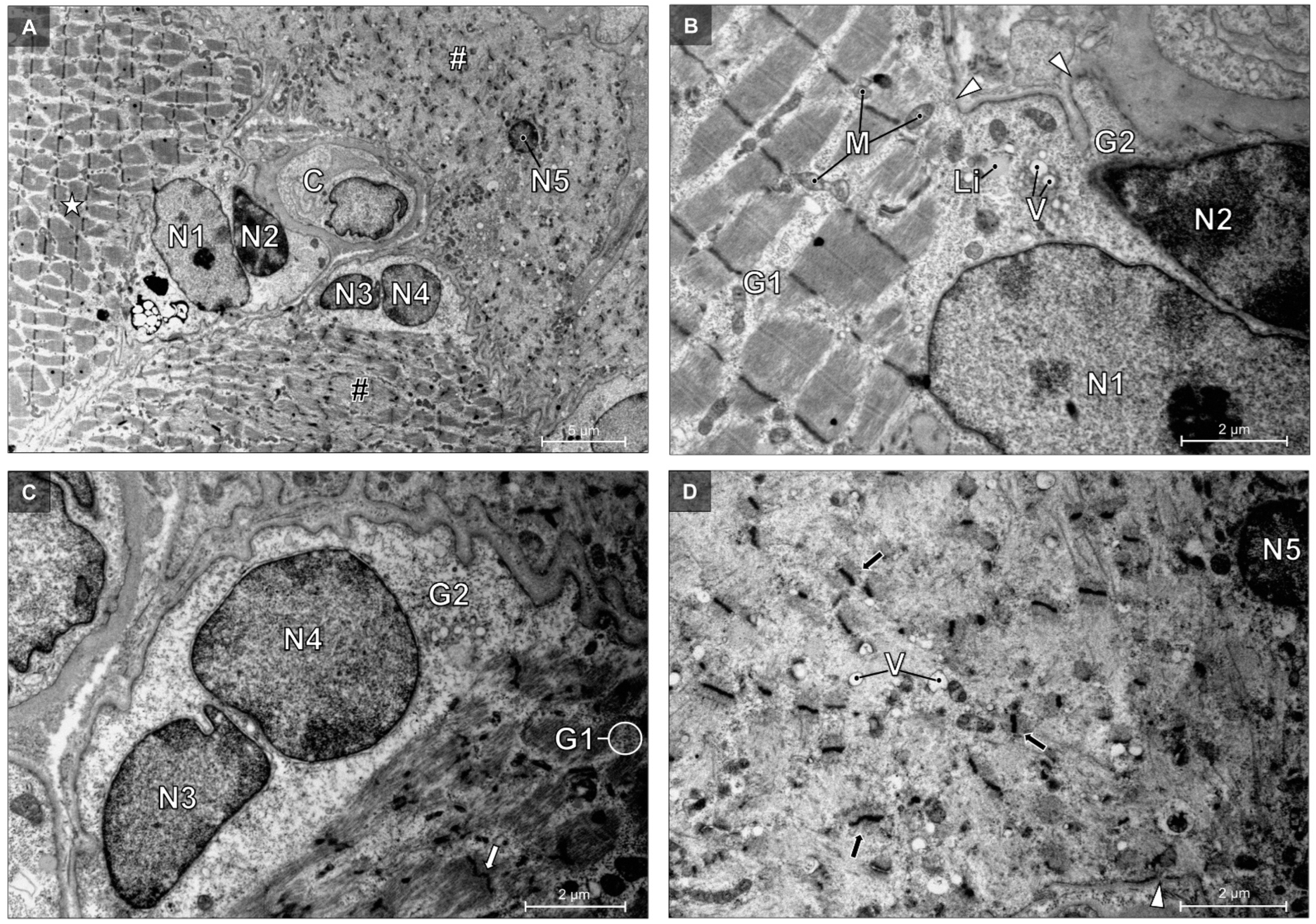
3.7. Transmission Electron Microscopy
4. Discussion
Perspectives, Significance, and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients with Comorbidities (n = 13) | Patients without Comorbidities (n = 4) | ||||
|---|---|---|---|---|---|
| Type | T0 | T1 | T0 | T1 | |
| Muscle fiber size (µm2) | I | 5176 ± 1235 | 5834 ± 2142 | 6048 ± 795 | 5221 ± 679 |
| II | 4212 ± 1301 | 4297 ± 1524 * | 4729 ± 963 | 3499 ± 1275 † | |
| Fiber type distribution (%) | I | 43 ± 14 | 46 ± 15 | 44 ± 11 | 51 ± 18 |
| II | 57 ± 14 | 54 ± 15 | 56 ± 11 | 49 ± 18 | |
| Myonuclear content (number/fiber) | I | 4.50 ± 0.95 | 5.12 ± 1.44 | 4.07 ± 0.86 | 4.45 ± 0.93 |
| II | 4.25 ± 0.94 | 4.59 ± 1.45 | 3.76 ± 0.57 | 3.66 ± 0.23 | |
| Myonuclear domain (µm2) | I | 1165 ± 232 | 1132 ± 238 | 1514 ± 184 | 1193 ± 160 |
| II | 987 ± 161 | 941 ± 179 * | 1257 ±152 | 961 ± 356 | |
| Proportion of fibers containing central nuclei (%) | I | 5.0 ± 3.0 | 6.0 ± 4.2 | 10.5 ± 8.0 | 5.4 ± 5.9 |
| II | 6.3 ± 5.1 | 3.6 ± 3.4 † | 5.0 ± 3.6 | 3.7 ± 2.4 | |
| CC | I | 3.30 ± 0.50 | 3.42 ± 0.61 | 3.34 ± 0.70 | 2.80 ± 0.71 |
| II | 2.80 ± 0.30 | 2.88 ± 0.64 * | 3.02 ± 0.70 | 1.94 ± 0.47 | |
| C/Fi | I | 1.14 ± 0.26 | 1.13 ± 0.42 | 1.20 ± 0.42 | 1.28 ± 0.51 |
| II | 0.84 ± 0.25 | 0.76 ± 0.27 * | 0.84 ± 0.44 | 0.75 ± 0.29 * | |
| CFPE index (capillaries·1000 µm−1) | I | 5.35 ± 0.92 | 5.09 ± 0.77 | 4.77 ± 0.84 | 4.44 ± 0.76 |
| II | 4.26 ± 0.64 | 3.92 ± 0.76 * | 3.76 ± 1.17 | 3.13 ± 0.81 * | |
| CD (capillaries per mm2) | I | 355 ± 100 | 315 ± 106 | 276 ± 59 | 273 ± 281 |
| II | 342 ± 102 | 327 ± 123 | 288 ± 118 | 280 ± 81 | |
References
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Busetto, G.M.; Porreca, A.; Del Giudice, F.; Maggi, M.; D’Agostino, D.; Romagnoli, D.; Musi, G.; Lucarelli, G.; Palmer, K.; Colonna di Paliano, A.; et al. SARS-CoV-2 Infection and High-Risk Non-Muscle-Invasive Bladder Cancer: Are There Any Common Features? Urol. Int. 2020, 104, 510–522. [Google Scholar] [CrossRef]
- Zhang, H.; Zhou, J.; Chen, R.; Ren, Y.; Cai, J.; Zhao, L.; Fei, X.; Liu, Z.; Zhang, Y.; Yuan, L.; et al. Autopsy and Histologic Findings of Patients with New Coronavirus Pneumonia: The Pathologic Associations with Hypoxemia. Med. Sci. Monit. 2021, 27, e928837. [Google Scholar] [CrossRef] [PubMed]
- Baj, J.; Karakuła-Juchnowicz, H.; Teresiński, G.; Buszewicz, G.; Ciesielka, M.; Sitarz, E.; Forma, A.; Karakuła, K.; Flieger, W.; Portincasa, P.; et al. COVID-19: Specific and Non-Specific Clinical Manifestations and Symptoms: The Current State of Knowledge. J. Clin. Med. 2020, 9, 1753. [Google Scholar] [CrossRef] [PubMed]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Kunugi, H. Skeletal Muscle Damage in COVID-19: A Call for Action. Medicina 2021, 57, 372. [Google Scholar] [CrossRef] [PubMed]
- Scaturro, D.; Vitagliani, F.; Di Bella, V.E.; Falco, V.; Tomasello, S.; Lauricella, L.; Letizia Mauro, G. The Role of Acetyl-Carnitine and Rehabilitation in the Management of Patients with Post-COVID Syndrome: Case-Control Study. Appl. Sci. 2022, 12, 4084. [Google Scholar] [CrossRef]
- De Carvalho, M. Intensive Care Unit-Acquired Weakness: Introductory Notes. J. Clin. Neurophysiol. 2020, 37, 195–196. [Google Scholar] [CrossRef]
- Wang, P.Y.; Li, Y.; Wang, Q. Sarcopenia: An underlying treatment target during the COVID-19 pandemic. Nutrition 2021, 84, 111104. [Google Scholar] [CrossRef]
- Motta-Santos, D.; Dos Santos, R.A.; Oliveira, M.; Qadri, F.; Poglitsch, M.; Mosienko, V.; Kappes Becker, L.; Campagnole-Santos, M.J.; Penninger, J.M.; Alenina, N.; et al. Effects of ACE2 deficiency on physical performance and physiological adaptations of cardiac and skeletal muscle to exercise. Hypertens. Res. 2016, 39, 506–512. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e278. [Google Scholar] [CrossRef]
- Riquelme, C.; Acuña, M.J.; Torrejón, J.; Rebolledo, D.; Cabrera, D.; Santos, R.A.; Brandan, E. ACE2 is augmented in dystrophic skeletal muscle and plays a role in decreasing associated fibrosis. PLoS ONE 2014, 9, e93449. [Google Scholar] [CrossRef] [PubMed]
- Disser, N.P.; De Micheli, A.J.; Schonk, M.M.; Konnaris, M.A.; Piacentini, A.N.; Edon, D.L.; Toresdahl, B.G.; Rodeo, S.A.; Casey, E.K.; Mendias, C.L. Musculoskeletal Consequences of COVID-19. J. Bone Jt. Surg. Am. 2020, 102, 1197–1204. [Google Scholar] [CrossRef]
- Ferrandi, P.J.; Alway, S.E.; Mohamed, J.S. The interaction between SARS-CoV-2 and ACE2 may have consequences for skeletal muscle viral susceptibility and myopathies. J. Appl. Physiol. 2020, 129, 864–867. [Google Scholar] [CrossRef] [PubMed]
- Aschman, T.; Schneider, J.; Greuel, S.; Meinhardt, J.; Streit, S.; Goebel, H.H.; Büttnerova, I.; Elezkurtaj, S.; Scheibe, F.; Radke, J.; et al. Association Between SARS-CoV-2 Infection and Immune-Mediated Myopathy in Patients Who Have Died. JAMA Neurol. 2021, 78, 948–960. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Agten, A.; Verbrugghe, J.; Stevens, S.; Boomgaert, L.; Eijnde, O.B.; Timmermans, A.; Vandenabeele, F. Feasibility, accuracy and safety of a percutaneous fine-needle biopsy technique to obtain qualitative muscle samples of the lumbar multifidus and erector spinae muscle in persons with low back pain. J. Anat. 2018, 233, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Betz, M.W.; Aussieker, T.; Kruger, C.Q.; Gorissen, S.H.M.; van Loon, L.J.C.; Snijders, T. Muscle fiber capillarization is associated with various indices of skeletal muscle mass in healthy, older men. Exp. Gerontol. 2021, 143, 111161. [Google Scholar] [CrossRef]
- Kosek, D.J.; Kim, J.S.; Petrella, J.K.; Cross, J.M.; Bamman, M.M. Efficacy of 3 days/wk resistance training on myofiber hypertrophy and myogenic mechanisms in young vs. older adults. J. Appl. Physiol. 2006, 101, 531–544. [Google Scholar] [CrossRef]
- Hepple, R.T. A new measurement of tissue capillarity: The capillary-to-fibre perimeter exchange index. Can. J. Appl. Physiol. 1997, 22, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, O.; Reid, M.B.; Van den Berghe, G.; Vanhorebeek, I.; Hermans, G.; Rich, M.M.; Larsson, L. The Sick and the Weak: Neuropathies/Myopathies in the Critically Ill. Physiol. Rev. 2015, 95, 1025–1109. [Google Scholar] [CrossRef]
- Stanley, M.; Chippa, V.; Aeddula, N.R.; Quintanilla Rodriguez, B.S.; Adigun, R. Rhabdomyolysis; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Heffner, R.R., Jr. Electron microscopy of disorders of skeletal muscle. Ann. Clin. Lab. Sci. 1975, 5, 338–347. [Google Scholar]
- Lauritzen, F.; Paulsen, G.; Raastad, T.; Bergersen, L.H.; Owe, S.G. Gross ultrastructural changes and necrotic fiber segments in elbow flexor muscles after maximal voluntary eccentric action in humans. J. Appl. Physiol. 2009, 107, 1923–1934. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Lee, J.E.; Choi, G.S.; Koo, H.; Han, S.J.; Yoo, J.H.; Choi, Y.C.; Park, K.D. Electron Microscopy Pathology of ADSSL1 Myopathy. J. Clin. Neurol. 2017, 13, 105–106. [Google Scholar] [CrossRef]
- Ghadially, F.N. Ultrastructural Pathology of the Cell. A text and Atlas of Physiological and Pathological Alterations in Cell Fine Structure. Med. J. Aust. 1976, 2, 28. [Google Scholar]
- Fernandez, C.; Figarella-Branger, D.; Meyronet, D.; Cassote, E.; Tong, S.; Pellissier, J.F. Electron microscopy in neuromuscular disorders. Ultrastruct. Pathol. 2005, 29, 437–450. [Google Scholar] [CrossRef]
- Selcen, D.; Ohno, K.; Engel, A.G. Myofibrillar myopathy: Clinical, morphological and genetic studies in 63 patients. Brain 2004, 127, 439–451. [Google Scholar] [CrossRef] [PubMed]
- Helliwell, T.R.; Wilkinson, A.; Griffiths, R.D.; McClelland, P.; Palmer, T.E.; Bone, J.M. Muscle fibre atrophy in critically ill patients is associated with the loss of myosin filaments and the presence of lysosomal enzymes and ubiquitin. Neuropathol. Appl. Neurobiol. 1998, 24, 507–517. [Google Scholar] [CrossRef]
- Stibler, H.; Edström, L.; Ahlbeck, K.; Remahl, S.; Ansved, T. Electrophoretic determination of the myosin/actin ratio in the diagnosis of critical illness myopathy. Intensive Care Med. 2003, 29, 1515–1527. [Google Scholar] [CrossRef]
- Wollersheim, T.; Woehlecke, J.; Krebs, M.; Hamati, J.; Lodka, D.; Luther-Schroeder, A.; Langhans, C.; Haas, K.; Radtke, T.; Kleber, C.; et al. Dynamics of myosin degradation in intensive care unit-acquired weakness during severe critical illness. Intensive Care Med. 2014, 40, 528–538. [Google Scholar] [CrossRef]
- Miller, M.A.; Zachary, J.F. Mechanisms and Morphology of Cellular Injury, Adaptation, and Death. Pathol. Basis Vet. Dis. 2017, 2, 43.e19. [Google Scholar]
- Hooper, J.E.; Uner, M.; Priemer, D.S.; Rosenberg, A.; Chen, L. Muscle Biopsy Findings in a Case of SARS-CoV-2-Associated Muscle Injury. J. Neuropathol. Exp. Neurol. 2021, 80, 377–378. [Google Scholar] [CrossRef]
- Mageriu, V.; Zurac, S.; Bastian, A.; Staniceanu, F.; Manole, E. Histological findings in skeletal muscle of SARS-CoV2 infected patient. J Immunoass. Immunochem. 2020, 41, 1000–1009. [Google Scholar] [CrossRef] [PubMed]
- Perico, L.; Benigni, A.; Casiraghi, F.; Ng, L.F.P.; Renia, L.; Remuzzi, G. Immunity, endothelial injury and complement-induced coagulopathy in COVID-19. Nat. Rev. Nephrol. 2021, 17, 46–64. [Google Scholar] [CrossRef]
- Amraei, R.; Rahimi, N. COVID-19, Renin-Angiotensin System and Endothelial Dysfunction. Cells 2020, 9, 1652. [Google Scholar] [CrossRef]
- Hauptmann, S.; Klosterhalfen, B.; Weis, J.; Mittermayer, C.; Kirkpatrick, C.J. Skeletal muscle oedema and muscle fibre necrosis during septic shock. Observations with a porcine septic shock model. Virchows Arch. 1994, 424, 653–659. [Google Scholar] [CrossRef] [PubMed]
- Prescott, H.C.; Girard, T.D. Recovery From Severe COVID-19: Leveraging the Lessons of Survival From Sepsis. JAMA 2020, 324, 739–740. [Google Scholar] [CrossRef]
- Ma, Y.; Deng, J.; Liu, Q.; Du, M.; Liu, M.; Liu, J. Long-Term Consequences of COVID-19 at 6 Months and Above: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6865. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute covid-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef] [PubMed]







| Demographics and Anthropometrics | Disease Severity | Blood Analysis | Comorbidities | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (Years) | BMI (kg/m2) | Sex (M:F) | Acute Physiology and Chronic Health Evaluation II | Sequential Organ Failure Assessment Score | Acute Respiratory Distress Syndrome (Yes/No) | Sepsis (Yes/No) | Mode of Ventilation | Extra Corporal Membrane Oxygenation (Yes/No) | Died during the Study (†) | Died on ICU (†) after T1 (End of Study) | Acute Respiratory Failure (PO2/FiO2 <300) | Acute Kidney Failure (Yes/No) | Acute Heart Failure (Yes/No) | White Blood Cells (×109/L) | C-Reactive Protein (mg/L) | Lactate Dehydrogenase (U/L) | Troponin (ng/L) | |
| 84 | 24.2 | M | 17 | 9 | Yes | Yes | HFNO, NIV | No | † | 113 | Yes | No | 3.1 | 40 | 530 | 39 | CVD, DM | |
| 83 * | 29.3 | F | 8 | 8 | Yes | Yes | NIV | No | † | 107 | No | No | 13.2 | 18 | 710 | 16.3 | CVD, HTN | |
| 81 | 26.0 | M | 7 | 15 | Yes | Yes | NIV, IMV | No | † | 75 | Yes | No | 8.0 | 96 | 640 | 26.5 | DM | |
| 73 | 26.0 | M | 10 | 6 | Yes | No | NIV | No | 110 | No | No | 9.0 | 260 | 430 | 17.9 | Cancer, CVA | ||
| 80 | 26.1 | M | 16 | 11 | No | Yes | NIV, IMV | No | † | 373 | No | No | 8.2 | 100 | 320 | 141 | CVD, CRD | |
| 73 * | 25.4 | M | 15 | N/A | Yes | No | HFNO | No | † | 77 | No | No | 4.7 | 50 | 460 | 20.6 | CRD | |
| 77 * | 22.6 | M | 12 | 8 | Yes | Yes | HFNO, NIV | No | 178 | No | No | 34.7 | 19 | 450 | 294 | HTN | ||
| 76 | 29.7 | M | 11 | 7 | No | No | HFNO | No | † | 224 | No | No | 6.2 | 31 | 240 | 164 | CVD, DM, CKD | |
| 75 | 26.3 | M | 20 | 12 | Yes | Yes | IMV | No | † | 114 | No | No | 12.4 | 43 | 370 | 115 | CRD | |
| 40 * | 24.3 | M | 11 | 11 | Yes | No | HFNO, NIV | No | † | 152 | No | No | 11.7 | 53 | 460 | <5 | DM, CLD | |
| 74 | 27.5 | F | 9 | 8 | Yes | Yes | HFNO, NIV, IMV | No | 70 | No | No | 6.1 | 100 | 370 | 12.2 | |||
| 82 | 24.3 | M | 10 | 8 | Yes | Yes | HFNO, IMV | No | † | 98 | No | No | 4.4 | 91 | 380 | 19.3 | ||
| 49 | 35.1 | M | 3 | 12 | Yes | Yes | HFNO, NIV, IMV | Yes | † | 111 | No | Yes | 9.7 | 42 | 370 | 8.3 | HTN, Obesity | |
| 54 | 45.5 | F | 5 | N/A | Yes | No | HFNO, NIV | No | 80 | No | No | 6.4 | 51 | 320 | 9 | DM, CRD, CVA Obesity | ||
| 68 | 31.4 | M | 9 | 14 | Yes | Yes | NIV, IMV | No | † | 78 | Yes | No | 6.1 | 140 | 430 | 33 | HTN, Obesity | |
| 68 | 29.3 | M | 13 | 10 | Yes | Yes | HFNO, NIV | No | 57 | No | No | 4.8 | 130 | 570 | 13.5 | DM | ||
| 69 | 23.0 | M | 9 | 11 | Yes | Yes | HFNO | No | † | 80 | No | No | 4.3 | 140 | 340 | 10.6 | Cancer | |
| 70 | 33.2 | F | 11 | N/A | Yes | Yes | HFNO | No | † | 142 | No | No | 7.6 | 94 | 410 | 20.6 | DM, Obesity | |
| 72 | 22.5 | M | 16 | 9 | Yes | No | HFNO, NIV | No | † | 88 | No | No | 3.1 | 120 | 670 | 16.1 | ||
| 70 | 27.7 | M | 9 | 8 | Yes | Yes | HFNO | No | 140 | No | No | 7.2 | 220 | 430 | 22.3 | HTN, DM | ||
| 33 * | 33.8 | M | 6 | 3 | Yes | No | HFNO | No | 136 | No | No | 6.8 | 27 | 820 | N/A | Obesity | ||
| 69 | 27.8 | M | 12 | 10 | Yes | Yes | HFNO, NIV, IMV | No | † | 53 | No | No | 6.6 | 50 | N/A | N/A | ||
| Fiber Type | T0 (n = 17) | T1 (n = 17) | |
|---|---|---|---|
| Fiber type distribution (%) | I | 43 ± 13 | 47 ± 13 |
| II | 57 ± 15 | 53 ± 15 | |
| Myonuclear content (number/fiber) | I | 4.40 ± 0.92 | 4.97 ± 1.35 |
| II | 4.14 ± 0.88 * | 4.37 ± 1.32 * | |
| Proportion of fibers containing a central nuclei (%) | I | 6.4 ± 4.9 | 5.8 ± 4.5 † |
| II | 6.0 ± 4.7 | 3.6 ± 3.1 † | |
| CC | I | 3.31 ± 0.53 | 3.26 ± 0.67 |
| II | 2.85 ± 0.41 * | 2.65 ± 0.72 * | |
| C/Fi | I | 1.15 ± 0.29 | 1.16 ± 0.43 |
| II | 0.84 ± 0.29 * | 0.76 ± 0.26 * | |
| CFPE index (capillaries·1000 µm−1) | I | 5.21 ± 0.91 | 4.93 ± 0.79 |
| II | 4.13 ± 0.79 * | 3.73 ± 0.83 * | |
| CD (Capillaries per mm2) | I | 335 ± 97 | 305 ± 94 |
| II | 328 ± 105 | 315 ± 114 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stevens, S.; Hendrickx, P.; Snijders, T.; Lambrichts, I.; Stessel, B.; Dubois, J.; van Loon, L.J.C.; Vandenabeele, F.; Agten, A. Skeletal Muscles of Patients Infected with SARS-CoV-2 Develop Severe Myofiber Damage upon One Week of Admission on the Intensive Care Unit. Appl. Sci. 2022, 12, 7310. https://doi.org/10.3390/app12147310
Stevens S, Hendrickx P, Snijders T, Lambrichts I, Stessel B, Dubois J, van Loon LJC, Vandenabeele F, Agten A. Skeletal Muscles of Patients Infected with SARS-CoV-2 Develop Severe Myofiber Damage upon One Week of Admission on the Intensive Care Unit. Applied Sciences. 2022; 12(14):7310. https://doi.org/10.3390/app12147310
Chicago/Turabian StyleStevens, Sjoerd, Paul Hendrickx, Tim Snijders, Ivo Lambrichts, Björn Stessel, Jasperina Dubois, Luc J. C. van Loon, Frank Vandenabeele, and Anouk Agten. 2022. "Skeletal Muscles of Patients Infected with SARS-CoV-2 Develop Severe Myofiber Damage upon One Week of Admission on the Intensive Care Unit" Applied Sciences 12, no. 14: 7310. https://doi.org/10.3390/app12147310
APA StyleStevens, S., Hendrickx, P., Snijders, T., Lambrichts, I., Stessel, B., Dubois, J., van Loon, L. J. C., Vandenabeele, F., & Agten, A. (2022). Skeletal Muscles of Patients Infected with SARS-CoV-2 Develop Severe Myofiber Damage upon One Week of Admission on the Intensive Care Unit. Applied Sciences, 12(14), 7310. https://doi.org/10.3390/app12147310