
In Vivo Evaluation of a Novel Radiofrequency Ablation Electrode in Pig Livers


Abstract
:1. Introduction
2. Materials and Methods
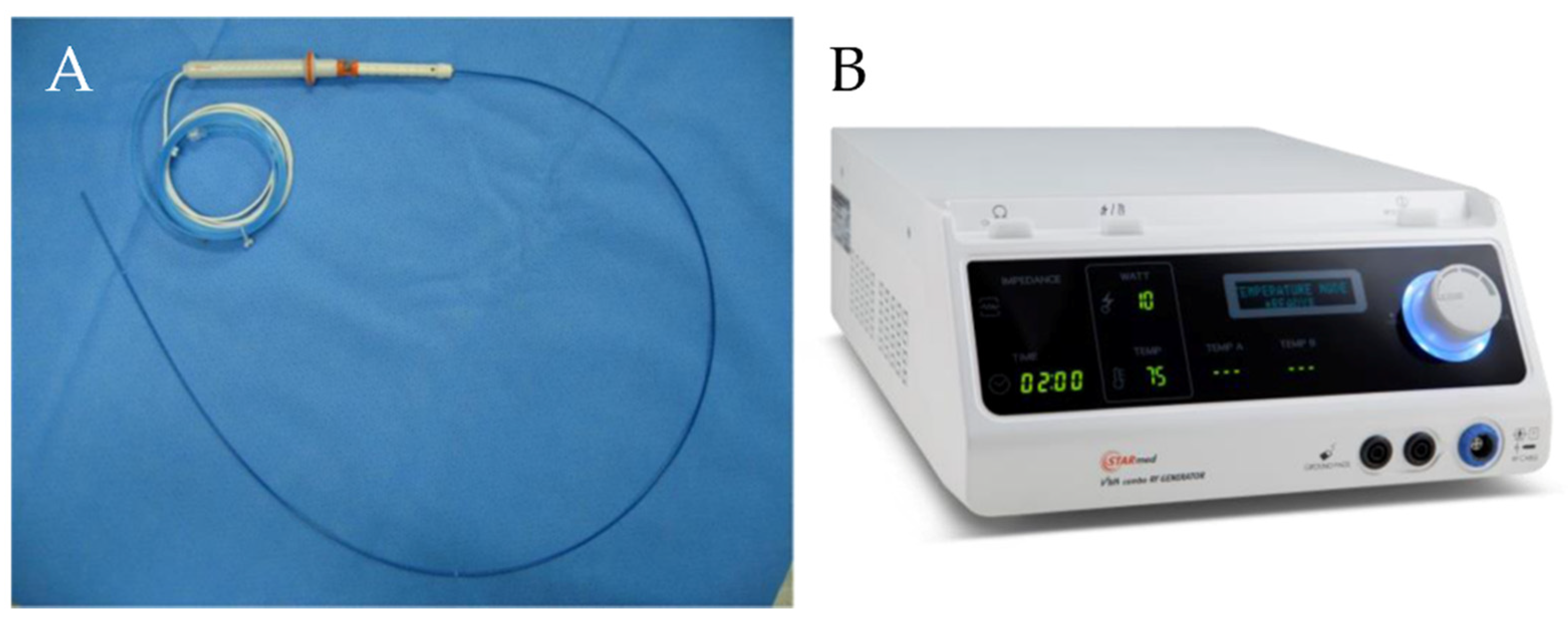
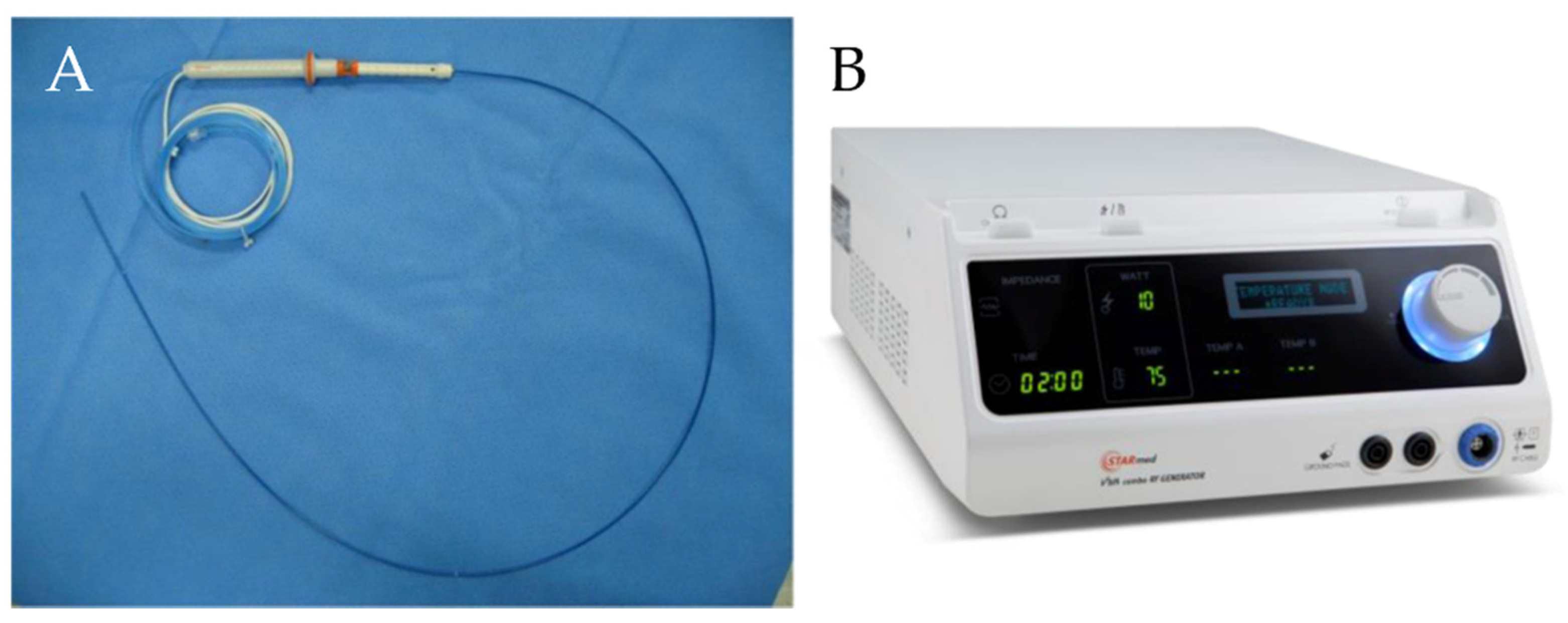
2.1. RFA Device
2.2. In Vivo Testing
2.3. Statistical Analysis
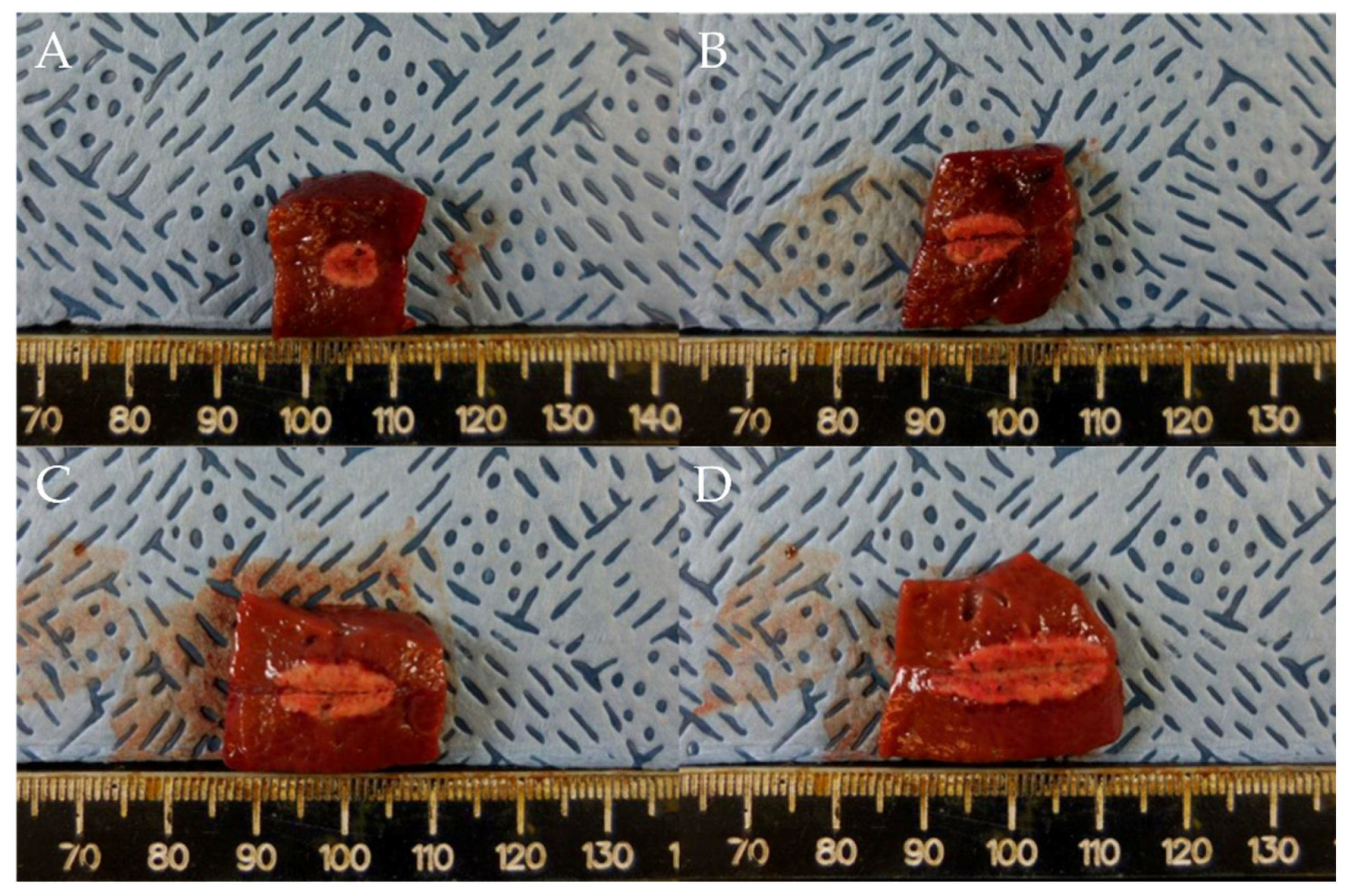
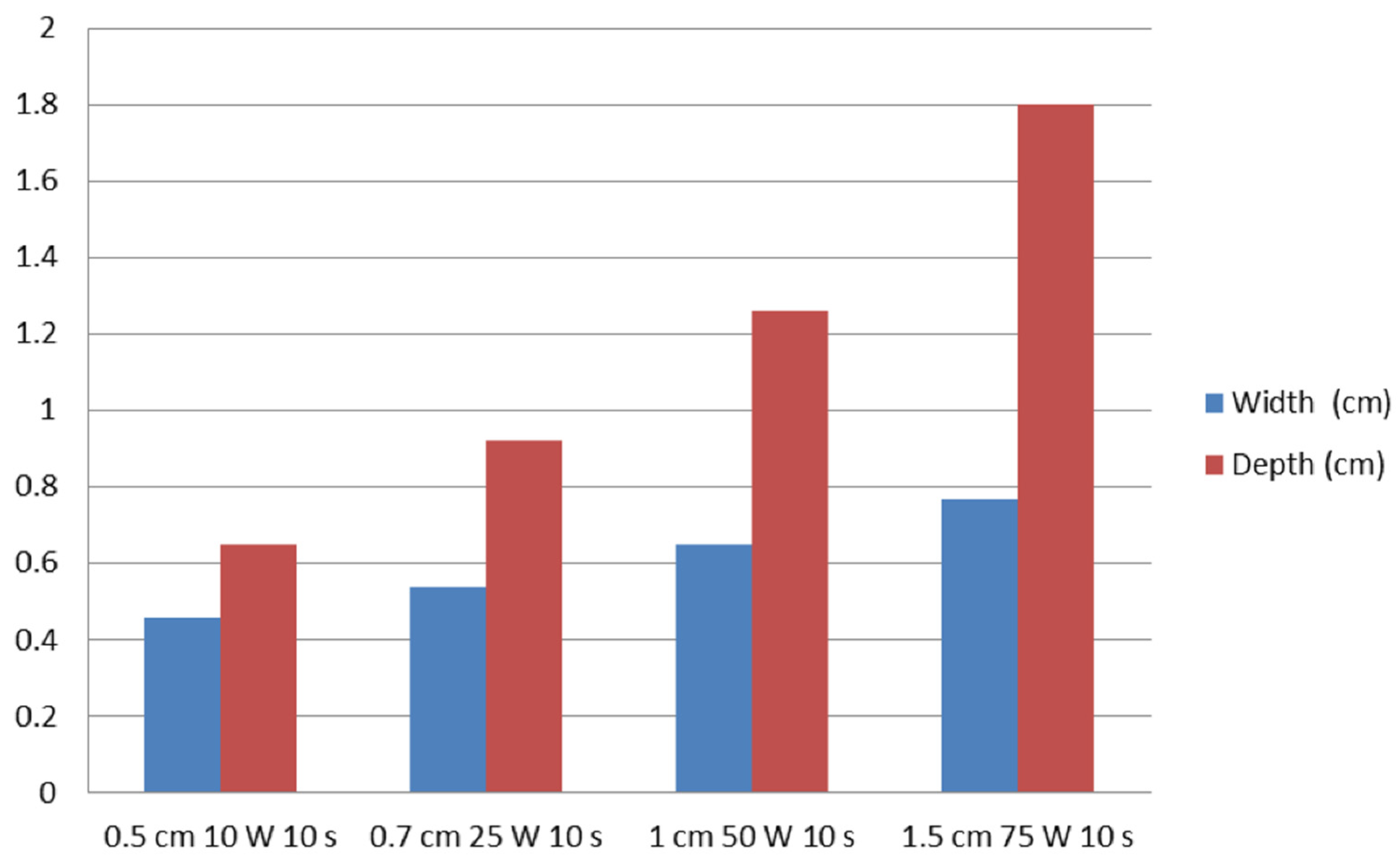
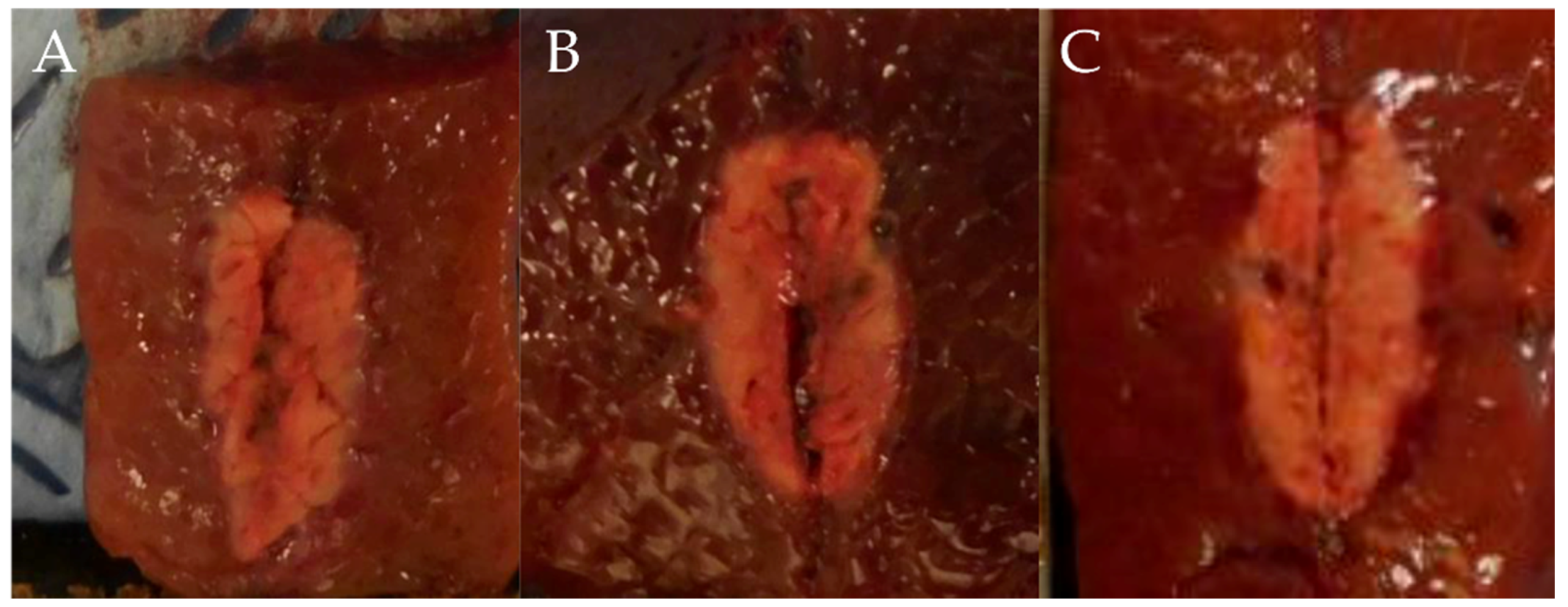
3. Results
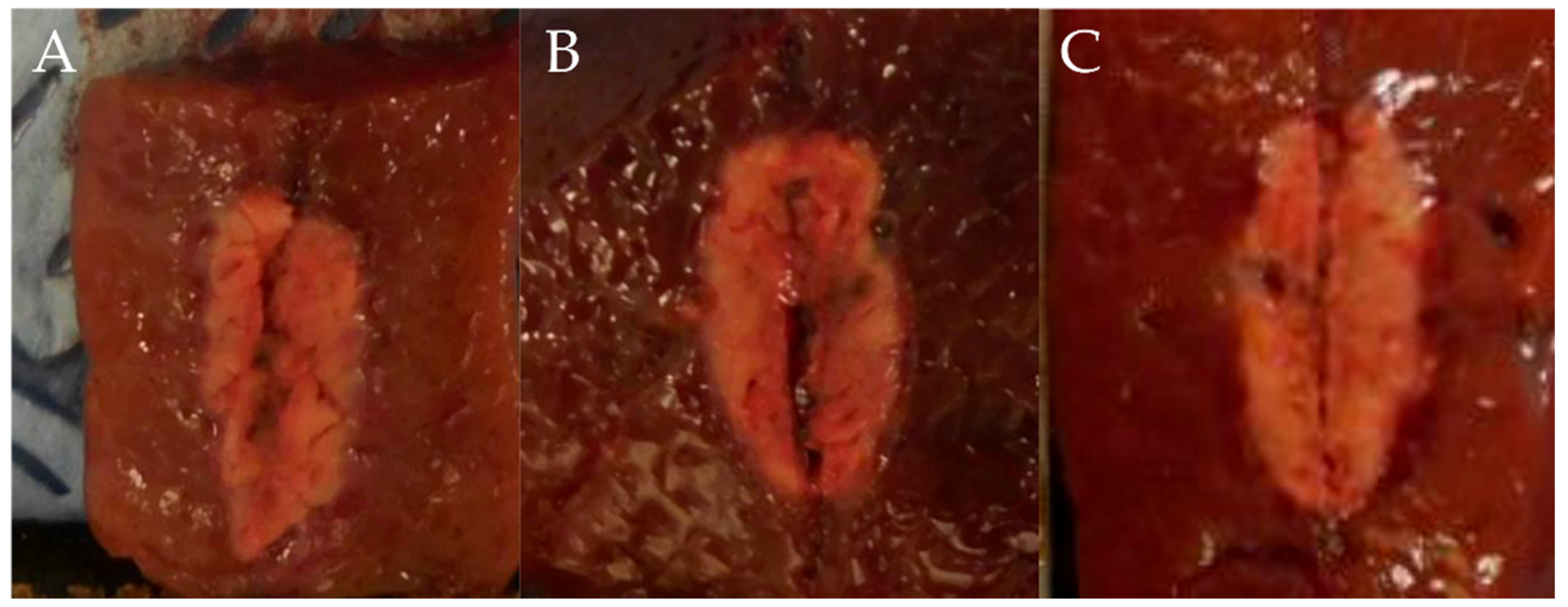
Outcomes of RFA
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Song, T.J.; Seo, D.W.; Lakhtakia, S.; Reddy, N.; Oh, D.W.; Park, D.H.; Lee, S.S.; Lee, S.K.; Kim, M.H. Initial experience of EUS-guided radiofrequency ablation of unresectable pancreatic cancer. Gastrointest. Endosc. 2016, 83, 440–443. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.H.; Yang, W.; Yan, K.; Gao, W.; Dai, Y.; Wang, Y.B.; Zhang, X.P.; Yin, S.S. Treatment efficacy of radiofrequency ablation of 338 patients with hepatic malignant tumor and the relevant complications. World J. Gastroenterol. 2005, 11, 6395–6401. [Google Scholar] [CrossRef]
- Choi, J.H.; Seo, D.W.; Song, T.J.; Park, D.H.; Lee, S.S.; Lee, S.K.; Kim, M.H. Endoscopic ultrasound-guided radiofrequency ablation for management of benign solid pancreatic tumors. Endoscopy 2018, 50, 1099–1104. [Google Scholar] [CrossRef]
- Oh, D.; Ko, S.W.; Seo, D.W.; Hong, S.M.; Kim, J.H.; Song, T.J.; Park, D.H.; Lee, S.K.; Kim, M.H. Endoscopic ultrasound-guided radiofrequency ablation of pancreatic microcystic serous cystic neoplasms: A retrospective study. Endoscopy 2021, 53, 739–743. [Google Scholar] [CrossRef]
- De Nucci, G.; Della Corte, C.; Reati, R.; Imperatore, N.; Arena, I.; Larghi, A.; Manes, G. Endoscopic ultrasound-guided radiofrequency ablation for hepatocellular carcinoma in cirrhosis: A case report test for efficacy and future perspectives. Endosc. Int. Open 2020, 8, E1713–E1716. [Google Scholar] [CrossRef] [PubMed]
- Attili, F.; Boškoski, I.; Bove, V.; Familiari, P.; Costamagna, G. EUS-guided radiofrequency ablation of a hepatocellular carcinoma of the liver. VideoGIE 2018, 3, 149–150. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.; Viera, F.T.; Ghittoni, G.; Cobianchi, L.; Rosa, L.L.; Siciliani, L.; Bortolotto, C.; Veronese, L.; Vercelli, A.; Gallotti, A.; et al. Radiofrequency ablation of pancreatic neuroendocrine tumors: A pilot study of feasibility, efficacy, and safety. Pancreas 2014, 43, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Crino, S.F.; D’Onofrio, M.; Bernardoni, L.; Frulloni, L.; Iannelli, M.; Malleo, G.; Paiella, S.; Larghi, A.; Gabbrielli, A. EUS-guided radiofrequency ablation (EUS-RFA) of solid pancreatic neoplasm using an 18-gauge needle electrode: Feasibility, safety, and technical success. J. Gastrointestin. Liver Dis. 2018, 27, 67–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakhtakia, S.; Ramchandani, M.; Galasso, D.; Gupta, R.; Venugopal, S.; Kalpala, R.; Reddy, D.N. EUS-guided radiofrequency ablation for management of pancreatic insulinoma by using a novel needle electrode (with videos). Gastrointest. Endosc. 2016, 83, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Scopelliti, F.; Pea, A.; Conigliaro, R.; Butturini, G.; Frigerio, I.; Regi, P.; Giardino, A.; Bertani, H.; Paini, M.; Pederzoli, P.; et al. Technique, safety, and feasibility of EUS-guided radiofrequency ablation in unresectable pancreatic cancer. Surg. Endosc. 2018, 32, 4022–4028. [Google Scholar] [CrossRef] [PubMed]
- Oh, D.; Seo, D.W.; Song, T.J.; Park, D.H.; Lee, S.K.; Kim, M.H. Clinical outcomes of EUS-guided radiofrequency ablation for unresectable pancreatic cancer: A prospective observational study. Endosc. Ultrasound 2022, 11, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Berzigotti, A.; Seijo, S.; Reverter, E.; Bosch, J. Assessing portal hypertension in liver diseases. Expert Rev. Gastroenterol. Hepatol. 2013, 7, 141–155. [Google Scholar] [CrossRef] [PubMed]
- Chiou, Y.Y.; Chou, Y.H. Radiofrequency ablation of hepatocellular carcinoma. J. Med. Ultrasound 2008, 16, 272–284. [Google Scholar] [CrossRef] [Green Version]
- Lencioni, R.; Crocetti, L.; Cioni, D.; Della Pina, C.; Bartolozzi, C. Percutaneous radiofrequency ablation of hepatic colorectal metastases: Technique, indications, results, and new promises. Investig. Radiol. 2004, 39, 689–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
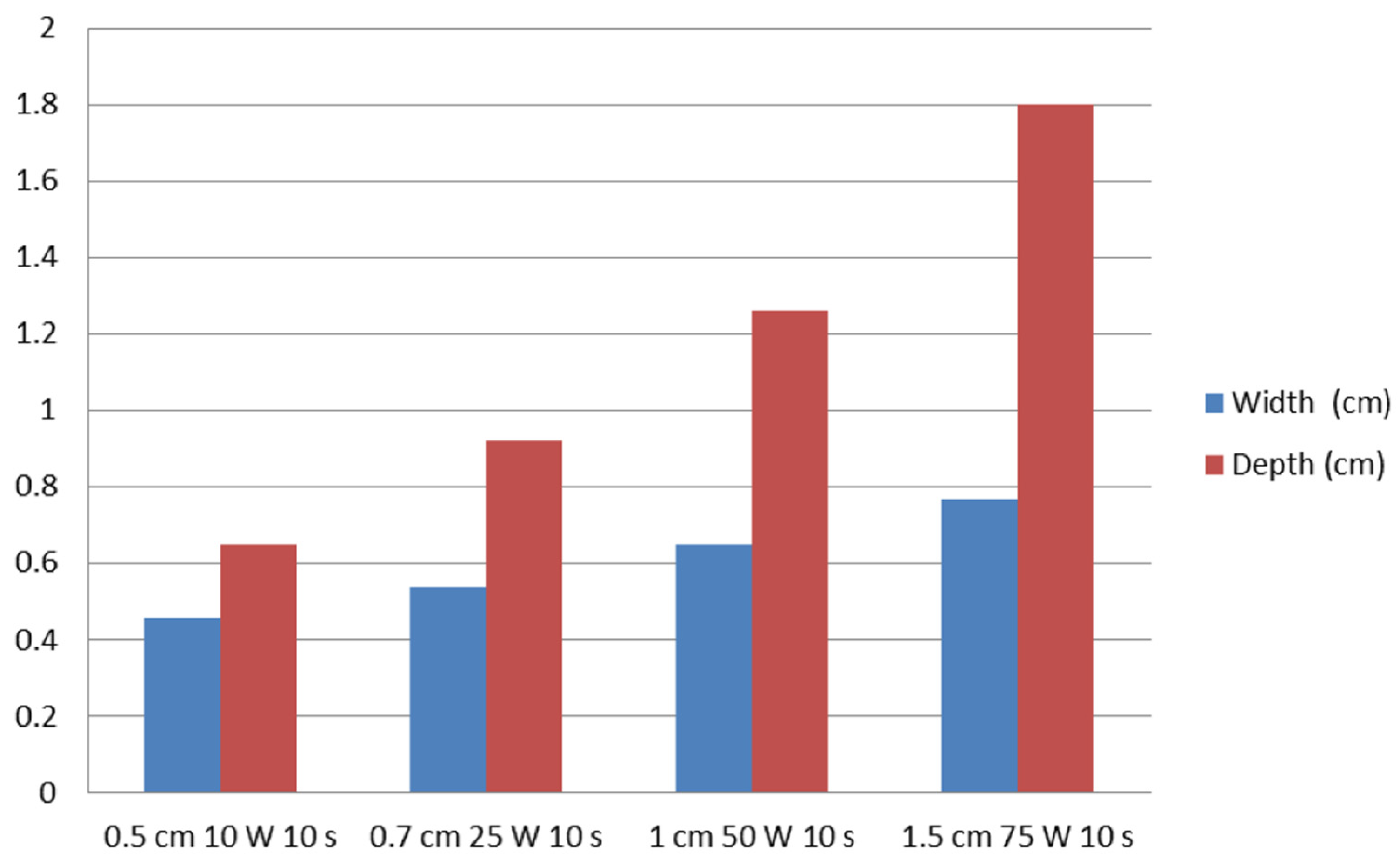
| Group A (0.5 cm, 10 W) | Group B (0.7 cm, 25 W) | Group C (1 cm, 50 W) | Group D (1.5 cm, 75 W) | |
|---|---|---|---|---|
| Ablation width, mean (SD), cm | 0.46 ± 0.07 | 0.54 ± 0.05 | 0.65 ± 0.05 | 0.77 ± 0.02 |
| Ablation depth, mean (SD), cm | 0.65 ± 0.07 | 0.92 ± 0.08 | 1.26 ± 0.14 | 1.80 ± 0.11 |
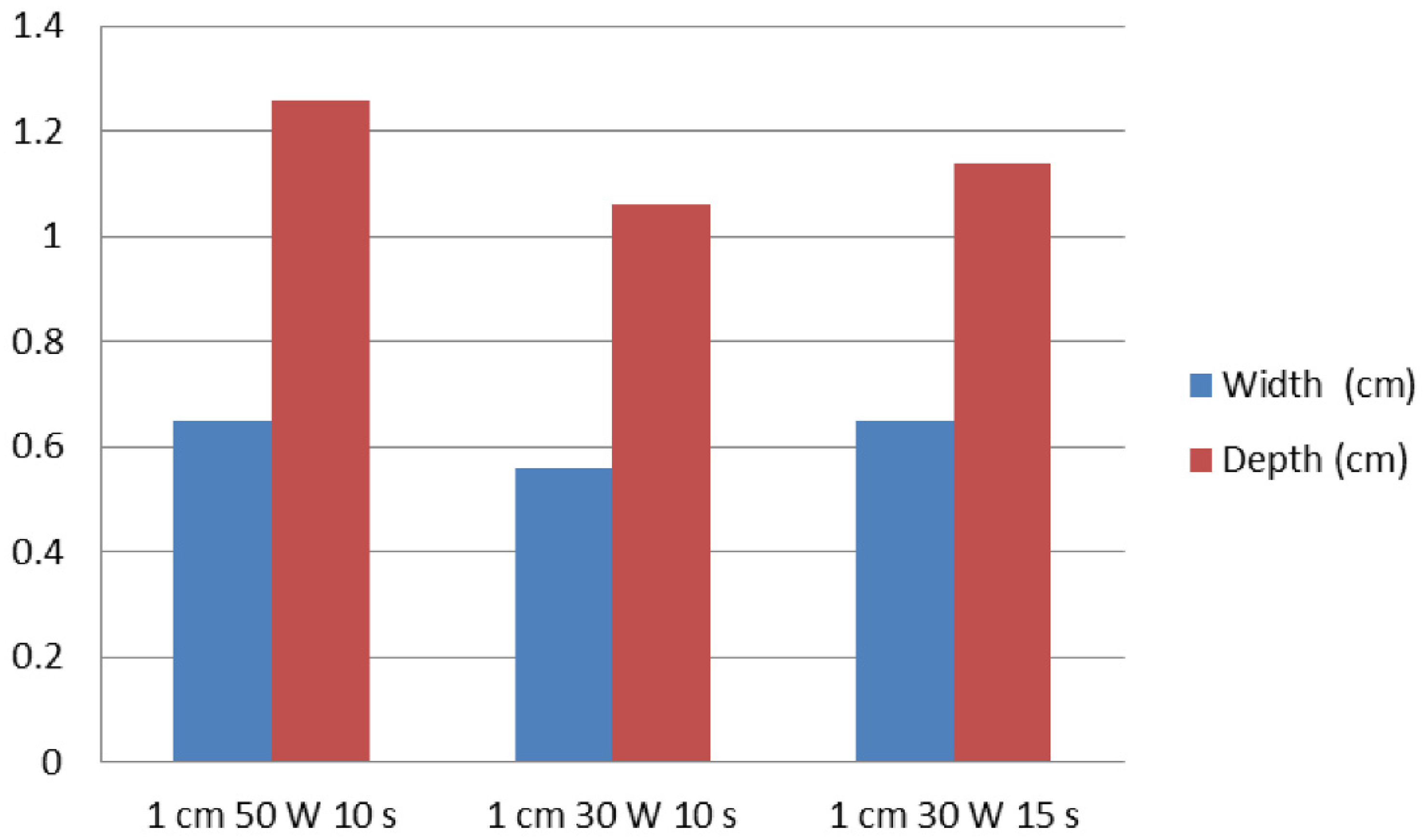
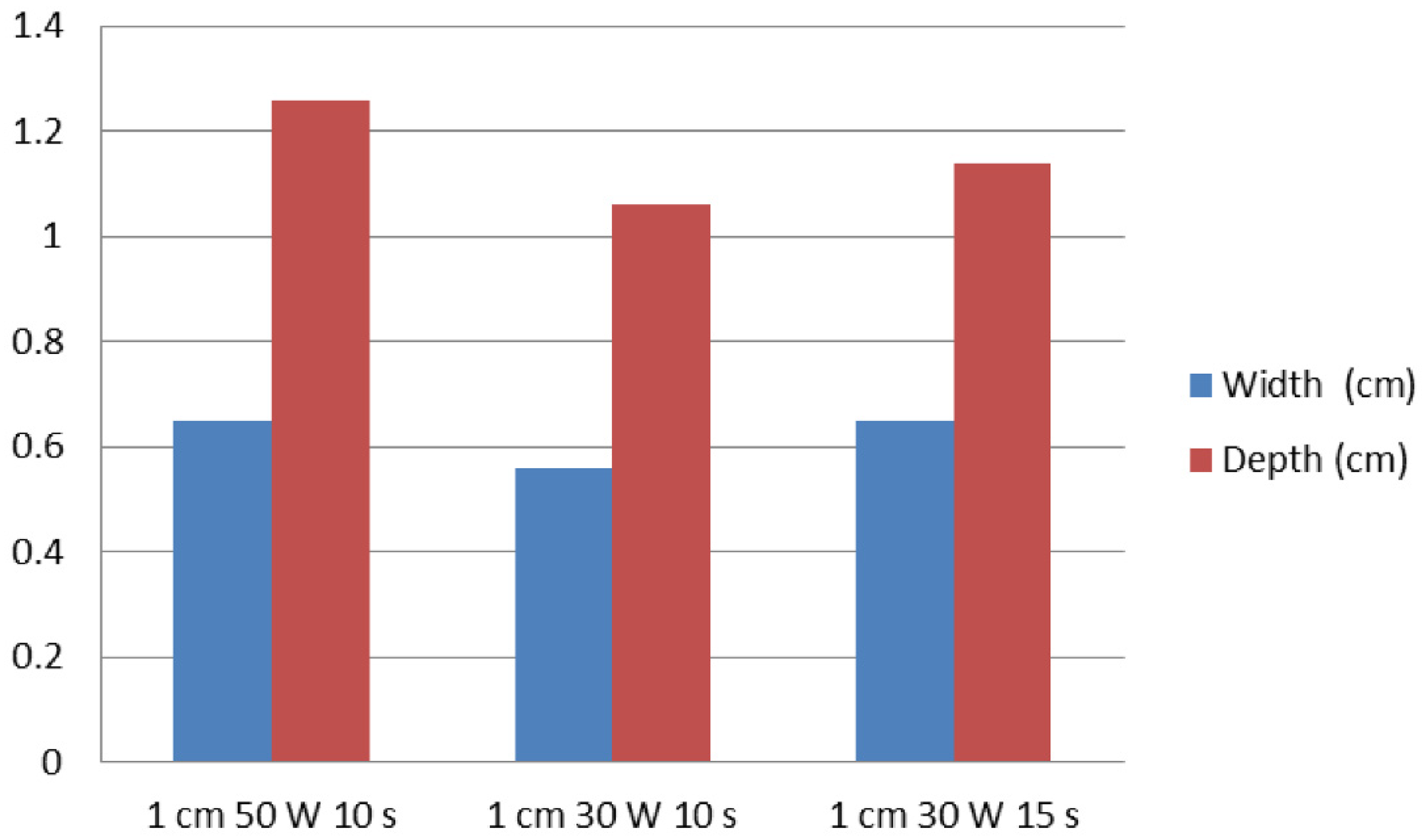
| Group A (1 cm, 30 W, 10 s) | Group B (1 cm, 30 W, 15 s) | Group C (1 cm, 50 W, 10 s) | |
|---|---|---|---|
| Ablation width, mean (SD), cm | 0.56 ± 0.05 | 0.65 ± 0.06 | 0.65 ± 0.05 |
| Ablation depth, mean (SD), cm | 1.06 ± 0.29 | 1.14 ± 0.05 | 1.26 ± 0.09 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, S.-H.; Oh, D.; Huh, G.; Song, T.-J.; Seo, D.-W. In Vivo Evaluation of a Novel Radiofrequency Ablation Electrode in Pig Livers. Appl. Sci. 2022, 12, 6791. https://doi.org/10.3390/app12136791
Cho S-H, Oh D, Huh G, Song T-J, Seo D-W. In Vivo Evaluation of a Novel Radiofrequency Ablation Electrode in Pig Livers. Applied Sciences. 2022; 12(13):6791. https://doi.org/10.3390/app12136791
Chicago/Turabian StyleCho, Sung-Hyun, Dongwook Oh, Gunn Huh, Tae-Jun Song, and Dong-Wan Seo. 2022. "In Vivo Evaluation of a Novel Radiofrequency Ablation Electrode in Pig Livers" Applied Sciences 12, no. 13: 6791. https://doi.org/10.3390/app12136791
APA StyleCho, S.-H., Oh, D., Huh, G., Song, T.-J., & Seo, D.-W. (2022). In Vivo Evaluation of a Novel Radiofrequency Ablation Electrode in Pig Livers. Applied Sciences, 12(13), 6791. https://doi.org/10.3390/app12136791