
Feasibility of Pilates for Late-Stage Frail Older Adults to Minimize Falls and Enhance Cognitive Functions

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Pilates Intervention
2.3. Assessments
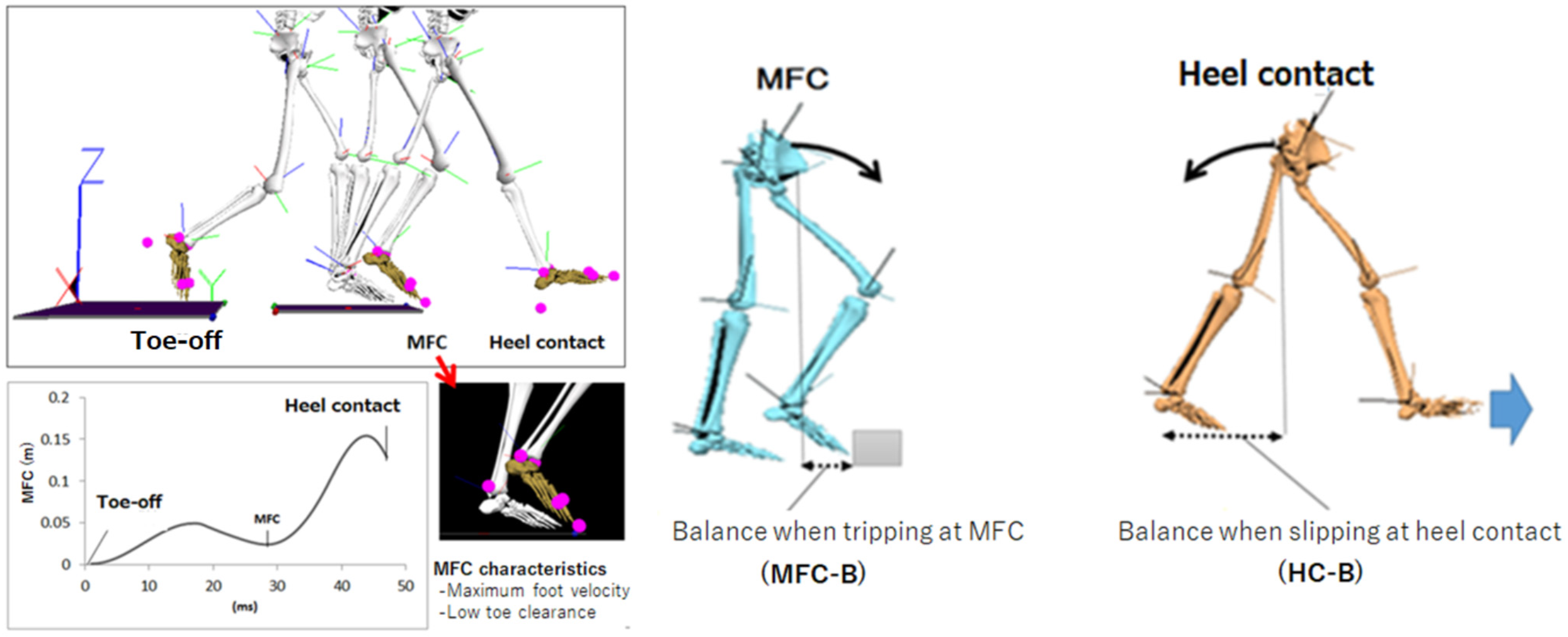
2.3.1. Falling Risks
2.3.2. Cognitive Functions
2.3.3. Two-Dimensional Mood Scale (TDMS)
2.4. Statistical Analysis
- (i)
- Falling risks (MFC, MFC-B and HC-B): motion capture data distinguished the right and left side separately; therefore, a (2 × 2 × 2 = group × limb × intervention) repeated measure of analysis of variance (ANOVA) was employed. Any interaction effects were further examined by Tukey’s post hoc analysis.
- (ii)
- Cognitive functions (MMSE and TMT-A): a (2 × 2 = group × intervention) design was applied to obtain Pilates effects.
- (iii)
- Mood (TMTS): averaged pre- and post-intervention TDMS scores were compared by independent t-tests in the Pilates group.
3. Results
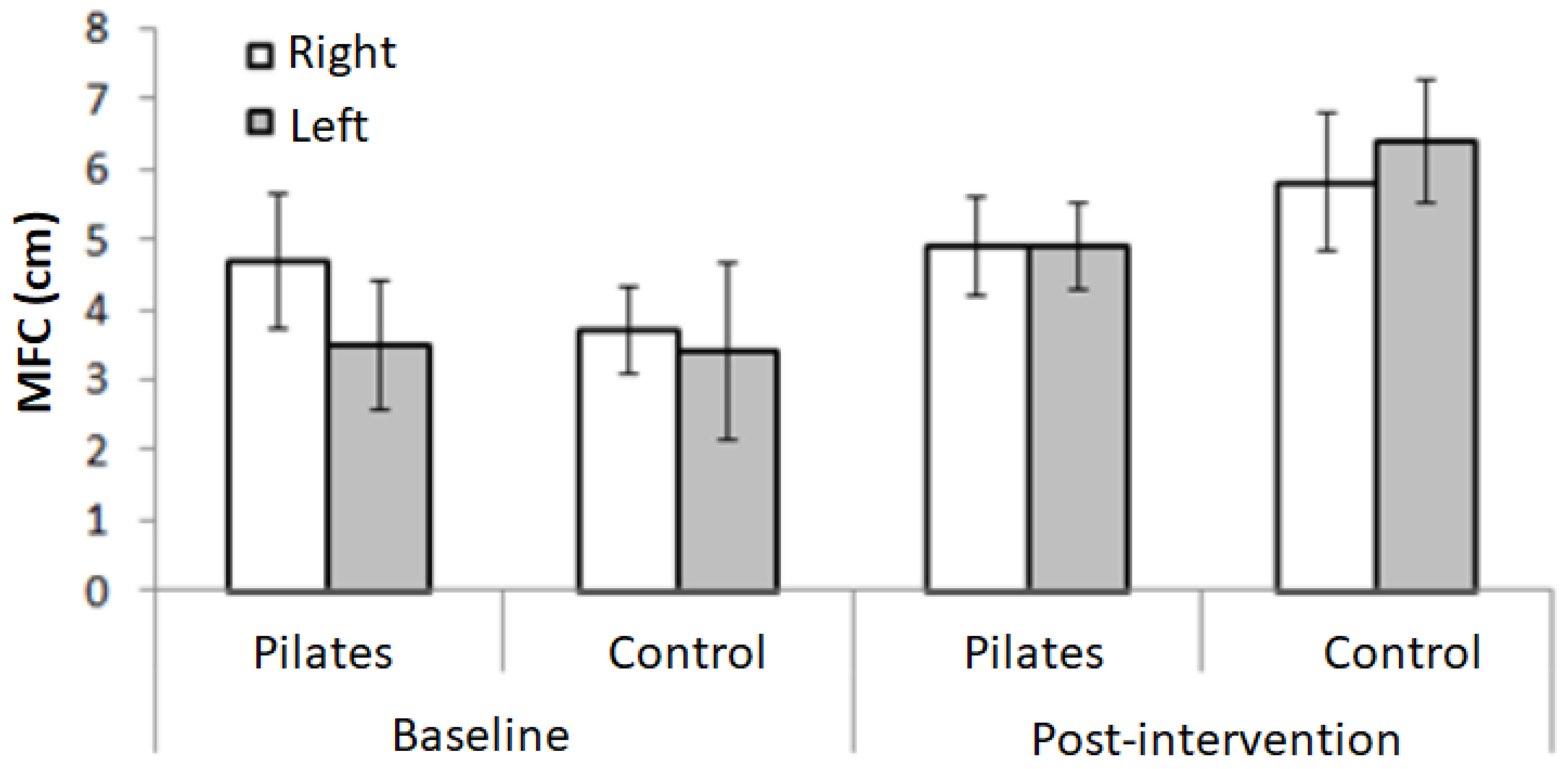
3.1. Pilates Effects on Falling Risks
3.2. Pilates Effects on Cognitive Functions
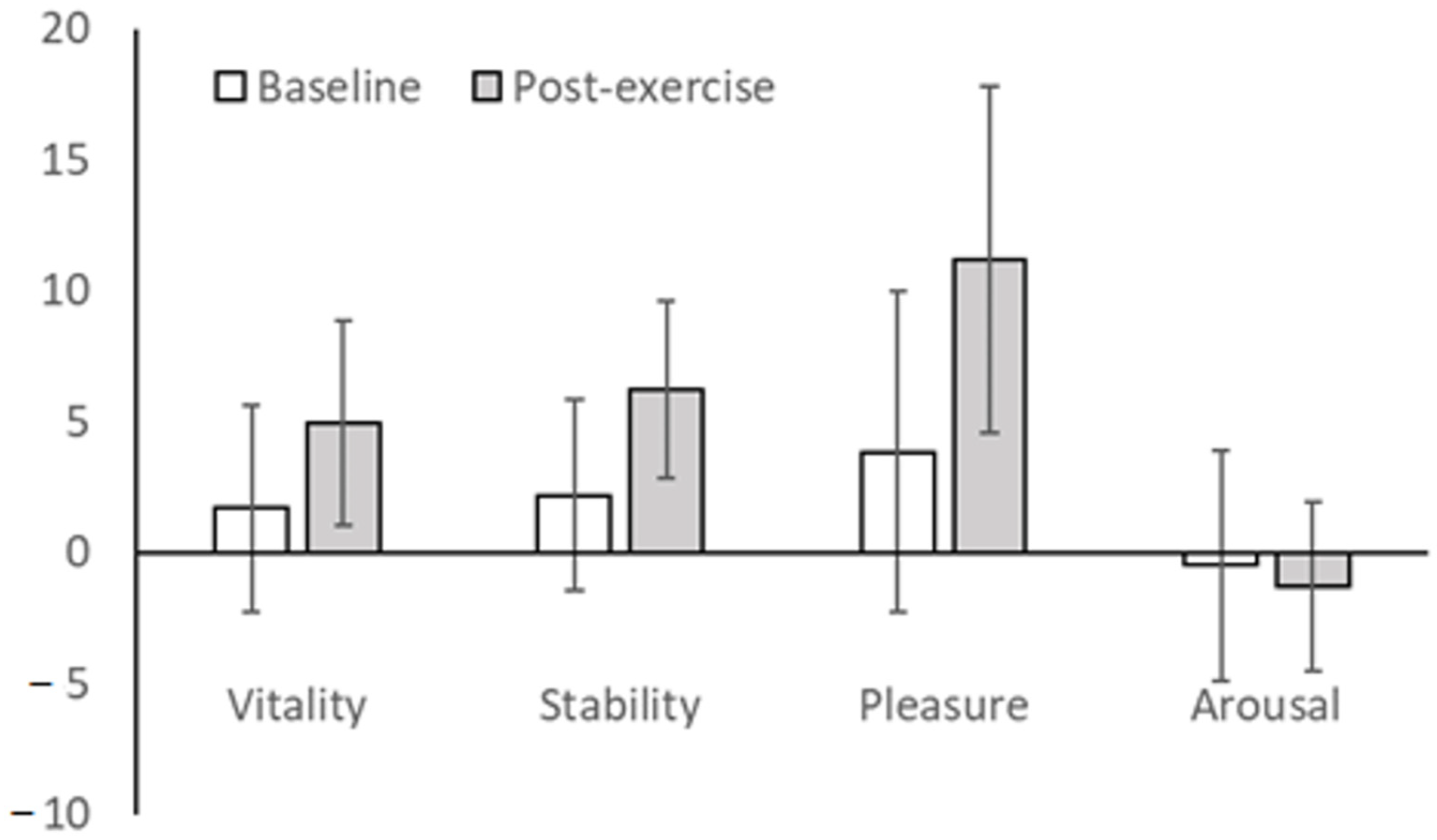
3.3. Pilates Effects on Mood
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| No | Contents | Detail | Reps |
|---|---|---|---|
| 1. Warm-up: Lower Body (3 min) | Position: Seated | ||
| A | Toe mobility | toe loosen (flex/extension/close-open) | 3 each |
| B | Ankle joint mobility | dorsi flexion/planter flexion/rotation | 3 each |
| C | Calf massage | from ankle joint to knee | 3 |
| D | Hip mobility | flex/extension/rotation | 3 |
| E | Knee mobility | flex/extension ※with towel | 3 |
| 2. Warm-up: Upper Body (2 min) | Position: Seated | ||
| A | Spine mobility | flex/extension/rotation/lateral flexion | 2 each |
| B | Shoulder stretch | retraction/protraction/elevation/depression/upward rotation/downward rotation | 2 each |
| C | Face stretch | clasp and unclasp face/tongue out | 3 each |
| 3. Core activation (5 min): ⌈Modified Pilates⌋ | Position: Seated | ||
| A | Pelvic rocking | Front-back/left-right/rotation | 3 each |
| B | Core activation | (1) confirming correct alignment of ischium/pubis/coccyx (2) set up ischium and extend spine toward ceiling (3) activating pelvic floor muscles (4) raise center of gravity (5–10 s) | 2 |
| 4. Breathing (5 min): ⌈Modified Pilates⌋ | Position: Seated/Child pose | ||
| A | Diaphragmatic breathing | Seated: inflate stomach when breathing | 3 |
| B | Breathing on the back | Child pose: breathing towards back | 3 |
| C | Lateral breathing | Seated: set pelvis to neutral position, continue applying abdominal pressure, spread rib cage | 2 |
| 5. Walking Exercise (3 min): ⌈Pitago⌋tm | Position: Standing | ||
| A | Standing on toe/heel | stand against wall and activate core shift weight back and forth | 5 |
| B | Standing one leg | stand against wall and activate core raise one leg and hold for 5 s | 3 each |
| C | Tandem stretch | line up right and left foot on line shift weight slowly back and forth | 2 each |
| 6. Warm-down (2 min) | Position: Seated | ||
| A | Tapping | awaken sensory nerves | 1 |
| B | Deep breath | breath deeply with movement of arms | 3 |
References
- Cabinet Office, Government of Japan (Japanese). Available online: https://www8.cao.go.jp/kourei/whitepaper/w-2021/zenbun/pdf/1s1s_01.pdf (accessed on 14 June 2022).
- Kropf, N.P. Life span: Older adultshood/seniors (from 60 to 75). Enclypedia Soc. Work 2020. [Google Scholar] [CrossRef]
- Portland University. Late Adulthood. Available online: https://pdx.pressbooks.pub/humandevelopment/chapter/late-adulthood/ (accessed on 8 June 2022).
- Arai, H. Definition of older people: Time to reconsider the definition? Jpn. Geriatr. Soc. 2019, 56, 1–5. (In Japanese) [Google Scholar]
- Orimo, H.; Ito, H.; Suzuki, T.; Atsushi, A.; Hosoi, T.; Sawabe, M. Reviewing the definition of “elderly”. Geriatr. Gerontol. Int. 2006, 6, 149–158. [Google Scholar] [CrossRef]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef]
- Cowley, A.; Goldberg, S.E.; Gordon, A.L.; Kerr, M.; Logan, P. Exploring rehabilitation potential in older people living with frailty: A qualitative focus group study. BMC Geriatr. 2021, 21, 165. [Google Scholar] [CrossRef]
- Tijsen, L.M.; Derksen, E.W.; Achterberg, W.P.; Buijck, B.I. Challenging rehabilitation environment for older patients. Clin. Interv. Aging 2019, 12, 1451–1460. [Google Scholar] [CrossRef]
- De Labra, C.; Guimaraes-Pinheiro, C.; Maseda, A.; Lorenzo, T.; Millán-Calenti, J.C. Effects of physical exercise interventions in frail older adults: A systematic review of randomized controlled trials. BMC Geriatr. 2015, 2, 154. [Google Scholar] [CrossRef]
- Vigelso, A.; Gram, M.; Wiuff, C.; Andersen, J.L.; Hilge, J.W.; Dela, F. Six weeks aerobic retraining after two weeks immobilization restores leg lean mass and aerobic capacity but does not fully rehabilitate leg strength in young and older men. J. Rehabil. Med. 2015, 47, 552–560. [Google Scholar] [CrossRef]
- Shanahan, C.J.; Boonstra, F.M.C.; Cofré Lizama, L.E.; Strik, M.; Moffat, B.A.; Khan, F.; Kilpatrick, T.J.; van der Walt, A.; Galea, M.P.; Kolbe, S.C. Technologies for advanced gait and balance assessments in people with multiple sclerosis. Front. Neurol. 2018, 2, 708. [Google Scholar] [CrossRef]
- Buisseret, F.; Catinus, L.; Grenard, R.; Jojczyk, L.; Fievez, D.; Barvaux, V.; Dierick, F. Timed Up and Go and Six-Minute Walking Tests with Wearable Inertial Sensor: One Step Further for the Prediction of the Risk of Fall in Elderly Nursing Home People. Sensors 2020, 20, 3207. [Google Scholar] [CrossRef]
- Beauchet, O.; Annweiler, C.; Montero-Odasso, M.; Fantino, B.; Herrmann, F.R.; Allali, G. Gait control: A specific subdomain of executive function? J. Neuroeng. Rehabil. 2012, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Dismore, L.; Hurst, C.; Sayer, A.A.; Aspray, T.; Granic, A. Study of the older adults’ motivators and barriers engaging in a nutrition and resistance exercise intervention for sarcopenia: An embedded qualitative project in the MilkMAN pilot study. Gerontol. Geriatr. Med. 2020, 6, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Boyle, P.A.; Buchman, A.S.; Wilson, R.S.; Leurgans, S.E.; Bennett, D.A. Association of muscle strength with the risk of Alzheimer disease and the rate of cognitive decline in community-dwelling older persons. Arch. Neurol. 2009, 66, 1339–1344. [Google Scholar] [CrossRef] [PubMed]
- Kitayuguchi, J.; Kamada, M.; Inoue, S.; Kamioka, H.; Abe, T.; Okada, S.; Mutoh, Y. Association of low back and knee pain with falls in Japanese community-dwelling older adults: A 3-year prospective cohort study. Geriatr. Gerontol. Int. 2017, 17, 875–884. [Google Scholar] [CrossRef]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.M.; Lamb, S.E. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012, 9, CD007146. [Google Scholar]
- Bennett, J.A.; Winters-Stone, K. Motivating older adults to exercise: What works? Age Ageing 2011, 40, 148–149. [Google Scholar] [CrossRef]
- Pilates, J.H. Return to Life through Contrology; Pilates Method Alliance Inc.: Miami, FL, USA, 2010. [Google Scholar]
- Rogers, F.R.; Pilates, J.H. The Pilates Pamphlet: Return to Life through Contrology; American Foundation for Physical Fitness: Reston, VA, USA, 1957. [Google Scholar]
- Falbo, S.; Condello, G.; Capranica, L.; Forte, R.; Pesce, C. Effects of physical-cognitive dual task training on executive function and gait performance in older adults: A randomized controlled trial. BioMed Res. Int. 2016, 2016, 5812092. [Google Scholar] [CrossRef]
- Schmidt, J.A.; Gruman, C.; King, M.B.; Wolfson, L.I. Attrition in an exercise intervention: A comparison of early and later dropouts. J. Am. Geriatr. Soc. 2000, 48, 952–960. [Google Scholar] [CrossRef]
- Culligan, P.L.; Scherer, J.; Dyer, K.; Priestley, J.L.; Guingon-White, G.; Delvecchio, D.; Vangeli, M. A randomized clinical trial comparing pelvic floor muscle training to a Pilates exercise program for improving pelvic strength. Int. Urogynecol. J. 2010, 21, 401–408. [Google Scholar] [CrossRef]
- Watanabe, D.; Yoshida, T.; Watanabe, Y.; Yamada, Y.; Miyachi, M.; Kimura, M. Validation of the Kihon Checklist and the frailty screening index for frailty defined by the phenotype model in older Japanese adults. BMC Geriatr. 2022, 22, 478. [Google Scholar] [CrossRef]
- Pilates Method Alliance. The PMA Pilates Certification Exam Study Guide; Pilates Method Alliance, Inc.: Miami, FL, USA, 2007. [Google Scholar]
- Sarashina, E.; Mizukami, K.; Nagano, H.; Begg, R.K. Validity of Simple Health Assessments to Evaluate Locomotive and Cognitive Functions of Late-Stage Older Adults in Japan. Int. J. Sports Exerc. 2017, 3, 068. [Google Scholar] [CrossRef][Green Version]
- Begg, R.; Best, R.; Dell’Oro, L.; Taylor, S. Minimum foot clearance during walking: Strategies for the minimisation of trip-related falls. Gait Posture 2007, 25, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Smeesters, C.; Hayes, W.C.; McMahon, T.A. Disturbance type and gait speed affect fall direction and impact location. J. Biomech. 2001, 34, 309–317. [Google Scholar] [CrossRef]
- Nagano, H.; Levinger, P.; Downie, C.; Hayes, A.; Begg, R. Contribution of lower limb eccentric work and different step responses to balance recovery among older adults. Gait Posture 2015, 42, 257–262. [Google Scholar] [CrossRef]
- Bhatt, T.; Pai, Y.C. Prevention of slip-related backward balance loss: The effect of session intensity and frequency on long-term retention. Arch. Phys. Med. Rehabil. 2009, 90, 34–42. [Google Scholar] [CrossRef]
- Crevin, S.T.; Wisniewski, S.; Noel-Storr, A.H.; Trevelyan, C.M.; Hampton, T.; Rayment, D.; Thom, V.M.; Nash, K.J.E.; Elhamoui, H.; Milligan, R.; et al. Mini-mental state examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populations. Cochrane Database Syst. Rev. 2016, 13, CD011145. [Google Scholar] [CrossRef]
- Kodama, A.; Suzuki, Y.; Sakuraba, K.; Kume, Y.; Ota, H. The effect of deep micro vibrotactile stimulation on cognitive function of mild cognitive impairment and mild dementia. Int. J. Environ. Res. Public Health 2022, 19, 3803. [Google Scholar] [CrossRef]
- Tombaugh, T.N. Trail Making Test A and B: Normative data stratified by age and education. Arch. Clin. Neuropsychol. 2004, 19, 203–214. [Google Scholar] [CrossRef]
- García-Garro, P.A.; Hita-Contreras, F.; Martínez-Amat, A.; Achalandabaso-Ochoa, A.; Jiménez-García, J.D.; Cruz-Díaz, D.; Aibar-Almazán, A. Effectiveness of a Pilates training program on cognitive and functional abilities in postmenopausal women. Int. J. Environ. Res. Public Health 2020, 17, 3580. [Google Scholar] [CrossRef]
- Moreno-Segura, N.; Igual-Camacho, C.; Ballester-Gil, Y.; Blasco-Igual, M.C.; Blasco, J.M. The effects of the Pilates training method on balance and falls of older adults: A systematic review and meta-analysis of randomized controlled trials. J. Aging Phys. Act. 2018, 26, 327–344. [Google Scholar] [CrossRef]
- Sakairi, Y.; Nakatsuka, K.; Shimizu, T. Development of the two-dimensional mood scale for self-monitoring and self-regulation of momentary mood states. Jpn. Psychol. Res. 2013, 55, 338–349. [Google Scholar] [CrossRef]
- Massy-Westropp, N.M.; Gill, T.K.; Taylor, A.W.; Bohannon, R.W.; Hill, C.L. Hand Grip Strength: Age and gender stratified normative data in a population-based study. BMC Res. Notes 2011, 14, 127. [Google Scholar] [CrossRef] [PubMed]
- Moosabhoy, M.A.; Gard, S.A. Methodology for determining the sensitivity of swing leg toe clearance and leg length to swing leg joint angles during gait. Gait Posture 2006, 24, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Case, L.E.; Coats, J. Commentary on “Progression of ankle plantarflexion contractures and functional decline in Duchenne muscular dystrophy: Implications for physical therapy management”. Pediatric Phys. Ther. 2019, 31, 67. [Google Scholar] [CrossRef] [PubMed]
- Nagano, H.; Begg, R.K.; Sparrow, W.A.; Taylor, S. Ageing and limb dominance effects on foot-ground clearance during treadmill and overground walking. Clin. Biomech. 2011, 26, 962–968. [Google Scholar] [CrossRef]
- Manckoundia, P.; Mourey, F.; Pérennou, D.; Pfitzenmeyer, P. Backward disequilibrium in elderly subjects. Clin. Interv. Aging 2008, 3, 667–672. [Google Scholar] [CrossRef]
- Corti, E.J.; Johnson, A.R.; Riddle, H.; Gasson, N.; Kane, R.; Loftus, A.M. The relationship between executive function and fine motor control in young and older adults. Hum. Mov. Sci. 2017, 51, 41–50. [Google Scholar] [CrossRef]
- Lim, E.-J.; Hyun, E.-J. The Impacts of Pilates and Yoga on Health-Promoting Behaviors and Subjective Health Status. Int. J. Environ. Res. Public Health 2021, 18, 3802. [Google Scholar] [CrossRef]
- De Silva, L.D.; Shiel, A.; McIntosh, C. Pilates reducing falls risk factors in healthy older adults: A systematic review and meta-analysis. Front. Med. 2021, 8, 708883. [Google Scholar] [CrossRef]



| Biological | ||||
|---|---|---|---|---|
| Pilates | Control | |||
| Age (years) | 83.4 ± 5.0 | 84.8 ± 4.3 | ||
| Height (cm) | 144.4 ± 4.3 | 148.6 ± 11.1 | ||
| Body mass (kg) | 48.3 ± 7.5 | 51.0 ± 9.9 | ||
| Systolic blood pressure (mmHg) | 145.8 ± 17.6 | 153.4 ± 22.9 | ||
| Diastolic blood pressure (mmHg) | 78.7 ± 11.3 | 84.0 ± 12.2 | ||
| Pulse (beats/min) | 85.8 ± 12.4 | 81.6 ± 9.1 | ||
| Physical | ||||
| Pilates | Control | |||
| Right | Left | Right | Left | |
| Grip strength (kg) | 15.8 ± 2.8 | 15.3 ± 3.1 | 18.3 ± 4.0 | 16.1 ± 3.3 |
| Single leg standing (s) | 8.8 ± 11.3 | 8.2 ± 11.5 | 3.4 ± 2.7 | 3.0 ± 1.8 |
| Step length (cm) | 8.1 ± 2.4 | 7.4 ± 3.0 | 9.3 ± 2.7 | 8.0 ± 2.6 |
| Step width (cm) | 10.6 ± 1.3 | 10.5 ± 1.3 | 9.3 ± 1.5 | 9.1 ± 1.9 |
| Double support time (s) | 0.23 ± 0.11 | 0.23 ± 0.13 | 0.26 ± 0.08 | 0.30 ± 0.17 |
| Sit and reach (cm) | 31.0 ± 10.4 | 23.9 ± 8.5 | ||
| Dynamic Balance | Pre-Intervention | Post-Intervention | Effects | ||
|---|---|---|---|---|---|
| Pilates | Control | Pilates | Control | ||
| MFC-B Right | 6.7 ± 3.0 | 7.8 ± 2.7 | 4.7 ± 2.3 | 5.7 ± 2.6 | NS |
| MFC-B Left | 4.8 ± 2.5 | 5.9 ± 3.1 | 8.5 ± 2.0 | 5.8 ± 2.1 | |
| HC-B Right | 5.8 ± 2.6 | 5.5 ± 2.5 | 9.9I×G ± 2.7 | 5.5 ± 2.0 | I, I × G |
| HC–B Left | 5.5 ± 2.7 | 4.6 ± 2.5 | 10.5I×G ± 2.9 | 4.7 ± 2.0 | |
| Baseline | Post-Intervention | |||
|---|---|---|---|---|
| Pilates | Control | Pilates | Control | |
| MMSE (points) | 23.4 ± 4.1 | 23.4 ± 4.6 | 24.1 ± 4.9 | 23.1 ± 6.4 |
| TMT-A (s) | 297.0 ± 240.4 | 191.2 ± 106.1 | 229.6 ± 124.7 | 239.6 ± 113.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarashina, E.; Mizukami, K.; Yoshizawa, Y.; Sakurai, J.; Tsuji, A.; Begg, R. Feasibility of Pilates for Late-Stage Frail Older Adults to Minimize Falls and Enhance Cognitive Functions. Appl. Sci. 2022, 12, 6716. https://doi.org/10.3390/app12136716
Sarashina E, Mizukami K, Yoshizawa Y, Sakurai J, Tsuji A, Begg R. Feasibility of Pilates for Late-Stage Frail Older Adults to Minimize Falls and Enhance Cognitive Functions. Applied Sciences. 2022; 12(13):6716. https://doi.org/10.3390/app12136716
Chicago/Turabian StyleSarashina, Eri, Katsuyoshi Mizukami, Yasuyo Yoshizawa, Junko Sakurai, Akane Tsuji, and Rezaul Begg. 2022. "Feasibility of Pilates for Late-Stage Frail Older Adults to Minimize Falls and Enhance Cognitive Functions" Applied Sciences 12, no. 13: 6716. https://doi.org/10.3390/app12136716
APA StyleSarashina, E., Mizukami, K., Yoshizawa, Y., Sakurai, J., Tsuji, A., & Begg, R. (2022). Feasibility of Pilates for Late-Stage Frail Older Adults to Minimize Falls and Enhance Cognitive Functions. Applied Sciences, 12(13), 6716. https://doi.org/10.3390/app12136716