1. Introduction
The recent COVID-19 pandemic has forced major changes onto many sectors, including commerce, manufacturing, education, and health care. This has resulted in business closures and reallocation of human resources to emergency functions [
1]. Working from home has become commonplace and encouraged where possible, and in-person interactions are being reduced. People are advised to wear masks, sanitize surfaces, and wash hands frequently. With human interactions strictly limited during this pandemic, robotics and artificial intelligence can be extremely useful to complement human resources remotely; thus, enabling sectors to continue normally and contributing to economic growth. Technological determinism is a socio-economic theory regarding how technology induces societal change and affects our lives [
1,
2,
3].
Robots are increasingly used in the health care field. For example, hospitals have used robots to disinfect rooms and provide comfort to patients [
4,
5]. Other uses for robots include delivery services, inventory control, replenishing stock, and measuring vital signs. Assistive robots are being designed to help quadriplegic patients with ADLs, such as feeding and self-care, and wearable “exoskeleton” robots assist with movement [
5]. More extensive use of robots could, not only help minimize the spread of COVID-19 between patients and essential workers, but also enhance the efficiency and accessibility of care, while dramatically improving patient outcomes. When considering expanding the scope of robots and integrating their presence into human lives, we must explore some ethical questions, to minimize any possible harm and whether this outweighs the benefit to humanity.
Robot technology has featured in popular culture such as movies and science fiction writing since the invention of automatic machines. Many works depict the rise of machines, resulting in human subservience or even the demise of humanity altogether. These portrayals affect public perception of real-life robotic technology. Surveys have shown that science fiction movies influence people’s ideas about robots [
6]. To reassure the public that their lives will not become real-life dystopic science-fiction scenarios ruled by robots, we must consider the ethical aspects of robotic development and adopt strict rules of conduct. Roboethics is a relatively new field; acknowledged in 2002 and in continuous development since. The principles of roboethics are considered in the design and manufacturing stage and in the implementation by end-users [
7]. The core ideas of roboethics are similar to the ethics of information technology, particularly regarding safe use and equitable access. Robots may also bring up new legal questions: who would be liable if a robot performed an illegal action? It is possible that an organization could be liable for the unforeseeable actions of a robot it created. There may also be gray areas in existing laws, as they apply to criminal intent when a machine makes decisions [
8,
9]. Roboethics establishes a structured way to address these kinds of moral or ethical dilemmas. Developing specific laws and ethical guidelines applicable to the robotics field may aid in integrating robots with daily life.
Within roboethics, the principle of respect for patients is associated with allowing informed and competent patients to make their own choices regarding their medical treatments. Moreover, ethical consideration respects a patient’s right to have control over information relating to their health and wellbeing. This concept is already well established in healthcare facilities with a traditional model of interaction between patient and healthcare practitioner; however, once a smart or semi-smart tool is designed and used in treatment, a deeper ethical investigation must be conducted. In this paper, we investigate several ethical aspects through which the iManus technology may impact the privacy of the patient–practitioner relationship and patient information. We propose some solutions to maintain confidentiality, with iManus acting in the treatment loop as a tech product. This paper reviews existing laws on the ethics in robotics, sensory systems, and AI fields, and selects the ethical aspects that are related to the iManus technology in particular, and which must be addressed to allow a patient or a therapist to safely, securely, and conveniently use the device.
2. The Laws of Roboethics
Isaac Asimov was the first to develop rules pertaining to robots in 1942 [
10]. At that time, robots were mainly the subject of fiction without real-life applications. Asimov described the following laws:
A robot may not injure a human being under any conditions or, through inaction, allow a human being to come to harm;
A robot must follow all orders given by qualified human beings as long as they do not conflict with Rule 1;
A robot must protect its own existence, except where that conflicts with Rules 1 and 2;
(Zeroth law) No robot may harm humanity or, through inaction, allow humanity to come to harm.
Asimov’s Laws are general and pre-date the wide variety of robotics applications used today. The field of robotics has undergone significant advancement since 1942, when Asimov wrote these rules. Some of these laws are applicable to modern robotic technology. However, Asimov’s Laws focus on the robots themselves and not the humans who design them. Revisions to the original laws have been attempted over the years, in consideration of the changes in robotic technologies that have emerged since then. There are now two branches of the roboethics field: engineering ethics, and machine ethics [
11]. Engineering ethics is applicable to engineers and computer scientists involved in the creation of new robotic technology. Machine ethics is about the designing of robots to incorporate the internal ethical principles and moral decision-making patterns that robots can perform automatically.
Murphy and Woods proposed a revised version of Asimov’s Laws. Rather than focusing on machine ethics, these revisions are more applicable to the humans that design them [
12].
Human-robot work systems must comply with rigorous professional and legal standards for safety and ethics. Without such compliance, humans cannot utilize robots in a working system;
Robots must respond to humans only so far as determined by each robot’s role;
Humans must provide robots with autonomous mechanisms for self-preservation. Those mechanisms must relinquish control as needed to comply with the previous two laws.
The updated Laws follow the ideas of engineering ethics, but the lack of specific directives makes them difficult to apply to all robots or to incorporate into government or industry policymaking. As a starting point, however, these Laws have been useful for institutions around the world as basic ethical standards in the field of robotics.
In Canada, roboethics are poorly regulated, as there is no central agency to offer oversight. Universities and funding bodies have developed their own guidelines but cannot enforce them without the authority to do so.
One of the most exhaustive AI ethics declarations has come from University of Montreal scholars, who in 2018 put forth the Montreal Declaration for Responsible Development of Artificial Intelligence [
13]. The Montreal Declaration establishes an ethical framework for AI development, to benefit the common good. The Montreal Declaration is for anyone who wishes to develop AI ethically, as well as political lobbyists and policymakers involved in AI development. The Montreal Declaration addresses ten ethical principles to follow during the development of AI:
The above principles have their limitations, in that they center around humans and not highly advanced AI systems. The ethical dilemmas presented here are further complicated in that it may be impossible to program a robot to know what “harm”, “humanity”, or “existence” are.
The University of British Columbia has established the survey-based N-Reasons Platform [
14]. This platform allows for public input; various types of robots are presented, and participants state why they feel a particular robot should be created or not. Results can be used to gauge public perspectives on robotics when developing future policies. For example, robots are now used in combat to carry loads [
4] and help in bomb disposal [
15]. It is conceivable that, in the future, this could lead to robots being used for carrying firearms and involvement in warfare. With the goal being to harm opposing human forces, this would clearly violate Asimov’s Laws. It could also be argued that the side that uses robots helps save the lives of its own troops. When the N-Reasons survey was conducted in 2010, the public generally supported robots for bomb disposal but disapproved of fully automated armed aircraft [
14]. In social and health care applications, the N-Reasons survey revealed that the public largely approved using therapeutic robot animals.
In Canada, the robotics field is under the realm of the funding agency Natural Sciences and Engineering Research Council of Canada (NSERC). NSERC provides policies regarding ethical standards and values, conflicts of interest, private interest, decision-making, and confidentiality. NSERC funds 1.2 billion dollars in capital towards research in engineering and the natural sciences; therefore, it heavily influences the direction of innovation in Canada. While the NSERC code of ethics does not provide robot-specific guidelines, it supports two robotics networks within its domain: (1) the NSERC Canadian Field Robotics Network (NCFRN), and (2) the NSERC Canadian Robotics Network (NCRN). The NCFRN [
16] consists of academic researchers, government, and industry partners creating robotic systems that are functional in outdoor environments such as land, water, air, and human communities [
17]. The NCRN currently streams robotics into two categories: interactive autonomy, and resilient autonomy. The interactive autonomy stream researches the design of robots that interact and collaborate with humans. The resilient autonomy stream involves designing robots capable of working in harsh conditions for lengthy expeditions. Both areas of NCRN research may play a significant role in developing robots that continue to be useful, even after the COVID-19 pandemic has ended.
3. Types of Roboethical Considerations
In the development of any new robotic technology, there are ethical questions to contemplate before it is released for use by and for the public. We explore three categories here:
The robotics field is ever evolving, and more categories may arise in future as the technology develops. Among these considerations, we identify the most recurrent ones related to the emerging technologies offering telecare and remote monitoring services. These emerging modalities of intervening with patients highlight ethical issues related to the transfer of data and the safety of a remote patient who may feel left unassisted. Above all, neuro-rehabilitation technologies have the merit of serving the common good by enabling access to care remotely and lowering the direct and indirect cost of care. Access to care for all geographic regions of a given jurisdiction brings a level of equity that healthcare systems struggle to attain.
3.1. Data
Data use and privacy has become a topic of interest as technology advances. As data rapidly grows into a valuable commodity, ethical questions arise regarding its use and storage. Robots may hold sensitive data that must be managed judiciously. Privacy of a user’s data is of utmost concern. User consent to record their data may be obtained, but the rules surrounding data security or ownership may be uncertain.
The following questions about data use should be considered:
Where is the data stored (local or in the cloud)?
Who does the recorded data belong to (user or robotics company)?
Is privacy of the recorded data assured?
Can the data be breached, and if so, can its use cause harm?
Should users be compensated if their data is used for research or sale to third parties?
For taxpayer-funded enterprises, should the data generated be made publicly accessible?
Issues surrounding data rights and security need to be dealt with in the early stages of robot design, so that the resulting robotic technology upholds human rights and contributes to the betterment of humanity rather than its detriment.
3.2. Common Good
With advances in robot technology and their increasing role in human society, those who design robots should contemplate their impact beyond the intended purpose. The Institute of Electrical and Electronics Engineers (IEEE) and European Commission European Group on Ethics in Science and New Technologies have developed specific guidelines regarding positive advancements for human welfare and humanity as a whole [
18]. As technologies are continually evolving, their future impact on humanity must be considered in the early stages of development. For example, with military research spending reaching astronomical levels, should an arms race of opposing AI forces be left unchecked? Can robots support human autonomy and prosperity? Can all humans around the world benefit from robot technology?
3.3. Safety
Human safety in robotics use is of primary concern. With the increasing use of autonomous machines operated by robots directly in charge of human safety, the trolley problem arises [
19]. Consider the example of self-driving cars and the decision-making necessary when a collision is imminent. Whose lives are prioritized, the car’s own passenger(s) or a larger group of bystanders? The robot would need to decide this instantaneously. A computer scientist would need to apply ethical principles when programming the robot’s algorithm, to ensure it is capable of making ethical decisions. The difficulty is that there is no right or wrong answer to this dilemma, especially in healthcare. Individual programmers may have different philosophical beliefs. Consistency in robotic safety algorithms would require oversight and regulation through governance bodies. Safety, transparency, documentation, and compliance with regulation would help ensure that robots benefit the future of life on earth.
Another ethical concern is the safety of robots themselves. If humans can create machines with human-like intelligence, is it ethical to destroy them after they developed a “social network” and a “social life” with other robots and humans? Are they intelligent beings to be treated with compassion, or merely tools for human use, to be destroyed when they have served their purpose?
4. Ethical Considerations for Robotics Research and Development during COVID-19
Automation has been favorable to the economy, as the industry benefits from faster product manufacture and distribution. Service and health care industries and educational institutions are embracing robots and AI systems. Advances in the field of robotics are producing robots with increased speed and ability. It has been forecast that robots could reach a level of intelligence on par with humans sometime during the 21st century [
20,
21]. It is, therefore, imperative to design roboethics policies that consider robotic intellect (usually AI-driven) and its implementation in human lives. The COVID-19 pandemic has sped up the use of robots, to minimize direct human contact and allow for remote working and learning. Although the use of robots in healthcare is less common than in industry, it seems likely that society will retain this increased use of robots, even once the pandemic is over. Ethical guidelines should be reviewed and updated, to ensure that the harm to society is minimized with the use of these newer, highly advanced robots.
4.1. Bonds between Humans and Robots
Although it may seem far-fetched to think of humans forming bonds with robots, this has been shown to happen when people are deprived of human contact. Consider the case of Paro, a social robot that took the form of a furry seal, which was used to provide stress relief and comfort to elderly care home residents who were isolated from their families because of the COVID-19 pandemic lockdowns [
22,
23]. Many elderly people bonded with Paro, expressing feelings of love for it.
To avoid this scenario, if robots are to be used for human emotional support, every effort should be made to guarantee their lifespan. Perhaps, if a company is sold or goes out of business and shuts off its servers, the source code could be made public to ensure the continued function of the robot is possible. A company should not be able to use planned obsolescence for its own profit, while neglecting the needs of the users who form trusting relationships with their robots or rely on them to perform important tasks.
4.2. Loss of Jobs
There is no question that automation continually changes the job market with every new advance in robotic technology. Machines have increased productivity worldwide, while workers have seen a change in employment opportunities. Automation has caused lost jobs, but also created new ones. It is now estimated that at least 30% of workers’ tasks could be done by machines in 60% of occupations [
24]. Consequently, 375 million people worldwide may need to change jobs in the next decade, especially in sectors such as agriculture and manufacturing. Demographics, economic policies, and industry frameworks will affect overall labor displacement by automation.
The rate of change in the job market toward automation has increased as a response to global aging, the need for high-quality care, and the recent pandemic. With emergency health mandates in effect, many businesses were forced to close and/or change their operations. Employment positions that relied on in-person contact were particularly affected. In some cases, human employees were replaced with remote technology. Many laid-off workers returning to the workforce found a constricted job market and elected to return to post-secondary education to train for new job skills. Others found themselves joining the gig economy, with reduced income and job stability.
To prevent robots from working to the detriment of the “common good” principle, governments should intervene to ensure that workers displaced through automation are given education and re-training opportunities, enabling them to take advantage of the new career opportunities that come with an increasingly automated job market.
4.3. Roboethics and Health Care Pre- and Post-COVID-19
Due to COVID-19, many health care settings needed to drastically cut back their in-person services to urgent care only and delegate many health care interactions to an online or remote format, such as teleconferencing. It is harder for a health care practitioner to properly observe and guide a patient in this situation. This is particularly challenging in rehabilitation settings, where a patient needs to perform exercises to re-learn motor skills impaired by injury or illness. Robot use in health care is already on the rise, with a promising future in tele-rehabilitation and remote rehabilitation [
25,
26]. For a robot to automatically evaluate a patient’s motor performance, its assessment should pass the following criteria [
27]:
Acceptance by experts in the relevant field
Reliability, i.e., providing consistent results with repeated testing
Validity, i.e., measurement of the skill being assessed (rather than that of a related skill being performed simultaneously).
In assessing the reliability and validity of an individual robot for its teaching of motor skills in rehabilitation, we need to evaluate the similarity of the robot-delivered assessment to that of a human counterpart, how well it forecasts future performance, and how it measures against the current gold standard [
27,
28].
When considering the ethics of health care, and particularly rehabilitation, the effectiveness of the intervention is one major concern. Can a robot be an effective health care provider when it is unable (at present) to read a patient’s non-verbal cues? The question of dehumanization arises. Human interaction can play a significant role in a patient’s emotional well-being and healing. Do robots lack the warmth and empathy needed for an effective healing encounter? For many patients, particularly the elderly and infirm, an in-person health care visit provides essential social interaction that may be otherwise lacking. The impact of robotic care on the emotional needs of the patient must not be ignored.
Accessibility is another concern. Internet access is often needed to use robotic programs. Some elderly patients may not be familiar with internet use; other patients may live in remote areas with poor or nonexistent internet access. This may negatively impact their access to timely care. Cost may also be a deterrent. With some services such as physiotherapy paid for privately and often not covered by insurance, patients may be reluctant to pay out of pocket on a service until effectiveness has been shown.
Remote health care encounters have increased since the COVID-19 pandemic began, creating a chance to collect data on their effectiveness. If shown to be effective as a replacement for at least some in-person interactions, without detrimental effects to patients, we may see increasing use of robotic rehabilitation techniques in a post-COVID world.
5. iManus for Remote Rehabilitation and Learning
5.1. iManus Platform
iManus [
29] is a comprehensive, yet portable and easy-to-use platform that provides a wide range of supervised rehabilitation practice for those with upper limb disabilities after brain injury, such as stroke, Parkinson’s Disease, or Multiple Sclerosis. In other words, iManus is a portable hand tele-rehabilitation platform that constructs a non-expensive, effective, and continuous relationship between the patient and the therapist, to provide the best conditions for the patient to get back to his/her normal capabilities, as soon, and as much, as possible. In the following, we provide a technical description of the platform and its components and explain the strategy, logic, and functionality behind its operational schemes.
The platform consists of the following elements: a pair of sensorized smart gloves, a mobile app for the patient, a desktop interface for the therapist, and a cloud-based communication and storage software incorporated into all the components.
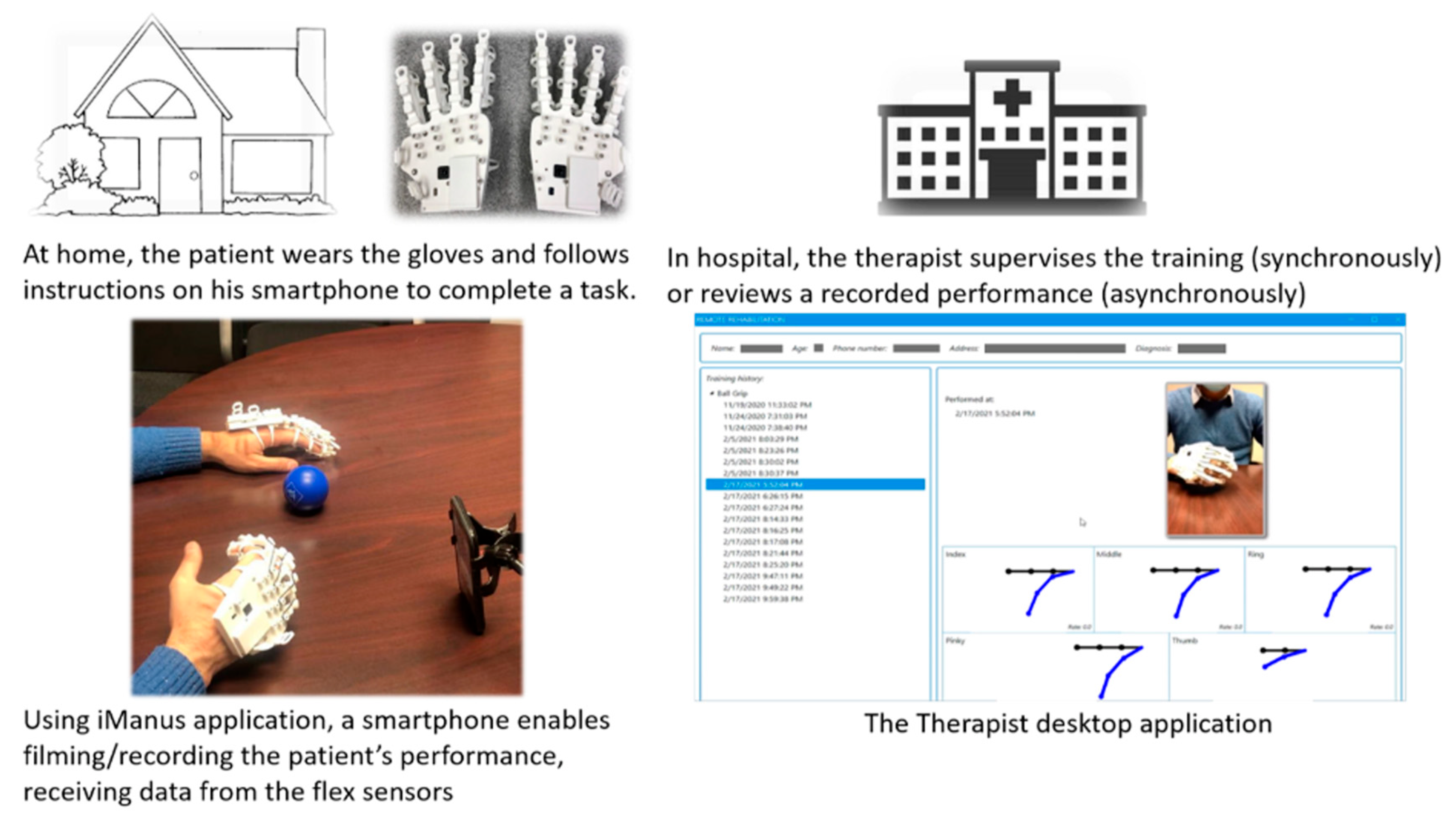
Figure 1 presents a schematic of the platform and its components. The philosophy behind the pair of smart gloves is that the best criterion to measure the quality of motion and acceptance level of practice is the normal and healthy body of the actual patient. The patient wears a glove on both healthy and impaired hands so that the target performance is personalized. When the patient performs a task, the healthy hand motion is recorded as the reference/target motion, which is patient specific. The glove is passively actuated with rubber band tensioners with different levels of elasticity, to help users regain control over their impaired hands when extending their fingers. To capture different kinematic and dynamic features of hand motion, the gloves are equipped with two types of sensory systems, which enable the platform to precisely capture and calculate all the key performance indicators (KPI) of each practice. This allows the rehab expert to gauge the user’s performance metrics. Each sensory system includes five flex sensors that measure the angle of each finger and one inertial measurement unit (IMU) that measures metrics of the palm section of the hand motion. There is compact hardware embedded inside the smart gloves which is connected to a set of flexible sensors located on the finger holder section of the gloves. The flexible sensors are resistance-based and measure the range of motion of each finger by translating the voltage levels (0 V~3.3 V) to the angles when a rehabilitation task is conducted. The hardware is also equipped with a 9-axis IMU module for measuring the rotations of the wrist, in terms of Euler Angles, and translating the roll, pitch, and yaw into supination, pronation, flexion, extension, ulnar deviation, and radial deviation movements. The acceleration data taken from the IMU sensor are also used for measuring the level of the shakiness of the patient’s hand.
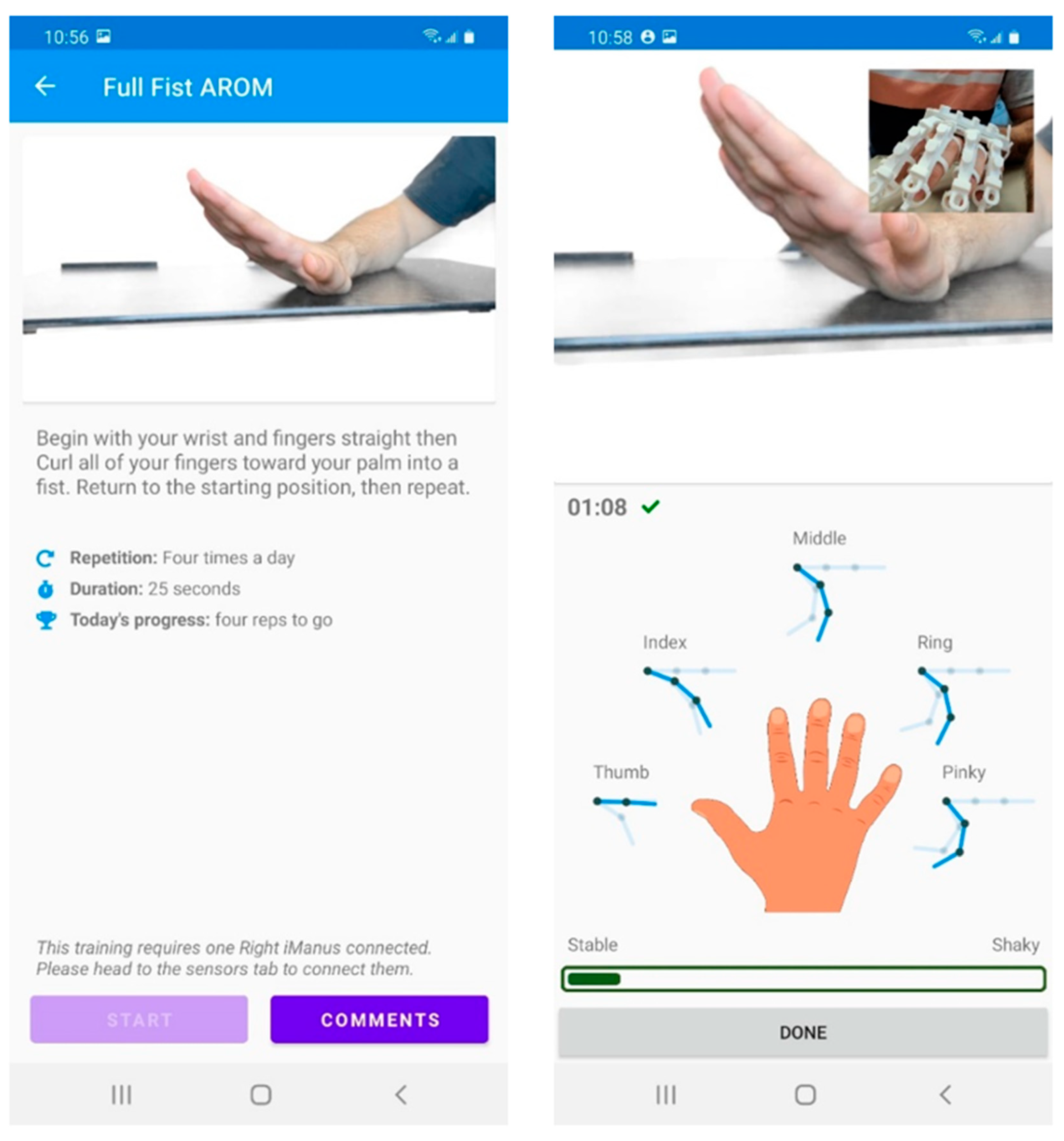
A cross-platform mobile app is also provided, which is compatible with both iOS and Android smartphones, as shown in
Figure 2. When the patient opens the mobile app and wears the gloves, the sensory system and the mobile app are wirelessly connected using the Bluetooth Low Energy (BLE) communication protocol, where the hardware processing unit acts as the peripheral, and the mobile app is the central. As such, all the sensory data (including IMU’s accelerations, gyro, and quaternion values and flex sensors’ raw data) are wirelessly transferred to the mobile app while the patient is conducting a task. The patient can then record both video and audio of the rehab task, while the task KPIs can be automatically saved in the cloud system as well. The system is designed to perform a scientific analysis of the patient’s performance KPIs and provide this to the therapist. The KPIs, along with the video/audio files, are accessible for both the patient and the therapist. On the other hand, the therapist can connect to the system using the desktop interface, monitor the performance and progress of the patient, and prescribe new tasks. The desktop interface is shown in
Figure 3. Thus, the therapist can judge the patient’s performance both qualitatively and quantitatively. As such, traditional treatment based on visually observing the patient’s performance and precise evaluation based on the recorded KPIs and their analysis is possible using the iManus platform. In addition, online and offline communication between the patient and the therapist enables the therapist to give immediate feedback on the patient’s practice, helping him/her increase the efficiency and effectiveness of each practice. The mobile and web applications are connected using a cloud-based mobile platform as a service (mPaaS). The cloud database is used to securely synchronize the data between the patient and therapist in real-time. Cloud storage is also used to store videos and the gathered sensory data.
It is worthwhile mentioning that when the therapist receives the data on the cloud system, he/she can also provide a pre-recorded task for the continuation of the patient’s training. This will also enable the therapist to manage remote patients in an organized, traceable, and standardized manner.
5.2. iManus in the Context of Treatment Domains
Patients who need neurorehabilitation undergo a learning process to regain as much of their lost mobility, coordination, and dexterity as possible. Bloom’s Taxonomy classifies the learning process into three domains: (1) cognitive, (2) psychomotor, and (3) effective [
30]. The cognitive learning domain applies to activities such as critical thinking, fact recall, decision-making, and overall understanding of a subject [
31,
32,
33]. The psychomotor domain involves learning applied skills, such as procedural knowledge and adaptive thinking. The psychomotor domain involves the honing of reflexes, dexterity, and purposeful, focused movement [
31,
32,
33]. The affective learning domain typically emphasizes emotional intelligence and personal values [
30,
32]. The interaction that iManus allows, in a way that we nowadays consider intuitive, namely teleconferencing, enables patients to manage their emotions positively as they interact with the therapist. Sharing information with their therapist in real-time and/or through an embedded messaging system relieves inner stress about overcoming recovery challenges.
A successful therapy program should have the following characteristics: technical competence on the therapist’s part, the implementation of ethical and professional values, socio-technical responsibility, patient management, and capability for self-assessment through feedback [
34]. These elements all relate to one or more of the learning domains described.
The psychomotor learning domain is where iManus has benefits to victims of brain injury, aiding them in recovery of hand motor skills. iManus also meets the above-described criteria of a successful therapy program, offering self-assessment through feedback. When patients complete hand rehabilitation tasks using iManus, they are practicing hand movements that are analyzed remotely through a sensor that offers instantaneous feedback. Patients can thereby recover their upper limb motor skills, spatial awareness, and proprioception. Patients using iManus work with a therapist, who can interpret their hand movements and offer guidance. During the COVID-19 pandemic, with many medical and therapeutic interactions transitioning to an online format, such rehabilitative programs are delivered via video conferencing. The application of new online technology can contribute to delivering quality rehabilitation once face-to-face sessions resume.
5.3. Ethical Aspects of iManus
As discussed, the impact of any new rehabilitative technology on health and quality of life must be considered when attempting to create new rehabilitation programs. The purpose of iManus is to enhance the current treatment model in rehabilitation settings, by improving accessibility to patients in-institution or remotely. We next discuss iManus regarding issues around data, common good, and safety. We also review possible ethical questions regarding the application of iManus in rehabilitation settings.
5.4. Data Considerations: Privacy, Security, Longevity
iManus gathers data through video footage and sensor data from patient movements. The recorded data are processed, transmitted, and saved, either on a local server or in cloud-based storage, both usually secured by the health institutions. Once the data is saved, it is available for both therapist and patient to review. For patient confidentiality, each patient can see only their own performance, while the therapist has access to the data for all patients under their care. This is a common way to store data in medical facilities, but this could also be vulnerable to hackers. With a device that relies on servers and cloud data backups, the importance of cybersecurity cannot be understated. Additionally, since remote therapists will assess patients solely on data from iManus, it is crucial to prevent tampering of the data, either by external forces or by the patients themselves. Personal health information acts, which vary according to the jurisdiction, establish rules that trustees of personal health information must follow when collecting, using, disclosing, maintaining, and destroying personal health information. Therefore, technology developers will manage the required technical maintenance under granted permission, but solely the trustees will own the data recorded by iManus and are responsible for its security. If data security is breached, videos remain problematic; however, each institution should develop its own policy to regulate the use of videos by, for example, restraining the content to the hand zones with no face or body parts shown. One great advantage of iManus is that it supports remote software upgrades. These upgrades are fast enough to be done between patients, thereby avoiding interference with the therapeutic session. iManus also comes with a 4-year guarantee and 24/7 support for the clinics that use it. Finally, to access data, install updates, and contact support for iManus, therapists and patients will require a strong internet connection, which brings up another ethical consideration. As more services switch to online platforms and newer technologies need the internet to function, internet access is increasingly being considered a human right [
35]. While internet use is widespread throughout most of North America, people living in more remote locations or abroad may still find lack of internet access a barrier. This should be considered in health care settings that serve patients living in areas without adequate internet access.
There is no feature in iManus that allows for human-like decision-making processes. As a result, it is the user’s responsibility to use iManus responsibly and ethically, as well as to adhere to privacy and security principles. Will iManus eventually replace therapists and render their jobs obsolete? No, it will not. Therapists’ workloads will remain unchanged, but the outcomes of their decisions will be enhanced due to their patients’ participation in iManus-led therapy remotely, in the absence of a face-to-face appointment. The therapist will also conduct the same number of face-to-face sessions remotely. In fact, iManus supports a synchronous mode of operation, which provides therapists and patients with the benefits of face-to-face interactions.
When vulnerable and/or disoriented patients become emotionally attached to robotic technology, ethical concerns may arise. Health technology may be taken away from a patient for a variety of reasons, or it may become unavailable due to business decisions. For example, Jibo, created by Jibo Inc., was the first robot to use intelligent speech and to learn new speech patterns as its users interacted with it [
23]. Jibo Inc. was eventually sold, and the servers that housed its source code were decommissioned. Furthermore, users who had been interacting with Jibo for some time discovered that it stopped working properly and eventually shut down completely. For some users, this was extremely upsetting. What about the iManus application? What could cause users to develop an emotional attachment to iManus? This is not a concern with iManus, because it is not a social robot, but an interactive platform designed for short-term use; usually a few months or as determined by the therapist. From the standpoint of the therapist, iManus will be an additional productivity tool that provides telecommunication, real-time or recorded quantitative data, and a discussion platform (chat). Texting patients is currently not permitted, because the privacy of the information could be jeopardized. However, in iManus, two-way information is communicated without the risk of it being compromised. The patient owns their account and can grant access to a therapist of their choosing or deny access to a therapist with whom they are no longer working.
5.5. Common Good: Benefits of iManus
Technological developments using the internet, virtual reality, 3D modeling, and high-level sensors are being applied to health care interventions beyond what was previously thought possible. Even with sophisticated technology, in-person supervision is required, and the devices are not portable, and therefore are not compatible with remote health care.
iManus is useful to support stroke rehabilitation programs remotely while social distancing measures are in place, during the pandemic, and once the pandemic response has ended. Health care settings such as rehabilitation clinics require program standardization and objective evaluation. iManus can give patients unbiased quantitative feedback in real-time. As therapists can upload rehabilitation programs to the server, patient programs can be designed to evidence-based guidelines and be individualized for specific patient needs. This provides rehabilitation clinics and health care researchers with a unique opportunity to standardize programs and assess the simulation session, with patients being the only experimental variable. Tactile Robotics is now carrying out studies for a comprehensive evaluation and comparison of rehabilitation programs in iManus-enabled versus standard clinical settings.
The COVID-19 pandemic was an important factor in changing the way we use traditional in-person healthcare models, and technology could help health care evolve to reach people who are unable to attend face-to-face visits with their providers. iManus allows patients to perform their prescribed exercises in their own time, which allows them to monitor and analyze their own progress, leading to faster recovery and better long-term outcomes. Since iManus is portable, it allows access to care for patients with brain injury around the globe, who may not otherwise be able to travel to a state-of-the-art rehabilitation clinic. Standardized programs could provide excellent clinical rehabilitation for patients living or working in remote places, far from quality health care facilities. To preserve the principle of equitable access to technology, Tactile Robotics has a marketing plan that can be adapted for interested facilities worldwide. Both right-hand and left-hand iManus smart-gloves are available, enabling treatment of impairments on either side. This parallels in-person therapeutic encounters and is inclusive of all patients in need of hand rehabilitative care. The outcomes from this rehabilitative approach are not only patient-oriented but also benefit society as whole, by reducing the family and community costs of care, and promoting the return to work and participation in daily activities.
5.6. Safety
iManus cannot cause harm to human beings when used as intended. As with any therapeutic exercise program, there is a risk of exacerbation of an injury, whether or not a robotic device is used. The guidance of a therapist in prescribing the exercises and checking on the patient’s progress minimizes that risk. It would be difficult to conceive a scenario where the use of iManus would cause further injury to the patient. Therefore, using iManus in a rehabilitation setting would not be a significant safety concern.
6. Potential Concerns with the Described Technology and Proposed Solutions
Since the iManus platform is a cutting-edge rehabilitation technology based on a remotely operable system Technology (See
Section 5.1) and is relatively new to the rehabilitation community, it is important to identify the possible risks associated with using the platform and suggest appropriate solutions and consideration of possible concerns. This would increase the platform’s reliability and determine its suitability and functionality in a well-defined framework. The following table addresses different operational concerns, their associated risks, and the proposed solution and considerations.
| Concern | Risk | Consideration/Solution |
| | |
| | The platform is operated on a secure local server, which is accessible only to authorized personnel Extra layers of security are provided in the cloud-based communication system.
|
| | |
| | |
| | |
| | |
| | The technology is designed to be easy to use, with guides and support videos. The programs offered are incremental, making it easy for the patient to follow easily, practice safely, and progress at a safe pace, as determined by the therapist.
|
| | The therapist will use/prescribe the product according to healthcare regulations and takes the responsibility defined in local jurisdictions. The technology provider will be obligated for after-sale support.
|
| | |
7. Conclusions
The COVID-19 pandemic has hastened the integration of robotics into many industries, as an effort to minimize human contact and slow the transmission of COVID-19. Moreover, due to factors such as global aging and the availability of quality care, robots have been used in place of humans for cleaning hospitals and comforting patients who found themselves isolated. With the sudden and unexpected onset of the pandemic and the need for emergency measures to contain it, robots were developed and deployed rapidly, without sufficient time to properly consider all aspects of roboethics. With recent advancements in technology and artificial intelligence, new devices are emerging every day for the treatment of patients with disabilities or movement deficiencies. Most of these devices collect data related to the patients’ health status. Usage of these devices requires a profound ethical investigation, to protect patients’ privacy. Several ethical aspects of the iManus technology are investigated in this paper. The relevant principles of data security, the common good, and safety should be fully examined.
This paper examines the ethical aspects of the creation and design of robots for hand rehabilitation. During the COVID-19 pandemic, rehabilitation services were forced to find alternatives to care for all but the most urgent cases, until it was deemed safe to resume close contact, with strict safety protocols in place. Since patient needs do not end with facility closures, it is a health care provider’s ethical responsibility to continue care, while minimizing risk to themselves. This has provided an opportunity for robots to train motor skills in rehabilitation patients. iManus is a new-generation, haptic-enabled smart glove that supports the recovery of upper limb function in patients with brain injury. When integrating iManus into a treatment plan, the security and privacy of patient data, and equal access to care should be prioritized. We discuss these ethical concerns and provide real-life examples of robotics use, as they applied to the COVID-19 pandemic. This may help engineers and researchers develop guidelines for the research and design of future robots.
Future work will focus on the implementation of the iManus technology in real clinical fields, to receive additional feedback from healthcare providers and patients and to update our ethical investigations on the platform. We will also include clinical and experimental data, to enhance the validity of the aspects highlighted in this paper.
8. Patents
The iManus technology has been disclosed in Maddahi, A.; Choukou, M.-A.; Nassiri, A.M.; Maddahi, Y. A remote training and practicing apparatus and system for upper-limb rehabilitation. United States Patent, US 63/178,735, 2021.
Author Contributions
Conceptualization, A.M., M.S., Y.M. and M.-A.C.; methodology, Y.M. and K.Z., software, A.M. and P.R.D.; validation, all authors; formal analysis, M.-A.C.; investigation, A.M.; resources, Y.M., M.-A.C. and K.Z.; writing—original draft preparation, A.M., T.R.L. and M.S.; writing—review and editing, A.M., T.R.L., M.S., P.R.D., Y.M., M.-A.C. and K.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by multiple grants awarded by the Mathematics of Information Technology and Complex Systems (Mitacs) to the University of Manitoba (IT13630) and Ryerson University (IT24322) in partnership with Tactile Robotics.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank Tactile Robotics Ltd. for providing in-kind sets of iManus for testing and conducting the experiments.
Conflicts of Interest
A.M., M.-A.C. and Y.M. are recognized as inventors of the iManus technology invention. The rest of the authors declare no conflict of interest.
References
- Detsky, A.; Bogoch, I. COVID-19 in Canada. JAMA 2020, 324, 743–744. [Google Scholar] [CrossRef] [PubMed]
- Marx, L.; Smith, M.R. Does Technology Drive History? The Dilemma of Technological Determinism; MIT Press: Cambridge, MA, USA, 1994. [Google Scholar]
- Chandler, D. 1995. Available online: http://www.aber.ac.uk/media/Documents/tecdet/tecdet.html (accessed on 9 August 2021).
- Ryan, D. Robotic Seal Provides Emotional Support for Alzheimer Patients at Vancouver General Hospital Vancouver Sun. 2020. Available online: https://vancouversun.com/news/robotic-seal-provides-emotional-support-for-alzheimers-patients-at-vancouver-general-hospital (accessed on 9 August 2021).
- Kyrarini, M.; Lygerakis, F.; Rajavenkatanarayanan, A.; Sevastopoulos, C.; Nambiappan, H.R.; Chaitanya, K.K.; Babu, A.R.; Mathew, J.; Makedon, F. A Survey of Robots in Healthcare. Technologies 2021, 9, 8. [Google Scholar] [CrossRef]
- Mesbahi, M.E. Human-Robot Interaction Ethics in Sci-Fi Movies: Ethics Are Not ’There’, We Are the Ethics! Springer International Publishing: Berlin, Germany, 2015. [Google Scholar]
- Verrugio, G. The EURON Roboethics Roadmap. In Proceedings of the 2006 6th IEEE-RAS International Conference on Humanoid Robots, HUMANOIDS, Genova, Italy, 4–6 December 2006. [Google Scholar]
- Pagallo, U. When Morals Ain’t Enough: Robots, Ethics, and the Rules of the Law. Minds Mach. 2017, 27, 628–638. [Google Scholar] [CrossRef]
- Bosl, D.; Bode, M. Roboethics and Robotic Governance—A Literature Review and Research Agenda. In Proceedings of the ROBOT 2017: Third Iberian Robotics Conference, Seville, Spain, 22–24 November 2017. [Google Scholar]
- Asimov, I. Runaround: Astounding Science Fiction; Street & Smith Publications: New York, NY, USA, 1942. [Google Scholar]
- Crnkovic, G.D.; Curuklu, B. Robots: Ethical by Design. Ethics Inf. Technol. 2012, 14, 61–71. [Google Scholar] [CrossRef]
- Murphy, R.; Woods, D. Beyond Asimov: The Three Laws of Responsible Robotics. IEEE Intell. Syst. 2009, 24, 14–20. [Google Scholar] [CrossRef]
- Montreal Declaration for a Responsible Development of Artificial Intelligence. In Proceedings of the Forum on the Socially Responsible Development of AI, Montreal, QC, Canada, 2–3 November 2017.
- Danielson, P. Designing a Machine to Learn about the Ethics of Robotics: The N-Reasons Platform. Ethics Inf. Technol. 2010, 12, 251–261. [Google Scholar] [CrossRef]
- US Department of Homeland Security. US Robot Accessory Arm Provides Enhanced Capabilities and Precise Manipulation. 2020. Available online: https://www.hstoday.us/subject-matter-areas/law-enforcement-and-public-safety/u-s-israeli-robot-accessory-arm-provides-enhanced-capabilities-and-precise-manipulation/ (accessed on 9 August 2021).
- NSERC Canadian Robotics Network. Creating the Resilient and Interacting Robots of the Future. 2018. Available online: https://ncrn-rcrc.mcgill.ca/ (accessed on 9 August 2021).
- NSERC Canadian Field Robotics Network. Natural Sciences and Engineering Research Council of Canada. 2018. Available online: https://www.nserc-crsng.gc.ca/Business-Entreprise/How-Comment/Networks-Reseaux/CFRN-RCRT_eng.asp (accessed on 9 August 2021).
- European Commission. Artificial Intelligence, Robotics, and ’Autonomous’ Systems; European Commission: London, UK, 2018. [Google Scholar]
- Thomson, J. The Trolley Problem. Yale Law J. 1985, 94, 1395–1415. [Google Scholar] [CrossRef] [Green Version]
- Kurzweil, R. The Singularity Is Near: When Humans Transcend Biology; Penguin: London, UK, 2005. [Google Scholar]
- Hibbard, B. The Technology of Mind and a New Social Contract. J. Evol. Technol. 2008, 17, 13–22. [Google Scholar]
- Knibbs, K. There’s No Cure for COVID-19 Loneliness, but Robots Can Help. 2020. Available online: https://www.wired.com/story/covid-19-robot-companions/ (accessed on 9 August 2021).
- Camp, J. My Jibo Is Dying and It’s Breaking My Heart. 2019. Available online: https://www.wired.com/story/jibo-is-dying-eulogy (accessed on 9 August 2021).
- Manyika, J.; Lund, S.; Chui, M.; Bughin, J.; Woetzel, J.; Batra, P. Jobs Lost, Jobs Gained: Workforce Transitions in a Time of Automation; McKinsey Global Institute: New York, NY, USA, 2017. [Google Scholar]
- Laut, J.; Porfiri, M.; Raghavan, P. The Present and Future of Robotic Technology in Rehabilitation. Curr. Phys. Med. Rehabil. Rep. 2016, 4, 312–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atashzar, S.F.; Carriere, J.; Tavakoli, M. Review: How Can Intelligent Robots and Smart Mechatronic Modules Facilitate Remote Assessment, Assistance, and Rehabilitation for Isolated Adults with Neuro-Musculoskeletal Conditions? Front. Robot. AI 2020, 8, 610529. [Google Scholar] [CrossRef] [PubMed]
- Kalu, P.; Atkins, J.; Bker, D.; Green, C.B.P. How Do We Assess Microsurgical Skill? Microsurgery 2005, 25, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Homboe, E.; Sherbino, J.; Long, D.; Swing, S.; Frank, J. The Role of Assessment in Competency-Based Medical Education. Med. Teach. 2010, 32, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Maddahi, A.; Choukou, M.-A.; Nassiri, A.M.; Maddahi, Y. A Remote Training and Practicing Apparatus and System for Upper-limb Rehabilitation. U.S. Patent 63/178,735, 2021. [Google Scholar]
- Bloom, B.S.; Engelhart, M.D.; Furst, E.J.; Hill, W.H.; Krathwohl, D.R. Taxonomy of Educational Objectives: The Classification of Educational Goals by a Committee of College and University Examiners; Longmans Publishing: New York, NY, USA, 1956. [Google Scholar]
- Anderson, L.W.; Krathwohl, D.R.; Airasian, P.W.; Cruikshank, K.A.; Mayer, R.; Pintrich, P.; Raths, J.; Wittrock, M.C. A Taxonomy for Learning, Teaching, and Assessing: A Revision of Bloom’s Taxonomy of Educational Objectives; Addison Wesley Longman: Boston, MA, USA, 2001. [Google Scholar]
- McHarg, J.; Kay, E. Designing a Dental Curriculum for the Twenty-First Century. Br. Dent. J. 2009, 207, 493–497. [Google Scholar] [CrossRef]
- Simpson, E. Educational Objectives in the Psychomotor Domain. Behav. Object. Curricul. Dev. Select. Read. Bibliog. 1971, 60, 1–35. [Google Scholar]
- Schneider, G.B.; Cunningham-Ford, M.A.; Johnsen, D.C.; Eckert, M.L.; Mulder, M. Outcomes Mapping: A Method for Dental Schools to Coordinate Learning and Assessment Based on Desired Characteristics of a Graduate. J. Dent. Educ. 2014, 78, 1268–1278. [Google Scholar] [CrossRef] [PubMed]
- Human Rights Council. Thirty-Second Session, Agenda Item 3: Oral Revisions of 30 June, in United Nations General Assembly 10802; Human Rights Council: Geneva, Switzerland, 2016. [Google Scholar]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 

{kind=link}
{kind=link}
{kind=link}


