
A Single Wearable Sensor for Gait Analysis in Parkinson’s Disease: A Preliminary Study

 ,
,  ,
,  ,
, 
 and
and 
Abstract
:1. Introduction
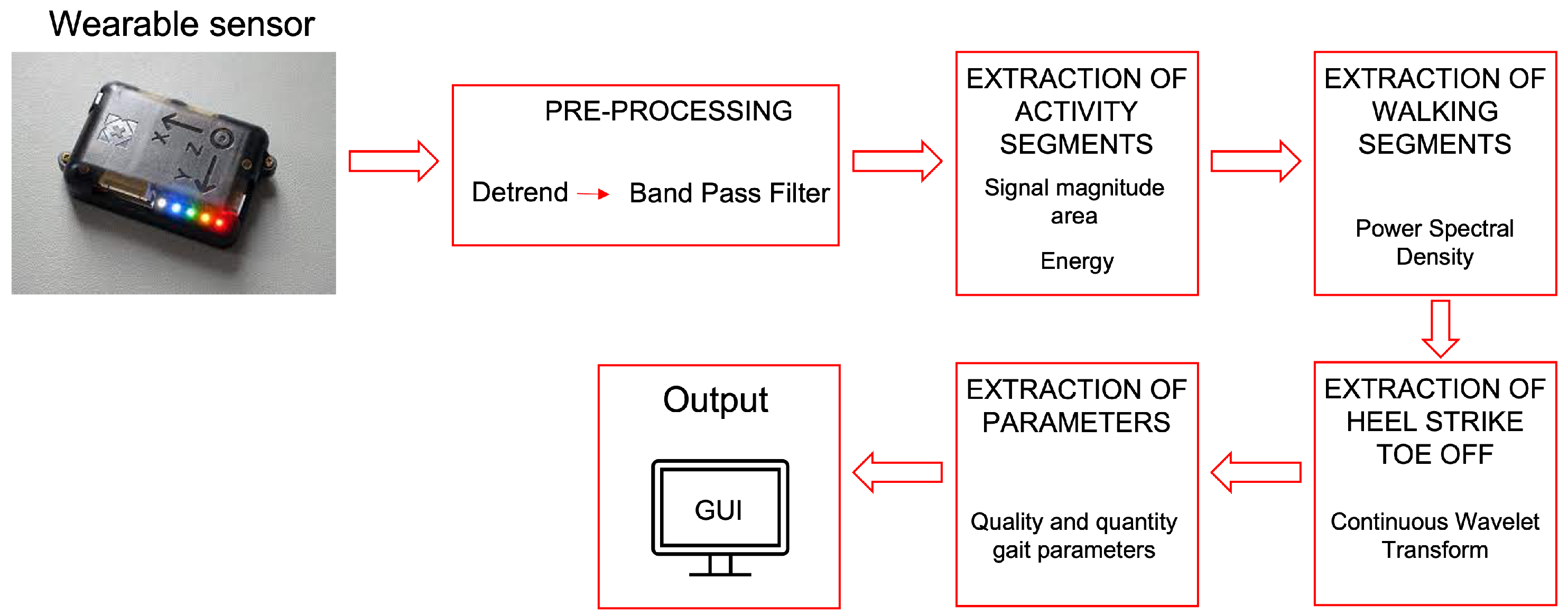
2. Design of the Proposed System
2.1. Pre-Processing
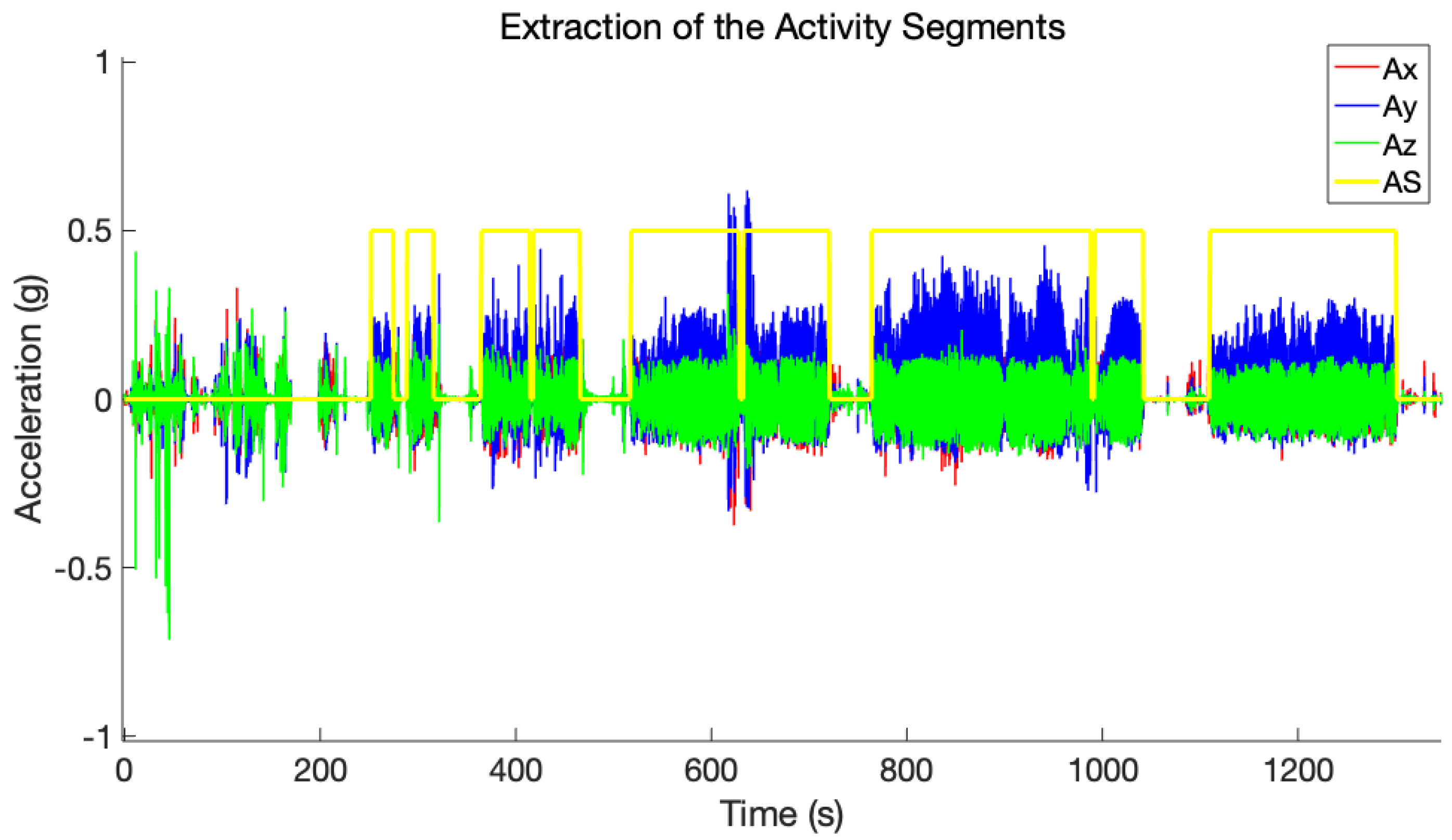
2.2. Extraction of the Activity Segments
2.3. Extraction of Walking Segments
2.4. Extraction of Heel Strike and Toe Off
2.5. Extraction of Parameters
3. Experimental Protocol
- Timed Up and Go (TUG) task: subject started from sitting on a chair, then walked straight on for some meters, completed a turn of 180° around an obstacle, moved straight on for some meters again, and finally sat again on the chair. This activity was performed twice;
- Stair task: subject started from sitting on a chair, then walked straight on for some meters, ascended and descended the stairs four times, walked straight on for some meters again, and finally sat again on the chair;
- Free walking task: subject walked “freely” inside and outside the clinic for 15 min (so experiencing several straight walks, turns, stair ascending and descending activities, and pauses).
Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Botros, A.; Schütz, N.; Camenzind, M.; Urwyler, P.; Bolliger, D.; Vanbellingen, T.; Kistler, R.; Bohlhalter, S.; Müri, R.M.; Mosimann, U.P.; et al. Long-term home-monitoring sensor technology in patients with Parkinson’s disease—Acceptance and adherence. Sensors 2019, 19, 5169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schapira, A.H. Science, medicine, and the future-Parkinson’s disease. Br. Med. J. 1999, 318, 311–314. [Google Scholar] [CrossRef] [PubMed]
- Van Uem, J.M.; Marinus, J.; Canning, C.; van Lummel, R.; Dodel, R.; Liepelt-Scarfone, I.; Berg, D.; Morris, M.E.; Maetzler, W. Health-related quality of life in patients with Parkinson’s disease—A systematic review based on the ICF model. Neurosci. Biobehav. Rev. 2016, 61, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Pardoel, S.; Kofman, J.; Nantel, J.; Lemaire, E.D. Wearable-sensor-based detection and prediction of freezing of gait in Parkinson’s disease: A review. Sensors 2019, 19, 5141. [Google Scholar] [CrossRef] [Green Version]
- Mancini, M.; Bloem, B.R.; Horak, F.B.; Lewis, S.J.; Nieuwboer, A.; Nonnekes, J. Clinical and methodological challenges for assessing freezing of gait: Future perspectives. Mov. Disord. 2019, 34, 783–790. [Google Scholar] [CrossRef]
- Spinsante, S.; Gambi, E. Remote health monitoring for elderly through interactive television. Biomed. Eng. Online 2012, 11, 54. [Google Scholar] [CrossRef] [Green Version]
- Zanela, A.; Schirinzi, T.; Mercuri, N.B.; Stefani, A.; Romagnoli, C.; Annino, G.; Bonaiuto, V.; Cerroni, R. Using a Video Device and a Deep Learning-Based Pose Estimator to Assess Gait Impairment in Neurodegenerative Related Disorders: A Pilot Study. Appl. Sci. 2022, 12, 4642. [Google Scholar] [CrossRef]
- Galperin, I.; Hillel, I.; Del Din, S.; Bekkers, E.M.; Nieuwboer, A.; Abbruzzese, G.; Avanzino, L.; Nieuwhof, F.; Bloem, B.R.; Rochester, L.; et al. Associations between daily-living physical activity and laboratory-based assessments of motor severity in patients with falls and Parkinson’s disease. Park. Relat. Disord. 2019, 62, 85–90. [Google Scholar] [CrossRef]
- Channa, A.; Popescu, N.; Ciobanu, V. Wearable solutions for patients with parkinson’s disease and neurocognitive disorder: A systematic review. Sensors 2020, 20, 2713. [Google Scholar] [CrossRef]
- Albán-Cadena, A.C.; Villalba-Meneses, F.; Pila-Varela, K.O.; Moreno-Calvo, A.; Villalba-Meneses, C.P.; Almeida-Galárraga, D.A. Wearable sensors in the diagnosis and study of Parkinson’s disease symptoms: A systematic review. J. Med. Eng. Technol. 2021, 45, 532–545. [Google Scholar] [CrossRef]
- Sica, M.; Tedesco, S.; Crowe, C.; Kenny, L.; Moore, K.; Timmons, S.; Barton, J.; O’Flynn, B.; Komaris, D.S. Continuous home monitoring of Parkinson’s disease using inertial sensors: A systematic review. PLoS ONE 2021, 16, e0246528. [Google Scholar] [CrossRef] [PubMed]
- Battista, L.; Romaniello, A. A novel device for continuous monitoring of tremor and other motor symptoms. Neurol. Sci. 2018, 39, 1333–1343. [Google Scholar] [CrossRef] [PubMed]
- Heijmans, M.; Habets, J.; Kuijf, M.; Kubben, P.; Herff, C. Evaluation of Parkinson’s disease at home: Predicting tremor from wearable sensors. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 584–587. [Google Scholar]
- McNames, J.; Shah, V.V.; Mancini, M.; Curtze, C.; El-Gohary, M.; Aboy, M.; Carlson-Kuhta, P.; Nutt, J.G.; Horak, F. A two-stage tremor detection algorithm for wearable inertial sensors during normal daily activities. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 2535–2538. [Google Scholar]
- Mancini, M.; Weiss, A.; Herman, T.; Hausdorff, J.M. Turn around freezing: Community-living turning behavior in people with Parkinson’s disease. Front. Neurol. 2018, 9, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Din, S.; Galna, B.; Godfrey, A.; Bekkers, E.M.; Pelosin, E.; Nieuwhof, F.; Mirelman, A.; Hausdorff, J.M.; Rochester, L. Analysis of free-living gait in older adults with and without Parkinson’s disease and with and without a history of falls: Identifying generic and disease-specific characteristics. J. Gerontol. Ser. A 2019, 74, 500–506. [Google Scholar] [CrossRef]
- Greene, B.R.; Premoli, I.; McManus, K.; McGrath, D.; Caulfield, B. Predicting Fall Counts Using Wearable Sensors: A Novel Digital Biomarker for Parkinson’s Disease. Sensors 2021, 22, 54. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Molinero, A.; Pérez-López, C.; Samà, A.; de Mingo, E.; Rodríguez-Martín, D.; Hernández-Vara, J.; Bayés, À.; Moral, A.; Álvarez, R.; Pérez-Martínez, D.A.; et al. A kinematic sensor and algorithm to detect motor fluctuations in Parkinson disease: Validation study under real conditions of use. JMIR Rehabil. Assist. Technol. 2018, 5, e8335. [Google Scholar] [CrossRef]
- Del Din, S.; Godfrey, A.; Galna, B.; Lord, S.; Rochester, L. Free-living gait characteristics in ageing and Parkinson’s disease: Impact of environment and ambulatory bout length. J. Neuroeng. Rehabil. 2016, 13, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Hickey, A.; Del Din, S.; Rochester, L.; Godfrey, A. Detecting free-living steps and walking bouts: Validating an algorithm for macro gait analysis. Physiol. Meas. 2016, 38, N1. [Google Scholar] [CrossRef]
- Pham, M.H.; Elshehabi, M.; Haertner, L.; Del Din, S.; Srulijes, K.; Heger, T.; Synofzik, M.; Hobert, M.A.; Faber, G.S.; Hansen, C.; et al. Validation of a step detection algorithm during straight walking and turning in patients with Parkinson’s disease and older adults using an inertial measurement unit at the lower back. Front. Neurol. 2017, 8, 457. [Google Scholar] [CrossRef] [Green Version]
- Peraza, L.R.; Kinnunen, K.M.; McNaney, R.; Craddock, I.J.; Whone, A.L.; Morgan, C.; Joules, R.; Wolz, R. An Automatic Gait Analysis Pipeline for Wearable Sensors: A Pilot Study in Parkinson’s Disease. Sensors 2021, 21, 8286. [Google Scholar] [CrossRef]
- Muthukrishnan, N.; Abbas, J.J.; Krishnamurthi, N. A wearable sensor system to measure step-based gait parameters for parkinson’s disease rehabilitation. Sensors 2020, 20, 6417. [Google Scholar] [CrossRef] [PubMed]
- Fischer, S.; Ullrich, M.; Küderle, A.; Gaßner, H.; Klucken, J.; Eskofier, B.M.; Kluge, F. Automatic clinical gait test detection from inertial sensor data. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 789–792. [Google Scholar]
- Keloth, S.M.; Arjunan, S.P.; Kumar, D.K. Variance of the gait parameters and fraction of double-support interval for determining the severity of Parkinson’s disease. Appl. Sci. 2020, 10, 577. [Google Scholar] [CrossRef] [Green Version]
- Adams, J.L.; Dinesh, K.; Snyder, C.W.; Xiong, M.; Tarolli, C.G.; Sharma, S.; Dorsey, E.; Sharma, G. A real-world study of wearable sensors in Parkinson’s disease. NPJ Parkinson’s Dis. 2021, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bendig, J.; Wolf, A.S.; Mark, T.; Frank, A.; Mathiebe, J.; Scheibe, M.; Müller, G.; Stahr, M.; Schmitt, J.; Reichmann, H.; et al. Feasibility of a Multimodal Telemedical Intervention for Patients with Parkinson’s Disease—A Pilot Study. J. Clin. Med. 2022, 11, 1074. [Google Scholar] [CrossRef] [PubMed]
- Del Din, S.; Godfrey, A.; Rochester, L. Validation of an accelerometer to quantify a comprehensive battery of gait characteristics in healthy older adults and Parkinson’s disease: Toward clinical and at home use. IEEE J. Biomed. Health Inform. 2015, 20, 838–847. [Google Scholar] [CrossRef]
- Weiss, A.; Brozgol, M.; Dorfman, M.; Herman, T.; Shema, S.; Giladi, N.; Hausdorff, J.M. Does the evaluation of gait quality during daily life provide insight into fall risk? A novel approach using 3-day accelerometer recordings. Neurorehabilit. Neural Repair 2013, 27, 742–752. [Google Scholar] [CrossRef]
- Banos, O.; Galvez, J.M.; Damas, M.; Pomares, H.; Rojas, I. Window size impact in human activity recognition. Sensors 2014, 14, 6474–6499. [Google Scholar] [CrossRef] [Green Version]
- Madgwick, S.O.; Harrison, A.J.; Vaidyanathan, R. Estimation of IMU and MARG orientation using a gradient descent algorithm. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; pp. 1–7. [Google Scholar]
- Pierleoni, P.; Belli, A.; Maurizi, L.; Palma, L.; Pernini, L.; Paniccia, M.; Valenti, S. A wearable fall detector for elderly people based on AHRS and barometric sensor. IEEE Sens. J. 2016, 16, 6733–6744. [Google Scholar] [CrossRef]
- McCamley, J.; Donati, M.; Grimpampi, E.; Mazza, C. An enhanced estimate of initial contact and final contact instants of time using lower trunk inertial sensor data. Gait Posture 2012, 36, 316–318. [Google Scholar] [CrossRef]
- Doğan, N.Ö. Bland–Altman analysis: A paradigm to understand correlation and agreement. Turk. J. Emerg. Med. 2018, 18, 139–141. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Unit | Axis |
|---|---|---|
| Total number of walks | n | AP |
| Total walking duration | % | AP |
| Total number of steps | n | AP |
| Median walking bout duration | s | AP |
| Median number of steps for bouts | n | AP |
| Cadence | steps/minute | AP |
| Parameters | Units | Axes | |
|---|---|---|---|
| Frequency measures | Dominant frequency | Hz | V, AP, ML |
| Amplitude of dominant frequency | PSD | V, AP, ML | |
| Width of dominant frequency | Hz | V, AP, ML | |
| Slope of dominant frequency | PSD/Hz | V, AP, ML | |
| Harmonic ratio | # | V, AP, ML | |
| Temporal measures | Step time | s | AP |
| Stride time | s | AP | |
| Stance time | s | AP | |
| Swing time | s | AP | |
| Double support time | s | AP | |
| Single support time | s | AP | |
| Step time variability | s | AP | |
| Stride time variability | s | AP | |
| Stance time variability | s | AP | |
| Double support time variability | s | AP | |
| Step regularity | # | V, AP, ML | |
| Stride regularity | # | V, AP, ML | |
| Step time asymmetry | s | V, AP, ML | |
| Stride time asymmetry | s | V, AP, ML | |
| Double support time asymmetry | s | V, AP, ML |
| Walking | Duration of Walking [s] | Number of Steps from Video Recording | Number of Steps Extracted from the Algorithm | Algorithm’s Percentage Error [%] | Sensitivity [%] | Specificity [%] |
|---|---|---|---|---|---|---|
| 1 | 21.59 | 37 | 37 | 0 | 98.60 | 100 |
| 2 | 10.78 | 19 | 19 | 0 | ||
| 3 | 21.50 | 39 | 39 | 0 | ||
| 4 | 23.69 | 40 | 40 | 0 | ||
| 5 | 81.66 | 148 | 146 | 1.35 | ||
| 6 | 75.16 | 132 | 130 | 0.52 | ||
| 7 | 193.10 | 346 | 340 | 1.73 | ||
| 8 | 39.96 | 68 | 67 | 1.47 | ||
| 9 | 185.46 | 310 | 305 | 1.61 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pierleoni, P.; Raggiunto, S.; Belli, A.; Paniccia, M.; Bazgir, O.; Palma, L. A Single Wearable Sensor for Gait Analysis in Parkinson’s Disease: A Preliminary Study. Appl. Sci. 2022, 12, 5486. https://doi.org/10.3390/app12115486
Pierleoni P, Raggiunto S, Belli A, Paniccia M, Bazgir O, Palma L. A Single Wearable Sensor for Gait Analysis in Parkinson’s Disease: A Preliminary Study. Applied Sciences. 2022; 12(11):5486. https://doi.org/10.3390/app12115486
Chicago/Turabian StylePierleoni, Paola, Sara Raggiunto, Alberto Belli, Michele Paniccia, Omid Bazgir, and Lorenzo Palma. 2022. "A Single Wearable Sensor for Gait Analysis in Parkinson’s Disease: A Preliminary Study" Applied Sciences 12, no. 11: 5486. https://doi.org/10.3390/app12115486
APA StylePierleoni, P., Raggiunto, S., Belli, A., Paniccia, M., Bazgir, O., & Palma, L. (2022). A Single Wearable Sensor for Gait Analysis in Parkinson’s Disease: A Preliminary Study. Applied Sciences, 12(11), 5486. https://doi.org/10.3390/app12115486