
Reservoir-Vascular Tubes Network for Self-Healing Concrete: Performance Analysis by Acoustic Emission, Digital Image Correlation and Ultrasound Velocity

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Research Significance
3. Materials and Methods
3.1. Concrete Beams
3.2. Healing Networks
3.3. Healing Agent
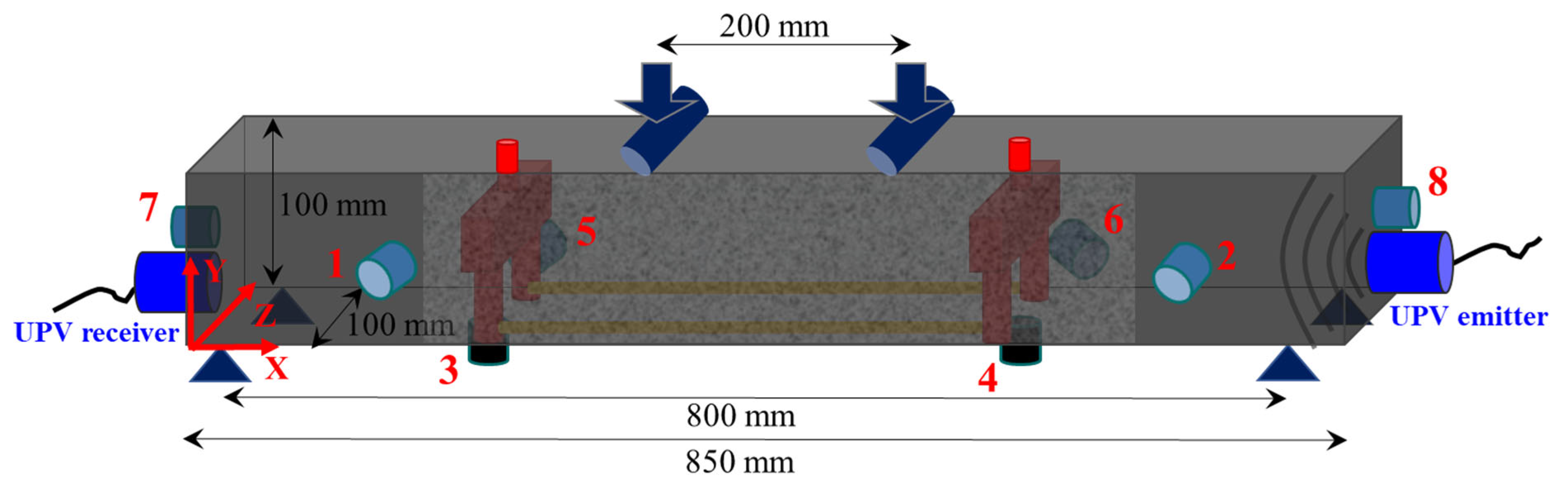
3.4. Four-Point Bending Test
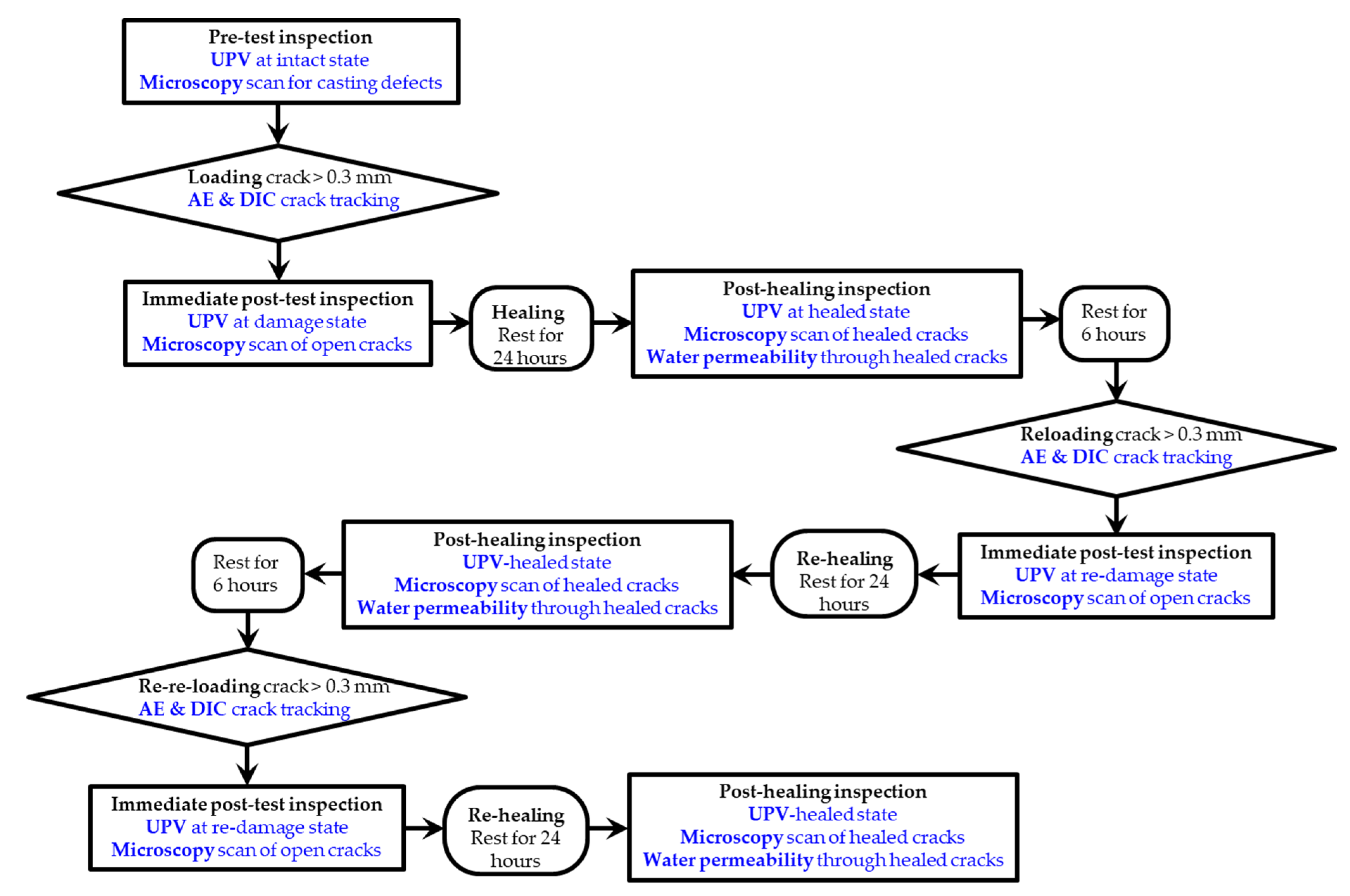
3.5. Inspection
4. Results
4.1. Mechanical Tests
- -
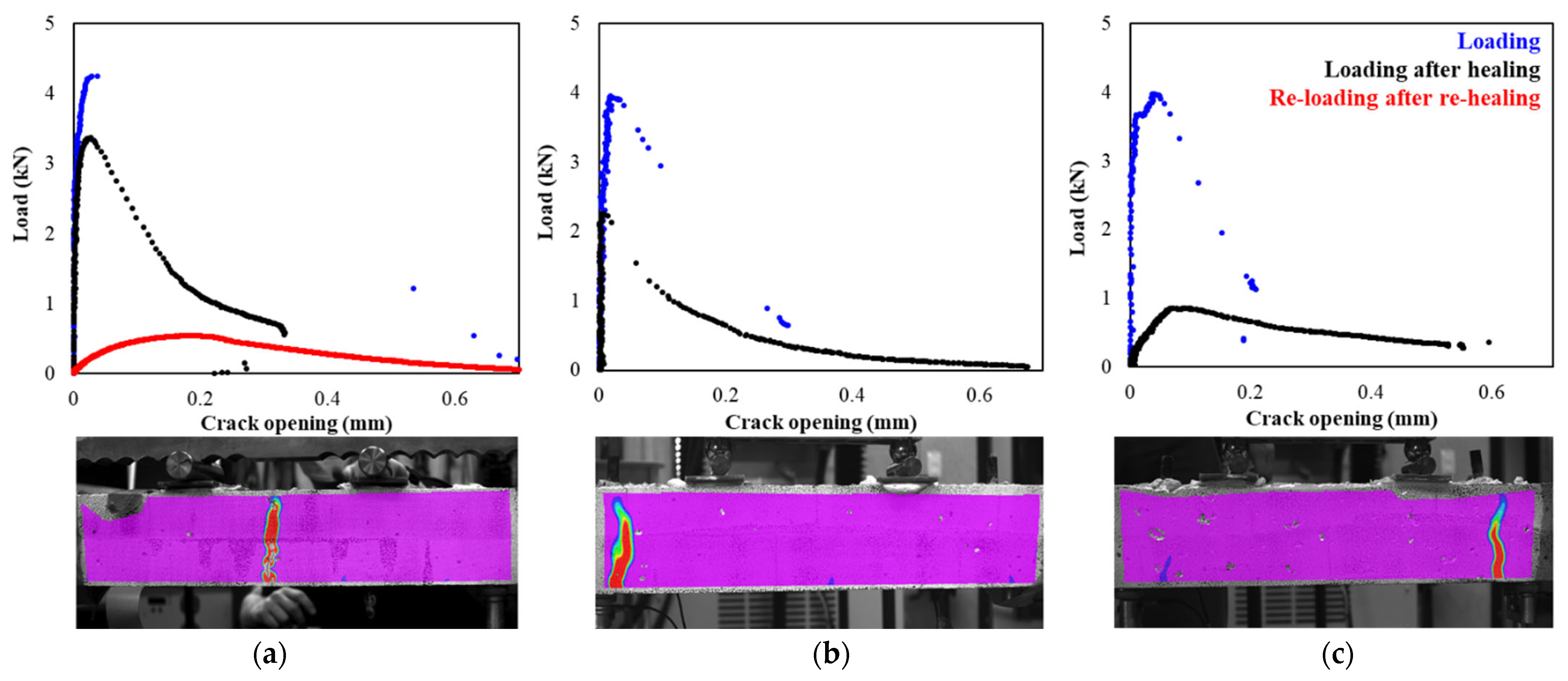
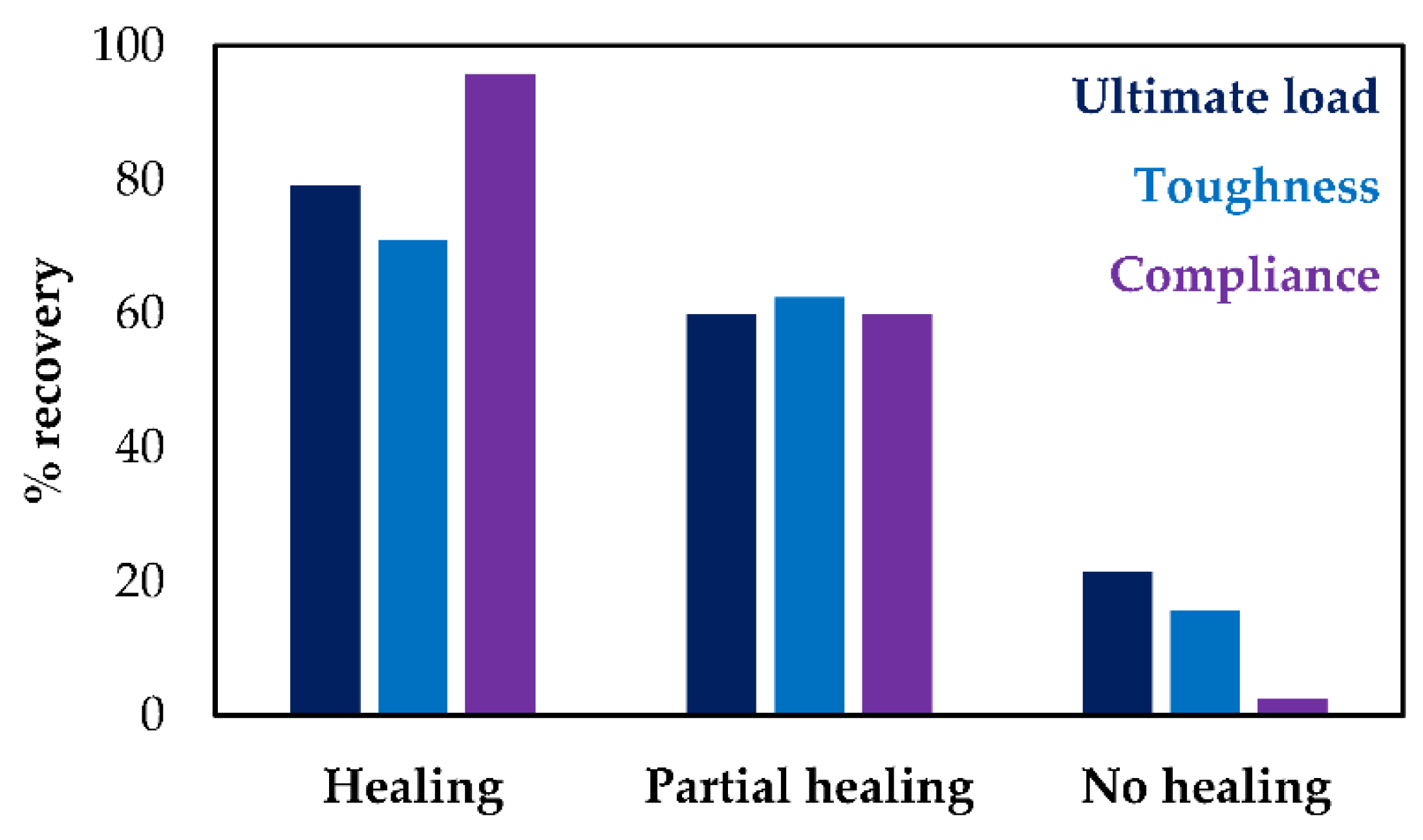
- Full crack healing (Beam 4): The early compliance was fully recovered (96%) and the ultimate load reached after healing was up to 80% of the original value. The initial crack reopened after healing; however, significant resistance to fracture was foreseen (Figure 5a), as proven by the significant toughness recovery (71%, Figure 6).
- -
- Partial healing (Beam 11): Figure 5b demonstrates the case of a beam at which partial healing and moderate restoration was reported (i.e., recovery of mechanical features by approximately 60%, see Figure 6). In this case, unexpectedly the crack was located at the limits of the bending zone. This phenomenon was reported for the majority of beams that carried 3D printed PET reservoirs. It was shown that the healing system design impacted both healing efficacy and crack formation. Since the PET reservoirs were standing only 30 mm away from the end of the limits of the bending zone, the cracks were attracted by the boundary effect at the reservoir-concrete interface. It should be noted that a clear distinction between the fully and partially healed samples could not be made with confidence; however, this classification was chosen to underline the healing potentials of the systems under design.
- -
- No healing (Beam 9): In a few cases, the crack was formed out of the healing zone; therefore, the agent delivery could not be obtained. This case reports the limited recovery (Figure 6). Indicatively, the ultimate load at re-loading stage was equal to the load reached at the end of the loading cycle. Additionally, considering the limited toughness measured after healing and the absence of compliance recovery, this case will be considered further in this study as the unhealed scenario.
4.2. Healing Inspection
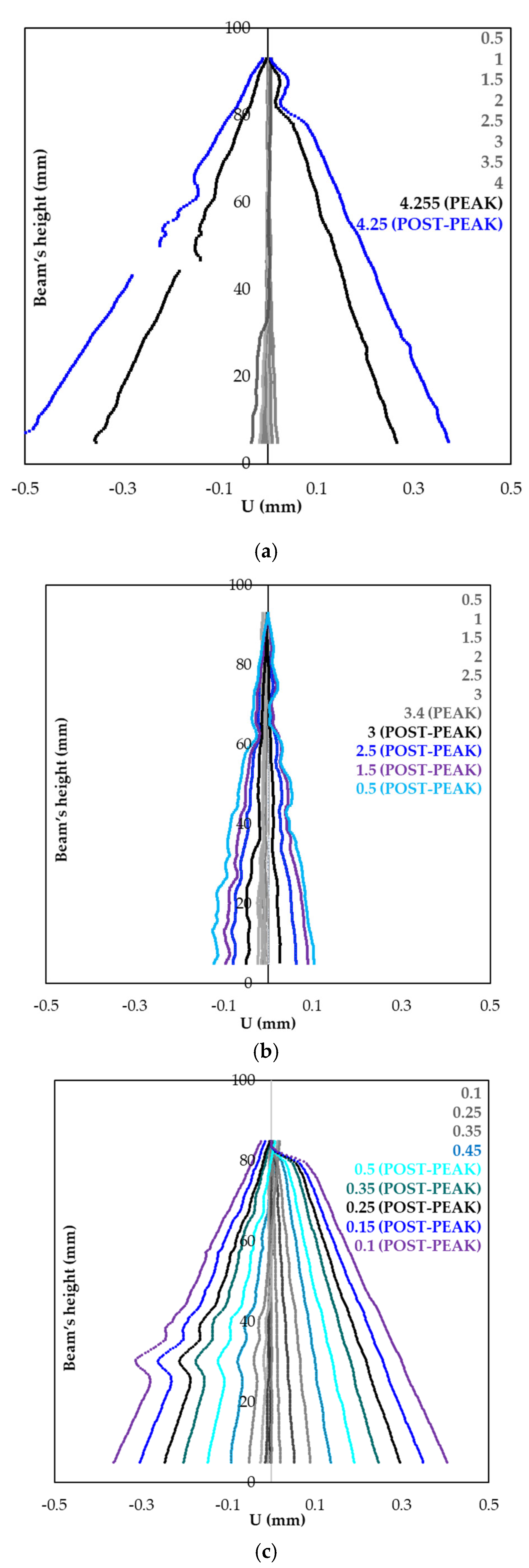
4.3. Post-Softening Fracture after Healing
- -
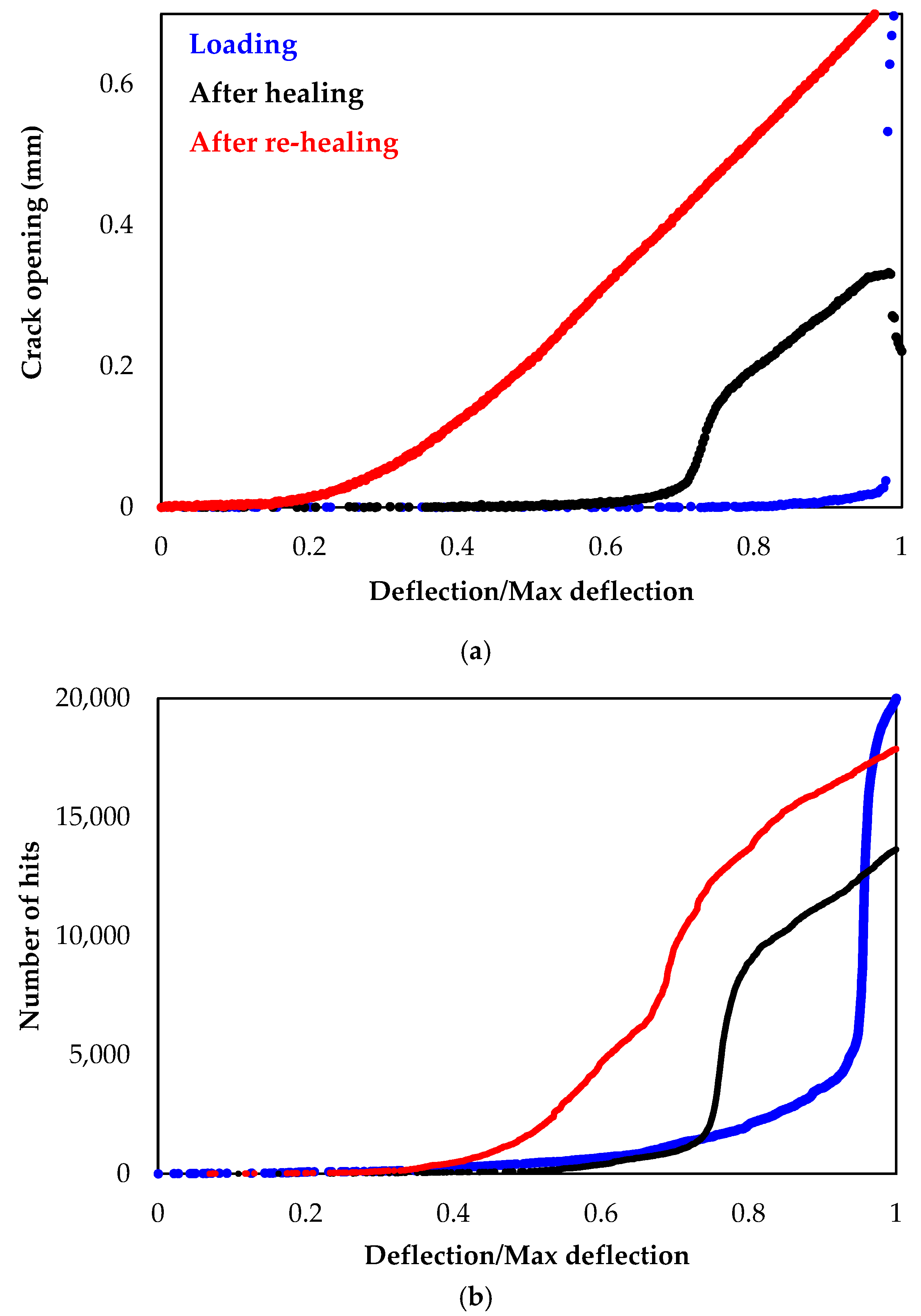
- The crack initially forms in a brittle mode and opens instantly (Figure 10a).
- -
- After healing, the cracked zone is restored and as a result, the crack widening is limited and occurs in a stable mode at the post-softening stage (Figure 10b).
- -
- After re-healing and since any additional healing agent cannot be delivered, the crack freely re-opens. At the post-softening stage, the crack is up to four times larger compared to the healed state (Figure 10c).
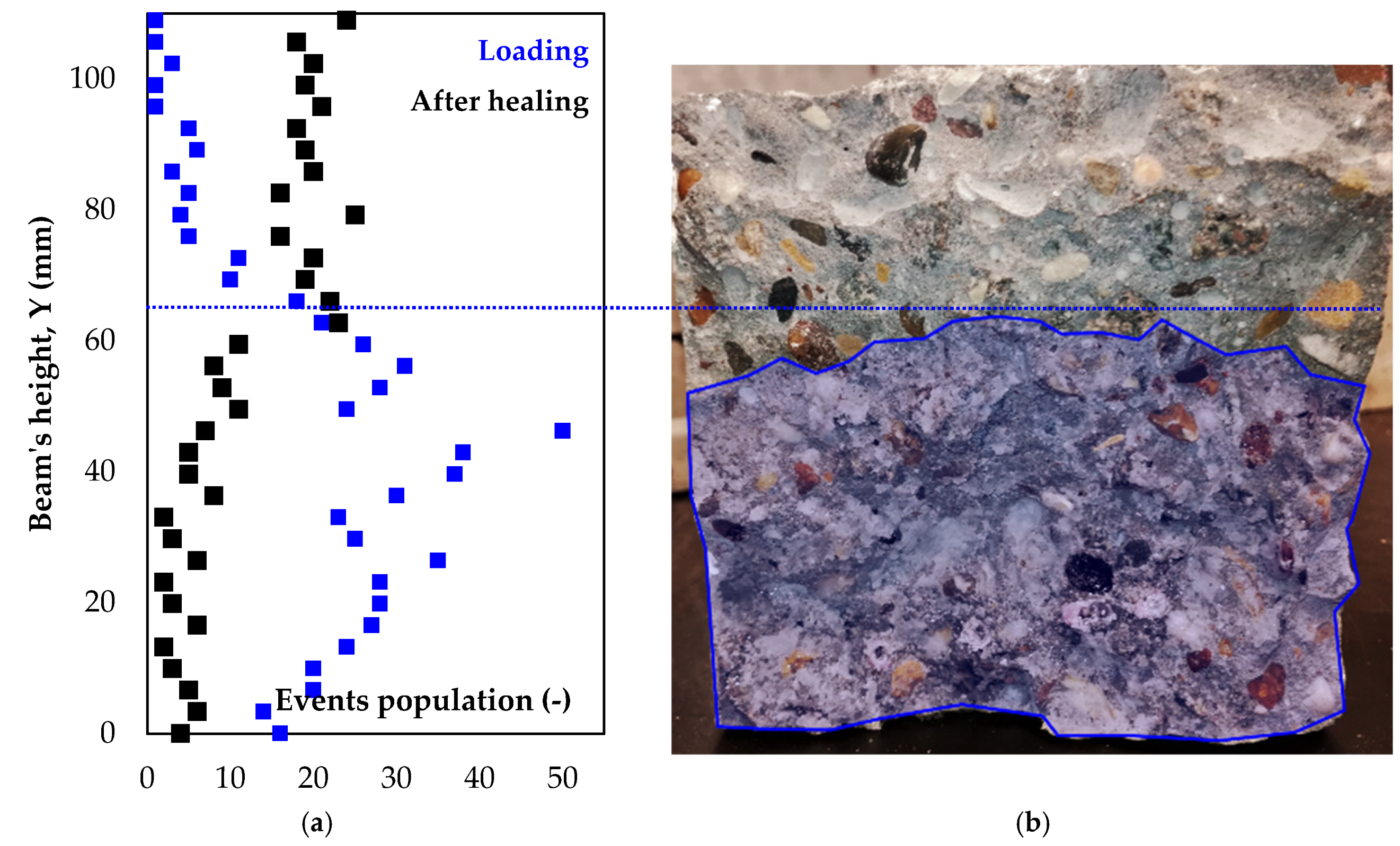
4.4. AE as a Tool to Track Crack Extension after Healing
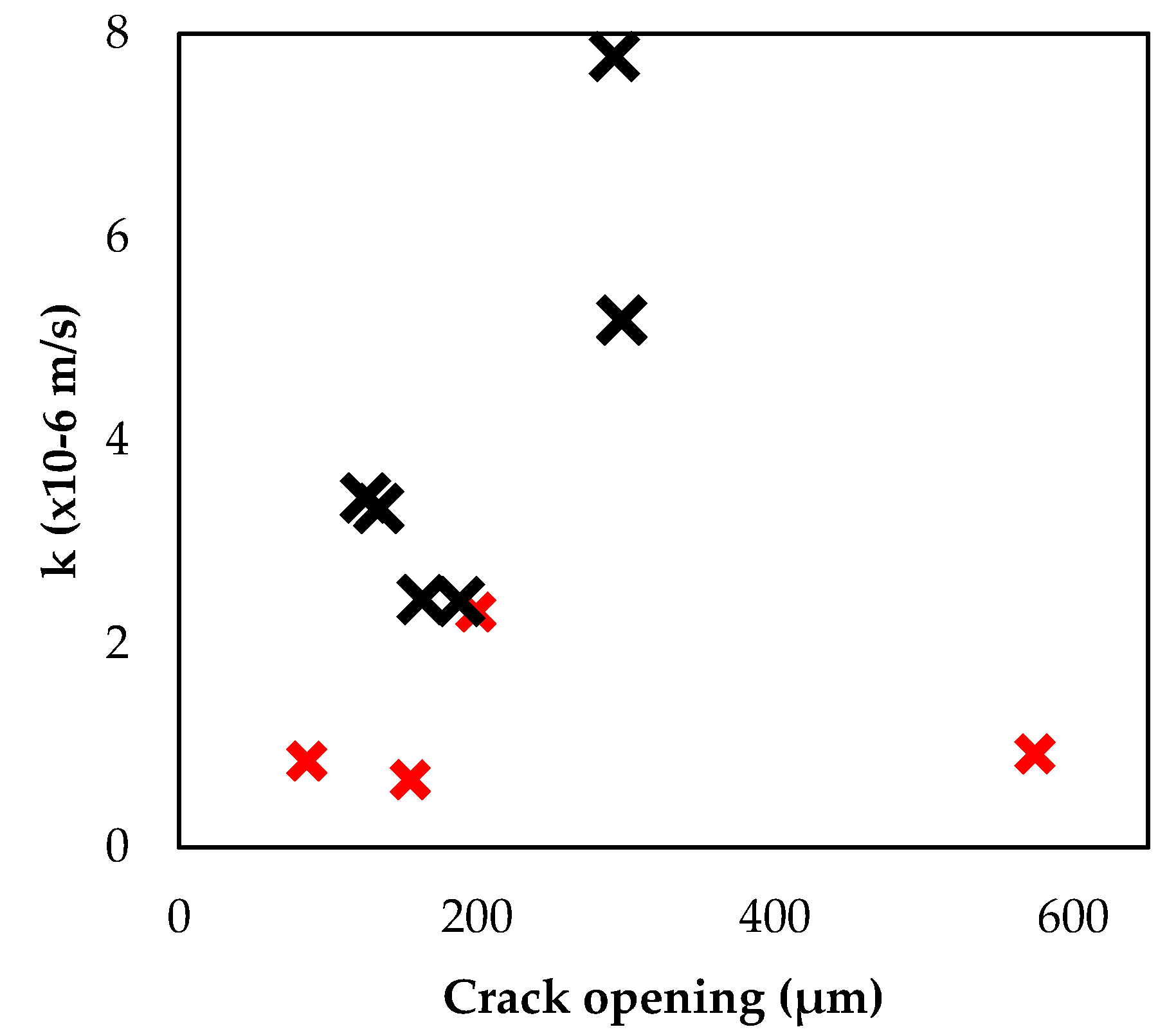
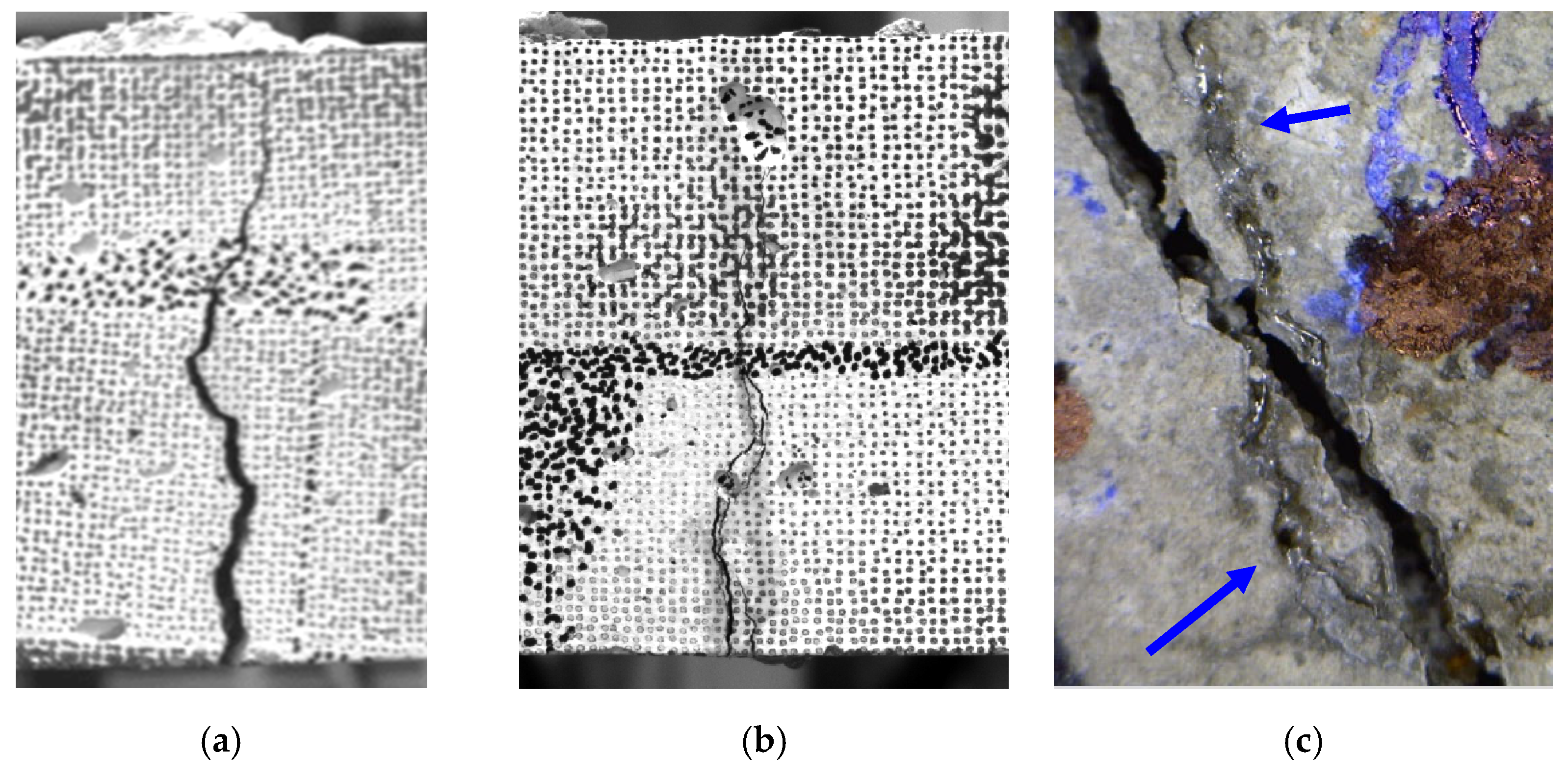
4.5. Effect of Crack Morphology on Healing
5. Discussion
5.1. Cracking Deviation Due to Reservoirs
5.2. Casting Irregularities Due to Vascular Network
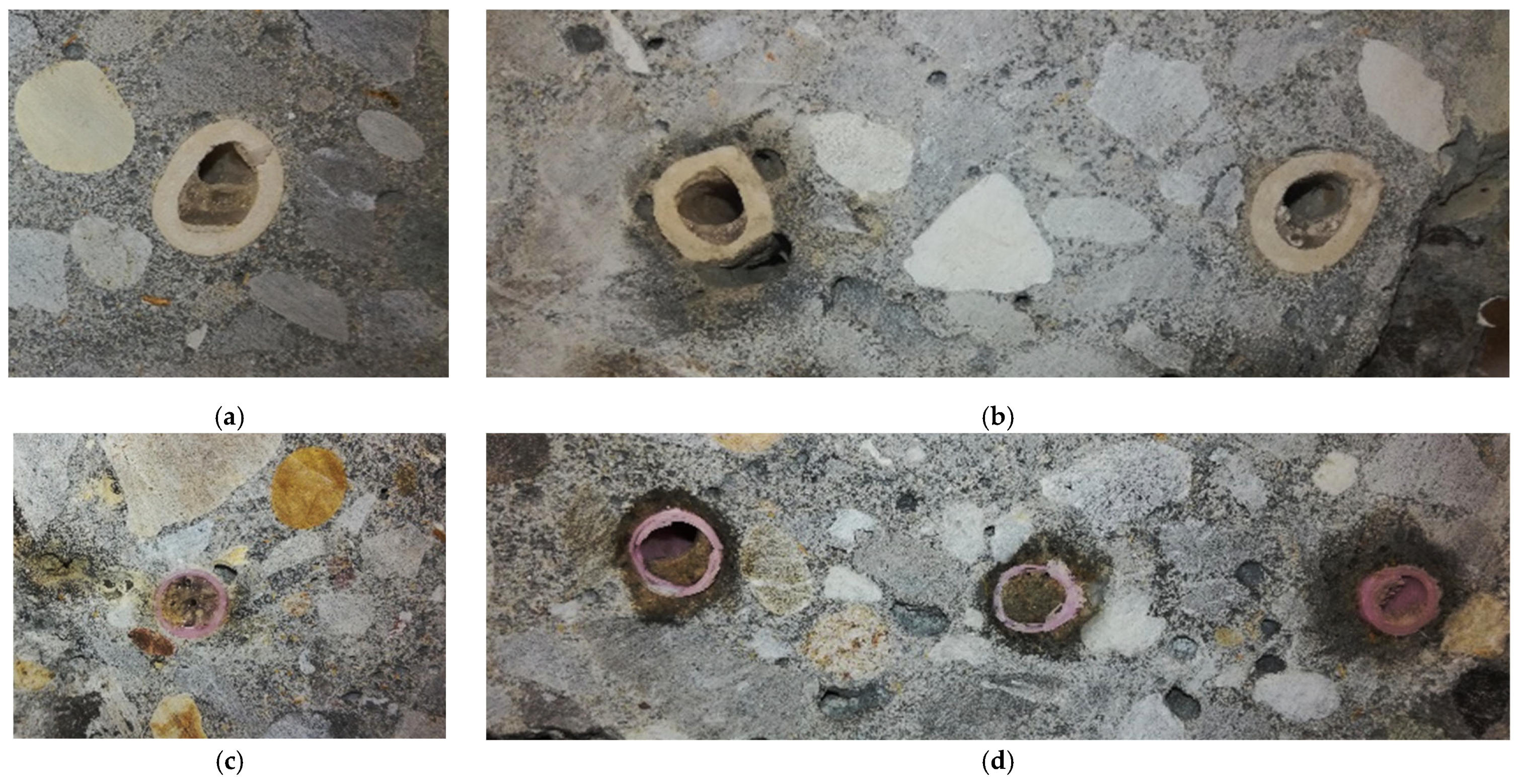
5.3. Tubes’ Thrombosis and Cleansing after Healing
6. Conclusions
- -
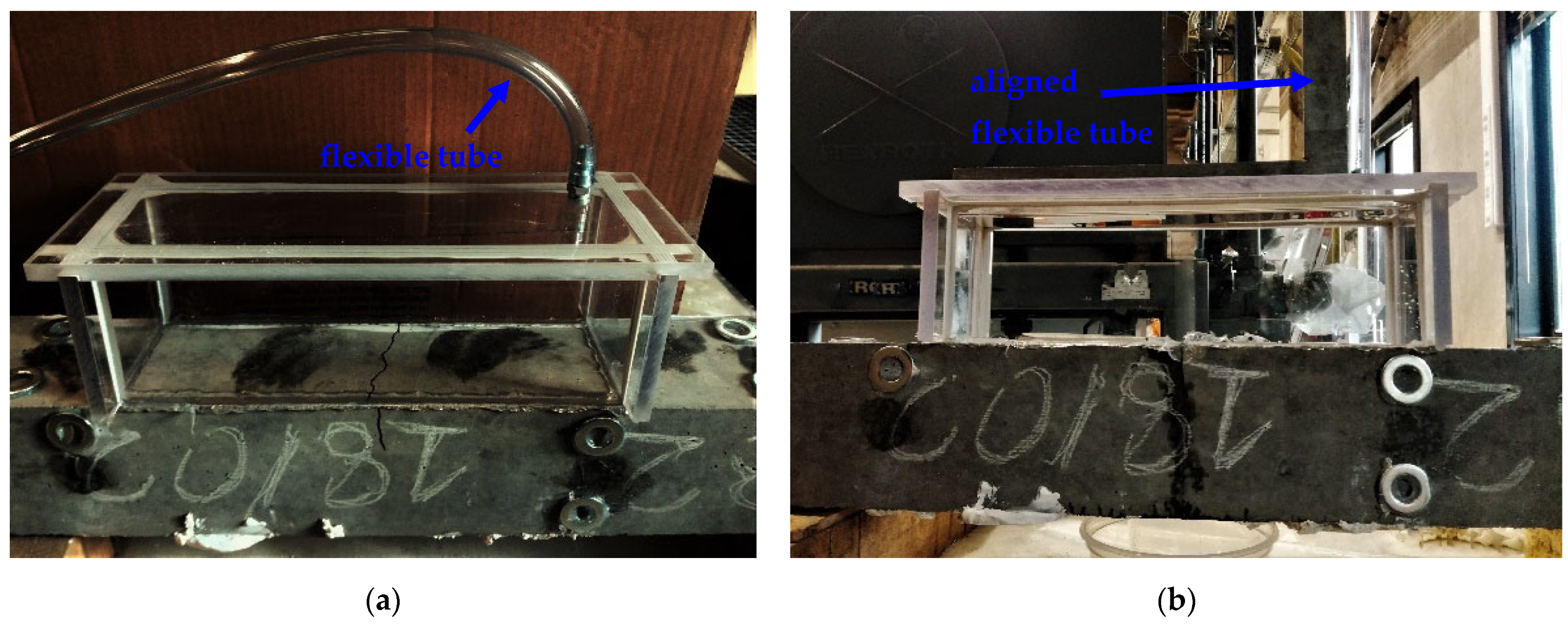
- The detrimental impact of embedded bulk agent reservoirs is reported since under bending the cracks deviate from the middle bending zone towards the reservoir sections and failure occurs at the concrete-reservoir interface. The incompatibility of concrete with a stiff polymer reservoir suggests that alternative agent delivery systems should be explored. The use of a thin flexible plastic inlet/outlet tube system proved its efficacy and it is recommended for future designs. The position of the connection tubes into the beam and relative to the vascular networks should be also revised.
- -
- The 3D printed polymer network appears equally effective compared to the conventional ceramic tubes since in both cases the tubes break instantly upon cracking and the subsequently healing agent is effectively released and distributed into the cracks.
- -
- The healing agent viscosity should be modified (reaching lower viscosity) since the tubes are only partially cleaned by pressurized air after the healing intervention. Future work should explore the tightness of the 3D printed vascular networks as it is observed that cement paste can penetrate through the tubes during concrete casting. Clogging phenomena should be eliminated in the future by printing polymers with a higher thickness.
- -
- Repeatable healing could not be reached due to the tubes’ internal clogging and to re-opening of the same crack or of a crack in its vicinity at the reloading cycles. The complex fracture process and dense cracks network should be taken into account in future works in order to design a network that performs optimally under concrete service loads.
- -
- Effective crack healing is described by a combination of two fracture phenomena: (1) the healed crack section elastically deforms under load, building great strength and toughness recovery; and (2) as the crack forms, the fracture gradually propagates along the crack contributing to great post-softening.
- -
- AE and DIC complementarily contribute to the online monitoring of crack formation and reopening after healing. The use of DIC for a precise crack opening analysis appears crucial for the accurate assessment of healing efficacy. The AE hits distribution indicates the transition of damage from brittle to pseudo-ductile for a healed crack. The AE localization analysis can identify the active cracking zones even after healing. In an upcoming study dedicated to the AE as a tool for damage and healing identification, both the damage mode shift and the post-healing crack kinetics will be associated to the AE wave features’ trends and variations during testing.
- -
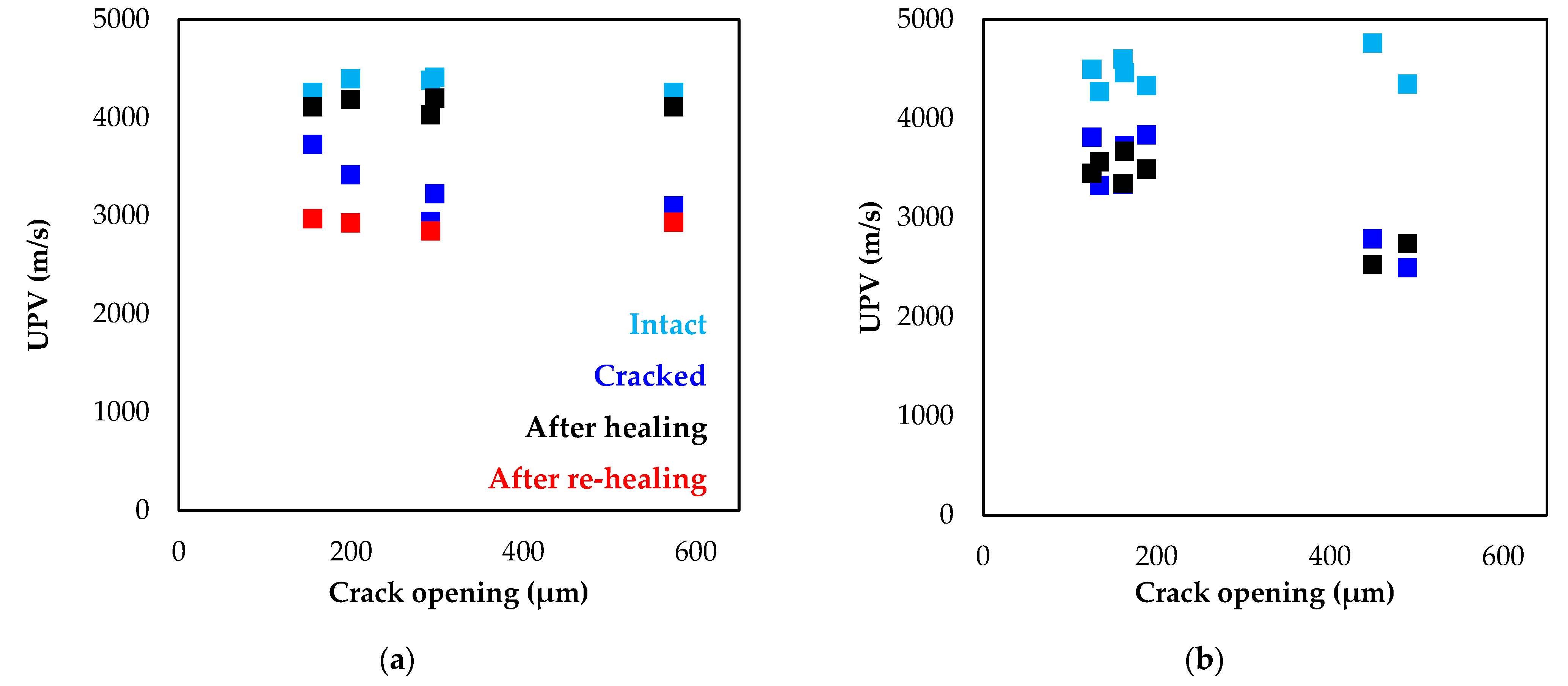
- UPV inspection before and after cracking and healing intervention provides direct information on the damage state of the concrete and can pinpoint the crack recovery cases.
- -
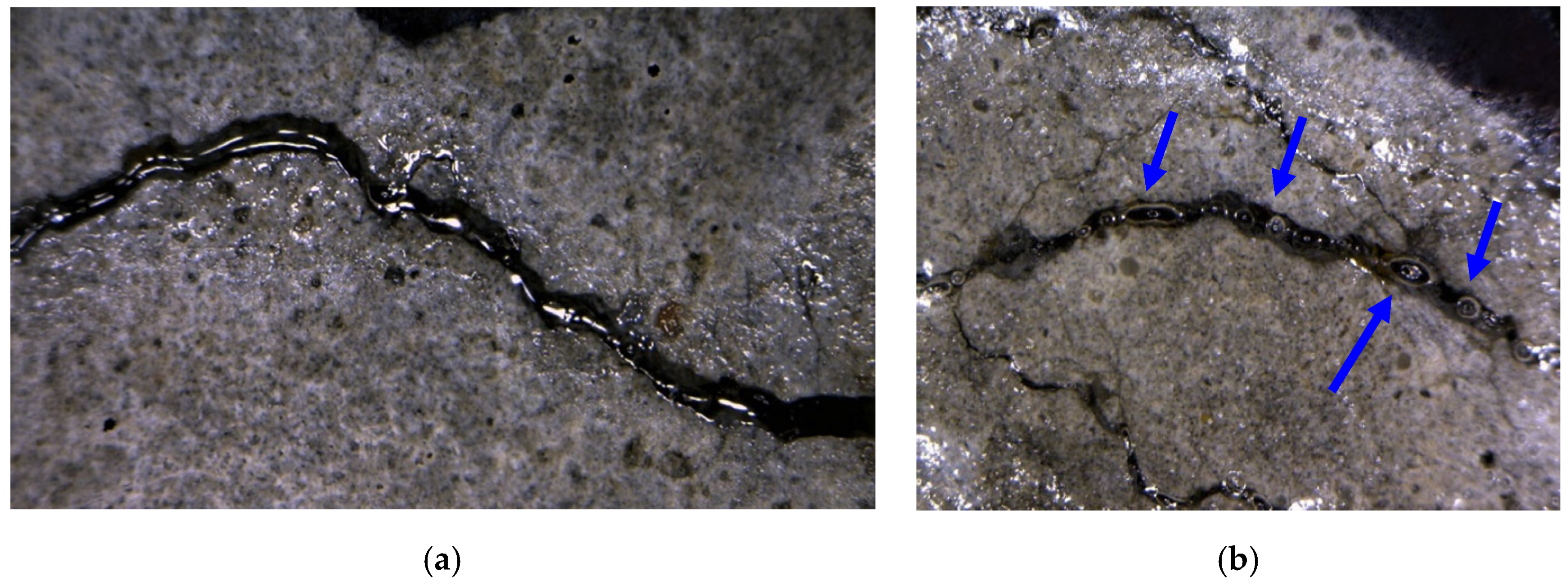
- Optical microscopy after each test cycle effectively detects the crack filling by agent and visual inspection at post-testing reports on the tubes clogging, cleansing issues and failures of the network.
Author Contributions
Funding

Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsangouri, E. A decade of research on self-healing concrete. In Sustainable Construction and Building Materials; IntechOpen: London, UK, 2018; pp. 21–36. [Google Scholar]
- Davies, R.; Teall, O.; Pilegis, M.; Kanellopoulos, A.; Sharma, T.; Jefferson, A.; Gardner, D.; Al-Tabbaa, A.; Paine, K.; Lark, R. Large scale application of self-healing concrete: Design, construction, and testing. Front. Mater. 2018, 2018, 51. [Google Scholar] [CrossRef] [Green Version]
- Papaioannou, S.; Amenta, M.; Kilikoglou, V.; Gournis, D.; Karatasios, I. Synthesis and integration of cement-based capsules modified with sodium silicate for developing self-healing cements. Constr. Build. Mater. 2022, 316, 125803. [Google Scholar] [CrossRef]
- Shields, Y.; De Belie, N.; Jefferson, A.; Van Tittelboom, K. A review of vascular networks for self-healing applications. Smart Mater. Struct. 2021, 30, 063001. [Google Scholar] [CrossRef]
- Tsangouri, E.; Lelon, J.; Minnebo, P.; Shiotani, T.; Van Tittelboom, K.; De Belie, N.; Aggelis, D.G.; Van Hemelrijck, D. Feasibility study on real-scale, self-healing concrete slab by developing a smart capsules network and assessed by a plethora of advanced monitoring techniques. Constr. Build. Mater. 2019, 228, 116780. [Google Scholar] [CrossRef]
- Minnebo, P.; Thierens, G.; De Valck, G.; Van Tittelboom, K.; De Belie, N.; Van Hemelrijck, D.; Tsangouri, E. A novel design of autonomously healed concrete: Towards a vascular healing network. Materials 2017, 10, 49. [Google Scholar] [CrossRef] [PubMed]
- Dry, C. Matrix cracking repair and filling using active and passive modes for smart timed release of chemicals from fibers into cement matrices. Smart Mater. Struct. 1994, 32, 118. [Google Scholar] [CrossRef]
- Van Tittelboom, K.; Tsangouri, E.; Van Hemelrijck, D.; De Belie, N. The efficiency of self-healing concrete using alternative manufacturing procedures and more realistic crack patterns. Cem. Concr. Compos. 2015, 57, 142–152. [Google Scholar] [CrossRef]
- Huang, H.; Ye, G.; Shui, Z. Feasibility of self-healing in cementitious materials–By using capsules or a vascular system? Constr. Build. Mater. 2014, 63, 108–118. [Google Scholar] [CrossRef]
- Hossain, M.; Sultana, R.; Patwary, M.; Khunga, N.; Sharma, P.; Shaker, S.J. Self-healing concrete for sustainable buildings. A review. Environ. Chem. Lett. 2022, 20, 1265–1273. [Google Scholar] [CrossRef]
- Shields, Y.; Van Mullem, T.; De Belie, N.; Van Tittelboom, K. An Investigation of Suitable Healing Agents for Vascular-Based Self-Healing in Cementitious Materials. Sustainability 2021, 13, 12948. [Google Scholar] [CrossRef]
- Li, Z.; de Souza, L.R.; Litina, C.; Markaki, A.E.; Al-Tabbaa, A. A novel biomimetic design of a 3D vascular structure for self-healing in cementitious materials using Murray’s law. Mater. Des. 2020, 190, 108572. [Google Scholar] [CrossRef]
- Selvarajoo, T.; Davies, R.E.; Freeman, B.L.; Jefferson, A.D. Mechanical response of a vascular self-healing cementitious material system under varying loading conditions. Constr. Build. Mater. 2020, 254, 119245. [Google Scholar] [CrossRef]
- Selvarajoo, T.; Davies, R.E.; Gardner, D.R.; Freeman, B.L.; Jefferson, A.D. Characterisation of a vascular self-healing cementitious material system: Flow and curing properties. Constr. Build. Mater. 2020, 245, 118332. [Google Scholar] [CrossRef]
- Jefferson, A.; Selvarajoo, T.; Freeman, B.; Davies, R. An experimental and numerical study on vascular self-healing cementitious materials. In Proceedings of the Concrete Solutions- 7th International Conference on Concrete Repair, Cluj, Romania, 30 September–2 October 2019. [Google Scholar]
- De Nardi, C.; Gardner, D.; Jefferson, A.J. Development of 3D printed networks in self-healing concrete. Materials 2020, 13, 1328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanellopoulos, A. Self-Healing Construction Materials: Fundamentals, Monitoring and Large-Scale Applications; Springer Nature: Berlin, Germany, 2022. [Google Scholar]
- De Belie, N.; Gruyaert, E.; Al-Tabbaa, A.; Antonaci, P.; Baera, C.; Bajare, D.; Darquennes, A.; Davies, R.; Ferrara, L.; Jefferson, T.; et al. A review of self-healing concrete for damage management of structures. Adv. Mater. Interfaces 2018, 5, 1800074. [Google Scholar] [CrossRef]
- Tsangouri, E.; Karaiskos, G.; Deramaeker, A.; Van Hemelrijck, D.; Aggelis, D.G. Assessment of acoustic emission localization accuracy on damaged and healed concrete. Constr. Build. Mater. 2016, 129, 163–171. [Google Scholar] [CrossRef] [Green Version]
- Hsu, N.N. Acoustic Emissions Simulator. U.S. Patent 4018084 A, 19 April 1977. [Google Scholar]
- Hou, S.; Li, K.; Wu, Z.; Li, F.; Shi, C. Quantitative evaluation on self-healing capacity of cracked concrete by water permeability test–A review. Cem. Concr. Compos. 2022, 127, 104404. [Google Scholar] [CrossRef]
- Wang, J.; Mignon, A.; Trenson, G.; Van Vlierberghe, S.; Boon, N.; De Belie, N. A chitosan-based pH-responsive hydrogel for encapsulation of bacteria for self-sealing concrete. Cem. Concr. Compos. 2018, 93, 309–322. [Google Scholar] [CrossRef]
- Van Mullem, T.; Gruyaert, E.; Debbaut, B.; Caspeele, R.; De Belie, N. Novel active crack width control technique to reduce the variation on water permeability results for self-healing concrete. Constr. Build. Mater. 2019, 203, 541–551. [Google Scholar] [CrossRef]
- Zhang, F.; Pahlavan, L.; Yang, Y. Evaluation of acoustic emission source localization accuracy in concrete structures. Struct. Health Monit. 2020, 19, 2063–2074. [Google Scholar] [CrossRef]
- Carpinteri, A.; Lacidogna, G.; Niccolini, G. Critical behaviour in concrete structures and damage localization by acoustic emission. Key Eng. Mater. 2006, 312, 305–310. [Google Scholar] [CrossRef]
- Zhang, X.; Qian, C. Effects of the crack geometric features on the probability density of spherical healing agent particles in concrete. Constr. Build. Mater. 2021, 301, 124083. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Polyurethane (PU) Healing Agent | Concrete | ||
|---|---|---|---|
| Polymerization Trigger | Moisture | Component | Weight (kg/m3) |
| Curing time (20 °C) | 1–5 min | CEM I 52.5 N | 300 |
| Density (20 °C) | 1.12 g/cm3 | Sand 0/4 | 670 |
| Viscosity (20 °C) | 4200 mPa·s | Aggregate 2/8 | 490 |
| Shelf life | 6 months | Aggregate 8/16 | 790 |
| Cost | 14 EUR/lt | Water | 150 |
| Beam | Healing Network | Supply System |
|---|---|---|
| 1 to 5 | 3D printed PLA tubes | Flexible PVC inlet/outlet tubes |
| 6 to 10 | 3D printed PLA tubes | 3D printed PET reservoirs |
| 11 to 15 | Ceramic tubes | 3D printed PET reservoirs |
| Beam | X (mm) | Y (mm) | Z (mm) |
|---|---|---|---|
| 1 | 150 | 0 | 50 |
| 2 | 700 | 0 | 50 |
| 3 | 200 | 50 | 0 |
| 4 | 650 | 50 | 0 |
| 5 | 250 | 100 | 50 |
| 6 | 600 | 100 | 50 |
| 7 | 0 | 50 | 75 |
| 8 | 850 | 50 | 75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsangouri, E.; Van Loo, C.; Shields, Y.; De Belie, N.; Van Tittelboom, K.; Aggelis, D.G. Reservoir-Vascular Tubes Network for Self-Healing Concrete: Performance Analysis by Acoustic Emission, Digital Image Correlation and Ultrasound Velocity. Appl. Sci. 2022, 12, 4821. https://doi.org/10.3390/app12104821
Tsangouri E, Van Loo C, Shields Y, De Belie N, Van Tittelboom K, Aggelis DG. Reservoir-Vascular Tubes Network for Self-Healing Concrete: Performance Analysis by Acoustic Emission, Digital Image Correlation and Ultrasound Velocity. Applied Sciences. 2022; 12(10):4821. https://doi.org/10.3390/app12104821
Chicago/Turabian StyleTsangouri, Eleni, Corentin Van Loo, Yasmina Shields, Nele De Belie, Kim Van Tittelboom, and Dimitrios G. Aggelis. 2022. "Reservoir-Vascular Tubes Network for Self-Healing Concrete: Performance Analysis by Acoustic Emission, Digital Image Correlation and Ultrasound Velocity" Applied Sciences 12, no. 10: 4821. https://doi.org/10.3390/app12104821
APA StyleTsangouri, E., Van Loo, C., Shields, Y., De Belie, N., Van Tittelboom, K., & Aggelis, D. G. (2022). Reservoir-Vascular Tubes Network for Self-Healing Concrete: Performance Analysis by Acoustic Emission, Digital Image Correlation and Ultrasound Velocity. Applied Sciences, 12(10), 4821. https://doi.org/10.3390/app12104821