
Clinical versus Dental Laboratory Survey Regarding Modern Fixed Implant Supported Prosthetic in Romania



Abstract
Featured Application
Abstract
1. Introduction
2. Materials and Methods
3. Results
- Respondents’ demographic data the demographic information collected in the respondents’ lot were age, sex and years of experience.
- Data regarding the design and impression technique of the fixed restoration with implant support
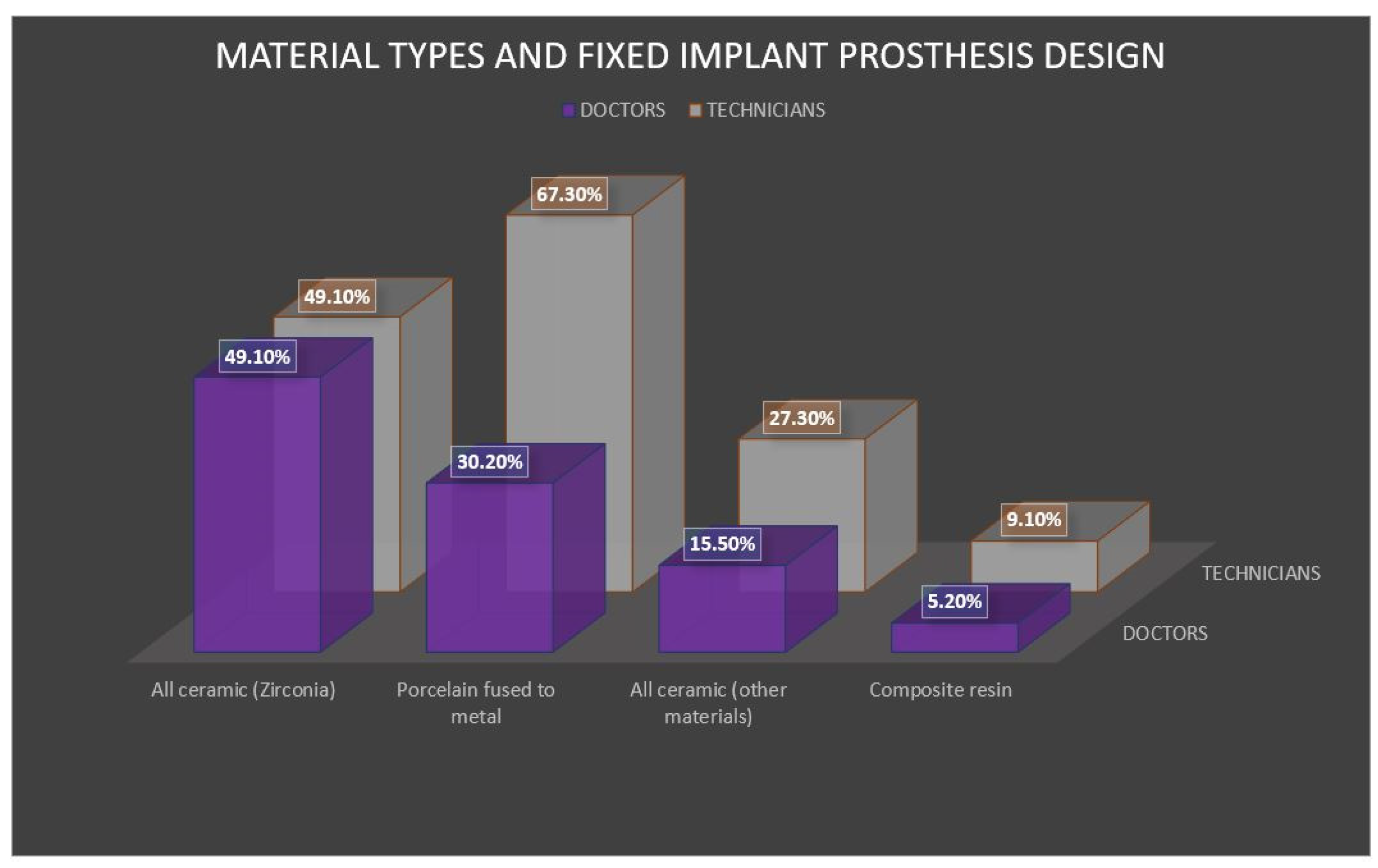
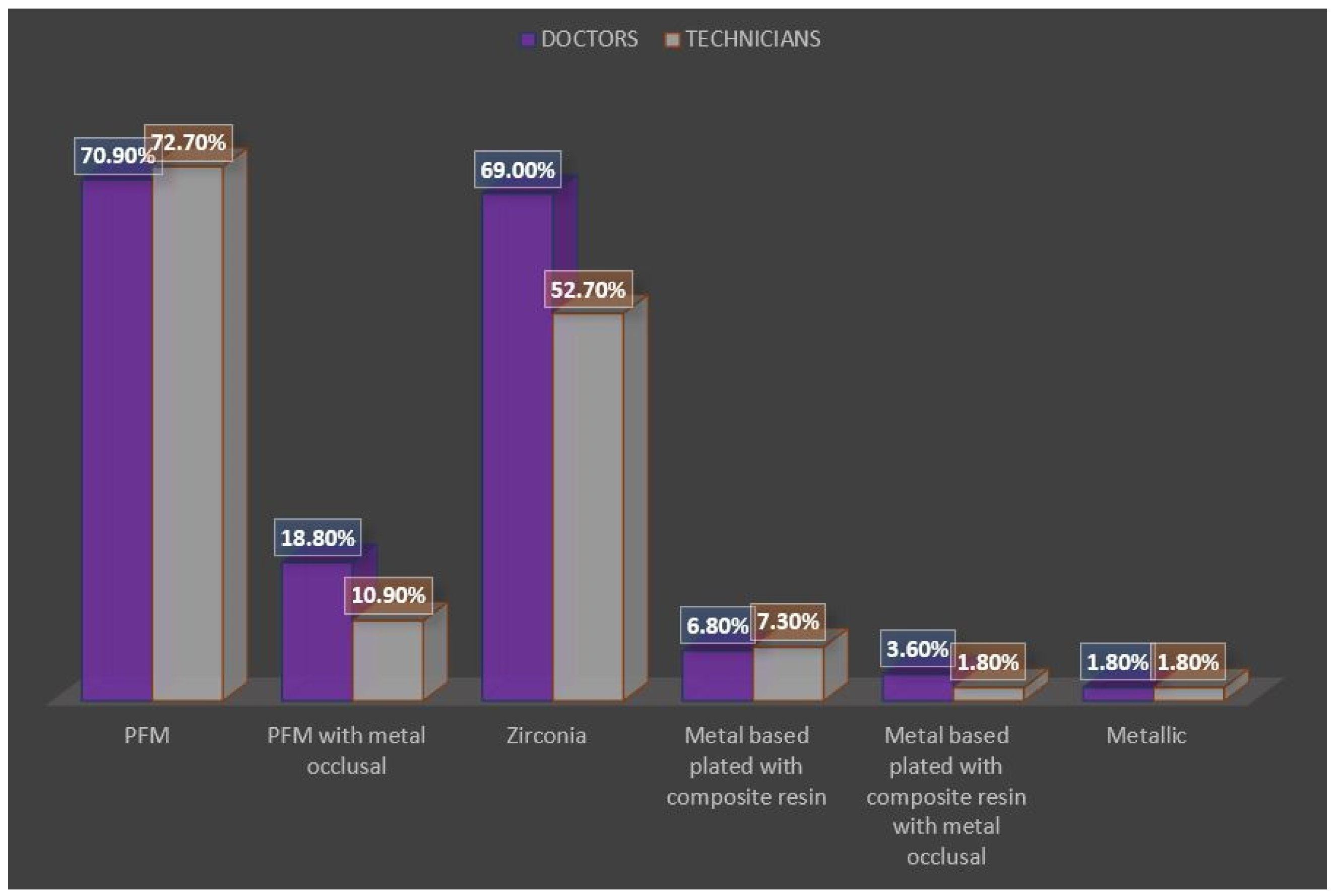
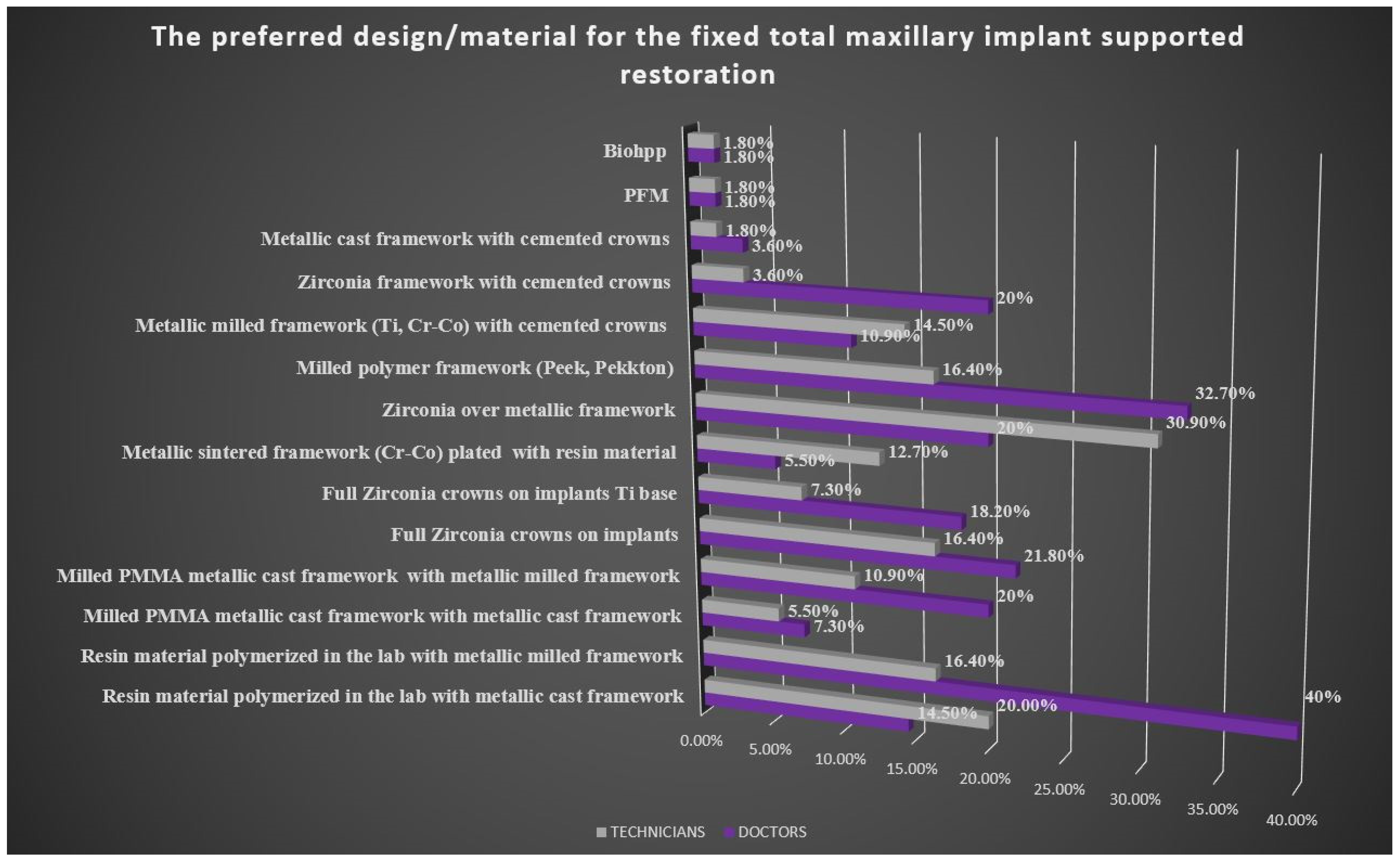
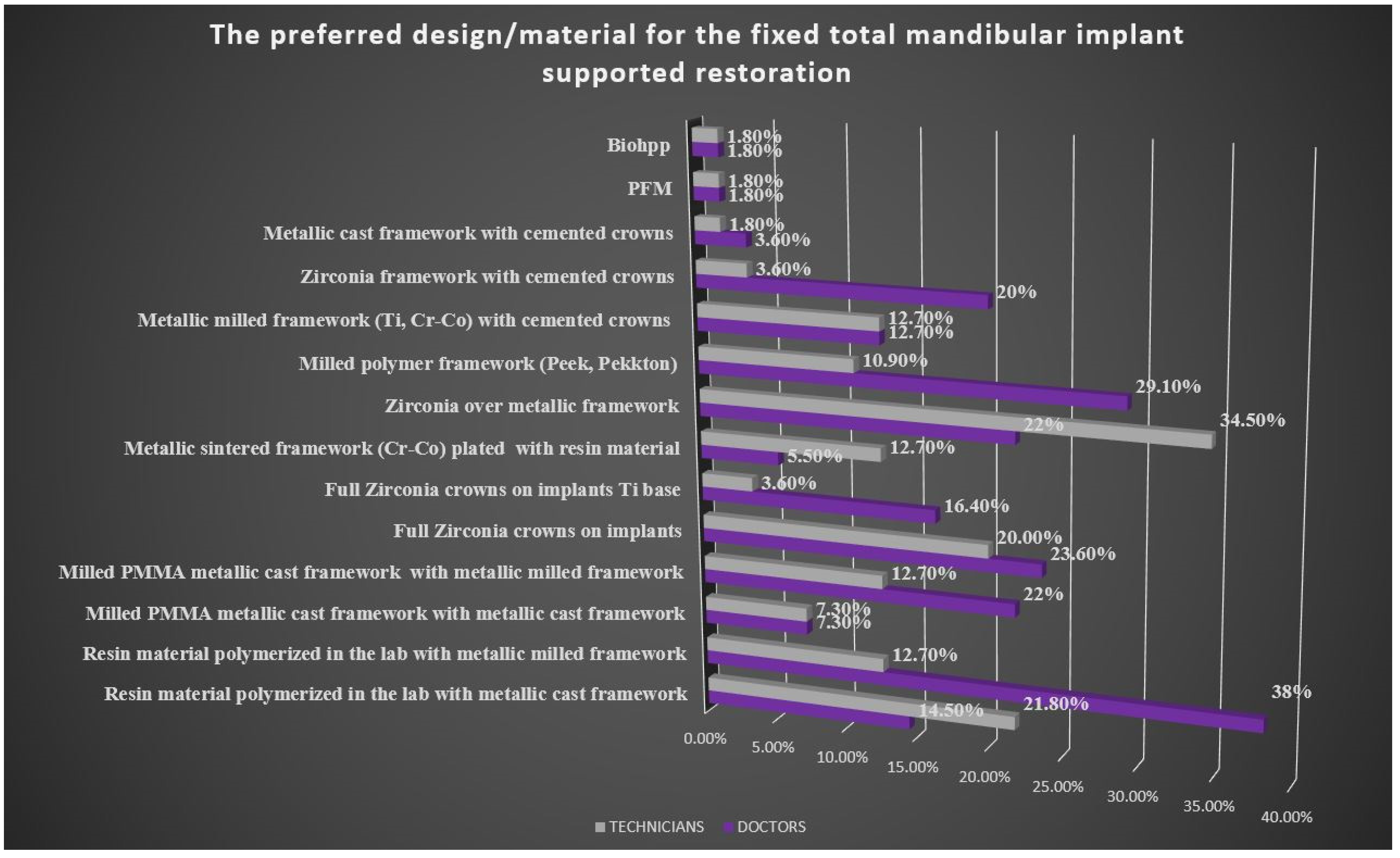
- Type of material and fixed implant prosthesis design
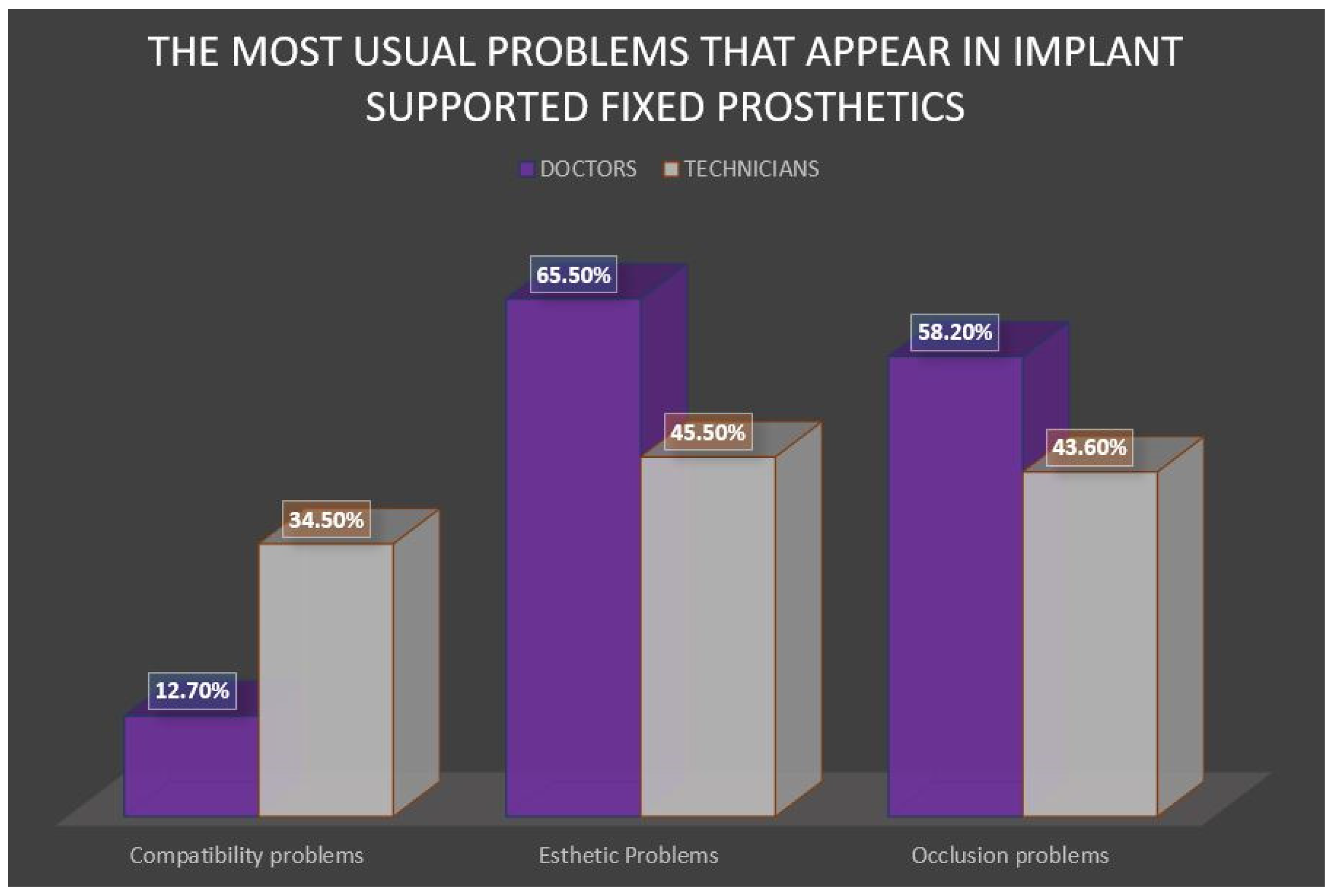
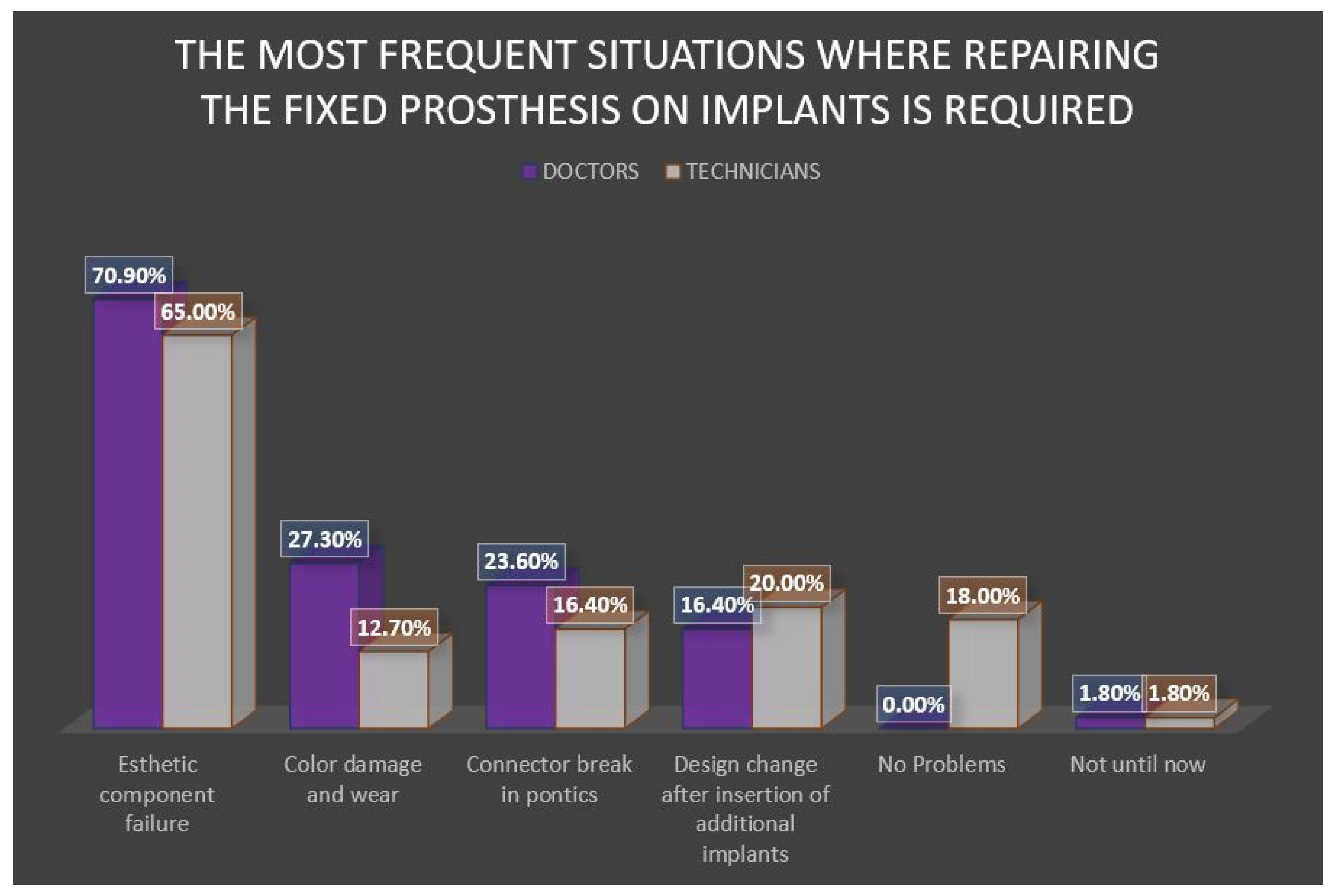
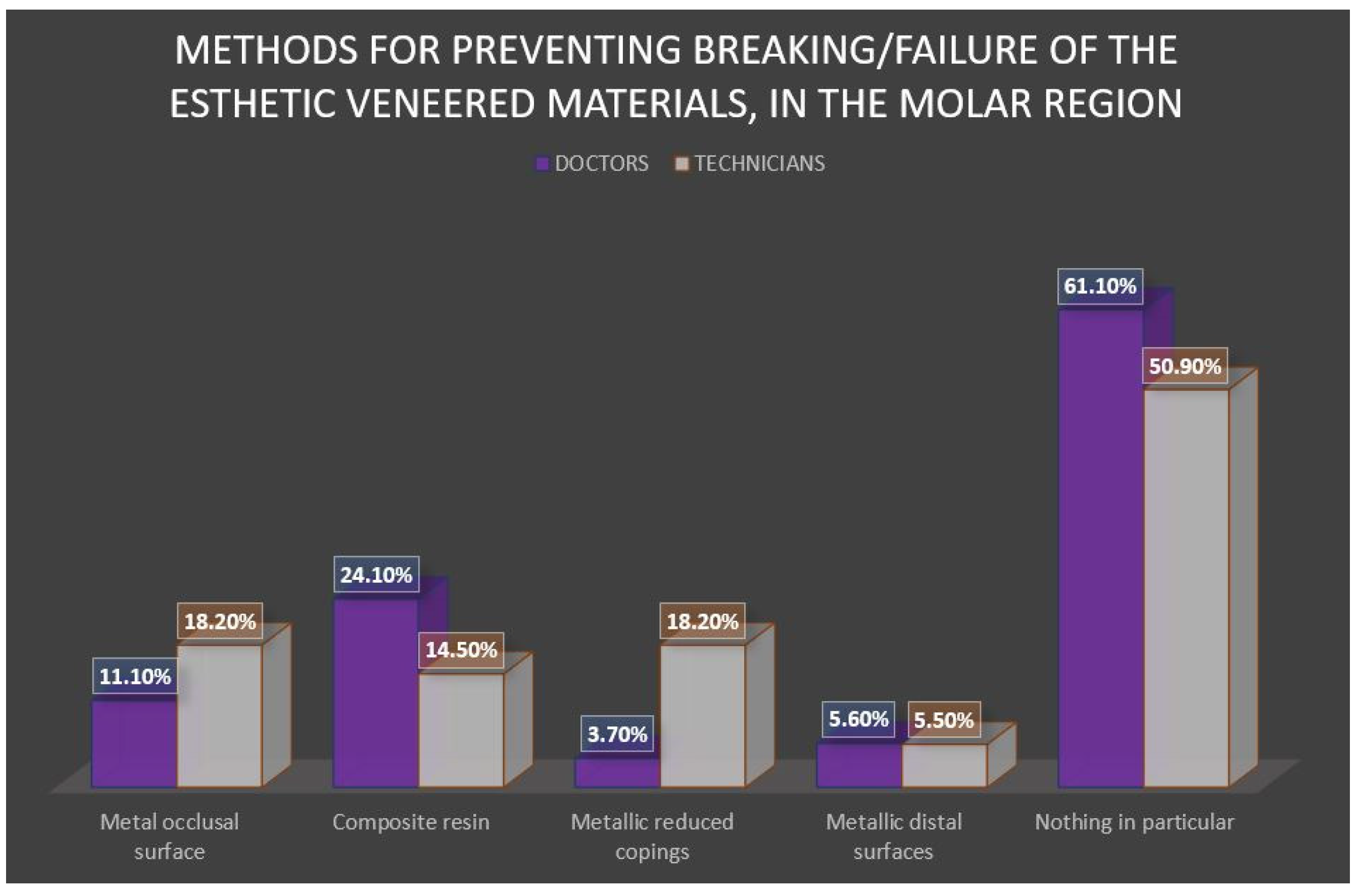
- Frequent complications in fixed prosthodontics with implant support
- The statistical analysis of correlation between the answers to pairs of the questions from the two questionnaires (doctors-technicians)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Schnitman, P.A.; Wöhrle, P.S.; Rubenstein, J.E.; DaSilva, J.D.; Wang, N.H. Ten-year results for Brånemark implants immediately loaded with fixed prostheses at implant placement. Int. J. Oral Maxillofac. Implant. 1997, 12, 1–14. [Google Scholar]
- Schwartz-Arad, D.; Chaushu, G. Full-arch restoration of the jaw with fixed ceramometal prosthesis. Int. J. Oral Maxillofac. Implant. 1998, 13, 819–825. [Google Scholar]
- Kumar, V.V.; Sagheb, K.; Kämmerer, P.W.; Al-Nawas, B.; Wagner, W. Retrospective clinical study of marginal bone level changes with two different screw-implant types: Comparison between tissue level (TE) and bone level (BL) implant. Int. J. Oral Maxillofac. Implant. 2014, 13, 259–266. [Google Scholar] [CrossRef]
- Lazzara, R.J.; Porter, S.S. Platform switching: A new concept in implant dentistry for controlling postrestorative crestal bone levels. Int. J. Periodontics Restor. Dent. 2006, 26, 9–17. [Google Scholar]
- Gallucci, G.O.; Papaspyridakos, P.; Ashy, L.M.; Kim, G.E.; Brady, N.J.; Weber, H.P.; Dent, M. Clinical accuracy outcomes of closed-tray and open-tray implant impression techniques for partially edentulous patients. Int. J. Prosthodont. 2011, 24, 469–472. [Google Scholar] [PubMed]
- Al-Otaibi, H.N.; Almutairi, A.; Alfarraj, J.; Algesadi, W. The effect of torque application technique on screw preload of implant-supported prostheses. Int. J. Oral Maxillofac. Implant. 2017, 32, 259–263. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Lang, N.P. Prosthetic treatment planning on the basis of scientific evidence. J. Oral Rehabil. 2008, 35 (Suppl. 1), 72–79. [Google Scholar] [CrossRef]
- Schoenbaum, T.R.; Guichet, D.L.; Jang, J.Y.; Kim, Y.K.; Wadhwani, C.P. Clinician preferences for complete-arch fixed implant-supported prostheses: A survey of the membership of the Pacific Coast Society for Prosthodontics. J. Prosthet. Dent. 2020, 124, 699–705, in press. [Google Scholar] [CrossRef]
- Harel, N.; Ormianer, Z.; Zecharia, E.; Meirowitz, A. Consequences of experience and specialist training on the fabrication of implant-supported prostheses: A survey. J. Prosthet. Dent. 2017, 117, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, R.; Hosadettu, S.R.; Chandrakar, N. A survey on the use of techniques, materials in dental implantology practice. Indian J. Dent. Res. 2012, 23, 297. [Google Scholar] [CrossRef]
- Jayachandran, S.; Bhandal, B.S.; Hill, K.B.; Walmsley, A. Maintaining dental implants do general dental practitioners have the necessary knowledge? Br. Dent. J. 2015, 219, 25–28. [Google Scholar] [CrossRef]
- Afsharzand, Z.; Rashedi, B.; Petropoulos, V.C. Dentist communication with the dental laboratory for prosthodontic treatment using implants. J. Prosthodont. Implant Esthet. Reconstr. Dent. 2006, 15, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, Y.; Narita, T.; Shioda, Y.; Iwasaki, K.; Ikeda, T.; Namaki, S.; Salinas, T.J. Current status of implant prosthetics in Japan: A survey among certified dental lab technicians. Int. J. Implant Dent. 2015, 1, 4. [Google Scholar] [CrossRef]
- Al Dosari, A.A.F.; Habib, S.R.; Alnassar, T.; Alshihri, A.; Kamalan, R. The current considerations in the fabrication of implant prostheses and the state of prosthetic complications: A survey among the dental technicians. Saudi Dent. J. 2018, 30, 299–305. [Google Scholar] [CrossRef]
- Al Saleh, F.; AbuZayeda, M.; Kiat-Amnuay, S.; Milosevic, A. Survey of Dental Implant and Restoration Selection by Prosthodontists in Dubai. Int. J. Dent. 2021, 2021, 8815775. [Google Scholar] [CrossRef]
- Conserva, E.; Menini, M.; Tealdo, T.; Bevilacqua, M.; Ravera, G.; Pera, F.; Pera, P. The use of a masticatory robot to analyze the shock absorption capacity of different restorative materials for prosthetic implants: A preliminary report. Int. J. Prosthodont. 2009, 22, 53–55. [Google Scholar]
- Saini, M.; Singh, Y.; Arora, P.; Arora, V.; Jain, K. Implant biomaterials: A comprehensive review. World J. Clin. Cases 2015, 3, 52. [Google Scholar] [CrossRef] [PubMed]
- Al-AlSheikh, H.M. Quality of communication between dentists and dental technicians for fixed and removable prosthodontics. King Saud Univ. J. Dent. Sci. 2012, 3, 55–60. [Google Scholar] [CrossRef][Green Version]
- Kondareddy, S.; Gooty, J.R. Evaluation of Communication between the Dental Practitioners and Laboratory Technicians. Indian J. Dent. Adv. 2021, 12, 1–4. [Google Scholar]
- Bower, E.J.; Newton, P.D.; Gibbons, D.E.; Newton, J.T. A national survey of dental technicians: Career development, professional status and job satisfaction. Br. Dent. J. 2004, 197, 144–148. [Google Scholar] [CrossRef][Green Version]
- Petrie, C.S.; Nakatani, B.; Scott, J.M.; Moniz, J.; Walker, M.P. A survey of US dental schools on predoctoral implant curricula with emphasis on diagnosing and treating implant complications. J. Prosthet. Dent. 2021, 125, 126–136. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.C.C.; Kaste, L.M.; Lee, D.J.; Harlow, R.F.; Knoernschild, K.L.; Campbell, S.D.; Sukotjo, C. Dental student perceptions of predoctoral implant education and plans for providing implant treatment. J. Dent. Educ. 2011, 75, 750–760. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P. Implant success rates for single crowns and fixed partial dentures in general dental practices may be lower than those achieved in well-controlled university or specialty settings. J. Evid.-Based Dent. Pract. 2015, 15, 30–32. [Google Scholar] [CrossRef]
- McGARRY, T.J.; Jacobson, T.E. The professions of dentistry and dental laboratory technology: Improving the interface. J. Am. Dent. Assoc. 2004, 135, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.; Henderson, A.; Johnson, N. The future of education and training in dental technology: Designing a dental curriculum that facilitates teamwork across the oral health professions. Br. Dent. J. 2010, 208, 227–230. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question | Response Options | Prosthodontic Specialists | Dental Technicians | ||
|---|---|---|---|---|---|
| Count | Percentage | Count | Percentage | ||
| Age (years) | Min | 25 | - | 20 | - |
| Max | 63 | - | 49 | - | |
| Mean (±st.dev) | 36 (±9.100) | - | 28.6 (±8.59) | - | |
| Sex | Feminin | 37 | 67.3 | 26 | 47.3 |
| Masculin | 18 | 32.7 | 29 | 52.7 | |
| How many years of experience do you have? | <5 | 13 | 23.2 | 6 | 10.9 |
| 5–10 | 22 | 40.5 | 34 | 62.7 | |
| >10 | 20 | 36.3 | 15 | 26.4 | |
| What is the total number of implant-supported restorations? | <10 | 28 | 50.9 | 28 | 50.9 |
| 10–20 | 4 | 7.3 | 5 | 9.1 | |
| >20 | 23 | 41.8 | 22 | 40 | |
| Who has the leading role in the implant supported restauration treatment plan? | Dentist | 34 | 61.2 | 8 | 14.5 |
| Dental technician | 1 | 3 | 3 | 5.5 | |
| Dentist and dental technician | 19 | 28.5 | 28 | 50.9 | |
| Dental technician and dentist | 4 | 7.3 | 20 | 29.1 | |
| 1. How Old Are You? (20–99) | |||
| 4. How many total implant-supported fixed restorations have you made by now? | N | Mean ± Std. Deviation | Median [interquartile range] |
| 1. 1–9 restorations | 28 | 22.54 ± 2.13 | 22.00 [21.00, 23.00] |
| 2. 10–19 restorations | 5 | 32.40 ± 9.91 | 35.00 [23.00, 40.50] |
| 3. 20+ restorations | 22 | 35.45 ± 8.20 | 35.00 [29.00, 42.00] |
| Question | Response Options | Prosthodontic Specialists | Dental Technicians | ||
|---|---|---|---|---|---|
| Count | Percentage | Count | Percentage | ||
| What type of fixed restauration on implants have you done the most often? | Screw-retained restorations | 44.27 | 80.5 | 37.05 | 67.3 |
| Cement-retained restorations | 10.72 | 19.5 | 17.98 | 32.7 | |
| What type of implant abutment do you use most often in the implant fixed restorations? | Titanium | 34 | 61.8 | 45.98 | 83.6 |
| Zirconia | - | 5 | 9.1 | ||
| Custom abutment | 17.98 | 32.7 | 9 | 16.4 | |
| Straight/angled/calcinable abutment | 3 | 5,5 | - | - | |
| What type of impression do you send to the lab/receive in the lab for implant supported crown and bridge? | Open tray with connected transfer copings | 34.98 | 63.6 | 34.65 | 63 |
| Open tray without connected transfer copings | 14 | 25.5 | 12 | 21.8 | |
| Closed tray | 7.97 | 14.5 | 5 | 9.1 | |
| Intraoral scanning | 22 | 40 | 11 | 20 | |
| Plastic copings | 1 | 1.8 | - | - | |
| What type of impression do you send to the lab/receive in the lab for implant supported full-arch fixed prosthesis? | Open tray with connected transfer copings | 34 | 61.8 | 34.98 | 63.6 |
| Open tray without connected transfer copings | 6.98 | 12.7 | 14 | 25.5 | |
| Closed tray | 7.97 | 14.5 | 4 | 7.3 | |
| Intraoral scanning | 12.98 | 23.6 | 7.97 | 14.5 | |
| Plastic copings | 1 | 1.8 | 1 | 1.8 | |
| Correlation between Years of Experience and the Design/the Material Preferred by the Doctors for Full-Arch Fixed Implant Supported Prosthesis | Prosthodontic Specialists | Dental Technicians | ||
|---|---|---|---|---|
| Likelihood Ratio-p Value | Linear-by-Linear Associations-p Value | Likelihood Ratio-p Value | Linear-by-Linear Associations-p Value | |
| Resin material polymerized in the lab, acrylic teeth and the metallic milled framework | 0.0391 | 0.0141 | - | - |
| Full zirconia crowns on implants in maxillary restorations | 0.028 | 0.014 | - | - |
| Milled metallic framework (Ti, Cr-Co) with cemented crowns for the maxillary definitive fixed implant supported prosthesis. | 0.155 | 0.046 | - | - |
| Polymer milled framework (Peek, Pekkton) with cemented crowns for full-arch fixed implant supported mandibular prosthesis | 0.108 | 0.036 | 0.060 | 0.043 |
| Metallic cast framework with cemented crowns for full-arch fixed implant supported mandibular prosthesis | 0.071 | 0.013 | - | - |
| Resin material polymerized in the lab, acrylic teeth and metallic milled framework for full-arch fixed implant supported mandibular prosthesis | - | 0.060 | - | - |
| Milled PMMA and metallic milled framework for full-arch fixed implant supported mandibular prosthesis | - | 0.035 | - | - |
| Zirconia milled framework with cemented crowns for full-ach fixed implant supported mandibular prosthesis | - | - | 0.110 | 0.043 |
| Crosstab | |||||
|---|---|---|---|---|---|
| I23_K | |||||
| 0 | 1 | Total | |||
| I27_A | 0 | Count | 16a | 0b | 16 |
| %within I23_K | 36.4% | 0.0% | 29.1% | ||
| 1 | Count | 28a | 11b | 39 | |
| %within I23_K | 63.6% | 100.0% | 70.9% | ||
| Total | Count | 44 | 11 | 55 | |
| %within I23_K | 100.0% | 100.0% | 100.0% | ||
| Answers to Questions | Doctors | Technicians | p Value (Test) |
|---|---|---|---|
| I9_TitanIUM | 34/55 (61.8%) | 46/55 (83.6%) | 0.010 (Pearson Chi-Square) |
| I9_CUSTOM ABUTMENT | 18/55 (32.7%) | 9/55 (16.4%) | 0.046 (Pearson Chi-Square) |
| I17_D | 21/55 (38.2%) | 10/55 (18.2%) | 0.010 (Pearson Chi-Square) |
| I18_A | 46/55 (83.6%) | 35/55 (63.6%) | 0.017 (Pearson Chi-Square) |
| I23_B | 22/55 (40.0%) | 10/55 (18.2%) | 0.011 (Pearson Chi-Square) |
| I23_F | 8/55 (14.5%) | 0/55 (0.0%) | 0.005 (Fisher’s Exact Test) |
| I24_B | 22/55 (40.0%) | 7/55 (12.7%) | 0.001 (Pearson Chi-Square) |
| I24_F | 10/55 (18.2%) | 0/55 (0.0%) | 0.000 (Pearson Chi-Square) |
| I25_A | 8/55 (14.5%) | 19/55 (34.5%) | 0.014 (Pearson Chi-Square) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oancea, L.; Panaitescu, E.; Burlibasa, M.; Gagiu, C. Clinical versus Dental Laboratory Survey Regarding Modern Fixed Implant Supported Prosthetic in Romania. Appl. Sci. 2022, 12, 472. https://doi.org/10.3390/app12010472
Oancea L, Panaitescu E, Burlibasa M, Gagiu C. Clinical versus Dental Laboratory Survey Regarding Modern Fixed Implant Supported Prosthetic in Romania. Applied Sciences. 2022; 12(1):472. https://doi.org/10.3390/app12010472
Chicago/Turabian StyleOancea, Luminita, Eugenia Panaitescu, Mihai Burlibasa, and Catalin Gagiu. 2022. "Clinical versus Dental Laboratory Survey Regarding Modern Fixed Implant Supported Prosthetic in Romania" Applied Sciences 12, no. 1: 472. https://doi.org/10.3390/app12010472
APA StyleOancea, L., Panaitescu, E., Burlibasa, M., & Gagiu, C. (2022). Clinical versus Dental Laboratory Survey Regarding Modern Fixed Implant Supported Prosthetic in Romania. Applied Sciences, 12(1), 472. https://doi.org/10.3390/app12010472