
Bone Damage during Dental Implant Insertion: A Pilot Study Combining Strain Gauge and Histologic Analysis



Abstract
:1. Introduction
2. Materials and Methods
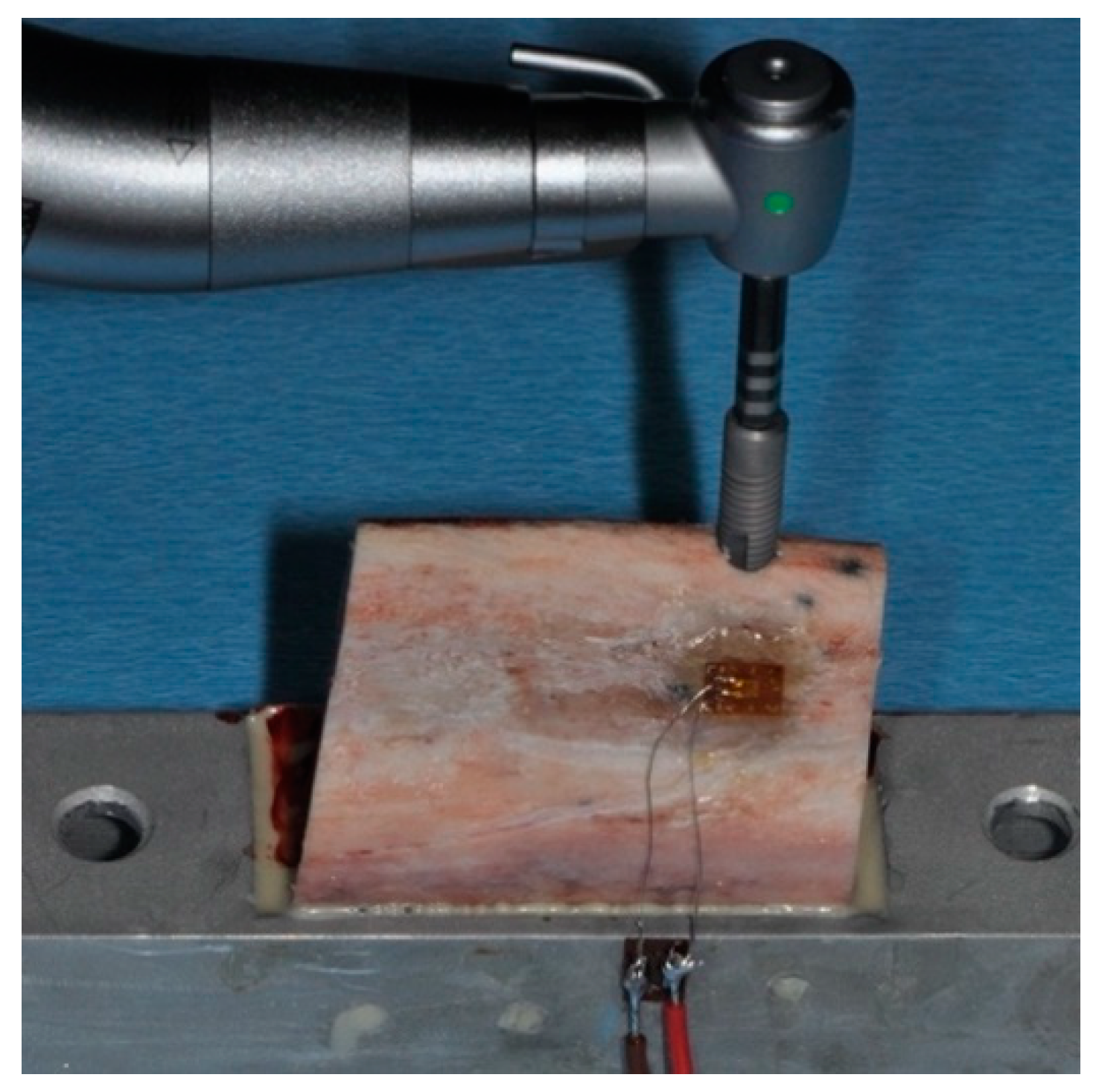
2.1. Biomechanical Measurements
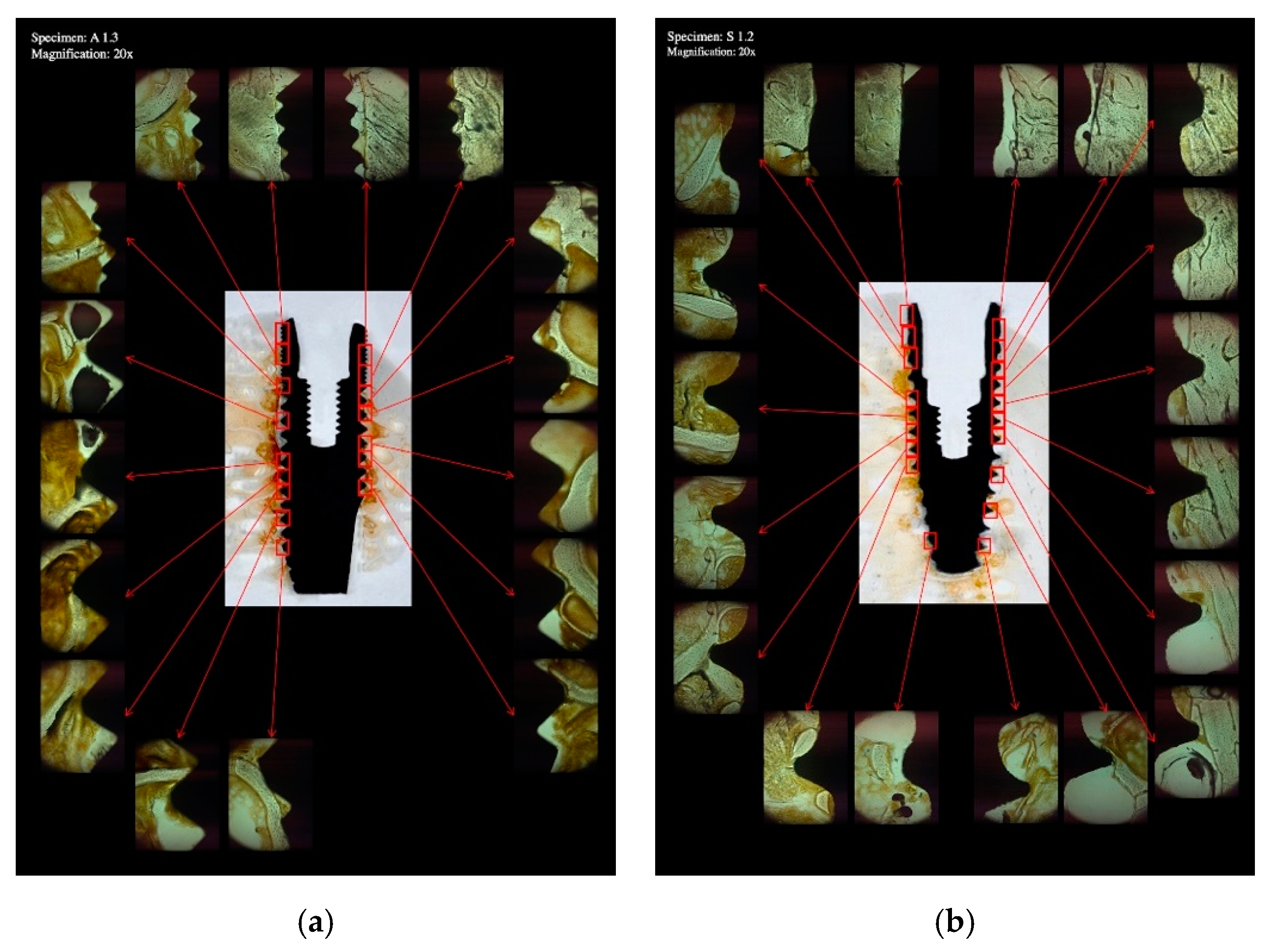
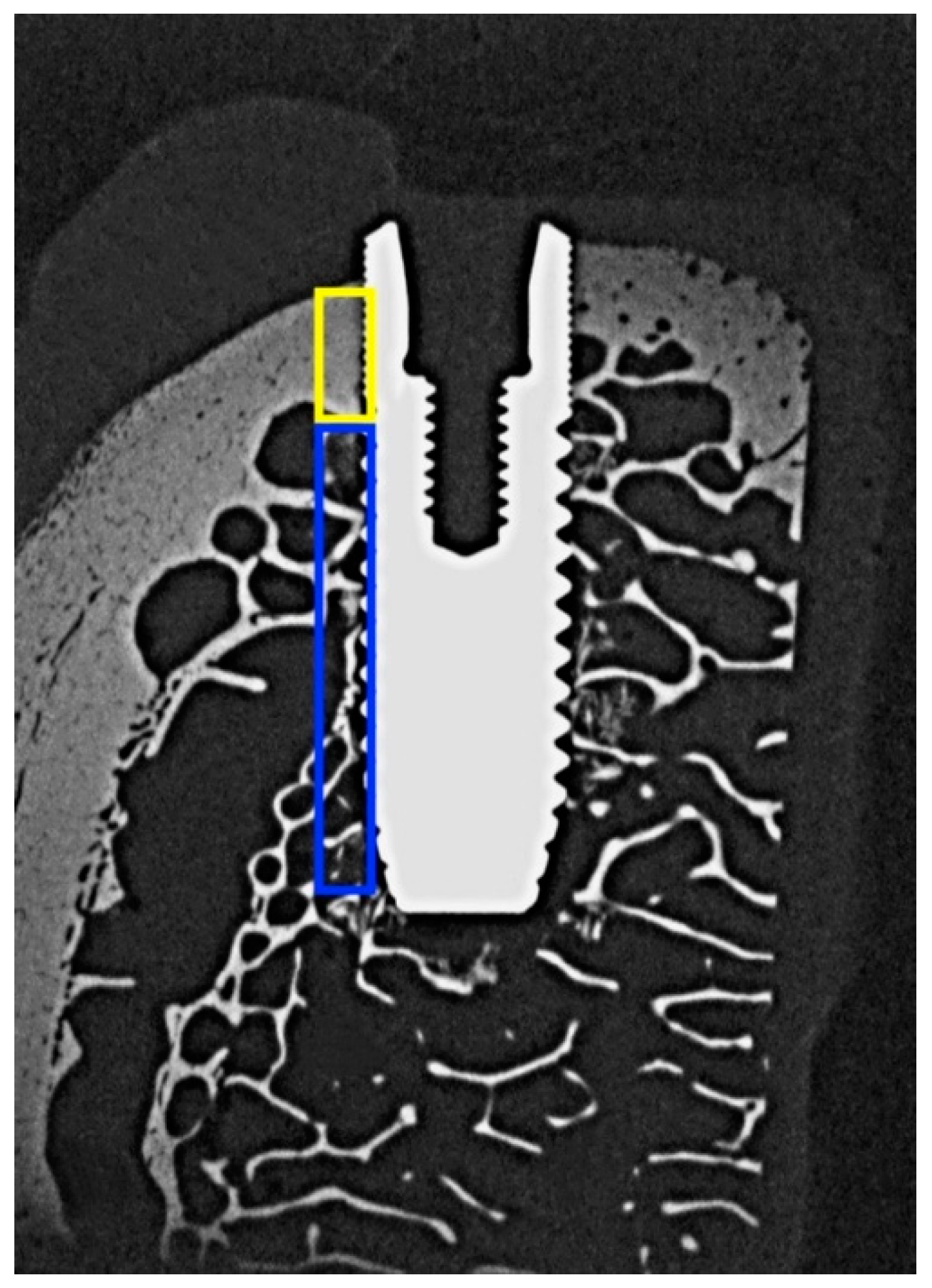
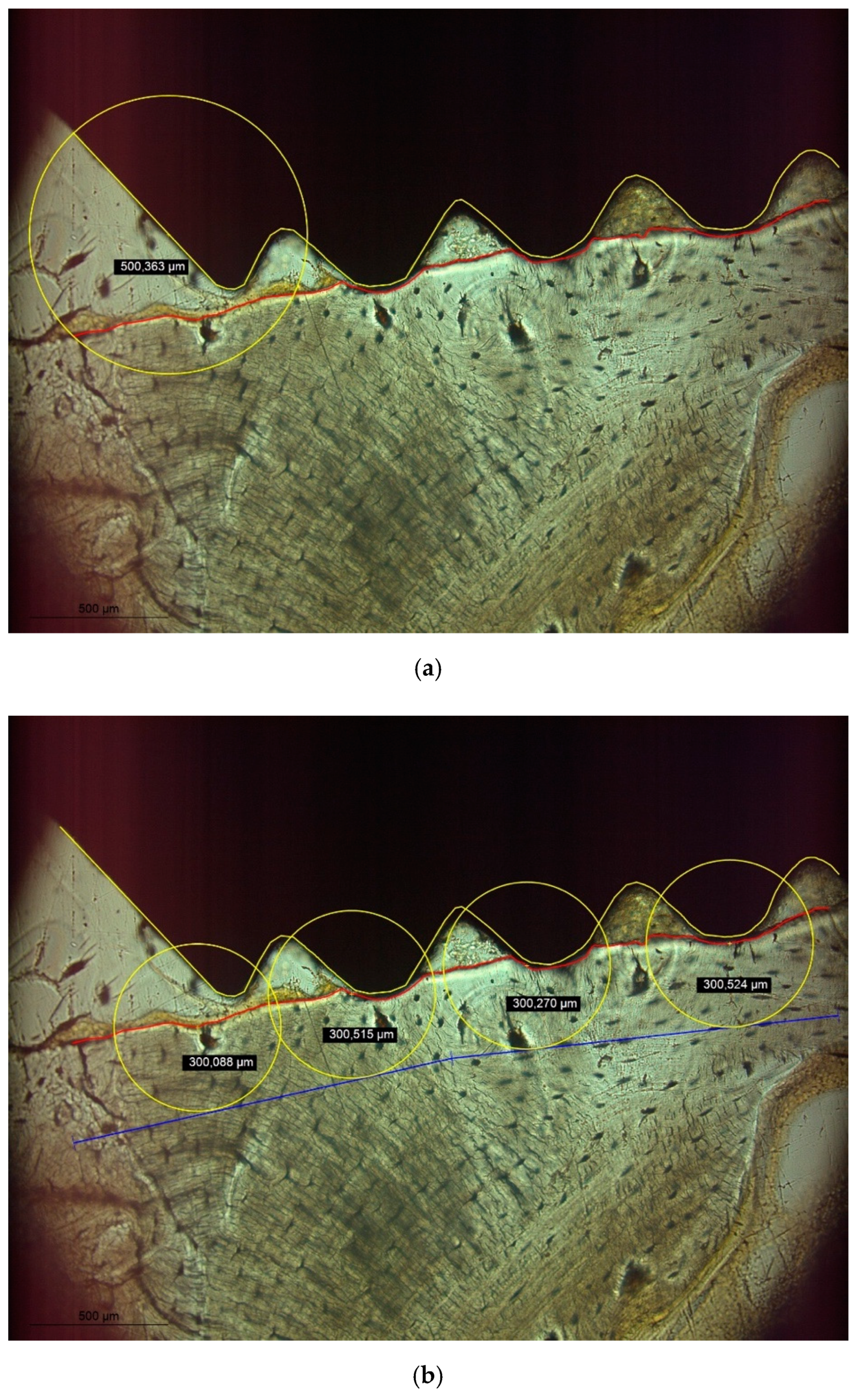
2.2. Histologic Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Dias, D.R.; Leles, C.R.; Lindh, C.; Ribeiro-Rotta, R.F. Marginal bone level changes and implant stability after loading are not influenced by baseline microstructural bone characteristics: 1-year follow-up. Clin. Oral Implant. Res. 2016, 27, 1212–1220. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, S.A.; Pérez-Díaz, L.; Mazón, P.; De Aza, P.N. Biomechanical Effects of a New Macrogeometry Design of Dental Implants: An In Vitro Experimental Analysis. J. Funct. Biomater. 2019, 10, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.H.; Lyons, K.; Tawse-Smith, A.; Ma, S. Resonance Frequency Analysis in Assessing Implant Stability: A Retrospective Analysis. Int. J. Prosthodont. 2019, 32, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Pevida, E.; Cherro, R.; Camps-Font, O.; Piqué, N. Effects of Drilling Protocol and Bone Density on the Stability of Implants According to Different Macrogeometries of the Implant Used: Results of an In Vitro Study. Int. J. Oral Maxillofac. Implant. 2020, 35, 955–964. [Google Scholar] [CrossRef] [PubMed]
- Dard, M.; Kuehne, S.; Obrecht, M.; Grandin, M.; Helfenstein, J.; Pippenger, B.E. Integrative Performance Analysis of a Novel Bone Level Tapered Implant. Adv. Dent. Res. 2016, 28, 28–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gazelakis, E.; Judge, R.B.; Palamara, J.E.A. The biomechanical profile of an osseo-integrated rectangular block implant: A pilot in vivo experimental study. Clin. Oral Implant. Res. 2021, 32, 1274–1287. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, I.; Carcuac, O.; Berglundh, T. Influence of implant geometry and osteotomy design on early bone healing: A pre-clinical in vivo study. Clin. Oral Implant. Res. 2021, 32, 1190–1199. [Google Scholar] [CrossRef] [PubMed]
- Nicolielo, L.F.P.; Van Dessel, J.; Jacobs, R.; Quirino Silveira Soares, M.; Collaert, B. Relationship between trabecular bone architecture and early dental implant failure in the posterior region of the mandible. Clin. Oral Implant. Res. 2020, 31, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Agustín-Panadero, R.; Martínez-Martínez, N.; Fernandez-Estevan, L.; Faus-López, J.; Solá-Ruíz, M.F. Influence of Transmucosal Area Morphology on Peri-Implant Bone Loss in Tissue-Level Implants. Int. J. Oral Maxillofac. Implant. 2019, 34, 947–952. [Google Scholar] [CrossRef] [PubMed]
- Palombo, D.; Rahmati, M.; Vignoletti, F.; Sanz-Esporrin, J.; Haugen, H.J.; Sanz, M. Hard and soft tissue healing around implants with a modified implant neck configuration: An experimental in vivo preclinical investigation. Clin. Oral Implant. Res. 2021, 32, 1127–1141. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Chrcanovic, B.; Östman, P.O.; Sennerby, L. Initial and long-term crestal bone responses to modern dental implants. Periodontol. 2000 2017, 73, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Friberg, B.; Ahmadzai, M. A prospective study on single tooth reconstructions using parallel walled implants with internal connection (NobelParallel CC) and abutments with angulated screw channels (ASC). Clin. Implant. Dent. Relat. Res. 2019, 21, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Li Manni, L.; Lecloux, G.; Rompen, E.; Aouini, W.; Shapira, L.; Lambert, F. Clinical and radiographic assessment of circular versus triangular cross-section neck Implants in the posterior maxilla: A 1-year randomized controlled trial. Clin. Oral Implant. Res. 2020, 31, 814–824. [Google Scholar] [CrossRef] [PubMed]
- Tokuc, B.; Kan, B. The effect of triangular cross-section neck design on crestal bone stability in the anterior mandible: A randomized, controlled, split-mouth clinical trial. Clin. Oral Implant. Res. 2021, 32, 1241–1250. [Google Scholar] [CrossRef] [PubMed]
- Grobecker-Karl, T.; Orujov, K.; Klär, V.; Karl, M. Use of a dentin bonding agent for the fixation of strain gauges on bone. J. Mech. Behav. Biomed. Mater. 2021, 119, 104545. [Google Scholar] [CrossRef] [PubMed]
- Donath, K.; Breuner, G. A method for the study of undecalcified bones and teeth with attached soft tissues. The Säge-Schliff (sawing and grinding) technique. J. Oral Pathol. 1982, 11, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Karl, M.; Palarie, V.; Nacu, V.; Grobecker-Karl, T. A Pilot Animal Study Aimed at Assessing the Mechanical Quality of Regenerated Alveolar Bone. Int. J. Oral Maxillofac. Implant. 2020, 35, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Grobecker-Karl, T.; Christian, M.; Karl, M. Effect of endodontic access cavity preparation on monolithic and ceramic veneered zirconia restorations. Quintessence Int. 2016, 47, 725–729. [Google Scholar] [PubMed]
- Burr, D.B.; Hooser, M. Alterations to the en bloc basic fuchsin staining protocol for the demonstration of microdamage produced in vivo. Bone 1995, 17, 431–433. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group Name | Straumann | Astra |
|---|---|---|
| Implant | Straumann Bone Level Tapered 4.1 × 12 mm (Institut Straumann AG, Basel, Switzerland) | OsseoSpeed TX 4.0 S × 13 mm (Astra Tech Implant System, Dentsply Implants Manufacturing GmbH, Mannheim, Germany) |
| Drill sequence | Needle drill | Round bur |
| 2.2 mm pilot drill | Twist drill 2.0 | |
| 2.8 mm BLT drill | Twist drill 3.2 | |
| 3.5 mm BLT drill | Twist drill 3.7 |
| ASTRA | Straumann | Welch t-Tests (p-Value) | |||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Torque | 29.76 | 26.893 | 34.08 | 17.428 | 0.772 |
| Strain | 383.38 | 299.860 | 410.84 | 284.754 | 0.893 |
| ISQ | * 79.20 | 11.339 | 81.80 | 2.842 | 0.642 |
| BMDc | 0.894 | 0.025 | 0.872 | 0.058 | 0.466 |
| BMDt | 0.486 | 0.099 | 0.434 | 0.065 | 0.360 |
| BICc | 0.756 | 0.059 | 0.868 | 0.054 | 0.014 |
| BICt | 0.428 | 0.064 | 0.600 | 0.101 | 0.016 |
| microC | ** 92.204 | 26.241 | 49.732 | 7.318 | 0.020 |
| microT | *** 44.484 | 18.810 | **** 45.034 | 23.733 | 0.969 |
| macroC | 10.862 | 1.443 | 11.020 | 2.073 | 0.893 |
| macroT | 5.494 | 0.976 | 6.286 | 3.045 | 0.600 |
| defC | 0.592 | 0.504 | 0.326 | 0.195 | 0.320 |
| defT | 0.368 | 0.161 | ***** 0.418 | 0.226 | 0.699 |
| (a) | |||||||||||||
| Correlation Coefficients | |||||||||||||
| Torque | Strain | ISQ | BMDc | BMDt | BICc | BICt | microC | microT | macroC | macroT | defC | defT | |
| Torque | −0.239 | 0.665 | 0.635 | 0.867 | −0.431 | 0.969 | −0.259 | −0.212 | −0.502 | 0.726 | 0.179 | 0.549 | |
| Strain | 0.761 | 0.511 | 0.443 | 0.300 | 0.859 | 0.013 | 0.861 | 0.745 | 0.870 | −0.700 | −0.566 | −0.902 | |
| ISQ | 0.221 | 0.490 | 0.664 | 0.762 | 0.003 | 0.665 | 0.093 | 0.393 | 0.107 | 0.943 | 0.313 | 0.006 | |
| BMDc | 0.250 | 0.557 | 0.222 | 0.652 | 0.385 | 0.782 | −0.007 | 0.003 | 0.220 | 0.503 | 0.339 | −0.115 | |
| BMDt | 0.057 | 0.700 | 0.134 | 0.233 | −0.128 | 0.896 | 0.251 | 0.270 | −0.105 | 0.685 | −0.173 | 0.119 | |
| BICc | 0.469 | 0.141 | 0.996 | 0.522 | 0.838 | −0.207 | 0.559 | 0.459 | 0.937 | −0.305 | −0.095 | −0.911 | |
| BICt | 0.007 | 0.987 | 0.220 | 0.118 | 0.039 | 0.738 | −0.140 | −0.152 | −0.320 | 0.650 | 0.135 | 0.369 | |
| microC | 0.674 | 0.140 | 0.882 | 0.992 | 0.684 | 0.327 | 0.823 | 0.885 | 0.721 | −0.171 | −0.773 | −0.809 | |
| microT | 0.732 | 0.255 | 0.513 | 0.997 | 0.660 | 0.437 | 0.807 | 0.046 | 0.718 | 0.180 | −0.485 | −0.743 | |
| macroC | 0.329 | 0.130 | 0.864 | 0.722 | 0.867 | 0.019 | 0.599 | 0.169 | 0.172 | −0.194 | −0.200 | −0.983 | |
| macroT | 0.165 | 0.230 | 0.016 | 0.388 | 0.202 | 0.618 | 0.236 | 0.783 | 0.772 | 0.755 | 0.439 | 0.310 | |
| defC | 0.774 | 0.434 | 0.609 | 0.577 | 0.780 | 0.879 | 0.828 | 0.125 | 0.408 | 0.746 | 0.460 | 0.370 | |
| defT | 0.338 | 0.098 | 0.993 | 0.854 | 0.849 | 0.032 | 0.541 | 0.098 | 0.150 | 0.003 | 0.612 | 0.540 | |
| p-values | |||||||||||||
| (b) | |||||||||||||
| Correlation Coefficients | |||||||||||||
| Torque | Strain | ISQ | BMDc | BMDt | BICc | BICt | microC | microT | macroC | macroT | defC | defT | |
| Torque | −0.138 | 0.040 | 0.120 | 0.237 | −0.916 | 0.458 | −0.308 | 0.483 | 0.498 | 0.681 | −0.036 | −0.764 | |
| Strain | 0.825 | 0.023 | 0.624 | 0.578 | 0.351 | −0.560 | −0.235 | −0.164 | −0.048 | −0.252 | 0.673 | −0.480 | |
| ISQ | 0.949 | 0.970 | 0.362 | 0.335 | 0.301 | −0.600 | 0.618 | −0.819 | 0.608 | −0.597 | 0.699 | −0.115 | |
| BMDc | 0.848 | 0.261 | 0.550 | 0.992 | 0.156 | −0.754 | 0.434 | −0.127 | 0.701 | −0.472 | 0.852 | −0.327 | |
| BMDt | 0.701 | 0.307 | 0.582 | 0.001 | 0.031 | −0.672 | 0.394 | −0.039 | 0.748 | −0.372 | 0.810 | −0.394 | |
| BICc | 0.029 | 0.562 | 0.623 | 0.803 | 0.960 | −0.737 | 0.435 | −0.739 | −0.251 | −0.868 | 0.415 | 0.545 | |
| BICt | 0.438 | 0.326 | 0.285 | 0.141 | 0.214 | 0.155 | −0.656 | 0.676 | −0.403 | 0.915 | −0.884 | −0.118 | |
| microC | 0.615 | 0.703 | 0.266 | 0.466 | 0.512 | 0.464 | 0.230 | −0.499 | 0.629 | −0.791 | 0.440 | 0.520 | |
| microT | 0.410 | 0.792 | 0.090 | 0.839 | 0.950 | 0.154 | 0.211 | 0.392 | −0.100 | 0.777 | −0.586 | −0.139 | |
| macroC | 0.394 | 0.939 | 0.277 | 0.187 | 0.146 | 0.684 | 0.502 | 0.255 | 0.873 | −0.256 | 0.576 | −0.272 | |
| macroT | 0.206 | 0.682 | 0.288 | 0.423 | 0.537 | 0.056 | 0.029 | 0.111 | 0.122 | 0.677 | −0.655 | −0.473 | |
| defC | 0.954 | 0.213 | 0.189 | 0.067 | 0.097 | 0.487 | 0.047 | 0.459 | 0.299 | 0.310 | 0.230 | −0.346 | |
| defT | 0.133 | 0.414 | 0.854 | 0.591 | 0.512 | 0.342 | 0.851 | 0.370 | 0.756 | 0.658 | 0.421 | 0.569 | |
| p-values | |||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klär, V.; Karl, M.; Grobecker-Karl, T. Bone Damage during Dental Implant Insertion: A Pilot Study Combining Strain Gauge and Histologic Analysis. Appl. Sci. 2022, 12, 291. https://doi.org/10.3390/app12010291
Klär V, Karl M, Grobecker-Karl T. Bone Damage during Dental Implant Insertion: A Pilot Study Combining Strain Gauge and Histologic Analysis. Applied Sciences. 2022; 12(1):291. https://doi.org/10.3390/app12010291
Chicago/Turabian StyleKlär, Virgilia, Matthias Karl, and Tanja Grobecker-Karl. 2022. "Bone Damage during Dental Implant Insertion: A Pilot Study Combining Strain Gauge and Histologic Analysis" Applied Sciences 12, no. 1: 291. https://doi.org/10.3390/app12010291
APA StyleKlär, V., Karl, M., & Grobecker-Karl, T. (2022). Bone Damage during Dental Implant Insertion: A Pilot Study Combining Strain Gauge and Histologic Analysis. Applied Sciences, 12(1), 291. https://doi.org/10.3390/app12010291