
A Review of the Challenges in Deep Learning for Skeletal and Smooth Muscle Ultrasound Images

 ,
, 
 ,
,  ,
, 
Abstract
Featured Application
Abstract
1. Introduction
2. Methods
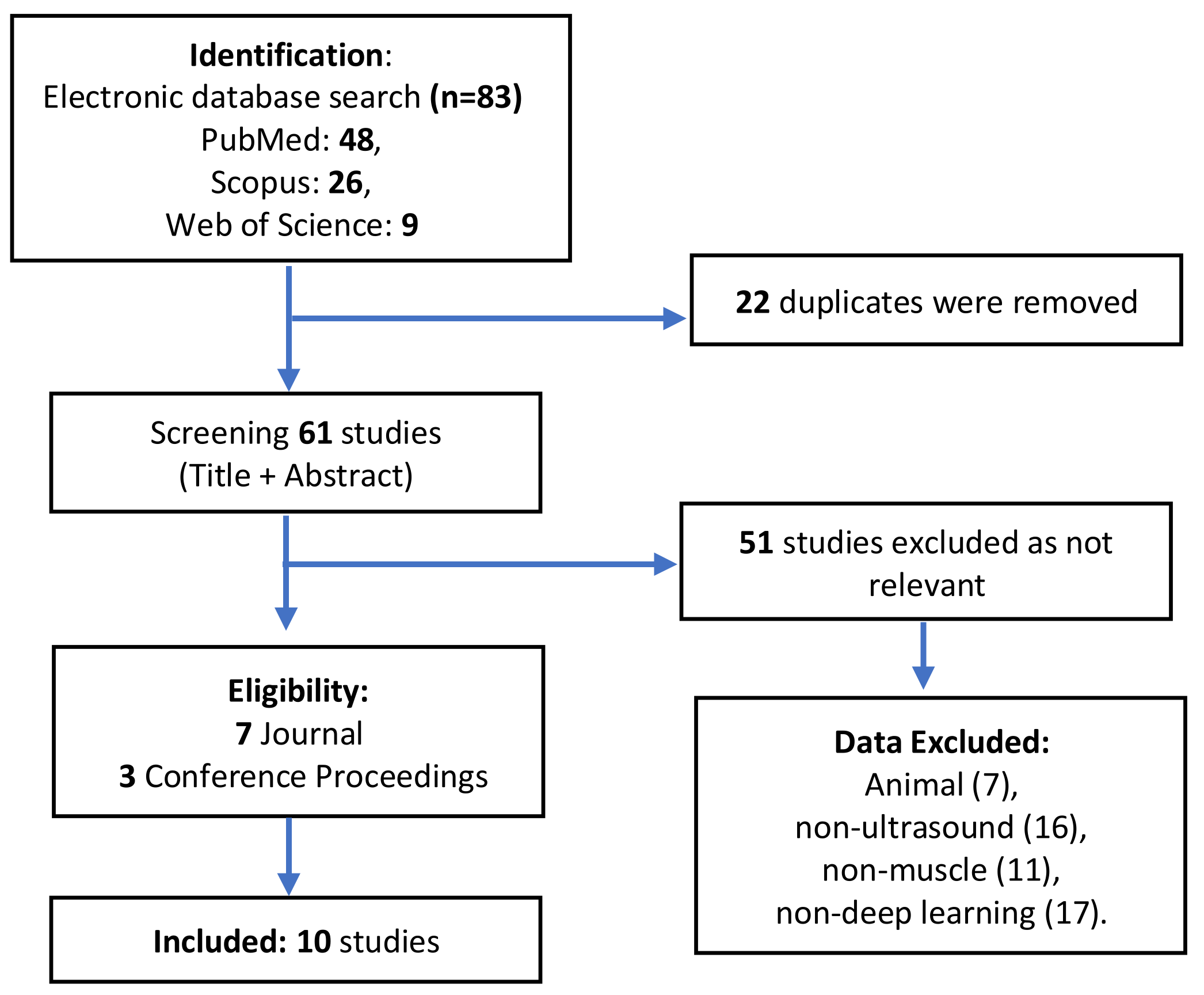
2.1. Analysis of the Literature
2.2. Data Eligibility Requirement
2.3. Data Analysis
3. Results and Discussion
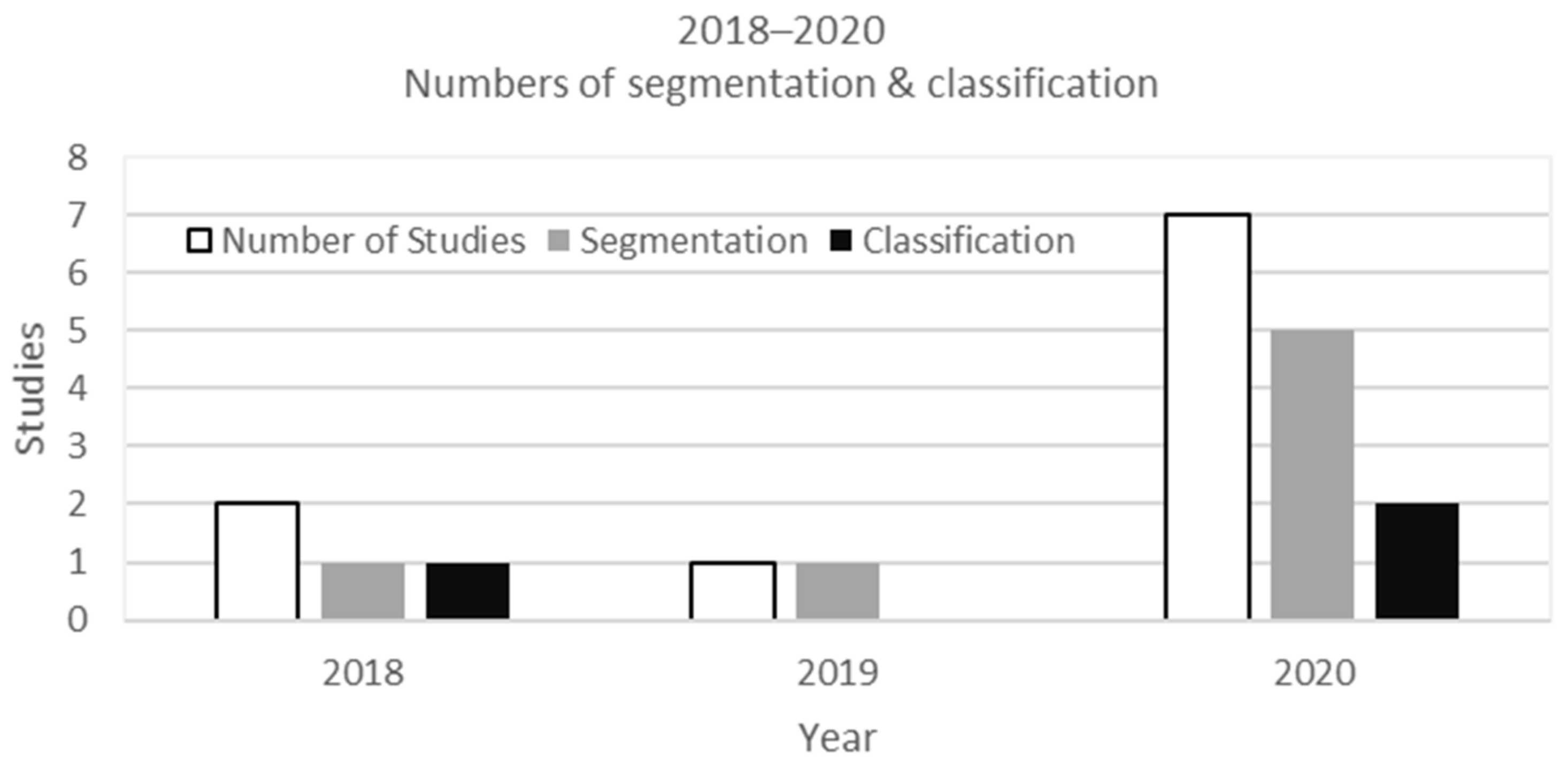
3.1. Numbers of Studies
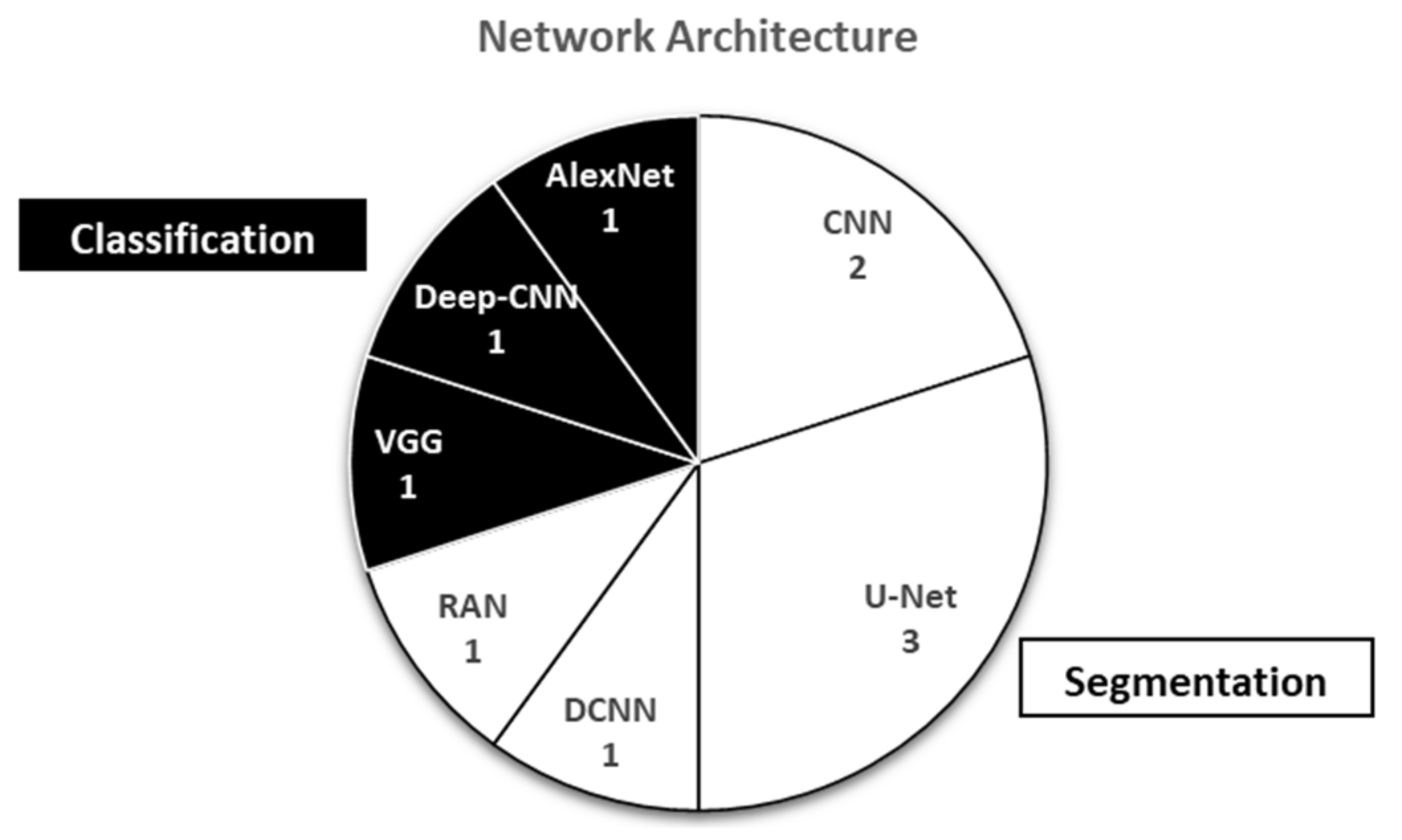
3.2. Network Architecture
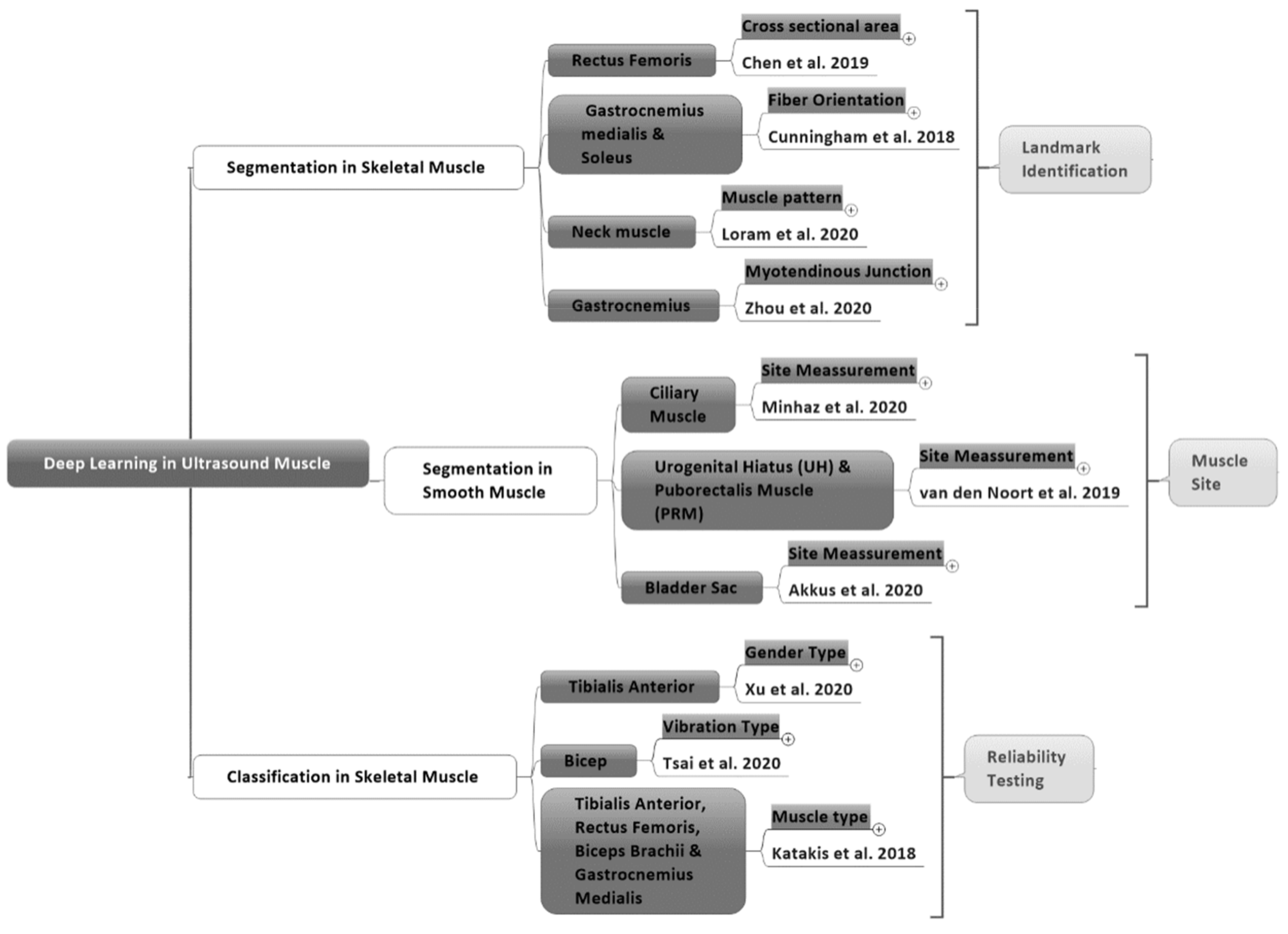
3.3. Segmentation in Skeletal Muscle
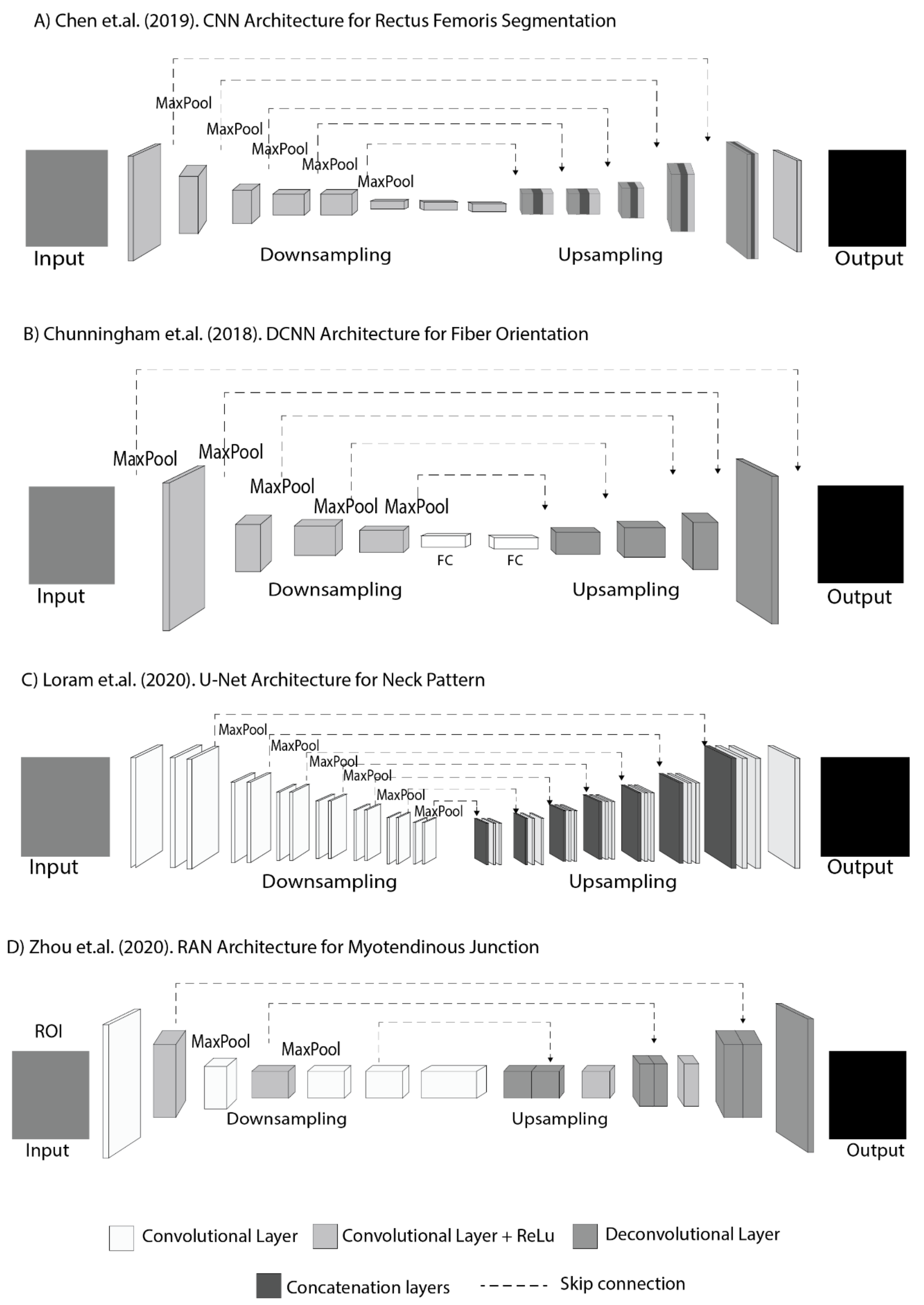
3.4. Segmentation Architecture in Skeletal Muscle
3.5. Segmentation in Smooth Muscle
3.6. Segmentation Architecture in Smooth Muscles
3.7. Classification in Skeletal Muscle
3.8. Classification Architecture in Skeletal Muscle
3.9. Dataset Requirement
3.10. Matrix Performance Result
3.11. Limitation
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wannamethee, S.G.; Atkins, J.L. Muscle loss and obesity: The health implications of sarcopenia and sarcopenic obesity. Proc. Nutr. Soc. 2015, 74, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Bruyère, O.; Beaudart, C.; Reginster, J.-Y.; Buckinx, F.; Schoene, D.; Hirani, V.; Cooper, C.; Kanis, J.A.; Rizzoli, R.; McCloskey, E. Assessment of muscle mass, muscle strength and physical performance in clinical practice: An international survey. Eur. Geriatr. Med. 2016, 7, 243–246. [Google Scholar] [CrossRef]
- van Alfen, N.; Gijsbertse, K.; de Korte, C.L. How useful is muscle ultrasound in the diagnostic workup of neuromuscular diseases? Curr. Opin. Neurol. 2018, 31, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Wijntjes, J.; van Alfen, N. Muscle ultrasound: Present state and future opportunities. Muscle Nerve 2020. [Google Scholar] [CrossRef] [PubMed]
- Alfen, N.V.; Gilhuis, H.J.; Keijzers, J.P.; Pillen, S.; Van Dijk, J.P. Quantitative facial muscle ultrasound: Feasibility and reproducibility. Muscle Nerve 2013, 48, 375–380. [Google Scholar] [CrossRef]
- Yang, X.; Sun, X.; Zhou, D.; Li, Y.; Liu, H. Towards wearable A-mode ultrasound sensing for real-time finger motion recognition. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1199–1208. [Google Scholar] [CrossRef]
- Mutalab Shaykat, M.A.; Islam, Y.; Ishtiaque Hossain, M. Shape Detection of Liver From 2D Ultrasound Images. arXiv 2019, arXiv:1911.10352. [Google Scholar]
- Lees, W. Ultrasound imaging in three and four dimensions. In Seminars in Ultrasound, CT and MRI; WB Saunders: Philadelphia, PA, USA, 2001; pp. 85–105. [Google Scholar] [CrossRef]
- Elnokrashy, A.F.; Kadah, Y. 4D ultrasound adaptive image pre-processing. In Proceedings of the 2018 35th National Radio Science Conference (NRSC), Cairo, Egypt, 20–22 March 2018; pp. 214–222. [Google Scholar]
- Garg, A.; Khandelwal, V. Combination of spatial domain filters for speckle noise reduction in ultrasound medical images. Adv. Electr. Electron. Eng. 2018, 15, 857–865. [Google Scholar] [CrossRef]
- Mourtzakis, M.; Parry, S.; Connolly, B.; Puthucheary, Z. Skeletal muscle ultrasound in critical care: A tool in need of translation. Ann. Am. Thorac. Soc. 2017, 14, 1495–1503. [Google Scholar] [CrossRef]
- Calas, M.J.G.; Pereira, F.P.A.; Gonçalves, L.P.; Lopes, F.P.P.L. Preliminary study of the technical limitations of automated breast ultrasound: From procedure to diagnosis. Radiol. Bras. 2020, 53, 293–300. [Google Scholar] [CrossRef]
- Zaidman, C.M.; Van Alfen, N. Ultrasound in the assessment of myopathic disorders. J. Clin. Neurophysiol. 2016, 33, 103–111. [Google Scholar] [CrossRef]
- Riaz, H.; Park, J.; Choi, H.; Kim, H.; Kim, J. Deep and densely connected networks for classification of diabetic retinopathy. Diagnostics 2020, 10, 24. [Google Scholar] [CrossRef]
- Chan, H.P.; Hadjiiski, L.M.; Samala, R.K. Computer-aided diagnosis in the era of deep learning. Med. Phys. 2020, 47, e218–e227. [Google Scholar] [CrossRef]
- Shortliffe, E.H.; Sepúlveda, M.J. Clinical decision support in the era of artificial intelligence. JAMA-J. Am. Med. Assoc. 2018, 320, 2199–2200. [Google Scholar] [CrossRef]
- Hesamian, M.H.; Jia, W.; He, X.; Kennedy, P. Deep learning techniques for medical image segmentation: Achievements and challenges. J. Digit. Imaging 2019, 32, 582–596. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar] [CrossRef]
- Long, J.; Shelhamer, E.; Darrell, T. Fully convolutional networks for semantic segmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 3431–3440. [Google Scholar] [CrossRef]
- Liu, S.; Wang, Y.; Yang, X.; Lei, B.; Liu, L.; Li, S.X.; Ni, D.; Wang, T. Deep learning in medical ultrasound analysis: A review. Engineering 2019, 5, 261–275. [Google Scholar] [CrossRef]
- Chen, H.; Ni, D.; Qin, J.; Li, S.; Yang, X.; Wang, T.; Heng, P.A. Standard plane localization in fetal ultrasound via domain transferred deep neural networks. IEEE J. Biomed. Health Inform. 2015, 19, 1627–1636. [Google Scholar] [CrossRef]
- Kumar, A.; Sridar, P.; Quinton, A.; Kumar, R.K.; Feng, D.; Nanan, R.; Kim, J. Plane identification in fetal ultrasound images using saliency maps and convolutional neural networks. In Proceedings of the 2016 IEEE 13th International Symposium on Biomedical Imaging (ISBI), Prague, Czech Republic, 13–16 April 2016; pp. 791–794. [Google Scholar]
- Baumgartner, C.F.; Kamnitsas, K.; Matthew, J.; Smith, S.; Kainz, B.; Rueckert, D. Real-time standard scan plane detection and localisation in fetal ultrasound using fully convolutional neural networks. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention (MICCAI), Athens, Greece, 17–21 October 2016; pp. 203–211. [Google Scholar]
- Ravishankar, H.; Prabhu, S.M.; Vaidya, V.; Singhal, N. Hybrid approach for automatic segmentation of fetal abdomen from ultrasound images using deep learning. In Proceedings of the 2016 IEEE 13th International Symposium on Biomedical Imaging (ISBI), Prague, Czech Republic, 13–16 April 2016; pp. 779–782. [Google Scholar]
- Smistad, E.; Løvstakken, L. Vessel detection in ultrasound images using deep convolutional neural networks. In Deep Learning and Data Labeling for Medical Applications; Springer: Berlin, Germany, 2016; pp. 30–38. [Google Scholar]
- Jaumard-Hakoun, A.; Xu, K.; Roussel-Ragot, P.; Dreyfus, G.; Denby, B. Tongue contour extraction from ultrasound images based on deep neural network. arXiv 2016, arXiv:1605.05912. [Google Scholar]
- Zheng, Y.; Liu, D.; Georgescu, B.; Nguyen, H.; Comaniciu, D. 3D deep learning for efficient and robust landmark detection in volumetric data. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention (MICCAI), Munich, Germany, 5–9 October 2015; pp. 565–572. [Google Scholar]
- Ma, J.; Wu, F.; Zhu, J.; Xu, D.; Kong, D. A pre-trained convolutional neural network based method for thyroid nodule diagnosis. Ultrasonics 2017, 73, 221–230. [Google Scholar] [CrossRef]
- Jabarulla, M.Y.; Lee, H.-N. Computer aided diagnostic system for ultrasound liver images: A systematic review. Optik 2017, 140, 1114–1126. [Google Scholar] [CrossRef]
- Katakis, S.; Barotsis, N.; Kastaniotis, D.; Theoharatos, C.; Tsourounis, D.; Fotopoulos, S.; Panagiotopoulos, E. Muscle Type Classification on Ultrasound Imaging Using Deep Convolutional Neural Networks. In Proceedings of the 2018 IEEE 13th Image, Video, and Multidimensional Signal Processing Workshop, IVMSP 2018—Proceedings, Aristi Village, Greece, 10–12 June 2018. [Google Scholar]
- Xu, J.; Xu, D.; Wei, Q.; Zhou, Y. Automatic classification of male and female skeletal muscles using ultrasound imaging. Biomed. Signal. Process. Control. 2020, 57. [Google Scholar] [CrossRef]
- Tsai, J.Y.; Jan, Y.K.; Liau, B.Y.; Subiakto, R.B.R.; Lin, C.Y.; Hendradi, R.; Hsu, Y.C.; Lin, Q.; Chang, H.T.; Lung, C.W. A Convolutional Neural Network Model to Classify the Effects of Vibrations on Biceps Muscles. Adv. Intell. Syst. Comput. 2020, 1215 AISC, 56–62. [Google Scholar] [CrossRef]
- Cunningham, R.; Sánchez, M.B.; May, G.; Loram, I. Estimating full regional skeletal muscle fibre orientation from b-mode ultrasound images using convolutional, residual, and deconvolutional neural networks. J. Imaging 2018, 4. [Google Scholar] [CrossRef]
- Chen, X.; Xie, C.; Chen, Z.; Li, Q. Automatic Tracking of Muscle Cross-Sectional Area Using Convolutional Neural Networks with Ultrasound. J. Ultrasound Med. 2019, 38, 2901–2908. [Google Scholar] [CrossRef] [PubMed]
- Loram, I.; Siddique, A.; Sanchez, M.B.; Harding, P.; Silverdale, M.; Kobylecki, C.; Cunningham, R. Objective Analysis of Neck Muscle Boundaries for Cervical Dystonia Using Ultrasound Imaging and Deep Learning. IEEE J. Biomed. Health Inform. 2020, 24, 1016–1027. [Google Scholar] [CrossRef] [PubMed]
- Zhou, G.Q.; Huo, E.Z.; Yuan, M.; Zhou, P.; Wang, R.L.; Wang, K.N.; Chen, Y.; He, X.P. A Single-Shot Region-Adaptive Network for Myotendinous Junction Segmentation in Muscular Ultrasound Images. IEEE Trans. Ultrason. Ferr. 2020. [Google Scholar] [CrossRef] [PubMed]
- van den Noort, F.; van der Vaart, C.H.; Grob, A.T.M.; van de Waarsenburg, M.K.; Slump, C.H.; van Stralen, M. Deep learning enables automatic quantitative assessment of puborectalis muscle and urogenital hiatus in plane of minimal hiatal dimensions. Ultrasound Obstet. Gynecol. 2019, 54, 270–275. [Google Scholar] [CrossRef]
- Akkus, Z.; Kim, B.H.; Nayak, R.; Gregory, A.; Alizad, A.; Fatemi, M. Fully Automated Segmentation of Bladder Sac and Measurement of Detrusor Wall Thickness from Transabdominal Ultrasound Images. Sensors 2020, 20, 4175. [Google Scholar] [CrossRef]
- Minhaz, A.T.; Wu, H.; Helms, R.W.; Sevgi, D.D.; Kim, A.; Kwak, S.; Orge, F.H.; Wilson, D.L. 3D ultrasound biomicroscopy (3D-UBM) imaging of the eye for unique 3D assessment of ciliary body. In Proceedings of the Progress in Biomedical Optics and Imaging—Proceedings of SPIE, Houston, TX, USA, 16 March 2020. [Google Scholar]
- Murray, I.R.; Baily, J.E.; Chen, W.C.; Dar, A.; Gonzalez, Z.N.; Jensen, A.R.; Petrigliano, F.A.; Deb, A.; Henderson, N.C. Skeletal and cardiac muscle pericytes: Functions and therapeutic potential. Pharmacol. Ther. 2017, 171, 65–74. [Google Scholar] [CrossRef]
- Rohlén, R. Segmentation of motor units in ultrasound image sequences. Dissertation. 2016. Available online: http://urn.kb.se/resolve?urn=urn:nbn:se:umu:diva-126896 (accessed on 23 April 2021).
- Ahhmed, A.M.; Nasu, T.; Muguruma, M. Impact of transglutaminase on the textural, physicochemical, and structural properties of chicken skeletal, smooth, and cardiac muscles. Meat Sci. 2009, 83, 759–767. [Google Scholar] [CrossRef]
- Haque, I.R.I.; Neubert, J. Deep learning approaches to biomedical image segmentation. Inform. Med. Unlocked. 2020, 18, 100297. [Google Scholar] [CrossRef]
- Géron, A. Hands-on Machine Learning with Scikit-Learn., Keras, and TensorFlow: Concepts, Tools, and Techniques to Build. Intelligent Systems; O’Reilly Media: Boston, MA, USA, 2019; Available online: https://www.oreilly.com/library/view/hands-on-machine-learning/9781492032632/ (accessed on 23 April 2021).
- Maggiori, E.; Tarabalka, Y.; Charpiat, G.; Alliez, P. Fully convolutional neural networks for remote sensing image classification. In Proceedings of the 2016 IEEE International Geoscience and Remote Sensing Symposium (IGARSS), Beijing, China, 10–15 July 2016; pp. 5071–5074. [Google Scholar]
- Huang, B.; Chen, Z.; Wu, P.-M.; Ye, Y.; Feng, S.-T.; Wong, C.-Y.O.; Zheng, L.; Liu, Y.; Wang, T.; Li, Q. Fully automated delineation of gross tumor volume for head and neck cancer on PET-CT using deep learning: A dual-center study. Contrast Media Mol. Imaging 2018, 2018, 1–12. [Google Scholar] [CrossRef]
- Shaziya, H.; Shyamala, K.; Zaheer, R. Automatic lung segmentation on thoracic CT scans using U-Net convolutional network. In Proceedings of the 2018 International Conference on Communication and Signal Processing (ICCSP), Chennai, India, 3–5 April 2018; pp. 643–647. [Google Scholar]
- Li, S.; Zhao, X.; Zhou, G. Automatic pixel-level multiple damage detection of concrete structure using fully convolutional network. Comput. Aided. Civ. Inf. 2019, 34, 616–634. [Google Scholar] [CrossRef]
- Hashimoto, F.; Kakimoto, A.; Ota, N.; Ito, S.; Nishizawa, S. Automated segmentation of 2D low-dose CT images of the psoas-major muscle using deep convolutional neural networks. Radiol. Phys. Technol. 2019, 12, 210–215. [Google Scholar] [CrossRef]
- Balamurugan, S.; Arumugam, G. Optimal Spatial Fuzzy Clustering Algorithm Based ROI Segmentation in Ultrasound Kidney Images. J. Comput. Theor. Nanosci. 2018, 15, 2794–2804. [Google Scholar] [CrossRef]
- Benrabha, J.; Meziane, F. Automatic ROI detection and classification of the Achilles tendon ultrasound images. In Proceedings of the 1st International Conference on Internet of Things and Machine Learning, Liverpool, UK, 17–18 October 2017; pp. 1–7. [Google Scholar] [CrossRef]
- Zhang, S.; Zhang, S.; Zhang, C.; Wang, X.; Shi, Y. Cucumber leaf disease identification with global pooling dilated convolutional neural network. Comput. Electron. Agric. 2019, 162, 422–430. [Google Scholar] [CrossRef]
- Yang, T.; Wu, Y.; Zhao, J.; Guan, L. Semantic segmentation via highly fused convolutional network with multiple soft cost functions. Cogn. Syst. Res. 2019, 53, 20–30. [Google Scholar] [CrossRef]
- Zeng, Y.; Chen, X.; Zhang, Y.; Bai, L.; Han, J. Dense-U-Net: Densely connected convolutional network for semantic segmentation with a small number of samples. In Proceedings of the Tenth International Conference on Graphics and Image Processing (Icgip 2018), Chengdu, China, 12–14 December 2018; p. 110692B. [Google Scholar] [CrossRef]
- Orhan, A.E.; Pitkow, X. Skip connections eliminate singularities. arXiv 2017, arXiv:1701.09175. [Google Scholar]
- Yasrab, R. SRNET: A Shallow Skip Connection Based Convolutional Neural Network Design for Resolving Singularities. J. Comput. Sci. Technol. 2019, 34, 924–938. [Google Scholar] [CrossRef]
- Wu, J.; Zhang, Y.; Wang, K.; Tang, X. Skip connection U-Net for white matter hyperintensities segmentation from MRI. IEEE Access 2019, 7, 155194–155202. [Google Scholar] [CrossRef]
- Dabiri, S.; Popuri, K.; Feliciano, E.M.C.; Caan, B.J.; Baracos, V.E.; Beg, M.F. Muscle segmentation in axial computed tomography (CT) images at the lumbar (L3) and thoracic (T4) levels for body composition analysis. Comput. Med. Imaging Graph. 2019, 75, 47–55. [Google Scholar] [CrossRef]
- Park, S.-Y.; Gifford, J.R.; Andtbacka, R.H.; Trinity, J.D.; Hyngstrom, J.R.; Garten, R.S.; Diakos, N.A.; Ives, S.J.; Dela, F.; Larsen, S. Cardiac, skeletal, and smooth muscle mitochondrial respiration: Are all mitochondria created equal? Am. J. Physiol.-Heart Circul. Physiol. 2014, 307, H346–H352. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical image Computing and Computer-Assisted Intervention (MICCAI), Munich, Germany, 5–9 October 2015; pp. 234–241. [Google Scholar]
- Bonmati, E.; Hu, Y.; Sindhwani, N.; Dietz, H.P.; D’hooge, J.; Barratt, D.; Deprest, J.; Vercauteren, T. Automatic segmentation method of pelvic floor levator hiatus in ultrasound using a self-normalizing neural network. J. Med. Imaging 2018, 5, 021206. [Google Scholar] [CrossRef]
- Anami, B.S.; Malvade, N.N.; Palaiah, S. Deep learning approach for recognition and classification of yield affecting paddy crop stresses using field images. Artif. Intell. Agric. 2020, 4, 12–20. [Google Scholar] [CrossRef]
- Lu, Y.; Yi, S.; Zeng, N.; Liu, Y.; Zhang, Y. Identification of rice diseases using deep convolutional neural networks. Neurocomputing 2017, 267, 378–384. [Google Scholar] [CrossRef]
- Ouahabi, A.; Taleb-Ahmed, A. Deep learning for real-time semantic segmentation: Application in ultrasound imaging. Pattern Recognit. Lett. 2021, 144, 27–34. [Google Scholar] [CrossRef]
- Zhou, Z.; Shin, J.Y.; Gurudu, S.R.; Gotway, M.B.; Liang, J. AFT*: Integrating active learning and transfer learning to reduce annotation efforts. arXiv 2018, arXiv:1802.00912. [Google Scholar]
- Sengupta, S.; Basak, S.; Saikia, P.; Paul, S.; Tsalavoutis, V.; Atiah, F.; Ravi, V.; Peters, A. A review of deep learning with special emphasis on architectures, applications and recent trends. Knowl.-Based Syst. 2020, 194, 105596. [Google Scholar] [CrossRef]
- Andermatt, S.; Pezold, S.; Cattin, P. Multi-dimensional gated recurrent units for the segmentation of biomedical 3D-data. In Deep Learning and Data Labeling for Medical Applications; Springer: Berlin, Germany, 2016; pp. 142–151. [Google Scholar]
- Sanford, T.H.; Zhang, L.; Harmon, S.A.; Sackett, J.; Yang, D.; Roth, H.; Xu, Z.; Kesani, D.; Mehralivand, S.; Baroni, R.H. Data Augmentation and Transfer Learning to Improve Generalizability of an Automated Prostate Segmentation Model. Am. J. Roentgenol. 2020, 215, 1403–1410. [Google Scholar] [CrossRef]
- Lashgari, E.; Liang, D.; Maoz, U. Data augmentation for deep-learning-based electroencephalography. J. Neurosci. Methods 2020, 346, 108885. [Google Scholar] [CrossRef]
- Abdalla, A.; Cen, H.; Wan, L.; Rashid, R.; Weng, H.; Zhou, W.; He, Y. Fine-tuning convolutional neural network with transfer learning for semantic segmentation of ground-level oilseed rape images in a field with high weed pressure. Comput. Electron. Agric. 2019, 167, 105091. [Google Scholar] [CrossRef]
- Swati, Z.N.K.; Zhao, Q.; Kabir, M.; Ali, F.; Ali, Z.; Ahmed, S.; Lu, J. Brain tumor classification for MR images using transfer learning and fine-tuning. Comput. Med. Imaging Graph. 2019, 75, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Yan, R.; Wang, J.; Mao, K. Learning to monitor machine health with convolutional bi-directional LSTM networks. Sensors 2017, 17, 273. [Google Scholar] [CrossRef] [PubMed]
- Jang, B.; Kim, M.; Harerimana, G.; Kang, S.-U.; Kim, J.W. Bi-LSTM model to increase accuracy in text classification: Combining Word2vec CNN and attention mechanism. Appl. Sci. 2020, 10, 5841. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Muscle Type | Deep Learning Method | Citation | Purpose | Method | Dataset (Images) | Output | Image Solution |
|---|---|---|---|---|---|---|---|
| Skeletal | Segmentation | Chen et al., 2019 [34] | Cross-sectional area Rectus femoris | CNN | 81,600 | Dice: 0.90 ± 0.02 Precision: 0.93 ± 0.02 Recall: 0.88 ± 0.04 | 180° rotation |
| Segmentation | Cunningham et al., 2018 [33] | Fiber orientation in medial gastrocnemius and soleus | DCNN | 1008 | MD 3.27° ± 10. MAE 10° ± 8.09° RMSE 10.62° | −5° +5° rotation | |
| Segmentation | Zhou et al., 2020 [36] | Tracking the myotendinous junction in the gastrocnemius | RAN | 300 | Dice 80.1% | Transfer Learning | |
| Segmentation | Loram et al., 2020 [35] | Objective visualization and pattern analysis neck muscle | U-Net | 3272 | Dice 64 ± 21% HD 5.7 ± 4.0 mm Precision 94 ± 3% | −8° +8° rotation | |
| Classification | Xu et al., 2020 [31] | Gender classification in the tibialis anterior area | CNN (VGG-16) | 115,916 | Accuracy: VGG-16 95.2% (Alex Net 83.3% Google Net 84.4%) | 4 Random rotation angles and flipping | |
| Classification | Katakis et al., 2018 [30] | Muscle type of the rectus femoris, tibialis anterior, gastrocnemius medialis and bicep brachii | Deep-CNN (VGG-F) | 300 | Accuracy: VGG-F 89.4% (VGG-16 87.5%, VGG-19 87.2%) | Transfer learning | |
| Classification | Tsai et al., 2020 [32] | Bicep vibration muscle | CNN (AlexNet) | 120,423 | Accuracy: AlexNet 82.5% (VGG-16 79.9%, VGG-19 79.7%) | 45° rotation, flipping, adjust contrast | |
| Smooth | Segmentation | Minhaz et al., 2020 [39] | 3D assessment ciliary muscle | U-Net | 1000 | Dice 0.72 ± 0.070 Accuracy 0.93 ± 0.010 Sensitivity 0.79 ± 0.070 | No |
| Segmentation | van den Noort et al., 2019 [37] | Area measurement in urogenital hiatus and puborectalis muscle | CNN | 713 | Dice 0.94 ± 0.020 and 0.73 ± 0.090 | No | |
| Segmentation | Akkus et al., 2020 [38] | Fully automated segmentation Bladder wall thickness. | U-Net | 800 | Dice 0.93 ± 0.040 mm RMSE 0.70 ± 0.20 mm | 10 times random elastic deformation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ardhianto, P.; Tsai, J.-Y.; Lin, C.-Y.; Liau, B.-Y.; Jan, Y.-K.; Akbari, V.B.H.; Lung, C.-W. A Review of the Challenges in Deep Learning for Skeletal and Smooth Muscle Ultrasound Images. Appl. Sci. 2021, 11, 4021. https://doi.org/10.3390/app11094021
Ardhianto P, Tsai J-Y, Lin C-Y, Liau B-Y, Jan Y-K, Akbari VBH, Lung C-W. A Review of the Challenges in Deep Learning for Skeletal and Smooth Muscle Ultrasound Images. Applied Sciences. 2021; 11(9):4021. https://doi.org/10.3390/app11094021
Chicago/Turabian StyleArdhianto, Peter, Jen-Yung Tsai, Chih-Yang Lin, Ben-Yi Liau, Yih-Kuen Jan, Veit Babak Hamun Akbari, and Chi-Wen Lung. 2021. "A Review of the Challenges in Deep Learning for Skeletal and Smooth Muscle Ultrasound Images" Applied Sciences 11, no. 9: 4021. https://doi.org/10.3390/app11094021
APA StyleArdhianto, P., Tsai, J.-Y., Lin, C.-Y., Liau, B.-Y., Jan, Y.-K., Akbari, V. B. H., & Lung, C.-W. (2021). A Review of the Challenges in Deep Learning for Skeletal and Smooth Muscle Ultrasound Images. Applied Sciences, 11(9), 4021. https://doi.org/10.3390/app11094021