
A Novel Magnetic Respiratory Sensor for Human Healthcare

 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
Featured Application
Abstract
1. Introduction
2. Materials and Methods
3. Results and Discussion
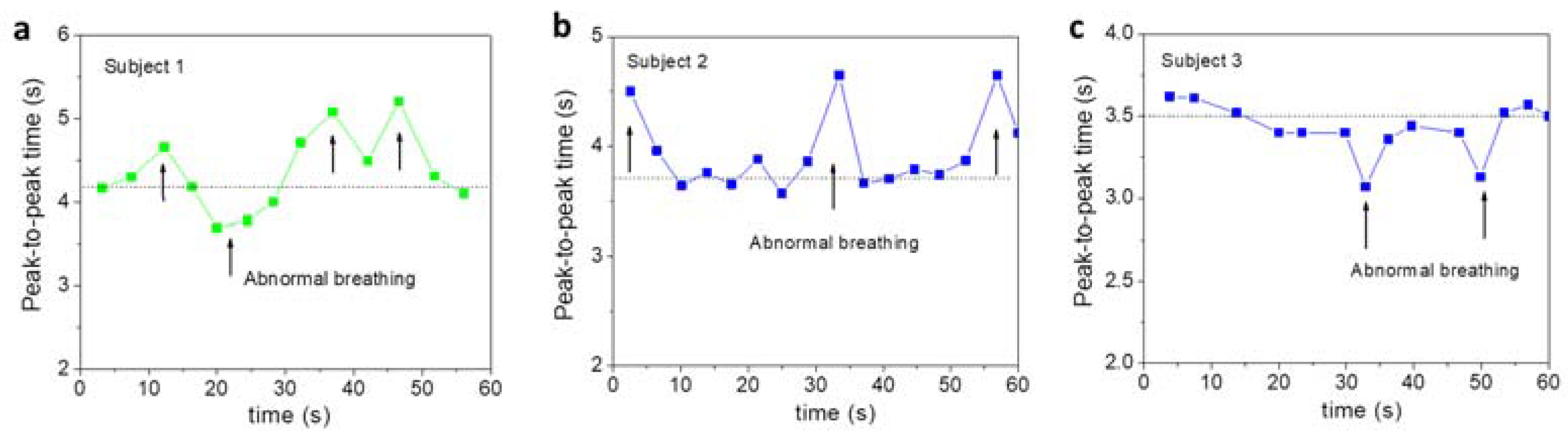
3.1. Real-Time Monitoring of Human Respiratory Motion at Different Ages
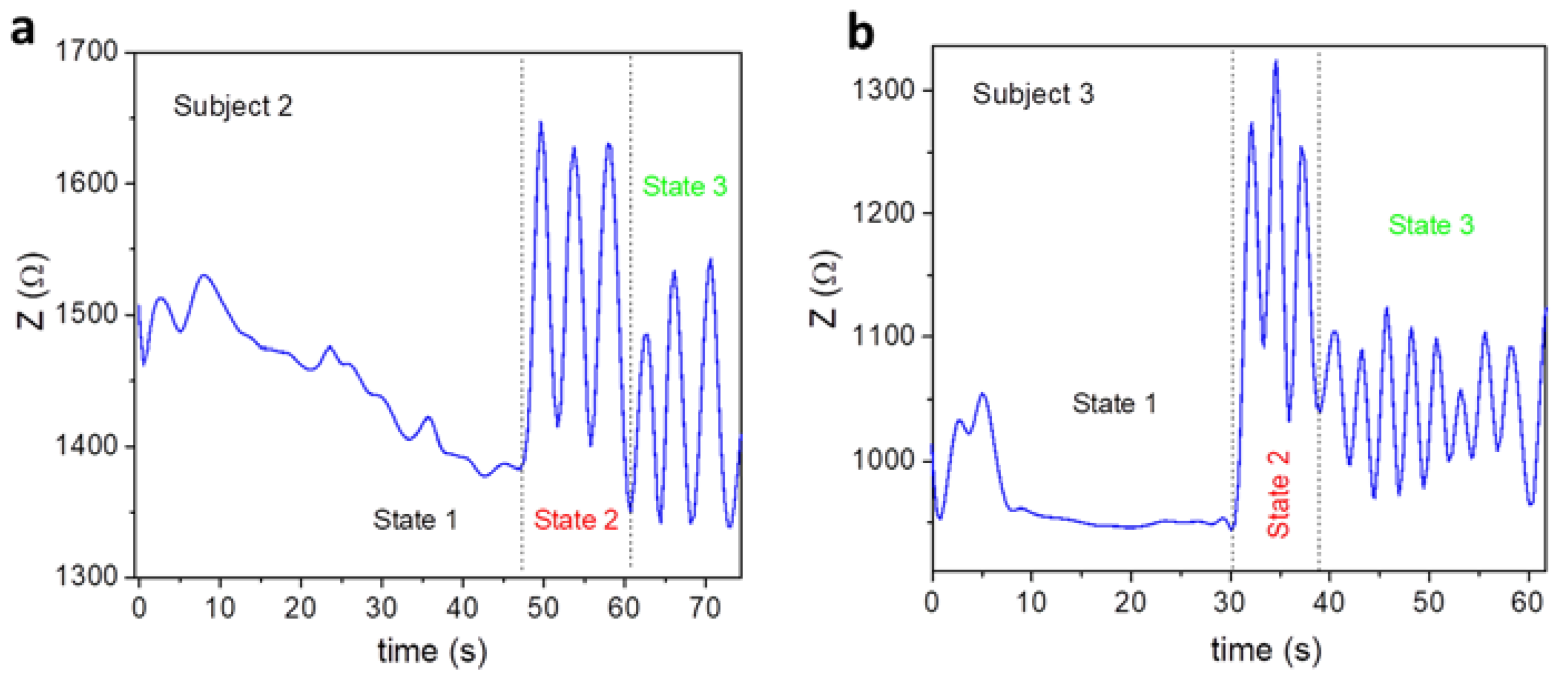
3.2. Real-Time Monitoring of Human Respiratory Motion in Multiple Breathing States
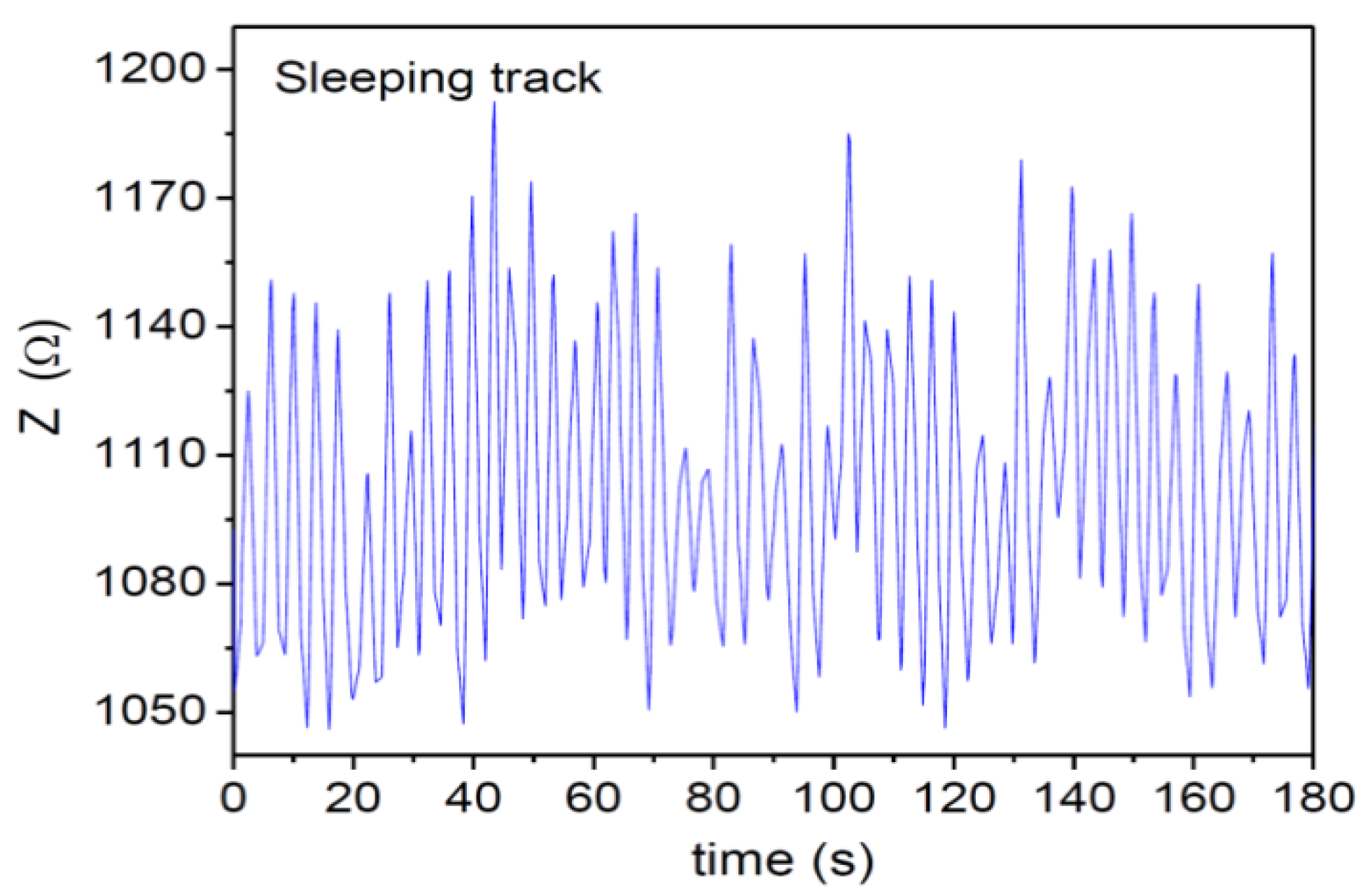
3.3. Real-Time Monitoring of Human Respiratory Motion in Wake-Up and Sleep Modes
4. Conclusions and Future Outlooks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lou, Z.; Wang, L.; Jiang, K.; Wei, Z.M.; Shen, G.Z. Reviews of wearable healthcare systems: Materials, devices and system integration. Mater. Sci. Eng. R Rep. 2020, 140, 100523. [Google Scholar] [CrossRef]
- Shaw-Taylor, L. An introduction to the history of infectious diseases, epidemics and the early phases of the long-run decline in mortality. Econ. Hist. Rev. 2020, 73, 19. [Google Scholar] [CrossRef] [PubMed]
- Walls, A.C.; Park, Y.-J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, Function, and Antigenicity of the SARSCoV-2 Spike Glycoprotein. Cell 2020, 181, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A Pneumonia Outbreak Associated with a New coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef]
- Kumar, D.; Manuel, O.; Natori, Y.; Egawa, H.; Grossi, P.; Han, S.-H.; Fernandez-Ruiz, M.; Humar, A. COVID-19: A Global Transplant Perspective on Successfully Navigating a Pandemic. Am. J. Transplant. 2020, 27, 1773–1779. [Google Scholar] [CrossRef] [PubMed]
- Spackman, E.; Senne, D.A.; Myers, T.J.; Bulaga, L.L.; Garber, L.P.; Perdue, M.L.; Lohman, K.; Daum, L.T.; Suarez, D.L. Development of a Real-Time Reverse Transcriptase PCR Assay for Type A Influenza Virus and the Avian H5 and H7 Hemagglutinin Subtypes. J. Clin. Microbiol. 2002, 40, 3256–3260. [Google Scholar] [CrossRef]
- Wu, J.; Liu, J.; Li, S.; Peng, Z.; Xiao, Z.; Wang, X.; Yan, R.; Luo, J. Detection and Analysis of Nucleic Acid in Various Biological Samples of COVID-19 Patients. Travel Med. Infect. Dis. 2020, 37, 101673. [Google Scholar] [CrossRef]
- Marras, S.A. Selection of Fluorophore and Quencher Pairs for Fluorescent Nucleic Acid Hybridization Probes. Methods Mol. Biol. 2006, 335, 3–16. [Google Scholar] [PubMed]
- Seo, G.; Lee, G.; Kim, M.J.; Baek, S.-H.; Choi, M.; Ku, K.B.; Lee, C.-S.; Jun, S.; Park, D.; Kim, H.G.; et al. Detection of COVID-19 Causative Virus (SARS-CoV-2) in Human Nasopharyngeal Swab Specimens Using Field-Effect Transistor-Based Biosensor. ACS Nano 2020, 14, 5135–5142. [Google Scholar] [CrossRef] [PubMed]
- Maier, S.A. Plasmonics: Fundamentals and Applications; Springer Science & Business Media: New York, NY, USA, 2007; pp. 6–10. [Google Scholar]
- Ligler, F.S.; Breimer, M.; Golden, J.P.; Nivens, D.A.; Dodson, J.P.; Green, T.M.; Haders, D.P.; Sadik, O.A. Integrating Waveguide Biosensor. Anal. Chem. 2002, 74, 713–719. [Google Scholar] [CrossRef] [PubMed]
- To, K.K.-W.; Tsang, O.T.-Y.; Leung, W.-S.; Tam, A.R.; Wu, T.-C.; Lung, D.C.; Yip, C.; Cai, J.-P.; Chan, J.M.-C.; Chik, T.S.-H.; et al. Temporal Profiles of Viral Load in Posterior Oropharyngeal Saliva Samples and Serum Antibody Responses During Infection by SARS-CoV-2: An Observational Cohort Study. Lancet Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef]
- Bhalla, N.; Pan, Y.; Yang, Z.; Farokh Payam, A. Opportunities and Challenges for Biosensors and Nanoscale Analytical Tools for Pandemics: COVID-19. ACS Nano 2020, 14, 7783–7807. [Google Scholar] [CrossRef] [PubMed]
- Medhi, R.; Srinoi, P.; Ngo, N.; Tran, H.V.; Lee, T.R. Nanoparticle-Based Strategies to Combat COVID-19. ACS Appl. Nano Mater. 2020, 3, 8557–8580. [Google Scholar] [CrossRef]
- Braun, S.R. Respiratory rate and pattern. In Clinical Method: The History, Physical, and Laboratory Examinations, 4th ed.; Walker, H.K., Hall, W.D., Hurst, J.W., Eds.; Butterworths: Boston, MA, USA, 1990; pp. 226–230. [Google Scholar]
- Hess, D.R.; MacIntyre, N.R.; Galvin, W.F. Respiratory Care: Principles and Practice, 3rd ed.; Jones & Bartlett Learning: Burlington, MA, USA, 2016. [Google Scholar]
- Liu, H.P.; Allen, J.; Zheng, D.C.; Chen, F. Recent development of respiratory rate measurement technologies. Phys. Meas. 2019, 40, 07TR01. [Google Scholar] [CrossRef] [PubMed]
- Phan, M.H.; Peng, H.X. Giant magnetoimpedance materials: Fundamentals and applications. Prog. Mater. Sci. 2008, 53, 323–420. [Google Scholar] [CrossRef]
- Thiabgoh, O.; Eggers, T.; Phan, M.H. A new contactless magneto-LC resonance technology for real-time respiratory motion monitoring. Sens. Actuators A 2017, 265, 120–126. [Google Scholar] [CrossRef]
- Jimenez, V.O.; Kalappattil, V.; Eggers, T.; Bonilla, M.; Kolekar, S.; Huy, P.T.; Batzill, M.; Phan, M.H. A magnetic sensor using a 2D van der Waals ferromagnetic material. Sci. Rep. 2020, 10, 4789. [Google Scholar] [CrossRef]
- Fekr, A.R.; Janidarmian, M.; Radecka, K.; Zilic, Z. A medical cloud-based platform for respiration rate measurement and hierarchical classification of breath disorders. Sensors 2014, 14, 11204–11224. [Google Scholar] [CrossRef]
- Al-Khalidi, F.Q.; Saatchi, R.; Burke, D.; Elphick, H.; Tan, S. Respiration rate monitoring methods: A review. Pediatr. Pulmonol. 2011, 46, 523–529. [Google Scholar] [CrossRef]
- Padasdao, B.; Shahhaidar, E.; Stickley, C.; Boric-Lubecke, O. Electromagnetic biosensing of respiratory rate. IEEE Sens. J. 2013, 13, 4204–4211. [Google Scholar] [CrossRef]
- Battista, L. A new system for continuous and remote monitoring of patients receiving home mechanical ventilation. Rev. Sci. Instrum. 2016, 87, 095105. [Google Scholar] [CrossRef]
- Min, S.D.; Kim, J.K.; Shin, H.S.; Yun, Y.H.; Lee, C.K.; Lee, M. Noncontact respiration rate measurement system using an ultrasonic proximity sensor. IEEE Sens. J. 2010, 10, 1732–1739. [Google Scholar]
- Daiana da Costa, T.; de Fatima Fernandes Vara, M.; Santos Cristino, C.; Zoraski Zanella, T.; Nunes Nogueira Neto, G.; Nohama, P. Breathing Monitoring and Pattern Recognition with Wearable Sensors. In Wearable Devices: The Big Wave of Innovation; Nasiri, N., Ed.; IntechOpen: London, UK, 2019. [Google Scholar]
- Kelley, S.D.; Ramsay, M.A.E. Respiratory rate monitoring: Characterizing performance for emerging technologies. Anesth. Analg. 2014, 119, 1246–1248. [Google Scholar] [CrossRef]
- Skow, R.J.; Day, T.A.; Fuller, J.E.; Bruce, C.D.; Steinback, C.D. The ins and outs of breath holding: Simple demonstrations of complex respiratory physiology. Adv. Physiol. Educ. 2015, 39, 223–231. [Google Scholar] [CrossRef]
- Ocampo, A.; Carlos Izpisua Belmonte, J. SIRT7 and Stem Cell Aging: Holding Your Breath for Longevity. Science 2015, 347, 1319–1320. [Google Scholar] [CrossRef] [PubMed]
- American Sleep Association. Available online: https://www.sleepassociation.org/ (accessed on 1 December 2020).
- Shan, B.; Broza, Y.Y.; Li, W.; Wang, Y.; Wu, S.; Liu, Z.Z.; Wang, J.; Gui, S.; Wang, L.; Zhang, Z.H.; et al. Multiplexed Nanomaterial-Based Sensor Array for Detection of COVID-19 in Exhaled Breath. ACS Nano 2020, 14, 12125–12132. [Google Scholar] [CrossRef]
- Funari, R.; Chu, K.Y.; Shen, A.Q. Detection of antibodies against SARS-CoV-2 spike protein by gold nanospikes in an opto-microfluidic chip. Biosens. Bioelectr. 2020, 169, 112578. [Google Scholar] [CrossRef]
- Lim, R.R.X.; Bonanni, A. The potential of electrochemistry for the detection of coronavirus-induced infections. TrAC Trends Anal. Chem. 2020, 133, 116081. [Google Scholar] [CrossRef] [PubMed]
- Fani, M.; Zandi, M.; Soltani, S.; Abbasi, S. Future developments in biosensors for field-ready SARS-CoV-2 virus diagnostics. Biotech. Appl. Biochem. 2020. [Google Scholar] [CrossRef] [PubMed]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, K.Y.; Jimenez, V.O.; Muchharla, B.; Eggers, T.; Le, A.-T.; Lam, V.D.; Phan, M.-H. A Novel Magnetic Respiratory Sensor for Human Healthcare. Appl. Sci. 2021, 11, 3585. https://doi.org/10.3390/app11083585
Hwang KY, Jimenez VO, Muchharla B, Eggers T, Le A-T, Lam VD, Phan M-H. A Novel Magnetic Respiratory Sensor for Human Healthcare. Applied Sciences. 2021; 11(8):3585. https://doi.org/10.3390/app11083585
Chicago/Turabian StyleHwang, Kee Young, Valery Ortiz Jimenez, Baleeswaraiah Muchharla, Tatiana Eggers, Anh-Tuan Le, Vu Dinh Lam, and Manh-Huong Phan. 2021. "A Novel Magnetic Respiratory Sensor for Human Healthcare" Applied Sciences 11, no. 8: 3585. https://doi.org/10.3390/app11083585
APA StyleHwang, K. Y., Jimenez, V. O., Muchharla, B., Eggers, T., Le, A.-T., Lam, V. D., & Phan, M.-H. (2021). A Novel Magnetic Respiratory Sensor for Human Healthcare. Applied Sciences, 11(8), 3585. https://doi.org/10.3390/app11083585