
Ultrasound-Guided Procedures in Common Tendinopathies at the Elbow: From Image to Needle

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
3. Common Elbow Pathologies
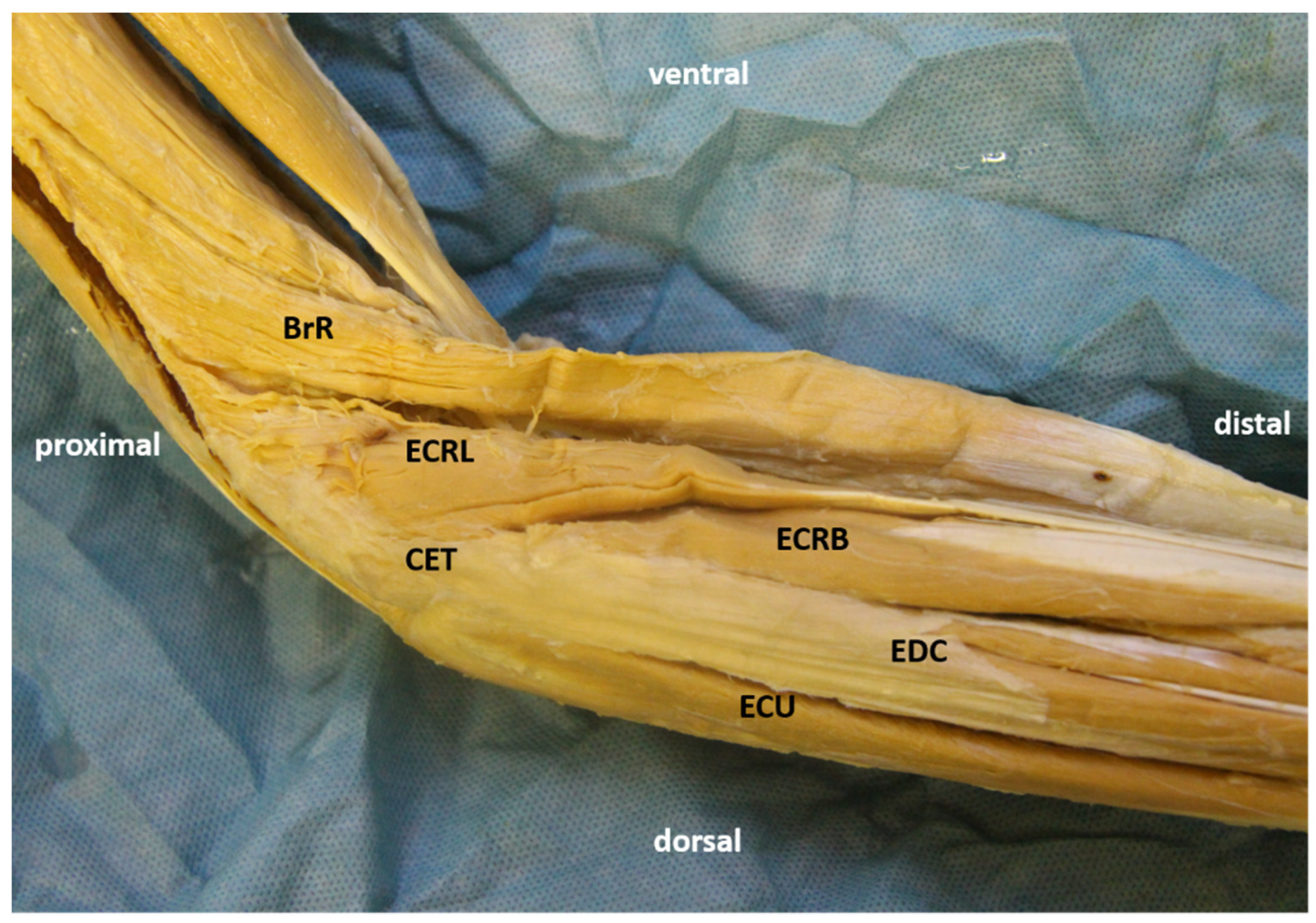
3.1. Tennis Elbow
3.1.1. Essential Anatomy
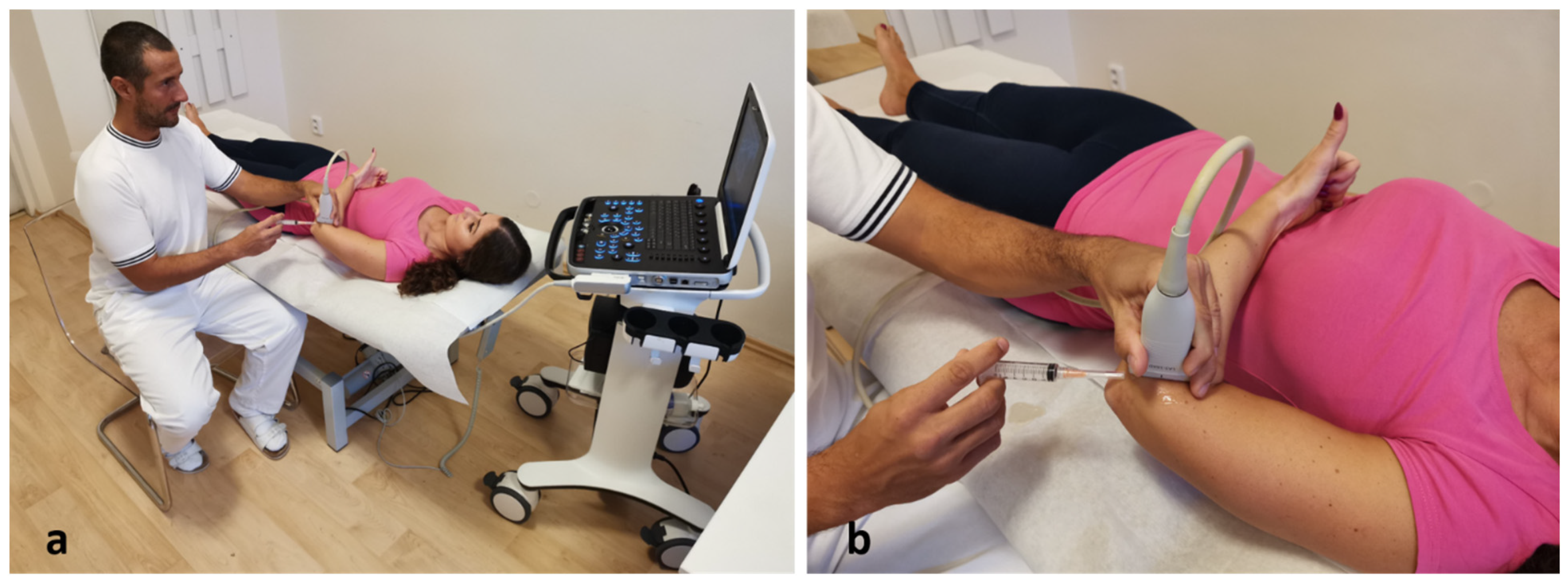
3.1.2. US scanning and Guided Injection
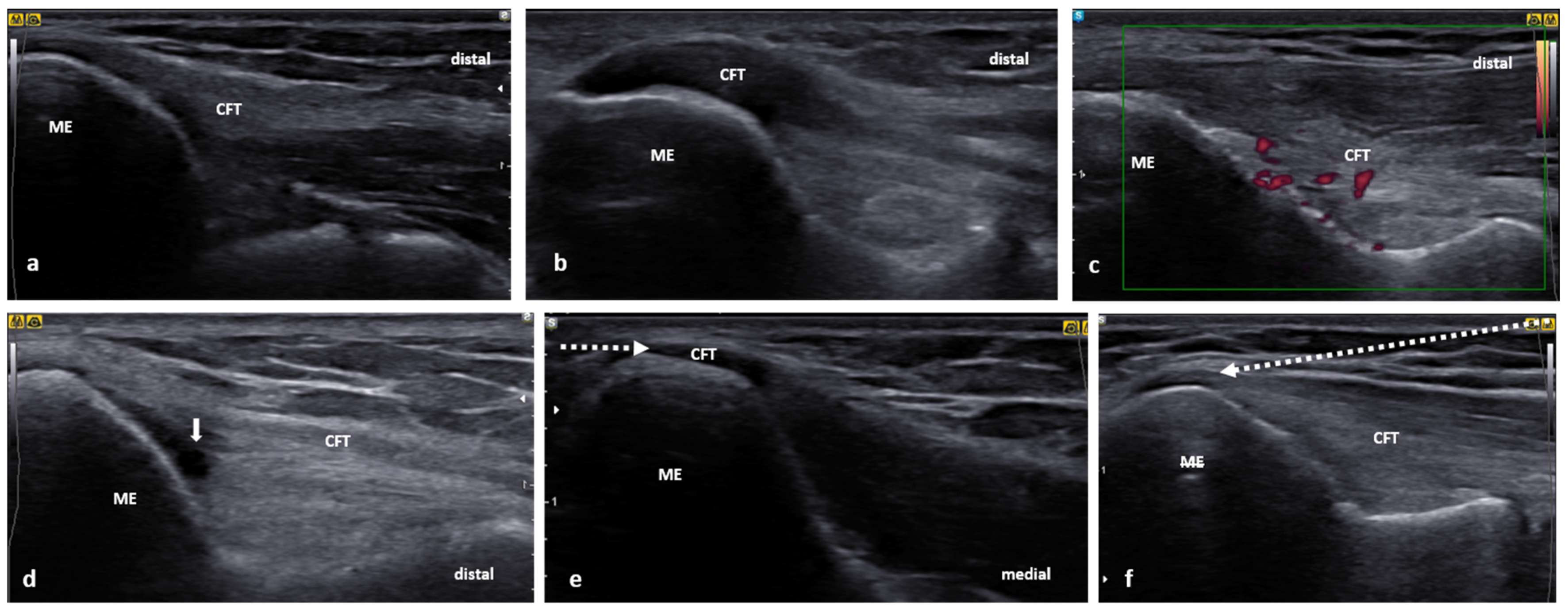
3.2. Golfer’s Elbow
3.2.1. Essential Anatomy
3.2.2. US scanning and Guided Injection
3.3. Distal Biceps Tendinopathy
3.3.1. Essential Anatomy
3.3.2. US Scanning and Guided Injection
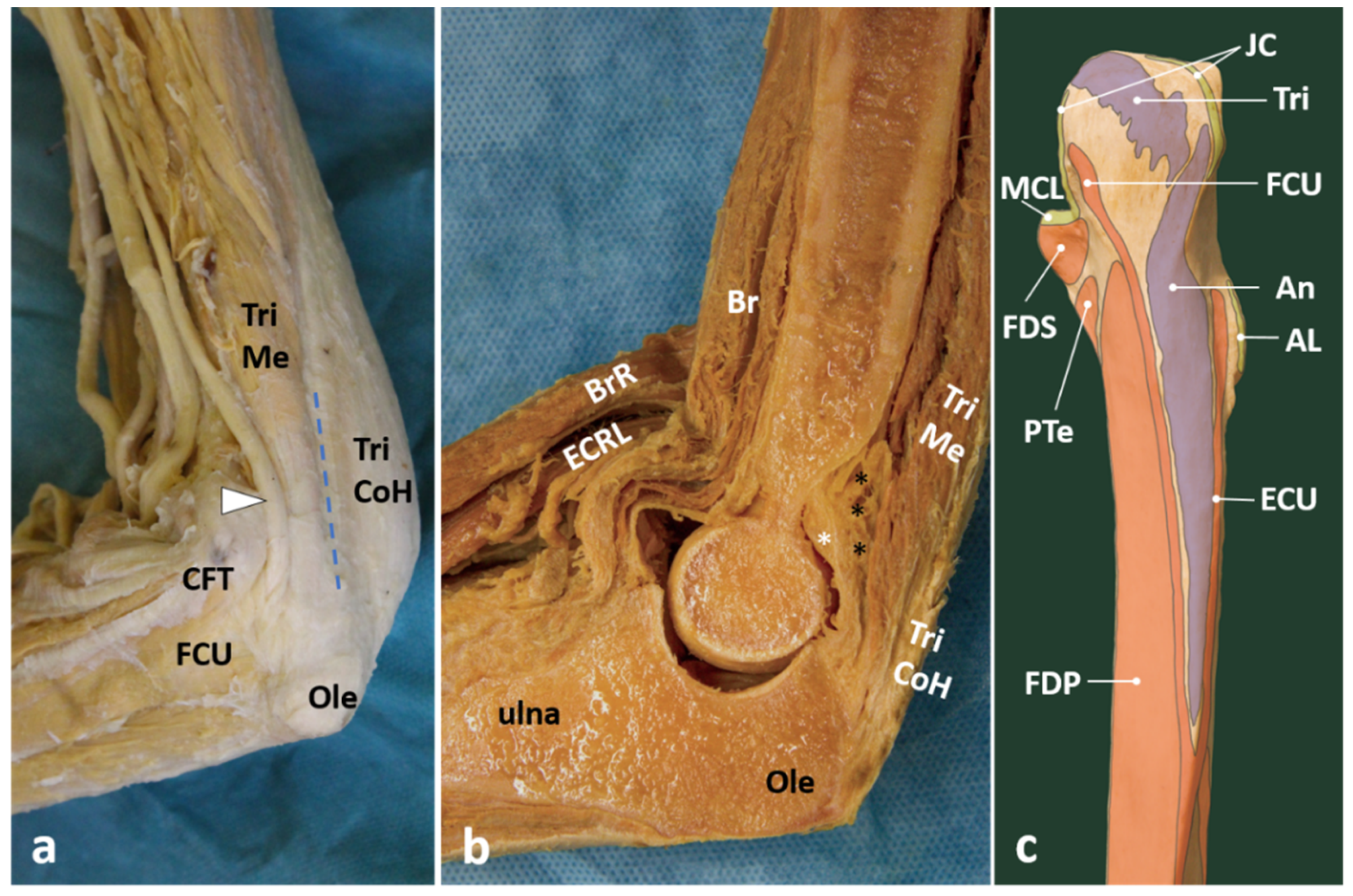
3.4. Distal Triceps Tendinopathy
3.4.1. Essential Anatomy
3.4.2. US Scanning and Guided Injection
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shiri, R.; Viikari-Juntura, E. Lateral and medial epicondylitis: Role of occupational factors. Best Pract. Res. Clin. Rheumatol. 2011, 25, 43–57. [Google Scholar] [CrossRef]
- Nirschl, R.P. Tennis elbow. Orthop. Clin. N. Am. 1973, 4, 787–800. [Google Scholar] [CrossRef]
- Bishai, S.; Plancher, K. The Basic Science of Lateral Epicondylosis: Update for the Future. Tech. Orthop. 2006, 4, 250–255. [Google Scholar] [CrossRef]
- Kannus, P.; Józsa, L. Histopathological changes preceding spontaneous rupture of a tendon. A controlled study of 891 patients. J. Bone Jt. Surg. Am. 1991, 73, 1507–1525. [Google Scholar] [CrossRef]
- Kraushaar, B.S.; Nirschl, R.P. Tendinosis of the elbow (tennis elbow). Clinical features and findings of histological, immunohistochemical, and electron microscopy studies. J. Bone Jt. Surg. Am. 1999, 81, 259–278. [Google Scholar] [CrossRef]
- Nirschl, R.; Alvarado, G. Tennis elbow tendinosis: Pathoanatomy, nonsurgical and surgical management. In Repetitive Motion Disorders of the Upper Extremity; American Academy of Orthopaedic Surgeons, Rosemont: Rosemont, IL, USA, 1995; pp. 467–479. [Google Scholar]
- Patterson-Kane, J.C.; Becker, D.L.; Rich, T. The pathogenesis of tendon microdamage in athletes: The horse as a natural model for basic cellular research. J. Comp. Pathol. 2012, 147, 227–247. [Google Scholar] [CrossRef] [PubMed]
- Kannus, P. Etiology and pathophysiology of chronic tendon disorders in sports. Scand. J. Med. Sci. Sports 1997, 7, 78–85. [Google Scholar] [CrossRef]
- Coombes, B.K.; Bisset, L.; Vicenzino, B. A new integrative model of lateral epicondylalgia. Br. J. Sports Med. 2009, 43, 252–258. [Google Scholar] [CrossRef]
- Boushel, R.; Langberg, H.; Green, S.; Skovgaard, D.; Bulow, J.; Kjaer, M. Blood flow and oxygenation in peritendinous tissue and calf muscle during dynamic exercise in humans. J. Physiol. 2000, 524 Pt 1, 305–313. [Google Scholar] [CrossRef]
- Kane, S.F.; Lynch, J.H.; Taylor, J.C. Evaluation of elbow pain in adults. Am. Fam. Phys. 2014, 89, 649–657. [Google Scholar]
- Kryger, A.I.; Lassen, C.F.; Andersen, J.H. The role of physical examinations in studies of musculoskeletal disorders of the elbow. Occup. Environ. Med. 2007, 64, 776–781. [Google Scholar] [CrossRef]
- Zwerus, E.L.; Somford, M.P.; Maissan, F.; Heisen, J.; Eygendaal, D.; van den Bekerom, M.P. Physical examination of the elbow, what is the evidence? A systematic literature review. Br. J. Sports Med. 2018, 52, 1253–1260. [Google Scholar] [CrossRef]
- Özçakar, L.; Muynck, M.D. Musculoskeletal Ultrasound in Physical Rehabilitation Medicine; Edi Ermes: Milan, Italy, 2014; ISBN 978-88-7051-420-9. [Google Scholar]
- Özçakar, L. Sonographic Atlas for Common Musculoskeletal Pathologies; Edi Ermes: Milan, Italy, 2017; ISBN 978-88-7051-576-3. [Google Scholar]
- Kara, M.; Gürçay, E.; Ekiz, T.; Sekizkardeş, M.; Yorulmaz, E.; Ata, A.M.; Chang, K.-V.; Wu, W.-T.; Akkaya, N.; Mezian, K.; et al. EURO-MUSCULUS/USPRM Global Report on Musculoskeletal Ultrasound Publications. Am. J. Phys. Med. Rehabil. 2020, 99, 847–852. [Google Scholar] [CrossRef] [PubMed]
- Jačisko, J.; Sobotová, K.; Mezian, K. The utility of ultrasound examination in cubital tunnel syndrome caused by heterotopic ossification. Med. Ultrason. 2020, 22, 117–118. [Google Scholar] [CrossRef]
- Özçakar, L. Ultrasound Imaging & Guidance for Musculoskeletal Interventions in Physical and Rehabilitation Medicine; Edi Ermes: Milan, Italy, 2019; ISBN 978-88-7051-698-2. [Google Scholar]
- Mezian, K.; Machač, S.; Zavareh, A.; Majerníková, L.; Vacek, J.; Navrátil, L.; Schmitz, M. Positioning Techniques to Improve the Ultrasound Evaluation of the Elbow. Ultrasound Q. 2019, 35, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Mezian, K.; Sobotová, K.; Angerová, Y. Sonographic elbow scanning is not yoga exercise. Adv. Rheumatol. 2019, 59, 33. [Google Scholar] [CrossRef] [PubMed]
- Özçakar, L.; Kara, M.; Chang, K.V.; Hung, C.Y.; Tekın, L.; Ulaşlı, A.M.; Wu, C.H.; Tok, F.; Hsıao, M.Y.; Akkaya, N.; et al. EURO-MUSCULUS/USPRM Basic Scanning Protocols for elbow. Eur. J. Phys. Rehabil. Med. 2015, 51, 485–489. [Google Scholar] [PubMed]
- Cutts, S.; Gangoo, S.; Modi, N.; Pasapula, C. Tennis elbow: A clinical review article. J. Orthop. 2020, 17, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Eygendaal, D.; Rahussen, F.T.G.; Diercks, R.L. Biomechanics of the elbow joint in tennis players and relation to pathology. Br. J. Sports Med. 2007, 41, 820–823. [Google Scholar] [CrossRef] [PubMed]
- Walz, D.M.; Newman, J.S.; Konin, G.P.; Ross, G. Epicondylitis: Pathogenesis, imaging, and treatment. Radiographics 2010, 30, 167–184. [Google Scholar] [CrossRef]
- Sanders, T.L.; Maradit Kremers, H.; Bryan, A.J.; Ransom, J.E.; Smith, J.; Morrey, B.F. The epidemiology and health care burden of tennis elbow: A population-based study. Am. J. Sports Med. 2015, 43, 1066–1071. [Google Scholar] [CrossRef]
- Allander, E. Prevalence, incidence, and remission rates of some common rheumatic diseases or syndromes. Scand. J. Rheumatol. 1974, 3, 145–153. [Google Scholar] [CrossRef]
- Bot, S.D.M.; van der Waal, J.M.; Terwee, C.B.; van der Windt, D.A.W.M.; Bouter, L.M.; Dekker, J. Course and prognosis of elbow complaints: A cohort study in general practice. Ann. Rheum. Dis. 2005, 64, 1331–1336. [Google Scholar] [CrossRef]
- Shiri, R.; Viikari-Juntura, E.; Varonen, H.; Heliövaara, M. Prevalence and determinants of lateral and medial epicondylitis: A population study. Am. J. Epidemiol. 2006, 164, 1065–1074. [Google Scholar] [CrossRef] [PubMed]
- Keijsers, R.; de Vos, R.-J.; Kuijer, P.P.F.; van den Bekerom, M.P.; van der Woude, H.-J.; Eygendaal, D. Tennis elbow. Shoulder Elb. 2019, 11, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Nayak, S.R.; Ramanathan, L.; Krishnamurthy, A.; Prabhu, L.V.; Madhyastha, S.; Potu, B.K.; Ranade, A.V. Extensor carpi radialis brevis origin, nerve supply and its role in lateral epicondylitis. Surg. Radiol. Anat. 2010, 32, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Greenbaum, B.; Itamura, J.; Vangsness, C.T.; Tibone, J.; Atkinson, R. Extensor carpi radialis brevis. An anatomical analysis of its origin. J. Bone Jt. Surg. Br. 1999, 81, 926–929. [Google Scholar] [CrossRef]
- Albright, J.A.; Linburg, R.M. Common variations of the radial writs extensors. J. Hand Surg. Am. 1978, 3, 134–138. [Google Scholar] [CrossRef]
- Standring, S. Gray’s Anatomy. The Anatomical Basis of Clinical Practice, 41st ed.; Churchill Livingstone/Elsevier: Edinburgh, UK, 2015. [Google Scholar]
- Boyer, M.I.; Hastings, H. Lateral tennis elbow: “Is there any science out there?”. J. Shoulder Elb. Surg. 1999, 8, 481–491. [Google Scholar] [CrossRef]
- Ricci, V.; Schroeder, A.; Özçakar, L. Ultrasound Imaging for Lateral Elbow Pain: Pinpointing the Epicondylosis. Am. J. Phys. Med. Rehabil. 2020, 99, 560–561. [Google Scholar] [CrossRef]
- Ricci, V.; Mezian, K.; Özçakar, L. Contemporary/Ultrasound Guidance for Musculoskeletal Interventions: Let Bygones be Bygones. Am. J. Phys. Med. Rehabil. 2021. [Google Scholar] [CrossRef] [PubMed]
- Pirri, C.; Stecco, C.; De Caro, R.; Foti, C.; Özçakar, L. Radiating Upper Limb Pain Due to a Large Subcutaneous Lipoma: Fascial Sono-Palpation. Pain Med. 2020, 21, 3721–3723. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, O.; Vannet, N.; Gosens, T.; Kulkarni, R. Tendinopathies Around the Elbow Part 2: Medial Elbow, Distal Biceps and Triceps Tendinopathies. Shoulder Elb. 2014, 6, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Sayegh, E.T.; Strauch, R.J. Does nonsurgical treatment improve longitudinal outcomes of lateral epicondylitis over no treatment? A meta-analysis. Clin. Orthop. Relat. Res. 2015, 473, 1093–1107. [Google Scholar] [CrossRef]
- Uygur, E.; Aktaş, B.; Özkut, A.; Erinç, S.; Yilmazoglu, E.G. Dry needling in lateral epicondylitis: A prospective controlled study. Int. Orthop. 2017, 41, 2321–2325. [Google Scholar] [CrossRef] [PubMed]
- Acosta-Olivo, C.A.; Millán-Alanís, J.M.; Simental-Mendía, L.E.; Álvarez-Villalobos, N.; Vilchez-Cavazos, F.; Peña-Martínez, V.M.; Simental-Mendía, M. Effect of Normal Saline Injections on Lateral Epicondylitis Symptoms: A Systematic Review and Meta-analysis of Randomized Clinical Trials. Am. J. Sports Med. 2020, 48, 3094–3102. [Google Scholar] [CrossRef]
- Gao, B.; Dwivedi, S.; DeFroda, S.; Bokshan, S.; Ready, L.V.; Cole, B.J.; Owens, B.D. The Therapeutic Benefits of Saline Solution Injection for Lateral Epicondylitis: A Meta-analysis of Randomized Controlled Trials Comparing Saline Injections With Nonsurgical Injection Therapies. Arthroscopy 2019, 35, 1847–1859. [Google Scholar] [CrossRef]
- Xiong, Y.; Xue, H.; Zhou, W.; Sun, Y.; Liu, Y.; Wu, Q.; Liu, J.; Hu, L.; Panayi, A.C.; Chen, L.; et al. Shock-wave therapy versus corticosteroid injection on lateral epicondylitis: A meta-analysis of randomized controlled trials. Phys. Sportsmed. 2019, 47, 284–289. [Google Scholar] [CrossRef]
- Simental-Mendía, M.; Vilchez-Cavazos, F.; Álvarez-Villalobos, N.; Blázquez-Saldaña, J.; Peña-Martínez, V.; Villarreal-Villarreal, G.; Acosta-Olivo, C. Clinical efficacy of platelet-rich plasma in the treatment of lateral epicondylitis: A systematic review and meta-analysis of randomized placebo-controlled clinical trials. Clin. Rheumatol. 2020, 39, 2255–2265. [Google Scholar] [CrossRef]
- Huang, K.; Giddins, G.; Wu, L.-D. Platelet-Rich Plasma Versus Corticosteroid Injections in the Management of Elbow Epicondylitis and Plantar Fasciitis: An Updated Systematic Review and Meta-analysis. Am. J. Sports Med. 2020, 48, 2572–2585. [Google Scholar] [CrossRef]
- Xu, Q.; Chen, J.; Cheng, L. Comparison of platelet rich plasma and corticosteroids in the management of lateral epicondylitis: A meta-analysis of randomized controlled trials. Int. J. Surg. 2019, 67, 37–46. [Google Scholar] [CrossRef]
- Li, A.; Wang, H.; Yu, Z.; Zhang, G.; Feng, S.; Liu, L.; Gao, Y. Platelet-rich plasma vs corticosteroids for elbow epicondylitis: A systematic review and meta-analysis. Medicine 2019, 98, e18358. [Google Scholar] [CrossRef]
- Mi, B.; Liu, G.; Zhou, W.; Lv, H.; Liu, Y.; Wu, Q.; Liu, J. Platelet rich plasma versus steroid on lateral epicondylitis: Meta-analysis of randomized clinical trials. Phys. Sportsmed. 2017, 45, 97–104. [Google Scholar] [CrossRef]
- Chou, L.-C.; Liou, T.-H.; Kuan, Y.-C.; Huang, Y.-H.; Chen, H.-C. Autologous blood injection for treatment of lateral epicondylosis: A meta-analysis of randomized controlled trials. Phys. Ther. Sport 2016, 18, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Arirachakaran, A.; Sukthuayat, A.; Sisayanarane, T.; Laoratanavoraphong, S.; Kanchanatawan, W.; Kongtharvonskul, J. Platelet-rich plasma versus autologous blood versus steroid injection in lateral epicondylitis: Systematic review and network meta-analysis. J. Orthop. Traumatol. 2016, 17, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, L.; Bannuru, R.R.; Severin, M.; Harvey, W. Injection of botulinum toxin for treatment of chronic lateral epicondylitis: Systematic review and meta-analysis. Semin. Arthritis Rheum. 2011, 40, 532–538. [Google Scholar] [CrossRef]
- David, T.S. Medial elbow pain in the throwing athlete. Orthopedics 2003, 26, 94–103, quiz 104–105. [Google Scholar]
- Wolf, J.M.; Mountcastle, S.; Burks, R.; Sturdivant, R.X.; Owens, B.D. Epidemiology of lateral and medial epicondylitis in a military population. Mil. Med. 2010, 175, 336–339. [Google Scholar] [CrossRef]
- Taylor, S.A.; Hannafin, J.A. Evaluation and management of elbow tendinopathy. Sports Health 2012, 4, 384–393. [Google Scholar] [CrossRef]
- Lynch, J.R.; Waitayawinyu, T.; Hanel, D.P.; Trumble, T.E. Medial collateral ligament injury in the overhand-throwing athlete. J. Hand Surg. Am. 2008, 33, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Mezian, K.; Jačisko, J.; Kaiser, R.; Machač, S.; Steyerová, P.; Sobotová, K.; Angerová, Y.; Naňka, O. Ulnar Neuropathy at the Elbow: From Ultrasound Scanning to Treatment. Front. Neurol. 2021, 12, 562. [Google Scholar]
- Mezian, K.; Steyeorova, P.; Vacek, J.; Navratil, L. Introduction to Neuromuscular Ultrasound. Cesk. Slov. Neurol. N. 2016, 79, 656–661. [Google Scholar] [CrossRef]
- Lee, A.T.; Lee-Robinson, A.L. The prevalence of medial epicondylitis among patients with c6 and c7 radiculopathy. Sports Health 2010, 2, 334–336. [Google Scholar] [CrossRef]
- Park, G.-Y.; Lee, S.-M.; Lee, M.Y. Diagnostic value of ultrasonography for clinical medial epicondylitis. Arch. Phys. Med. Rehabil. 2008, 89, 738–742. [Google Scholar] [CrossRef] [PubMed]
- Ellington, M.D.; Edmonds, E.W. Pediatric Elbow and Wrist Pathology Related to Sports Participation. Orthop. Clin. N. Am. 2016, 47, 743–748. [Google Scholar] [CrossRef]
- Ciccotti, M.C.; Schwartz, M.A.; Ciccotti, M.G. Diagnosis and treatment of medial epicondylitis of the elbow. Clin. Sports Med. 2004, 23, 693–705. [Google Scholar] [CrossRef] [PubMed]
- Amin, N.H.; Kumar, N.S.; Schickendantz, M.S. Medial epicondylitis: Evaluation and management. J. Am. Acad. Orthop. Surg. 2015, 23, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Ciccotti, M.G.; Ramani, M.N. Medial epicondylitis. Tech. Hand Extrem. Surg. 2003, 7, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Stahl, S.; Kaufman, T. The efficacy of an injection of steroids for medial epicondylitis. A prospective study of sixty elbows. J. Bone Jt. Surg. Am. 1997, 79, 1648–1652. [Google Scholar] [CrossRef] [PubMed]
- Suresh, S.P.; Ali, K.E.; Jones, H.; Connell, D.A. Medial epicondylitis: Is ultrasound guided autologous blood injection an effective treatment? Br. J. Sports Med. 2006, 40, 935–939; discussion 939. [Google Scholar] [CrossRef] [PubMed]
- Bohlen, H.L.; Schwartz, Z.E.; Wu, V.J.; Thon, S.G.; Finley, Z.J.; O’Brien, M.J.; Savoie, F.H. Platelet-Rich Plasma Is an Equal Alternative to Surgery in the Treatment of Type 1 Medial Epicondylitis. Orthop. J. Sports Med. 2020, 8, 2325967120908952. [Google Scholar] [CrossRef] [PubMed]
- Chuang, H.-J.; Hsiao, M.-Y.; Wu, C.-H.; Özçakar, L. Dynamic Ultrasound Imaging for Ulnar Nerve Subluxation and Snapping Triceps Syndrome. Am. J. Phys. Med. Rehabil. 2016, 95, e113–e114. [Google Scholar] [CrossRef]
- Frazier, M.S.; Boardman, M.J.; Westland, M.; Imbriglia, J.E. Surgical treatment of partial distal biceps tendon ruptures. J. Hand Surg. Am. 2010, 35, 1111–1114. [Google Scholar] [CrossRef]
- Kelly, M.P.; Perkinson, S.G.; Ablove, R.H.; Tueting, J.L. Distal Biceps Tendon Ruptures: An Epidemiological Analysis Using a Large Population Database. Am. J. Sports Med. 2015, 43, 2012–2017. [Google Scholar] [CrossRef] [PubMed]
- Safran, M.R.; Graham, S.M. Distal biceps tendon ruptures: Incidence, demographics, and the effect of smoking. Clin. Orthop. Relat. Res. 2002, 404, 275–283. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, K.C.; Lee, J.-H.; Ahn, K.B.; Rhyou, I.H. A Case Series of Symptomatic Distal Biceps Tendinopathy. Clin. Shoulder Elb. 2018, 21, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Chew, M.L.; Giuffrè, B.M. Disorders of the distal biceps brachii tendon. Radiographics 2005, 25, 1227–1237. [Google Scholar] [CrossRef] [PubMed]
- Cho, C.-H.; Song, K.-S.; Choi, I.-J.; Kim, D.-K.; Lee, J.-H.; Kim, H.-T.; Moon, Y.-S. Insertional anatomy and clinical relevance of the distal biceps tendon. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 1930–1935. [Google Scholar] [CrossRef]
- Cucca, Y.Y.; McLay, S.V.B.; Okamoto, T.; Ecker, J.; McMenamin, P.G. The biceps brachii muscle and its distal insertion: Observations of surgical and evolutionary relevance. Surg. Radiol. Anat. 2010, 32, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Seiler, J.G.; Parker, L.M.; Chamberland, P.D.; Sherbourne, G.M.; Carpenter, W.A. The distal biceps tendon. Two potential mechanisms involved in its rupture: Arterial supply and mechanical impingement. J. Shoulder Elb. Surg. 1995, 4, 149–156. [Google Scholar] [CrossRef]
- Brigido, M.K.; De Maeseneer, M.; Morag, Y. Distal biceps brachii. Semin. Musculoskelet. Radiol. 2013, 17, 20–27. [Google Scholar] [CrossRef]
- Sanli, I.; Morgan, B.; van Tilborg, F.; Funk, L.; Gosens, T. Single injection of platelet-rich plasma (PRP) for the treatment of refractory distal biceps tendonitis: Long-term results of a prospective multicenter cohort study. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 2308–2312. [Google Scholar] [CrossRef]
- Barker, S.L.; Bell, S.N.; Connell, D.; Coghlan, J.A. Ultrasound-guided platelet-rich plasma injection for distal biceps tendinopathy. Shoulder Elb. 2015, 7, 110–114. [Google Scholar] [CrossRef]
- Al-Ani, Z.; Lauder, J. Ultrasound assessment in distal biceps tendon injuries: Techniques, pearls and pitfalls. Clin. Imaging 2021, 75, 46–54. [Google Scholar] [CrossRef]
- Ultrasound Imaging for the Cutaneous Nerves of the Extremities and Relevant Entrapment Syndromes: From Anatomy to Clinical Implications—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/30469370/ (accessed on 4 April 2021).
- Nirschl, R.P. Prevention and treatment of elbow and shoulder injuries in the tennis player. Clin. Sports Med. 1988, 7, 289–308. [Google Scholar] [CrossRef]
- Keener, J.D.; Chafik, D.; Kim, H.M.; Galatz, L.M.; Yamaguchi, K. Insertional anatomy of the triceps brachii tendon. J. Shoulder Elb. Surg. 2010, 19, 399–405. [Google Scholar] [CrossRef]
- Dunn, J.C.; Kusnezov, N.; Fares, A.; Rubin, S.; Orr, J.; Friedman, D.; Kilcoyne, K. Triceps Tendon Ruptures: A Systematic Review. Hand 2017, 12, 431–438. [Google Scholar] [CrossRef]
- Yeh, P.C.; Stephens, K.T.; Solovyova, O.; Obopilwe, E.; Smart, L.R.; Mazzocca, A.D.; Sethi, P.M. The distal triceps tendon footprint and a biomechanical analysis of 3 repair techniques. Am. J. Sports Med. 2010, 38, 1025–1033. [Google Scholar] [CrossRef] [PubMed]
- Madsen, M.; Marx, R.G.; Millett, P.J.; Rodeo, S.A.; Sperling, J.W.; Warren, R.F. Surgical anatomy of the triceps brachii tendon: Anatomical study and clinical correlation. Am. J. Sports Med. 2006, 34, 1839–1843. [Google Scholar] [CrossRef]
- Belentani, C.; Pastore, D.; Wangwinyuvirat, M.; Dirim, B.; Trudell, D.J.; Haghighi, P.; Resnick, D. Triceps brachii tendon: Anatomic-MR imaging study in cadavers with histologic correlation. Skelet. Radiol. 2009, 38, 171–175. [Google Scholar] [CrossRef]
- Akamatsu, F.E.; Negrão, J.R.; Rodrigues, M.B.; Itezerote, A.M.; Saleh, S.O.; Hojaij, F.; Andrade, M.; Jacomo, A.L. Is there something new regarding triceps brachii muscle insertion? Acta Cir. Bras. 2020, 35, e202001007. [Google Scholar] [CrossRef]
- Özçakar, L.; Onat, Ş.Ş.; Gürçay, E.; Kara, M. Are Blind Injections Ethical or Historical?: Think Twice with Ultrasound. Am. J. Phys. Med. Rehabil. 2016, 95, 158–160. [Google Scholar] [CrossRef]
- Cheatham, S.W.; Kolber, M.J.; Salamh, P.A.; Hanney, W.J. Rehabilitation of a partially torn distal triceps tendon after platelet rich plasma injection: A case report. Int. J. Sports Phys. Ther. 2013, 8, 290–299. [Google Scholar]
- Chang, K.V.; Wu, W.T.; Chen, I.J.; Lin, C.Y. Strain Ratio of Ultrasound Elastography for the Evaluation of Tendon Elasticity. Korean J. Radiol. 2020, 21, 384–385. [Google Scholar] [CrossRef]
- Domenichini, R.; Pialat, J.-B.; Podda, A.; Aubry, S. Ultrasound elastography in tendon pathology: State of the art. Skelet. Radiol. 2017, 46, 1643–1655. [Google Scholar] [CrossRef]
- Orujov, F.; Maskeliūnas, R.; Damaševičius, R.; Wei, W. Fuzzy based image edge detection algorithm for blood vessel detection in retinal images. Appl. Soft Comput. 2020, 94, 106452. [Google Scholar] [CrossRef]
- Versaci, M.; Morabito, F.C. Image Edge Detection: A New Approach Based on Fuzzy Entropy and Fuzzy Divergence. Int. J. Fuzzy Syst. 2021. [Google Scholar] [CrossRef]













Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mezian, K.; Jačisko, J.; Novotný, T.; Hrehová, L.; Angerová, Y.; Sobotová, K.; Naňka, O. Ultrasound-Guided Procedures in Common Tendinopathies at the Elbow: From Image to Needle. Appl. Sci. 2021, 11, 3431. https://doi.org/10.3390/app11083431
Mezian K, Jačisko J, Novotný T, Hrehová L, Angerová Y, Sobotová K, Naňka O. Ultrasound-Guided Procedures in Common Tendinopathies at the Elbow: From Image to Needle. Applied Sciences. 2021; 11(8):3431. https://doi.org/10.3390/app11083431
Chicago/Turabian StyleMezian, Kamal, Jakub Jačisko, Tomáš Novotný, Laura Hrehová, Yvona Angerová, Karolína Sobotová, and Ondřej Naňka. 2021. "Ultrasound-Guided Procedures in Common Tendinopathies at the Elbow: From Image to Needle" Applied Sciences 11, no. 8: 3431. https://doi.org/10.3390/app11083431
APA StyleMezian, K., Jačisko, J., Novotný, T., Hrehová, L., Angerová, Y., Sobotová, K., & Naňka, O. (2021). Ultrasound-Guided Procedures in Common Tendinopathies at the Elbow: From Image to Needle. Applied Sciences, 11(8), 3431. https://doi.org/10.3390/app11083431