
Left Atrial Volume Correlates with Mitral Annulus Size: An MDCT Study

 ,
,  ,
,  ,
,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Subjects and Procedure
2.2. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dwivedi, A.; Vainrib, A.; Saric, M. Functional mitral regurgitation in patients with heart failure and depressed ejection fraction. Curr. Opin. Cardiol. 2016, 31, 483–492. [Google Scholar] [CrossRef]
- Schmitto, J.D.; Lee, L.S.; Mokashi, S.A.; Bolman, R.M., 3rd; Cohn, L.H.; Chen, F.Y. Functional mitral regurgitation. Cardiol. Rev. 2010, 18, 285–291. [Google Scholar] [CrossRef]
- Otsuji, Y.; Kumanohoso, T.; Yoshifuku, S.; Matsukida, K.; Koriyama, C.; Kisanuki, A.; Minagoe, S.; Levine, R.A.; Tei, C. Isolated annular dilation does not usually cause important functional mitral regurgitation: Comparison between patients with lone atrial fibrillation and those with idiopathic or ischemic cardiomyopathy. J. Am. Coll. Cardiol. 2002, 39, 1651–1656. [Google Scholar] [CrossRef]
- Zhou, X.; Otsuji, Y.; Yoshifuku, S.; Yuasa, T.; Zhang, H.; Takasaki, K.; Matsukida, K.; Kisanuki, A.; Minagoe, S.; Tei, C. Impact of atrial fibrillation on tricuspid and mitral annular dilatation and valvular regurgitation. Circ. J. Off. J. Jpn. Circ. Soc. 2002, 66, 913–916. [Google Scholar] [CrossRef]
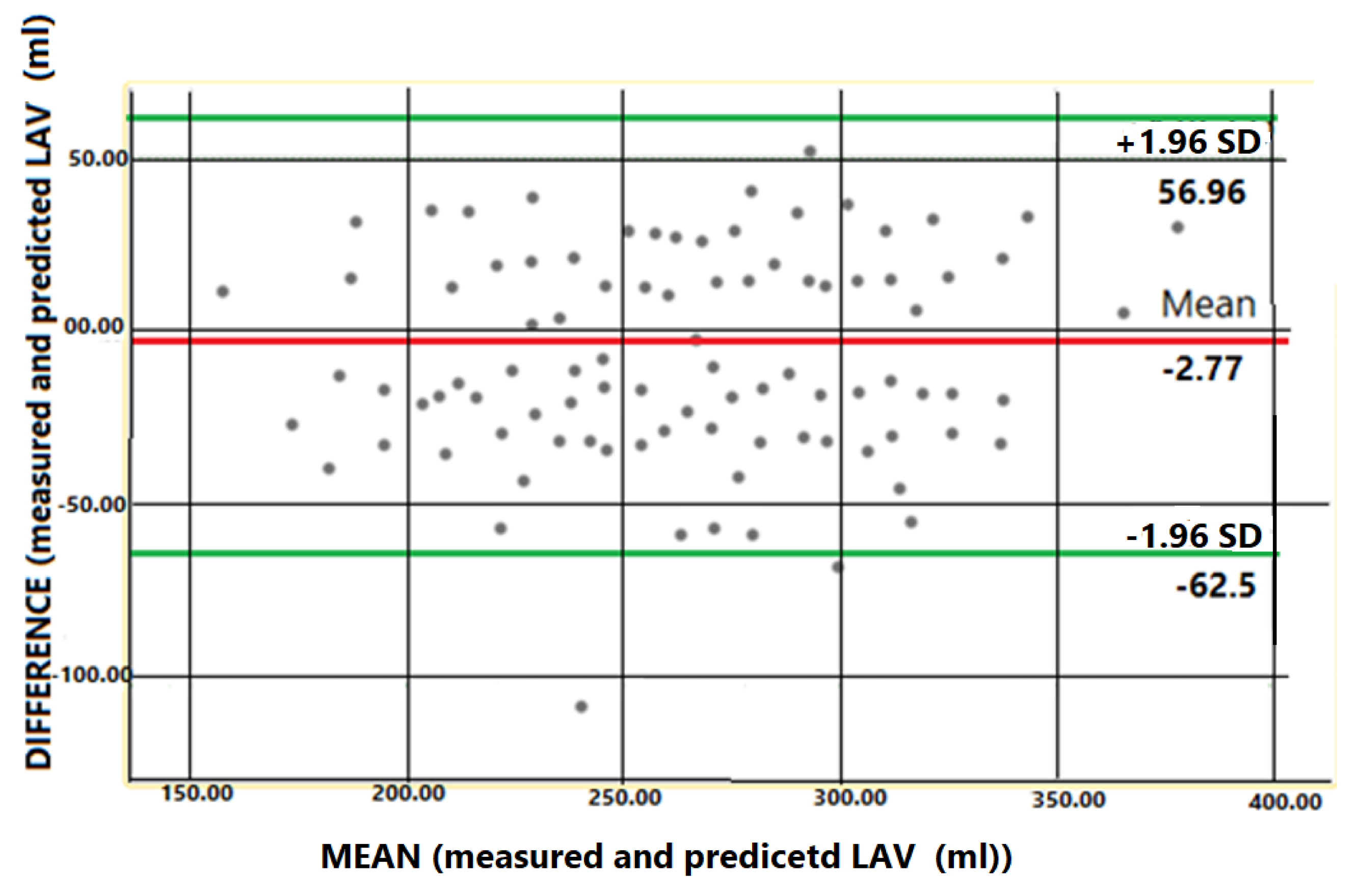
- Altman, D.G.; Bland, J.M. Measurement in Medicine: The Analysis of Method Comparison Studies. J. R. Stat. Soc. Ser. D 1983, 32, 307–317. [Google Scholar] [CrossRef]
- Stojanovska, J.; Cronin, P.; Patel, S.; Gross, B.H.; Oral, H.; Chughtai, K.; Kazerooni, E.A. Reference normal absolute and indexed values from ECG-gated MDCT: Left atrial volume, function, and diameter. AJR Am. J. Roentgenol. 2011, 197, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Stojanovska, J.; Cronin, P.; Gross, B.H.; Kazerooni, E.A.; Tsodikov, A.; Frank, L.; Oral, H. Left atrial function and maximum volume as determined by MDCT are independently associated with atrial fibrillation. Acad. Radiol. 2014, 21, 1162–1171. [Google Scholar] [CrossRef] [PubMed]
- Grover, R.; Ohana, M.; Arepalli, C.D.; Sellers, S.L.; Mooney, J.; Kueh, S.H.; Kim, U.; Blanke, P.; Leipsic, J.A. Role of MDCT Imaging in Planning Mitral Valve Intervention. Curr. Cardiol. Rep. 2018, 20, 16. [Google Scholar] [CrossRef] [PubMed]
- Naoum, C.; Leipsic, J.; Cheung, A.; Ye, J.; Bilbey, N.; Mak, G.; Berger, A.; Dvir, D.; Arepalli, C.; Grewal, J.; et al. Mitral Annular Dimensions and Geometry in Patients With Functional Mitral Regurgitation and Mitral Valve Prolapse: Implications for Transcatheter Mitral Valve Implantation. JACC Cardiovasc. Imaging 2016, 9, 269–280. [Google Scholar] [CrossRef]
- Hoffmann, U.; Bamberg, F.; Chae, C.U.; Nichols, J.H.; Rogers, I.S.; Seneviratne, S.K.; Truong, Q.A.; Cury, R.C.; Abbara, S.; Shapiro, M.D.; et al. Coronary computed tomography angiography for early triage of patients with acute chest pain: The ROMICAT (Rule Out Myocardial Infarction using Computer Assisted Tomography) trial. J. Am. Coll. Cardiol. 2009, 53, 1642–1650. [Google Scholar] [CrossRef]
- Hirasawa, K.; Vo, N.M.; Gegenava, T.; Pio, S.M.; van Wijngaarden, S.E.; Ajmone Marsan, N.; Bax, J.J.; Delgado, V. Mitral Valve Annulus Dimensions Assessment with Three-Dimensional Echocardiography Versus Computed Tomography: Implications for Transcatheter Interventions. J. Clin. Med. 2021, 10, 649. [Google Scholar] [CrossRef]
- Cong, T.; Gu, J.; Lee, A.P.; Shang, Z.; Sun, Y.; Sun, Q.; Wei, H.; Chen, N.; Sun, S.; Fu, T. Quantitative analysis of mitral valve morphology in atrial functional mitral regurgitation using real-time 3-dimensional echocardiography atrial functional mitral regurgitation. Cardiovasc. Ultrasound 2018, 16, 13. [Google Scholar] [CrossRef] [PubMed]
- Mihaila Baldea, S.; Muraru, D.; Miglioranza, M.H.; Iliceto, S.; Vinereanu, D.; Badano, L.P. Relation of Mitral Annulus and Left Atrial Dysfunction to the Severity of Functional Mitral Regurgitation in Patients with Dilated Cardiomyopathy. Cardiol. Res. Pract. 2020, 2020, 3261714. [Google Scholar] [CrossRef] [PubMed]
- Tanimoto, M.; Pai, R.G. Effect of isolated left atrial enlargement on mitral annular size and valve competence. Am. J. Cardiol. 1996, 77, 769–774. [Google Scholar] [CrossRef]
- Gertz, Z.M.; Raina, A.; Saghy, L.; Zado, E.S.; Callans, D.J.; Marchlinski, F.E.; Keane, M.G.; Silvestry, F.E. Evidence of atrial functional mitral regurgitation due to atrial fibrillation: Reversal with arrhythmia control. J. Am. Coll. Cardiol. 2011, 58, 1474–1481. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Heo, R.; Handschumacher, M.D.; Lee, S.; Choi, Y.S.; Kim, K.R.; Shin, Y.; Park, H.K.; Bischoff, J.; Aikawa, E.; et al. Mitral Valve Adaptation to Isolated Annular Dilation: Insights Into the Mechanism of Atrial Functional Mitral Regurgitation. JACC Cardiovasc. Imaging 2019, 12, 665–677. [Google Scholar] [CrossRef]
- Quinn, T.A.; Kohl, P. Cardiac Mechano-Electric Coupling: Acute Effects of Mechanical Stimulation on Heart Rate and Rhythm. Physiol. Rev. 2021, 101, 37–92. [Google Scholar] [CrossRef]
- Walters, T.E.; Lee, G.; Spence, S.; Larobina, M.; Atkinson, V.; Antippa, P.; Goldblatt, J.; O’Keefe, M.; Sanders, P.; Kistler, P.M.; et al. Acute atrial stretch results in conduction slowing and complex signals at the pulmonary vein to left atrial junction: Insights into the mechanism of pulmonary vein arrhythmogenesis. Circ. Arrhythm. Electrophysiol. 2014, 7, 1189–1197. [Google Scholar] [CrossRef]
- Mihaila, S.; Muraru, D.; Miglioranza, M.H.; Piasentini, E.; Aruta, P.; Cucchini, U.; Iliceto, S.; Vinereanu, D.; Badano, L.P. Relationship between mitral annulus function and mitral regurgitation severity and left atrial remodelling in patients with primary mitral regurgitation. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 918–929. [Google Scholar] [CrossRef][Green Version]
- Levy, M.J.; Edwards, J.E. Anatomy of mitral insufficiency. Prog. Cardiovasc. Dis. 1962, 5, 119–144. [Google Scholar] [CrossRef]
- Perloff, J.K.; Roberts, W.C. The mitral apparatus. Functional anatomy of mitral regurgitation. Circulation 1972, 46, 227–239. [Google Scholar] [CrossRef]
- Abdelghani, M.; Spitzer, E.; Soliman, O.I.I.; Beitzke, D.; Laggner, R.; Cavalcante, R.; Tateishi, H.; Campos, C.M.; Verstraeten, L.; Sotomi, Y.; et al. A simplified and reproducible method to size the mitral annulus: Implications for transcatheter mitral valve replacement. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Abe, Y.; Takahashi, Y.; Shibata, T. Functional mitral regurgitation, updated: Ventricular or atrial? J. Echocardiogr. 2020, 18, 1–8. [Google Scholar] [CrossRef]
- Kagiyama, N.; Hayashida, A.; Toki, M.; Fukuda, S.; Ohara, M.; Hirohata, A.; Yamamoto, K.; Isobe, M.; Yoshida, K. Insufficient Leaflet Remodeling in Patients With Atrial Fibrillation: Association With the Severity of Mitral Regurgitation. Circ. Cardiovasc. Imaging 2017, 10, e005451. [Google Scholar] [CrossRef] [PubMed]
- Kucuk, H.O.; Jouni, H.; Oguz, D.; Thaden, J.J.; Nkomo, V.T.; Pislaru, C.; Foley, T.A.; Muraru, D.; Pellikka, P.A.; Pislaru, S.V. Large, Unpredictable Beat-To-Beat Variability of Mitral Annulus Size in Atrial Fibrillation. JACC Cardiovasc. Interv. 2020, 13, 1387–1389. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, S.R.; Bashein, G.; Sheehan, F.H.; Legget, M.E.; Munt, B.; Li, X.N.; Sivarajan, M.; Bolson, E.L.; Zeppa, M.; Arch, M.Z.; et al. Three-dimensional echocardiographic assessment of annular shape changes in the normal and regurgitant mitral valve. Am. Heart J. 2000, 139, 378–387. [Google Scholar] [CrossRef]
- Mihaila, S.; Muraru, D.; Piasentini, E.; Miglioranza, M.H.; Peluso, D.; Cucchini, U.; Iliceto, S.; Vinereanu, D.; Badano, L.P. Quantitative analysis of mitral annular geometry and function in healthy volunteers using transthoracic three-dimensional echocardiography. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2014, 27, 846–857. [Google Scholar] [CrossRef]
- Vo, A.T.; Nguyen, N.T.H.; Le, K.M.; Vuong, N.L.; Nguyen, T.T.T.; Vu, T.T.; Hoang, S.V.; Nguyen, D.H. Mitral prosthetic size predictor in minimally invasive mitral valve replacement. J. Cardiothorac. Surg. 2020, 15, 147. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MITRAL ANNULUS | LEFT ATRIUM | |||||||
|---|---|---|---|---|---|---|---|---|
| Long Diameter (mm) | Transversal Diameter (mm) | Circumference (cm) | Area (cm2) | AP Diameter (mm) | LL Diameter (mm) | SI Diameter (mm) | Volume (mL) | |
| Mean ± SD | 41.9 ± 7.6 | 29.9 ± 5.3 | 15.0 ± 3.5 | 14.2 ± 4.6 | 41.1 ± 9.6 | 56.5 ± 10.7 | 48.2 ± 9.7 | 139 ± 56.3 |
| Range (Min–Max) | 23.9–57.1 | 21.3–39.4 | 9.6–23.6 | 6.4–22.0 | 26–71 | 39–88 | 27–68 | 101–349.6 |
| Paroxysmal AF (61) | Persistent AF (46) | p Value | |
|---|---|---|---|
| age | 54.05 ± 9.5 years | 58.2 ± 9.0 years | <0.05 |
| Left atrium | |||
| 38.7 ± 6.4 | 42.8 ± 11.2 | <0.05 |
| 56.1 ± 10.5 | 56.8 ± 10.9 | NS |
| 48.15 ± 10.6 | 48.2 ± 8.6 | NS |
| Mitral valve | |||
| 43.4 | 46.0 ± 8.1 | <0.05 |
| 30.4 | 32.8 ± 8.5 | NS |
| Category | R1 | p Value |
|---|---|---|
| MA longitudinal diameter—LA volume | 0.423 | 0.005 |
| MA transversal diameter—LA volume | 0.32 | 0.036 |
| MA circumference—LA volume | 0.535 | <0.001 |
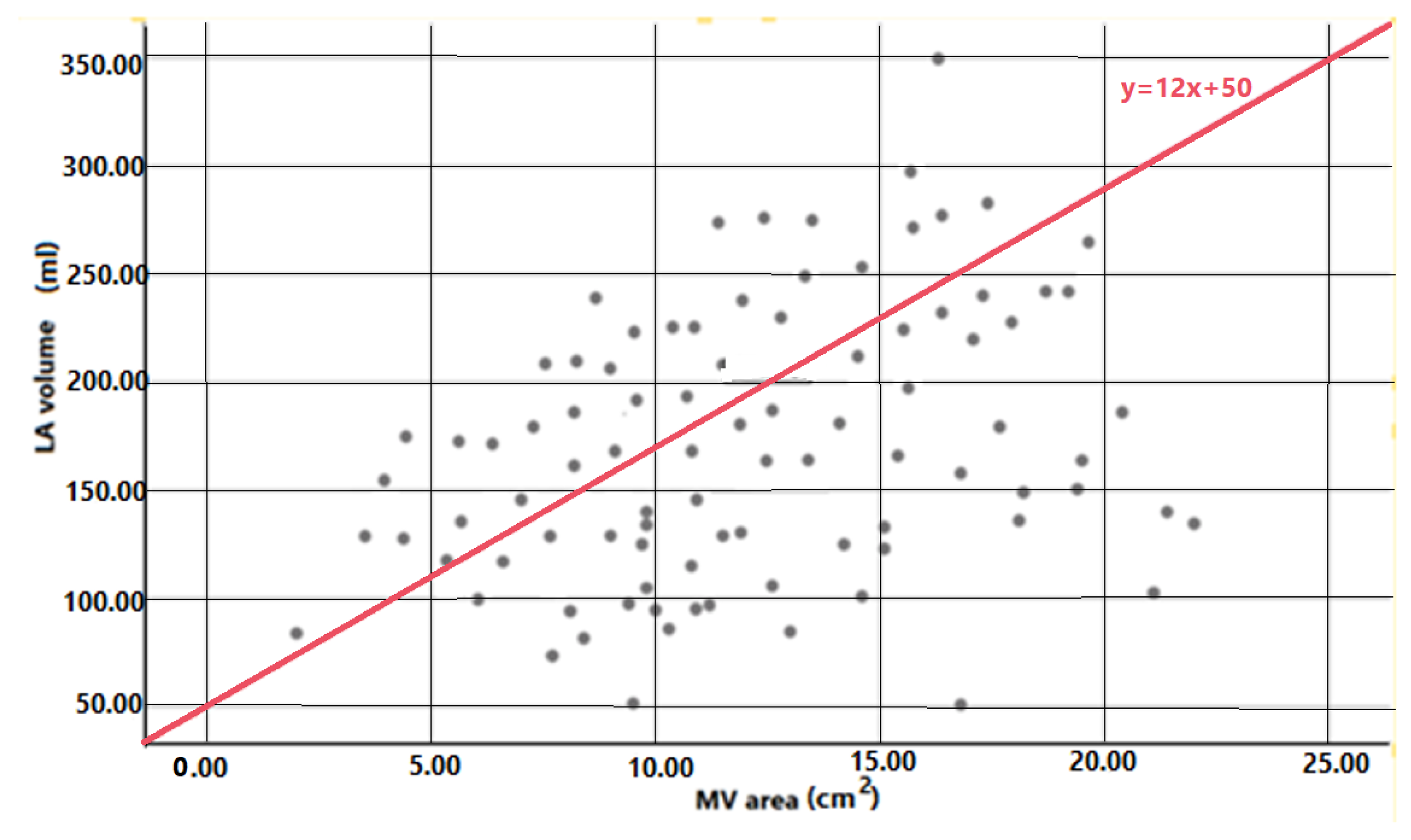
| MA area—LA volume | 0.639 | <0.001 |
| MA long diameter—LL diameter | 0.576 | <0.001 |
| MA transversal diameter—AP diameter | 0.594 | <0.001 |
| MA long—MA transversal | 0.726 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cismaru, G.; Valean, I.; Zirbo, M.C.; Tirpe, A.; Cismaru, A.; Rosu, R.; Puiu, M.; Muresan, L.; Gusetu, G.; Minciuna, I.-A.; et al. Left Atrial Volume Correlates with Mitral Annulus Size: An MDCT Study. Appl. Sci. 2021, 11, 11329. https://doi.org/10.3390/app112311329
Cismaru G, Valean I, Zirbo MC, Tirpe A, Cismaru A, Rosu R, Puiu M, Muresan L, Gusetu G, Minciuna I-A, et al. Left Atrial Volume Correlates with Mitral Annulus Size: An MDCT Study. Applied Sciences. 2021; 11(23):11329. https://doi.org/10.3390/app112311329
Chicago/Turabian StyleCismaru, Gabriel, Iulia Valean, Mihnea Cantemir Zirbo, Alexandru Tirpe, Andrei Cismaru, Radu Rosu, Mihai Puiu, Lucian Muresan, Gabriel Gusetu, Ioan-Alxandru Minciuna, and et al. 2021. "Left Atrial Volume Correlates with Mitral Annulus Size: An MDCT Study" Applied Sciences 11, no. 23: 11329. https://doi.org/10.3390/app112311329
APA StyleCismaru, G., Valean, I., Zirbo, M. C., Tirpe, A., Cismaru, A., Rosu, R., Puiu, M., Muresan, L., Gusetu, G., Minciuna, I.-A., Florea, C. M., Tomoaia, R., Zdrenghea, D., & Pop, D. (2021). Left Atrial Volume Correlates with Mitral Annulus Size: An MDCT Study. Applied Sciences, 11(23), 11329. https://doi.org/10.3390/app112311329