
Biomechanical Analysis of Clavicle Hook Plates with a Range of Posterior Hook Offsets Implanted at Different Acromion Positions in the Acromioclavicular Joint: A Finite Element Analysis Study



Abstract
:1. Introduction
2. Materials and Methods
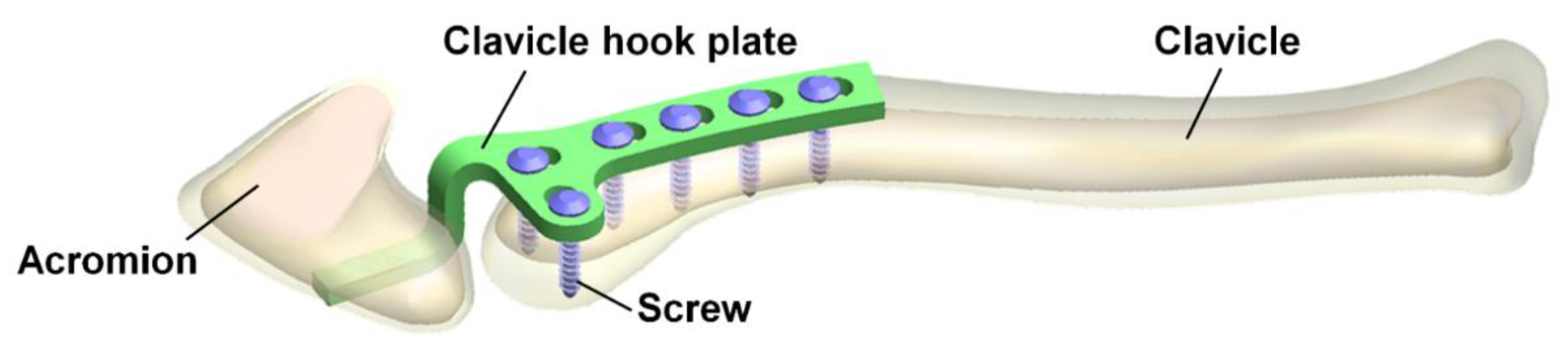
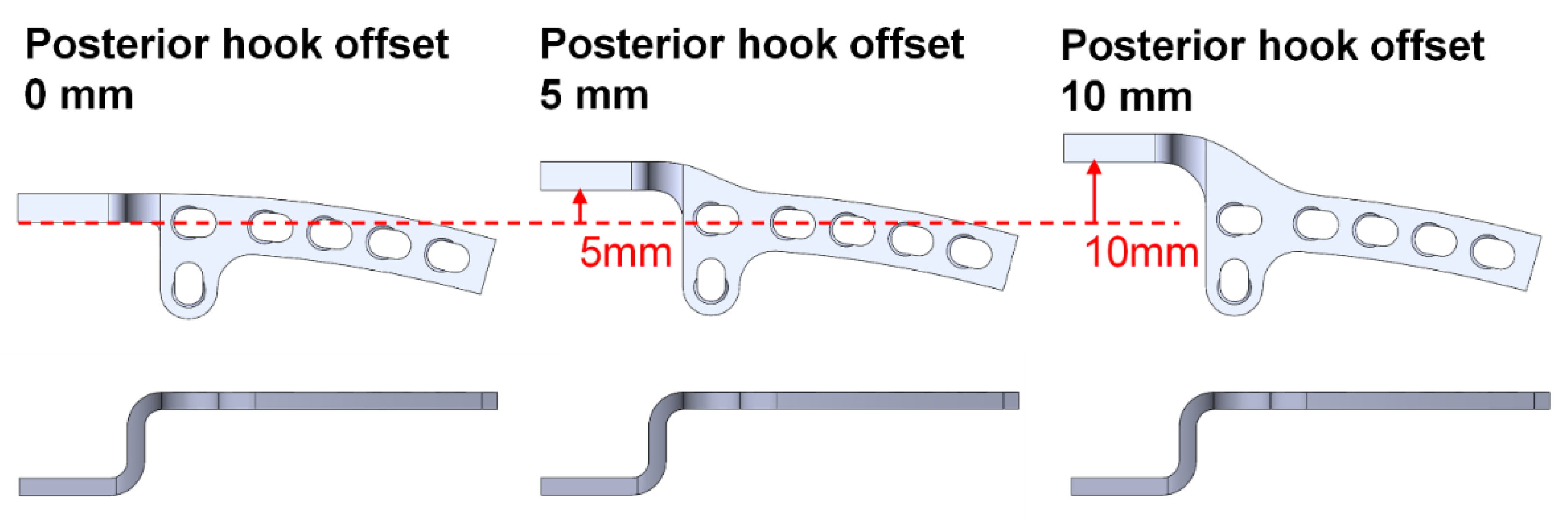
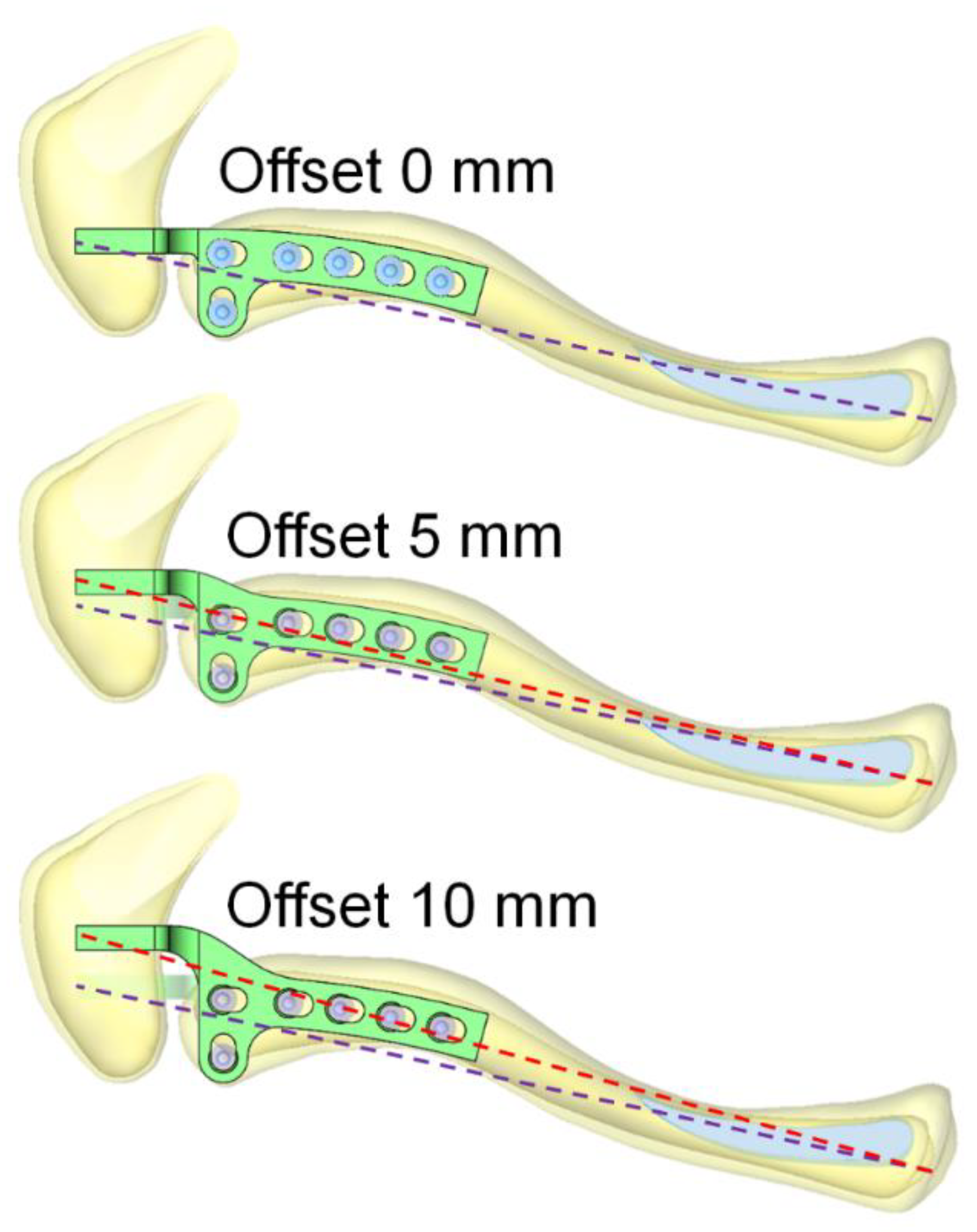
2.1. The Simulation Geometry Model
2.2. Loading Conditions and Boundary Conditions
2.3. Material Properties of the Model
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Di Francesco, A.; Zoccali, C.; Colafarina, O.; Pizzoferrato, R.; Flamini, S. The use of hook plate in type III and V acromio-clavicular Rockwood dislocations: Clinical and radiological midterm results and MRI evaluation in 42 patients. Injury 2012, 43, 147–152. [Google Scholar] [CrossRef]
- Tiren, D.; van Bemmel, A.J.; Swank, D.J.; van der Linden, F.M. Hook plate fixation of acute displaced lateral clavicle fractures: Mid-term results and a brief literature overview. J. Orthop. Surg. Res. 2012, 7, 2. [Google Scholar] [CrossRef] [Green Version]
- Kumar, N.; Sharma, V. Hook plate fixation for acute acromioclavicular dislocations without coracoclavicular ligament reconstruction: A functional outcome study in military personnel. Strategies. Trauma. Limb. Reconstr. 2015, 10, 79–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baunach, D.; Eid, K.; Ricks, M.; Borbas, P. Long-term clinical and radiological results after hook plate osteosynthesis of lateral clavicle fractures. J. Orthop. Trauma. 2021, 35, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Yoon, B.; Kim, J.Y.; Lee, J.-S.; Jung, H.S. The Radiologic Comparison of Operative Treatment Using a Hook Plate versus a Distal Clavicle Locking Plate of Distal Clavicle Fracture. Clin. Shoulder Elb. 2018, 21, 227–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemmann, P.; Koch, M.; Guehring, M.; Bahrs, C.; Ziegler, P. Acromioclavicular joint separation treated with clavicular hook plate: A study of radiological and functional outcomes. Arch. Orthop. Trauma. Surg. 2021, 141, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Yoo, Y.-S.; Jang, S.W.; Nair, A.V.; Jin, H.; Song, H.-S. In vivo analysis of acromioclavicular joint motion after hook plate fixation using three-dimensional computed tomography. J. Shoulder Elb. Surg. 2015, 24, 1106–1111. [Google Scholar] [CrossRef]
- Hoffler, C.E.; Karas, S.G. Transacromial erosion of a locked subacromial hook plate: Case report and review of literature. J. Shoulder Elb. Surg. 2010, 19, e12–e15. [Google Scholar] [CrossRef]
- Chiang, C.-L.; Yang, S.-W.; Tsai, M.-Y.; Chen, C.K.-H. Acromion osteolysis and fracture after hook plate fixation for acromioclavicular joint dislocation: A case report. J. Shoulder Elb. Surg. 2010, 19, e13–e15. [Google Scholar] [CrossRef]
- Lopiz, Y.; Checa, P.; García-Fernández, C.; Valle, J.; Vega, M.L.; Marco, F. Complications with the clavicle hook plate after fixation of Neer type II clavicle fractures. Int. Orthop. 2019, 43, 1701–1708. [Google Scholar] [CrossRef]
- Lin, H.-Y.; Wong, P.-K.; Ho, W.-P.; Chuang, T.-Y.; Liao, Y.-S.; Wong, C.-C. Clavicular hook plate may induce subacromial shoulder impingement and rotator cuff lesion-dynamic sonographic evaluation. J. Orthop. Surg. Res. 2014, 9, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charity, R.M.; Haidar, S.G.; Ghosh, S.; Tillu, A.B. Fixation failure of the clavicular hook plate: A report of three cases. J. Orthop. Surg. 2006, 14, 333–335. [Google Scholar] [CrossRef]
- Ding, M.; Ni, J.; Hu, J.; Song, D. Rare complication of clavicular hook plate: Clavicle fracture at the medial end of the plate. J. Shoulder Elb. Surg. 2011, 20, e18–e20. [Google Scholar] [CrossRef] [PubMed]
- Ni, P.-L.; Lin, K.-C.; Chen, C.-Y.; Tarng, Y.-W.; Chang, W.-N.; Renn, J.-H. Peri-implant Fractures Following Hook Plate Fixation for Unstable Distal Clavicle Fractures. Orthopedics 2020, 43, e359–e363. [Google Scholar] [CrossRef] [PubMed]
- Shih, J.-T.; Wu, C.-C.; Wang, C.-C.; Yeh, T.-T.; Pan, R.-Y.; Chen, C.-L.; Chien, W.-C.; Shen, P.-H. Midshaft clavicle fracture following osteosynthesis with a hook plate: A retrospective case analysis. Arch. Orthop. Trauma Surg. 2020, 140, 1713–1718. [Google Scholar] [CrossRef]
- ElMaraghy, A.W.; Devereaux, M.W.; Ravichandiran, K.; Agur, A.M. Subacromial morphometric assessment of the clavicle hook plate. Injury 2010, 41, 613–619. [Google Scholar] [CrossRef]
- Deng, Z.; Cai, L.; Ping, A.; Ai, Q.; Wang, Y. Anatomical research on the subacromial interval following implantation of clavicle hook plates. Int J. Sports Med. 2014, 35, 857–862. [Google Scholar] [CrossRef]
- Shen, P.-C.; Zhu, Y.; Zhang, H.; Zhu, L.-F.; Weng, F.-B.; Jiang, F.-G.; Xu, N.; Ju, W.; Li, X.-L. Three-dimensional morphological analysis of acromioclavicular joint in patients with and without subacromial erosion after hook plate fixation. J. Int. Med. Res. 2018, 46, 511–521. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.-J.; Kee, Y.-M.; Park, D.-H.; Ko, Y.-I.; Lee, B.-G. Evaluation of the Acromioclavicular Joint Morphology for Minimizing Subacromial Erosion after Surgical Fixation of the Joint Using a Clavicular Hook Plate. Clin. Shoulder Elb. 2018, 21, 138–144. [Google Scholar] [CrossRef]
- Lee, C.-H.; Shih, C.-M.; Huang, K.-C.; Chen, K.-H.; Hung, L.-K.; Su, K.-C. Biomechanical analysis of implanted clavicle hook plates with different implant depths and materials in the acromioclavicular joint: A finite element analysis study. Artif. Organs. 2016, 40, 1062–1070. [Google Scholar] [CrossRef]
- Shih, C.-M.; Huang, K.-C.; Pan, C.-C.; Lee, C.-H.; Su, K.-C. Biomechanical analysis of acromioclavicular joint dislocation treated with clavicle hook plates in different lengths. Int. Orthop. 2015, 39, 2239–2244. [Google Scholar] [CrossRef] [PubMed]
- Hung, L.-K.; Su, K.-C.; Lu, W.-H.; Lee, C.-H. Biomechanical analysis of clavicle hook plate implantation with different hook angles in the acromioclavicular joint. Int. Orthop. 2017, 41, 1663–1669. [Google Scholar] [CrossRef]
- Wu, K.; Su, X.; Roche, S.J.L.; Held, M.F.G.; Yang, H.; Dunn, R.N.; Guo, J.J. Relationship between the lateral acromion angle and postoperative persistent pain of distal clavicle fracture treated with clavicle hook plate. J. Orthop. Surg. Res. 2020, 15, 217. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Liu, T.; Shao, X.; Liu, Z.; Duan, J.; Akileh, R.; Cao, S.; Jin, D. Fifteen-degree clavicular hook plate achieves better clinical outcomes in the treatment of acromioclavicular joint dislocation. J. Int. Med. Res. 2018, 46, 4547–4559. [Google Scholar] [CrossRef]
- Qiao, R.; Yang, J.; Zhang, K.; Song, Z. To explore the reasonable selection of clavicular hook plate to reduce the occurrence of subacromial impingement syndrome after operation. J. Orthop. Surg. Res. 2021, 16, 180. [Google Scholar] [CrossRef] [PubMed]
- Cronskär, M.; Rasmussen, J.; Tinnsten, M. Combined finite element and multibody musculoskeletal investigation of a fractured clavicle with reconstruction plate. Comput. Methods Biomech. Biomed. Eng. 2015, 18, 740–748. [Google Scholar] [CrossRef]
- Lee, H.H. Finite Element Simulations with ANSYS Workbench 15; Chuan Hwa Book Co.: Taiwan, Taiwan, 2014. [Google Scholar]
- Enderle, J.; Bronzino, J. Introduction to Biomedical Engineering; Academic Press: Boston, MA, USA, 2012. [Google Scholar]
- Wu, D.-K.; Chen, W.-C.; Lin, K.-J.; Tsai, C.-L.; Lin, K.-P.; Wei, H.-W. Advantage of Multi-Directional Stability of Spiral Clavicle Plate in Treatment of Middle One-Third Clavicle Fracture: A Finite Element Study. J. Med. Biol. Eng. 2021, 41, 405–411. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Young’s Modulus (MPa) | Poisson’s Ratio |
|---|---|---|
| Cortical bone | 17,000 | 0.3 |
| Cancellous bone | 1000 | 0.3 |
| Clavicle hook plate | 200,000 | 0.3 |
| Screws | 118,000 | 0.3 |
| Anterior Acromion | Middle Acromion | Posterior Acromion | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Posterior Hook Offset | 0 mm | 5 mm | 10 mm | 0 mm | 5 mm | 10 mm | 0 mm | 5 mm | 10 mm |
| Mesh nodes | 188,882 | 190,086 | 191,971 | 188,217 | 189,421 | 191,445 | 188,467 | 189,553 | 191,507 |
| Mesh elements | 103,576 | 104,296 | 105,362 | 103,171 | 103,889 | 105,064 | 103,335 | 103,983 | 105,102 |
| Hook Position | Anterior Acromion | Middle Acromion | Posterior Acromion | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Posterior Hook Offset | 0 mm | 5 mm | 10 mm | 0 mm | 5 mm | 10 mm | 0 mm | 5 mm | 10 mm | |
| Reaction force on acromion (N) | X-Axis | −3.5615 | −0.4431 | −0.37351 | −3.4105 | −0.4572 | −0.38434 | −4.2696 | −0.62777 | −0.50583 |
| Y-Axis | −2.1026 | −2.5631 | −2.5622 | −2.1436 | −2.5634 | −2.562 | −2.0026 | −2.4803 | −2.4812 | |
| Z-Axis | 0.4186 | 1.4168 | 1.4555 | 0.45633 | 1.4107 | 1.4511 | 0.25256 | 1.3597 | 1.4068 | |
| Total | 4.157 | 2.9619 | 2.9703 | 4.054 | 2.9615 | 2.9694 | 4.7227 | 2.8974 | 2.8967 | |
| Maximum stress (MPa) | Plate | 44.944 | 74.086 | 74.503 | 30.718 | 73.785 | 74.059 | 44.162 | 73.357 | 73.872 |
| S1 | 2.6561 | 0.17302 | 0.17333 | 2.0829 | 0.17919 | 0.18024 | 2.6496 | 0.18685 | 0.18839 | |
| S2 | 2.0644 | 5.3123 | 5.3011 | 1.8372 | 5.3895 | 5.5165 | 1.9973 | 5.5796 | 5.5942 | |
| S3 | 3.9743 | 16.426 | 16.46 | 4.7258 | 17.008 | 17.123 | 5.2918 | 17.813 | 17.978 | |
| S4 | 9.4925 | 32.812 | 32.778 | 11.137 | 34.008 | 34.102 | 12.17 | 35.307 | 35.463 | |
| S5 | 1.7393 | 6.7224 | 6.7844 | 1.998 | 6.9667 | 7.0806 | 2.206 | 7.4543 | 7.5953 | |
| S6 | 10.331 | 33.743 | 33.689 | 11.943 | 35.022 | 35.112 | 13.181 | 36.512 | 36.674 | |
| Point P | 0.91762 | 1.0059 | 1.0136 | 0.91661 | 1.0045 | 1.0127 | 0.90326 | 1.0195 | 1.0299 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, L.-K.; Lee, C.-H.; Su, K.-C. Biomechanical Analysis of Clavicle Hook Plates with a Range of Posterior Hook Offsets Implanted at Different Acromion Positions in the Acromioclavicular Joint: A Finite Element Analysis Study. Appl. Sci. 2021, 11, 11105. https://doi.org/10.3390/app112311105
Hung L-K, Lee C-H, Su K-C. Biomechanical Analysis of Clavicle Hook Plates with a Range of Posterior Hook Offsets Implanted at Different Acromion Positions in the Acromioclavicular Joint: A Finite Element Analysis Study. Applied Sciences. 2021; 11(23):11105. https://doi.org/10.3390/app112311105
Chicago/Turabian StyleHung, Li-Kun, Cheng-Hung Lee, and Kuo-Chih Su. 2021. "Biomechanical Analysis of Clavicle Hook Plates with a Range of Posterior Hook Offsets Implanted at Different Acromion Positions in the Acromioclavicular Joint: A Finite Element Analysis Study" Applied Sciences 11, no. 23: 11105. https://doi.org/10.3390/app112311105
APA StyleHung, L.-K., Lee, C.-H., & Su, K.-C. (2021). Biomechanical Analysis of Clavicle Hook Plates with a Range of Posterior Hook Offsets Implanted at Different Acromion Positions in the Acromioclavicular Joint: A Finite Element Analysis Study. Applied Sciences, 11(23), 11105. https://doi.org/10.3390/app112311105