
A Validation Method for EPID In Vivo Dosimetry Algorithms

 , , , and
, , , and
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
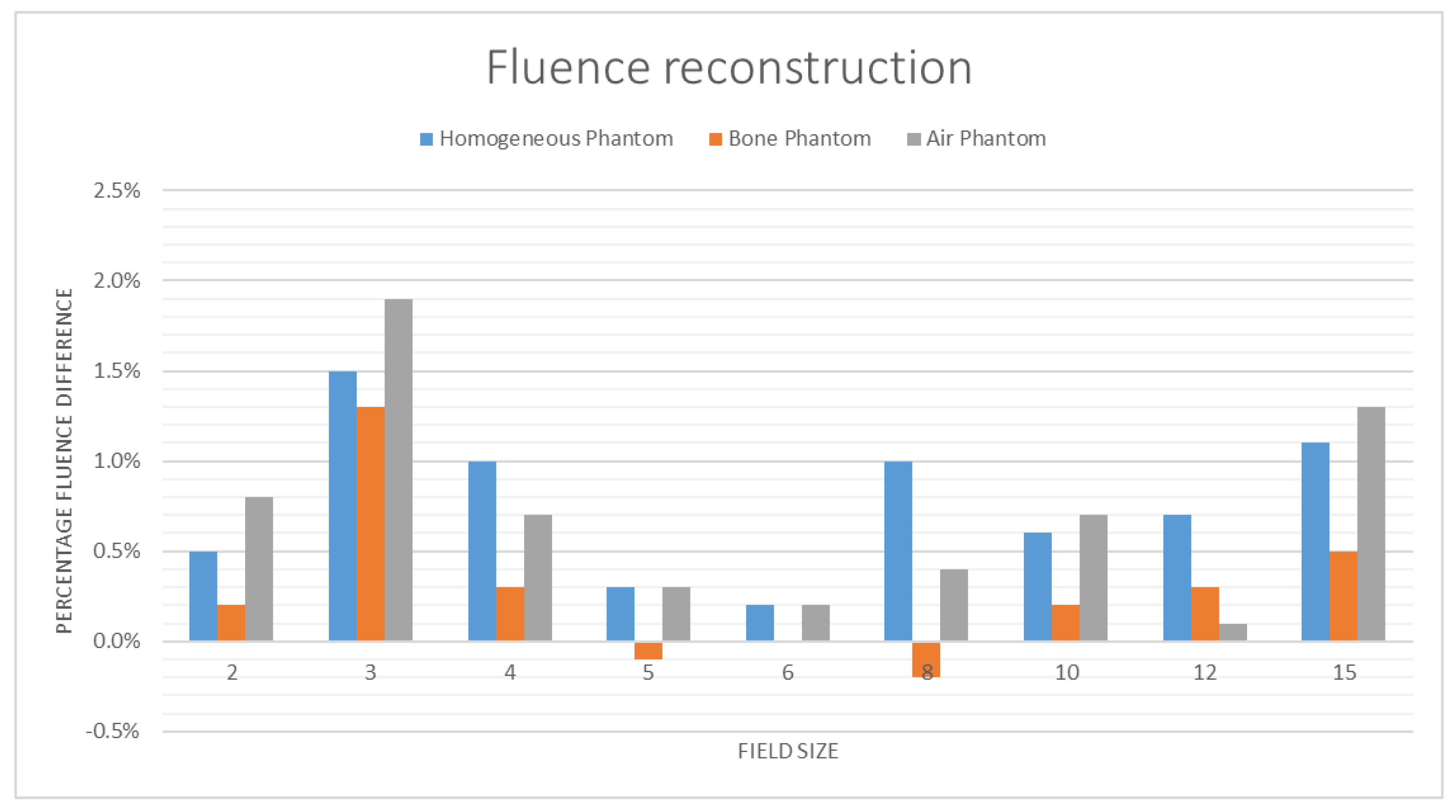
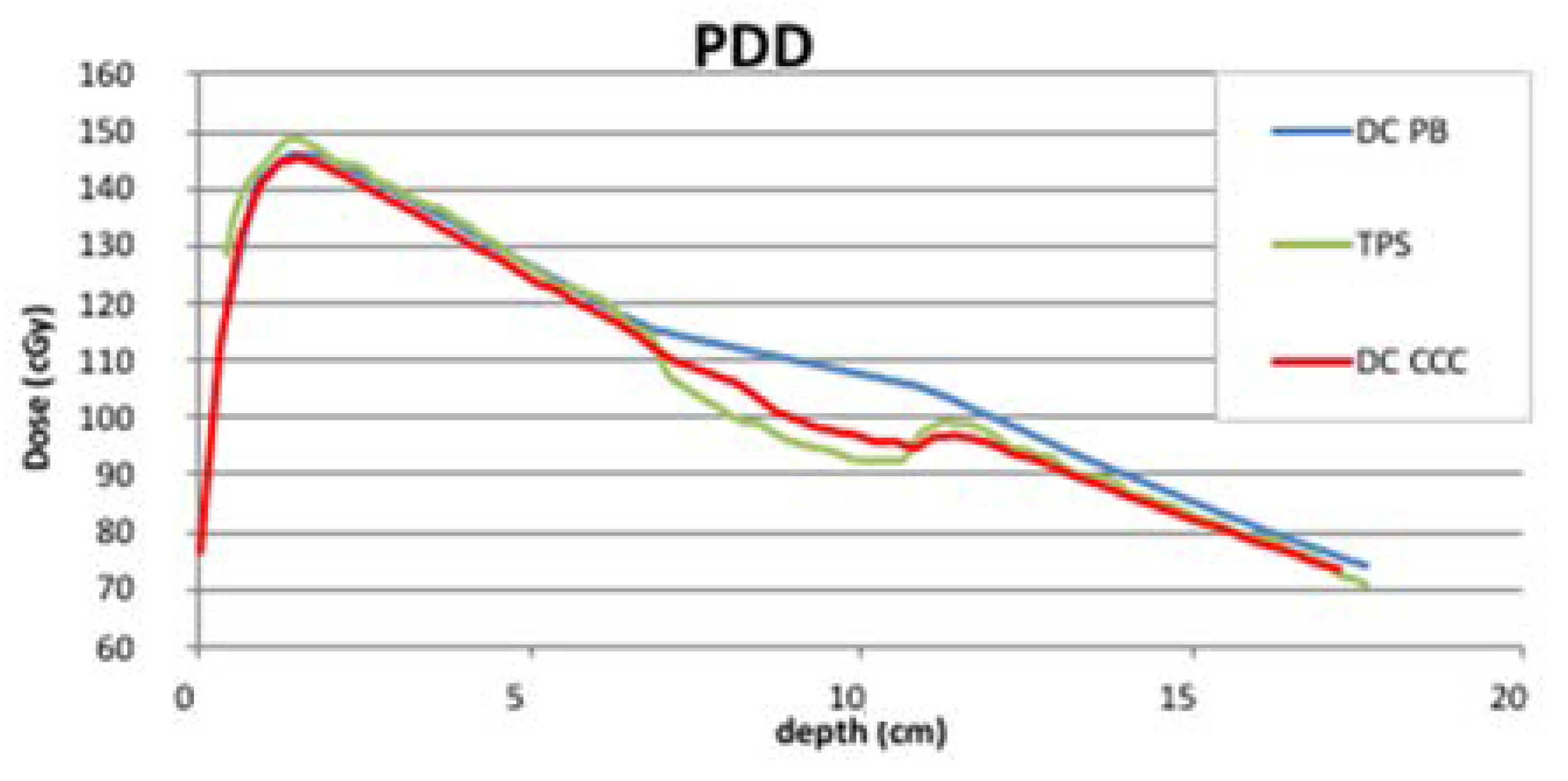
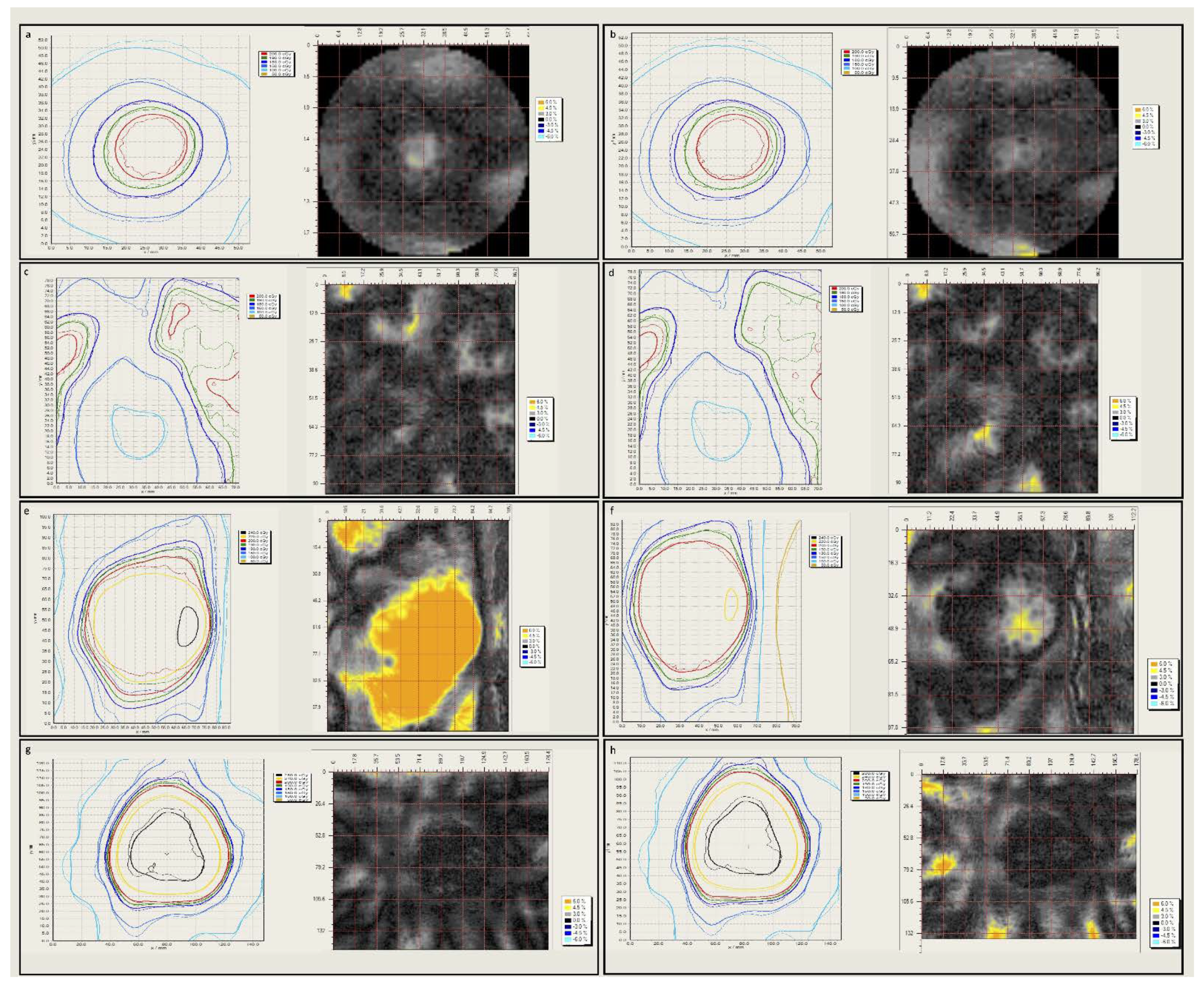
2.1. Slab Phantom Tests
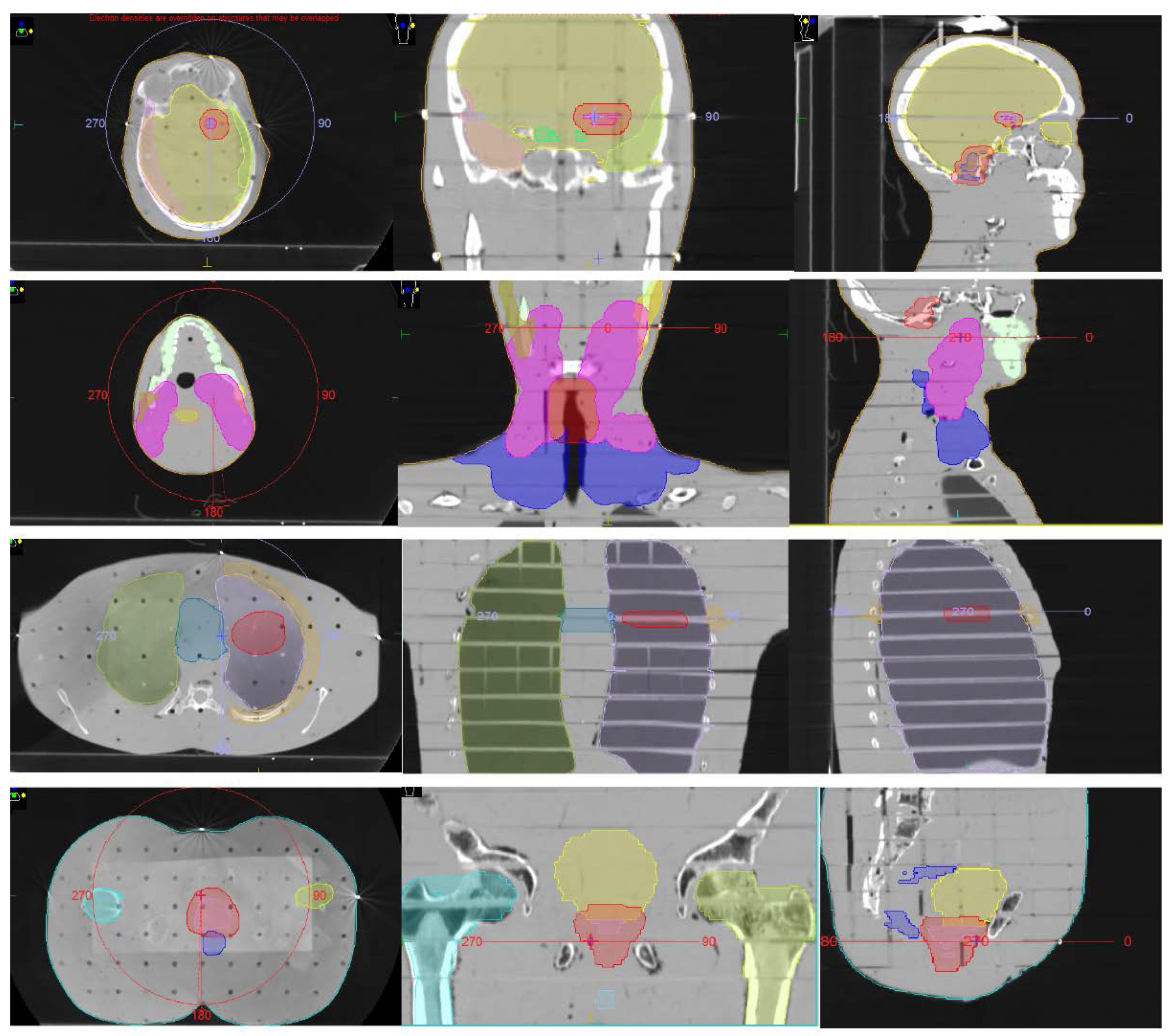
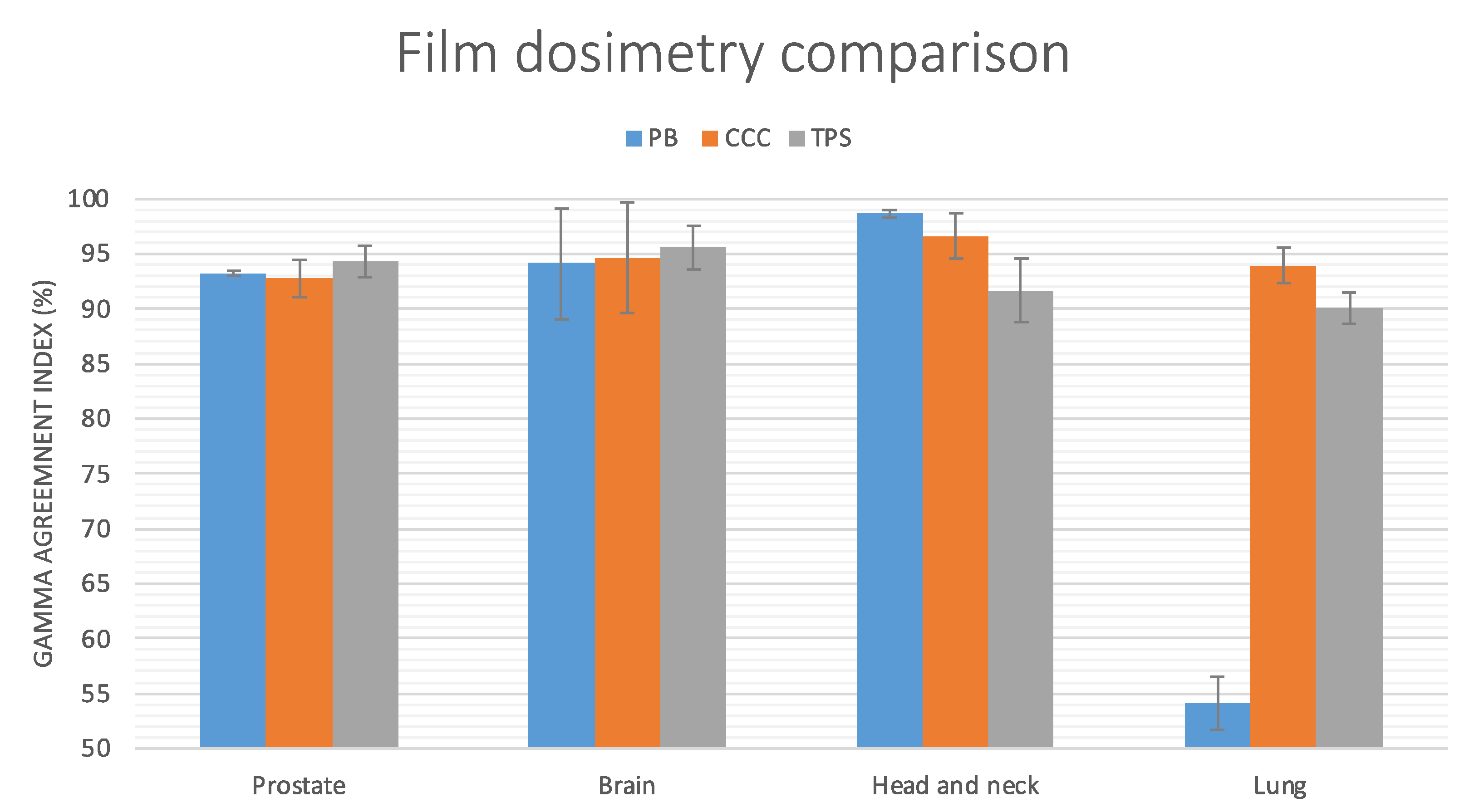
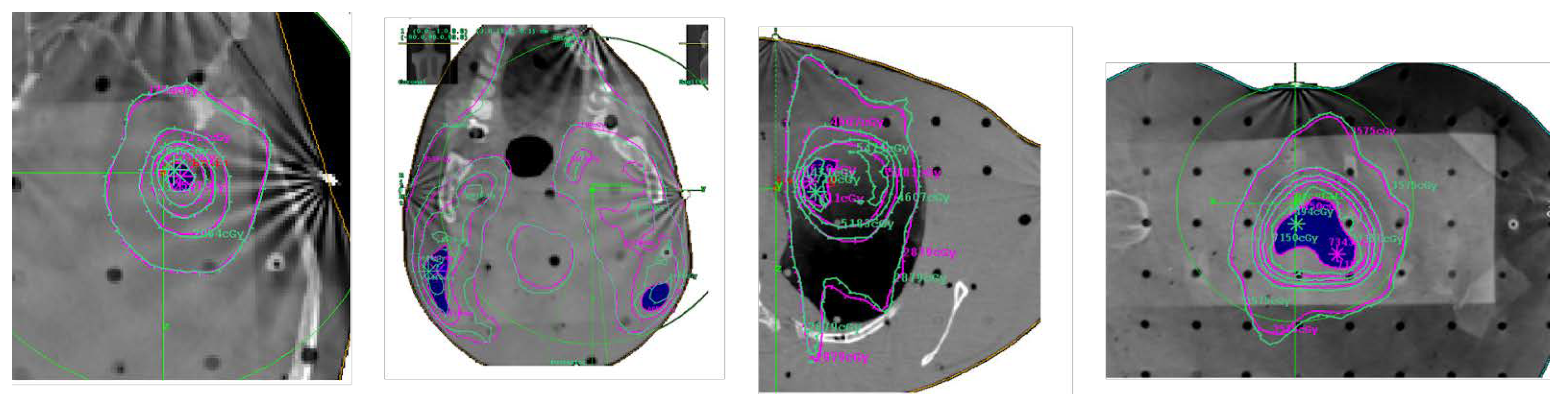
2.2. Anthropomorphic Phantom Tests
2.3. Plans Delivery
2.4. EPID Dosimetry
2.5. Radiochromic Films Analysis
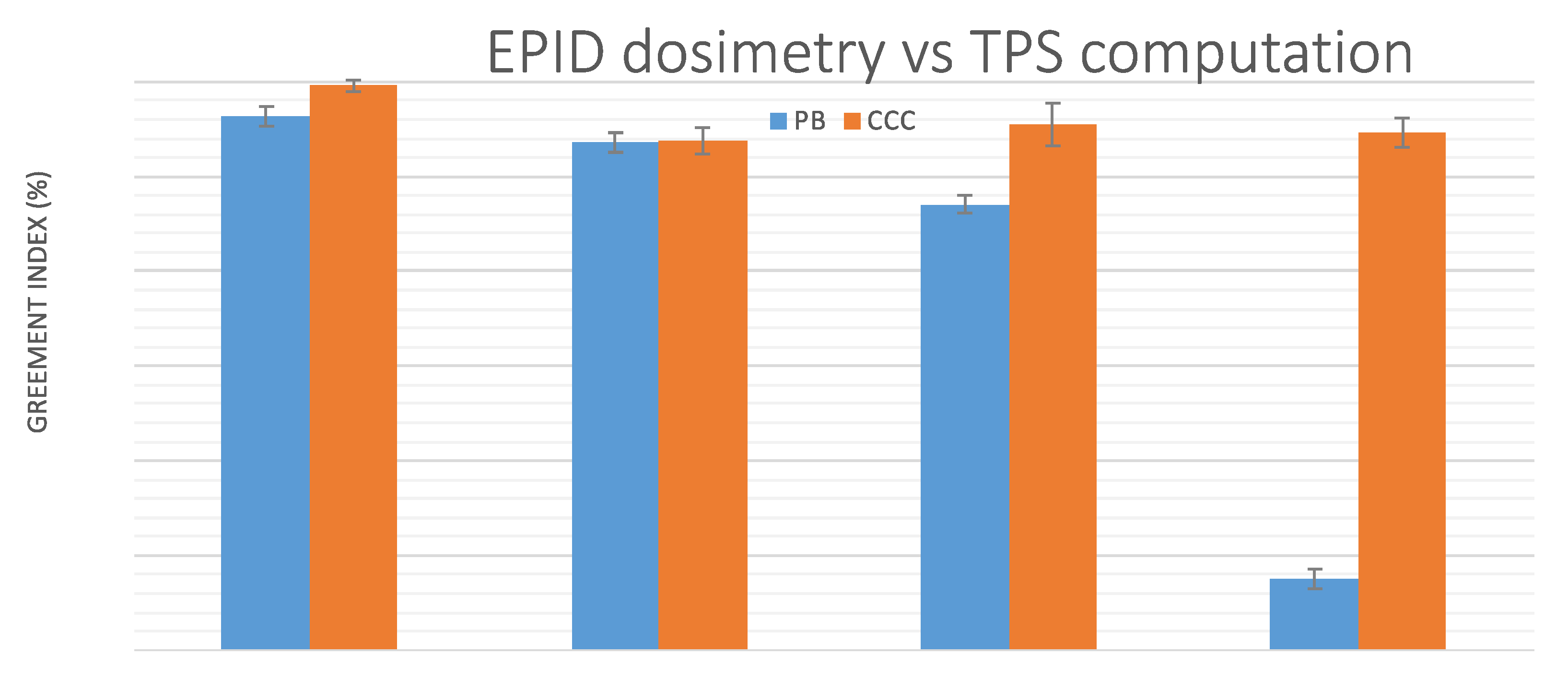
2.6. Dose Distributions Agreement Analysis
3. Results
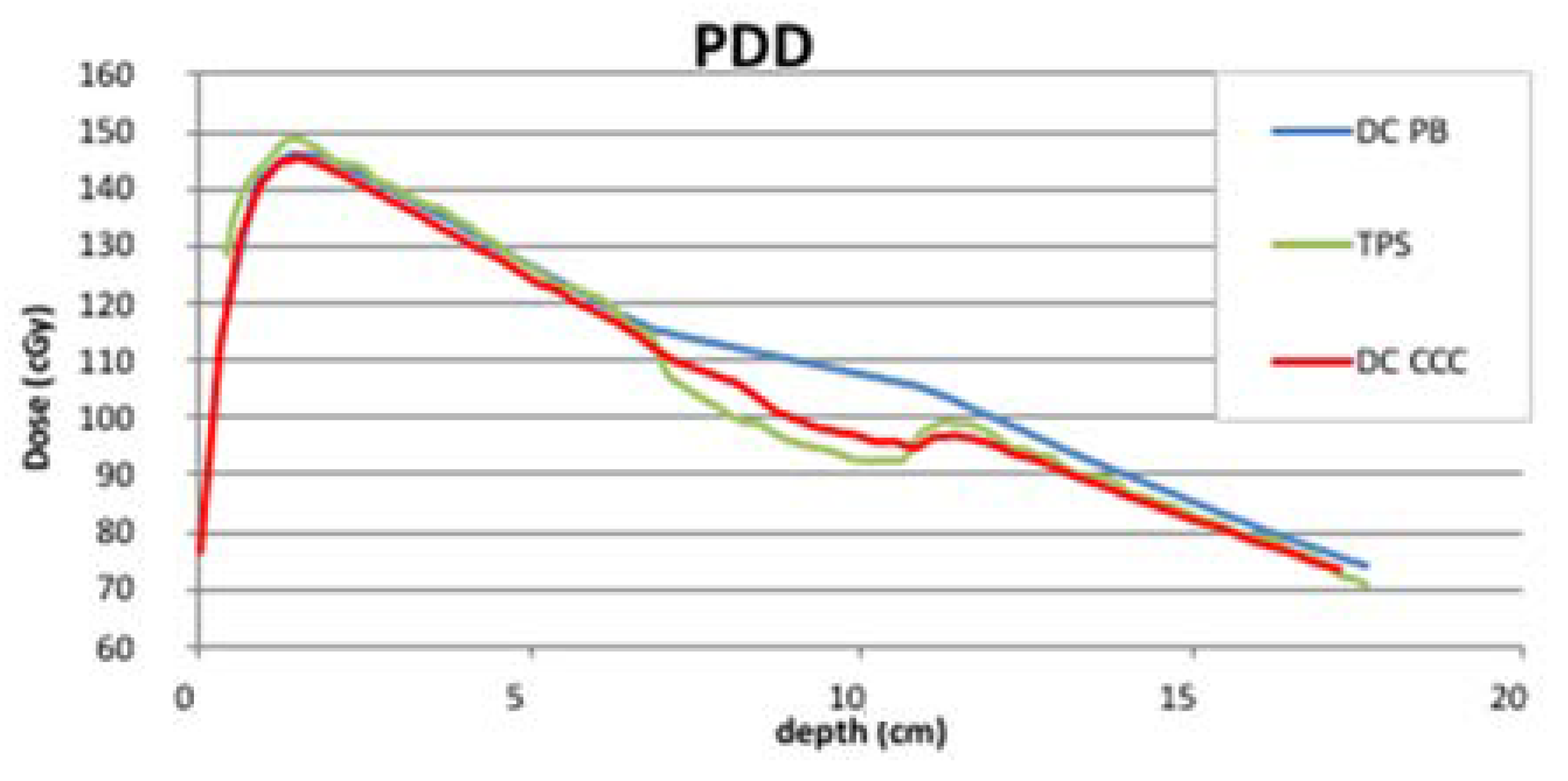
3.1. Slab Phantom Tests
3.2. Anthropomorphic Phantom Tests
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Atomic Energy Agency. Development of Procedures for In Vivo Dosimetry in Radiotherapy; IAEA Human Health Report No. 8; IAEA: Vienna, Austria, 2013. [Google Scholar]
- COUNCIL DIRECTIVE 2013/59/EURATOM of 5 December 2013. Available online: https://eur-lex.europa.eu/eli/dir/2013/59/oj (accessed on 5 November 2021).
- Esposito, M.; Villaggi, E.; Bresciani, S.; Cilla, S.; Falco, M.D.; Garibaldi, C.; Russo, S.; Talamonti, C.; Stasi, M.; Mancosu, P. Estimating dose delivery accuracy in stereotactic body radiation therapy: A review of in-vivo measurement methods. Radiother. Oncol. 2020, 149, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Bruschi, A.; Bastiani, P.; Ghirelli, A.; Pini, S.; Russo, S.; Zatelli, G. Characterization of EPID software for VMAT transit dosimetry. Australas. Phys. Eng. Sci. Med. 2018, 41, 1021–1027. [Google Scholar] [CrossRef] [PubMed]
- Arilli, C.; Wandael, Y.; Galeotti, C.; Marrazzo, L.; Calusi, S.; Grusio, M.; Desideri, I.; Fusi, F.; Piermattei, A.; Pallotta, S.; et al. Combined Use of a Transmission Detector and an EPID-Based In Vivo Dose Monitoring System in External Beam Whole Breast Irradiation: A Study with an Anthropomorphic Female Phantom. Appl. Sci. 2020, 10, 7611. [Google Scholar] [CrossRef]
- Esposito, M.; Ghirelli, A.; Pini, S.; Alpi, P.; Barca, R.; Fondelli, S.; Leonulli, B.G.; Paoletti, L.; Rossi, F.; Bastiani, P.; et al. Clinical implementation of 3D in vivo dosimetry for abdominal and pelvic stereotactic treatments. Radiother. Oncol. 2021, 154, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Bossuyt, E.; Weytjens, R.; Nevens, D.; De Vos, S.; Verellen, D. Evaluation of automated pre-treatment and transit in-vivo dosimetry in radiotherapy using empirically determined parameters. Phys. Imaging Radiat. Oncol. 2020, 16, 113–129. [Google Scholar] [CrossRef] [PubMed]
- ICRU: Prescribing, Recording, and Reporting Photon-Beam Intensity-Modulated Radiation Therapy (IMRT); ICRU Report 83, J. ICRU; Oxford University Press: Oxford, UK, 2010; Volume 10.
- Esposito, M.; Piermattei, A.; Bresciani, S.; Orlandini, L.C.; Falco, M.D.; Giancaterino, S.; Cilla, S.; Ianiro, A.; Nigro, R.; Botez, L.; et al. Improving dose delivery accuracy with EPID in vivo dosimetry: Results from a multicenter study. Strahlenther. Und Onkol. 2021, 197, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Mijnheer, B.J.; González, P.; Olaciregui-Ruiz, I.; Rozendaal, R.A.; van Herk, M.; Mans, A. Overview of 3-year experience with large-scale electronic portal imaging device–based 3-dimensional transit dosimetry. Pract. Radiat. Oncol. 2015, 5, e679–e687. [Google Scholar] [CrossRef] [PubMed]
- Hanson, I.; Hansen, V.N.; Olaciregui-Ruiz, I.; van Herk, M. Clinical implementation and rapid commissioning of an EPID basedin-vivodosimetry system. Phys. Med. Biol. 2014, 59, N171–N179. [Google Scholar] [CrossRef] [PubMed]
- Olaciregui-Ruiz, I.; Vivas-Maiques, B.; Kaas, J.; Perik, T.; Wittkamper, F.; Mijnheer, B.; Mans, A. Transit and non-transit 3D EPID dosimetry versus detector arrays for patient specific QA. J. Appl. Clin. Med. Phys. 2019, 20, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Chendi, A.; Botti, A.; Orlandi, M.; Sghedoni, R.; Iori, M.; Cagni, E. EPID-based 3D dosimetry for pre-treatment FFF VMAT stereotactic body radiotherapy plan verification using dosimetry CheckTM. Phys. Med. 2021, 81, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Olaciregui-Ruiz, I.; Beddar, S.; Greer, P.; Jornet, N.; McCurdy, B.; Paiva-Fonseca, G.; Mijnheer, B.; Verhaegen, F. In vivo dosimetry in external beam photon radiotherapy: Requirements and future directions for research, development, and clinical practice. Phys. Imaging Radiat. Oncol. 2020, 15, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Papanikolaou, N.; Stathakis, S. Dose-calculation algorithms in the context of inhomogeneity corrections for high energy photon beams. Med. Phys. 2009, 36, 4765–4775. [Google Scholar] [CrossRef] [PubMed]
- Marrazzo, L.; Zani, M.; Pallotta, S.; Arilli, C.; Casati, M.; Compagnucci, A.; Talamonti, C.; Bucciolini, M. GafChromic® EBT3 films for patient specific IMRT QA using a multichannel approach. Phys. Med. 2015, 31, 1035–1042. [Google Scholar] [CrossRef] [PubMed]
- Wendling, M.; McDermott, L.N.; Mans, A.; Sonke, J.-J.; Stroom, J.; van Herk, M.; Mijnheer, B.J. In aqua vivo EPID dosimetry. Med. Phys. 2011, 39, 367–377. [Google Scholar] [CrossRef] [PubMed]
- Wendling, M.; Louwe, R.J.W.; McDermott, L.N.; Sonke, J.-J.; Van Herk, M.; Mijnheer, B.J. Accurate two-dimensional IMRT verification using a back-projection EPID dosimetry method. Med. Phys. 2006, 33, 259–273. [Google Scholar] [CrossRef] [PubMed]
- Van Uytven, E.; Van Beek, T.; McCowan, P.M.; Chytyk-Praznik, K.; Greer, P.; McCurdy, B.M.C. Validation of a method for in vivo 3D dose reconstruction for IMRT and VMAT treatments using on-treatment EPID images and a model-based forward-calculation algorithm. Med. Phys. 2015, 42, 6945–6954. [Google Scholar] [CrossRef] [PubMed]
- Micke, A.; Lewis, D.F.; Yu, X. Multichannel film dosimetry with nonuniformity correction. Med. Phys. 2011, 38, 2523–2534. [Google Scholar] [CrossRef] [PubMed]
- Lewis, D.; Micke, A.; Yu, X.; Chan, M.F. An efficient protocol for radiochromic film dosimetry combining calibration and measurement in a single scan. Med. Phys. 2012, 39, 6339–6350. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Plan | Arcs | Beam Energy | Tot MU | Structures Used in Plan Optimization | Dose Prescription Tot (frac) Gy |
|---|---|---|---|---|---|
| Prostate | One 360° arc | 10 MV | 896.3 | PTV; CTV; Bladder; Rectum; Femoral Heads; Penil Bulb | 70.2 (2.7) |
| Brain | One 360° arc | 6 MV | 324.1 | PTV; CTV; Brain, Brainstem, Ocular Bulbs | 24 (2) |
| Head and neck | Four 360° arcs | 6 MV | 838.1 | PTV 70; PTV 60; PTV 54; Parotids glands; Cord; Brainstem | 70–60–54 (2.1–1.8–1.7) |
| Lung | One 180° arc | 6 MV | 439.1 | PTV; CTV; Lungs; Mediastinum; Chest wall | 50 (2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esposito, M.; Marrazzo, L.; Vanzi, E.; Russo, S.; Pallotta, S.; Talamonti, C. A Validation Method for EPID In Vivo Dosimetry Algorithms. Appl. Sci. 2021, 11, 10715. https://doi.org/10.3390/app112210715
Esposito M, Marrazzo L, Vanzi E, Russo S, Pallotta S, Talamonti C. A Validation Method for EPID In Vivo Dosimetry Algorithms. Applied Sciences. 2021; 11(22):10715. https://doi.org/10.3390/app112210715
Chicago/Turabian StyleEsposito, Marco, Livia Marrazzo, Eleonora Vanzi, Serenella Russo, Stefania Pallotta, and Cinzia Talamonti. 2021. "A Validation Method for EPID In Vivo Dosimetry Algorithms" Applied Sciences 11, no. 22: 10715. https://doi.org/10.3390/app112210715
APA StyleEsposito, M., Marrazzo, L., Vanzi, E., Russo, S., Pallotta, S., & Talamonti, C. (2021). A Validation Method for EPID In Vivo Dosimetry Algorithms. Applied Sciences, 11(22), 10715. https://doi.org/10.3390/app112210715