
Are Mechanical Vibrations an Effective Alternative to Accelerate Orthodontic Tooth Movement in Humans? A Systematic Review

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Methods for Identification of Studies
2.2. Sources of Information
2.3. Inclusion Criteria
- (1)
- The study must have evaluated the effectiveness of high- or low-frequency vibratory stimuli in the Orthodontic Tooth Movement (OTM).
- (2)
- Study design: only randomized controlled trials (RCTs) were included in order to evaluate the gold standard articles for judging the benefits of treatments.
- (3)
- Participants: studies where only healthy subjects requiring orthodontic treatment were included.
- (4)
- Type of interventions: subjects must have been assigned to an experimental or control/placebo group in order to receive or not high- or low-frequency vibratory stimuli.
- (5)
- Result type: indicator of tooth movement speed and related treatment parameters.
2.4. Exclusion Criteria
- (1)
- Retrospective design studies, cohort study, case reports, descriptive studies or letters, review articles, and animal studies.
- (2)
- Participants with systematic diseases affecting bone metabolism or orthodontic treatment.
2.5. Search Strategy and Study Selection
2.6. Data Collection Process
2.7. Risk of Bias in Individual Studies
2.8. Evidence Level
3. Results
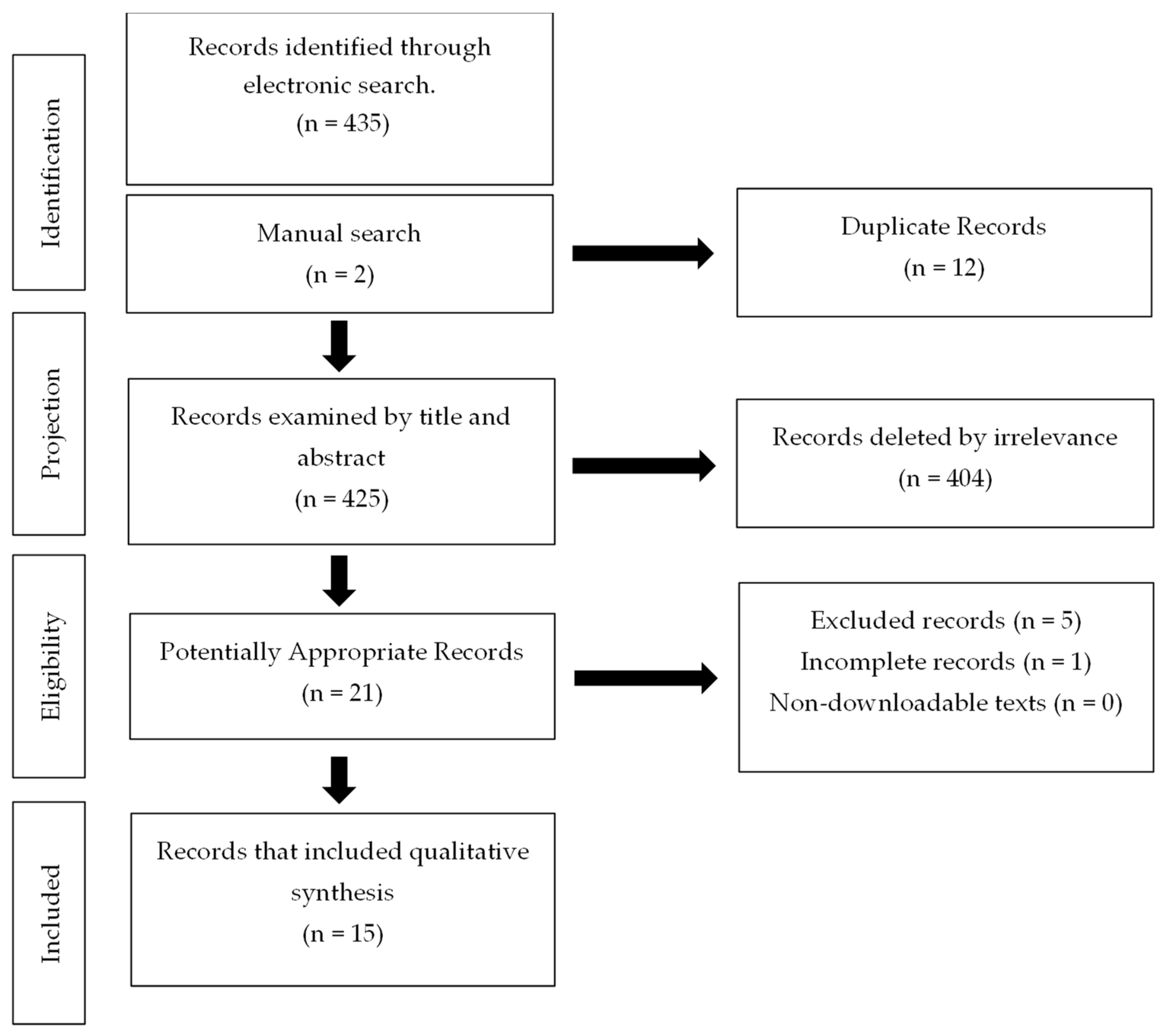
3.1. Selection of Studies
3.2. Characteristics of the Studies
3.3. Risk of Bias in Studies
3.4. Results of Individual Studies
3.5. Assessment of the GRADE Test Certainty
4. Discussion
4.1. High-Frequency Studies
4.2. Low-Frequency Studies
4.3. Studies Carried Out with Electric Toothbrushes
4.4. Studies That Evaluated the Canine Retraction
4.5. Studies That Evaluated the Alignment Phase
5. Excluded Studies
Strengths and Limitations of This Systematic Review
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsichlaki, A.; Chin, S.Y.; Pandis, N.; Fleming, P.S. How long does treatment with fixed orthodontic appliances last? A systematic review. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 308–318. [Google Scholar] [CrossRef]
- El-Bialy, T.; Farouk, K.; Shipley, T. Effect of the application of high-frequency mechanical vibration on tooth length concurrent with orthodontic treatment using clear aligners: A retrospective study. J. Orthod. Sci. 2018, 7, 20. [Google Scholar] [CrossRef]
- Apalimova, A.; Roselló, À.; Jané-Salas, E.; Arranz-Obispo, C.; Marí-Roig, A.; López-López, J. Corticotomy in orthodontic treatment: Systematic review. Heliyon 2020, 6, 1–10. [Google Scholar] [CrossRef]
- Chatmahamongkol, C.; Pravitharangul, A.; Suttapreyasri, S.; Leethanakul, C. The effect of compressive force combined with mechanical vibration on human alveolar bone osteoblasts. J. Oral Biol. Craniofacial Res. 2019, 9, 81–85. [Google Scholar] [CrossRef]
- Padilla, R.G.; Razo, C. Aceleración del tratamiento de ortodoncia: Técnicas de activación biológica. Rev. Latinoam. Ortod. Odontopediatría 2017, 113, 112–120. [Google Scholar]
- Vannala, V.; Katta, A.; Reddy, M.S.; Shetty, S.; Shetty, R.M.; Khazi, S.S. Periodontal Accelerated Osteogenic Orthodontics Technique for Rapid Orthodontic Tooth Movement: A Systematic Review. J. Pharm. Bioallied. Sci. 2019, 11, S97–S106. [Google Scholar] [CrossRef]
- Shapiro, E.; Roeber, F.W.; Klempner, L.S. Orhtodontic movement using pulsating force induced piezoelectricity. Am. J. Orthod. Dentofac. Orthop. 1979, 76, 59–66. [Google Scholar] [CrossRef]
- Bowman, S.J. The Effect of Vibration on Molar Distalization. J. Clin. Orthod. JCO 2016, 50, 683–693. [Google Scholar] [PubMed]
- Bowman, S.J. The effect of vibration on the rate of leveling and alignment. J. Clin. Orthod. JCO 2014, 48, 678–688. [Google Scholar] [PubMed]
- El-Bialy, T.; Shipley, T.; Farouk, K. Effect of high-frequency vibration on orthodontic tooth movement and bone density. J. Orthod. Sci. 2019, 8, 15. [Google Scholar] [CrossRef] [PubMed]
- Alikhani, M.; Alansari, S.; Hamidaddin, M.A.; Sangsuwon, C.; Alyami, B.; Thirumoorthy, S.N.; Oliveira, S.M.; Nervina, J.M.; Teixeira, C.C. Vibration paradox in orthodontics: Anabolic and catabolic effects. PLoS ONE 2018, 13, e0196540. [Google Scholar] [CrossRef] [Green Version]
- Judex, S.; Pongkitwitoon, S. Differential Efficacy of 2 Vibrating Orthodontic Devices to Alter the Cellular Response in Osteoblasts, Fibroblasts, and Osteoclasts. Dose-Response 2018, 16, 1559325818792112. [Google Scholar] [CrossRef] [Green Version]
- Yadav, S.; Dobie, T.; Assefnia, A.; Gupta, H.; Kalajzic, Z.; Nanda, R. Effect of low-frequency mechanical vibration on orthodontic tooth movement. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, M.; Chiba, M.; Ohashi, T.; Sato, M.; Shimizu, Y.; Igarashi, K.; Mitani, H. Periodontal tissue activation by vibration: Intermittent stimulation by resonance vibration accelerates experimental tooth movement in rats. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 572–583. [Google Scholar] [CrossRef]
- Oroszi, T.; van Heuvelen, M.J.G.; Nyakas, C.; van der Zee, E.A. Vibration detection: Its function and recent advances in medical applications. F1000Research 2020, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Catalá-López, F.; Moher, D. La extensión de la declaración PRISMA para revisiones sistemáticas que incorporan metaanálisis en red: PRISMA-NMA. Med. Clin. 2016, 147, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, 332–336. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oñate-Ocaña, L.; Ochoa-Carrillo, F. Sistema GRADE para clasificar nivel de evidencia y grado de las recomendaciones para la elaboración de guías de buena práctica clínica. Cirugía Cir. 2009, 77, 417–419. [Google Scholar]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Miles, P.; Smith, H.; Weyant, R.; Rinchuse, D.J. The effects of a vibrational appliance on tooth movement and patient discomfort: A prospective randomised clinical trial. Aust. Orthod. J. 2012, 28, 213–218. [Google Scholar]
- Pavlin, D.; Anthony, R.; Raj, V.; Gakunga, P.T. Cyclic loading (vibration) accelerates tooth movement in orthodontic patients: A double-blind, randomized controlled trial. Semin. Orthod. 2015, 21, 187–194. [Google Scholar] [CrossRef] [Green Version]
- Woodhouse, N.R.; Dibiase, A.T.; Johnson, N.; Slipper, C.; Grant, J.; Alsaleh, M.; Donaldson, A.N.A.; Cobourne, M.T. Supplemental vibrational force during orthodontic alignment: A randomized trial. J. Dent. Res. 2015, 94, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Leethanakul, C.; Suamphan, S.; Jitpukdeebodintra, S.; Thongudomporn, U.; Charoemratrote, C. Vibratory stimulation increases interleukin-1 beta secretion during orthodontic tooth movement. Angle Orthod. 2015, 86, 74–80. [Google Scholar] [CrossRef] [Green Version]
- Miles, P.; Fisher, E. Assessment of the changes in arch perimeter and irregularity in the mandibular arch during initial alignment with the AcceleDent Aura appliance vs no appliance in adolescents: A single-blind randomized clinical trial. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 928–936. [Google Scholar] [CrossRef]
- Lombardo, L.; Arreghini, A.; Ghislanzoni, L.T.H.; Siciliani, G. Does low-frequency vibration have an effect on aligner treatment? A single-centre, randomized controlled trial. Eur. J. Orthod. 2018, 41, 434–443. [Google Scholar] [CrossRef] [PubMed]
- Liao, Z.; Elekdag-Turk, S.; Turk, T.; Grove, J.; Dalci, O.; Chen, J.; Zheng, K.; Darendeliler, M.A.; Swain, M.; Li, Q. Computational and clinical investigation on the role of mechanical vibration on orthodontic tooth movement. J. Biomech. 2017, 60, 57–64. [Google Scholar] [CrossRef]
- Azeem, M.; Afzal, A.; Jawa, S.A.; Haq, A.U.; Khan, M.; Akram, H. Effectiveness of electric toothbrush as vibration method on orthodontic tooth movement: A split-mouth study. Dent. Press J. Orthod. 2019, 24, 49–55. [Google Scholar] [CrossRef]
- Alansari, S.; Atique, M.I.; Gomez, J.P.; Hamidaddin, M.; Thirumoorthy, S.N.; Sangsuwon, C.; Khoo, E.; Nervina, J.M. The effects of brief daily vibration on clear aligner orthodontic treatment. J. World Fed. Orthod. 2018, 7, 134–140. [Google Scholar] [CrossRef]
- Kannan, S.; Fassul, S.; Singh, A.K.; Arora, N.; Malhotra, A.; Saini, N. Effectiveness and importance of powered tooth brushes in tooth movement. J. Fam. Med. Prim. Care 2019, 8, 2478–2483. [Google Scholar] [CrossRef] [PubMed]
- DiBiase, A.T.; Woodhouse, N.R.; Papageorgiou, S.N.; Johnson, N.; Slipper, C.; Grant, J.; Alsaleh, M.; Khaja, Y.; Cobourne, M.T. Effects of supplemental vibrational force on space closure, treatment duration, and occlusal outcome: A multicenter randomized clinical trial. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 469–480.e4. [Google Scholar] [CrossRef] [Green Version]
- Siriphan, N.; Leethanakul, C.; Thongudomporn, U. Effects of two frequencies of vibration on the maxillary canine distalization rate and RANKL and OPG secretion: A randomized controlled trial. Orthod. Craniofacial Res. 2019, 22, 131–138. [Google Scholar] [CrossRef]
- Taha, K.; Conley, R.S.; Arany, P.; Warunek, S.; Al-Jewair, T. Effects of mechanical vibrations on maxillary canine retraction and perceived pain: A pilot, single-center, randomized-controlled clinical trial. Odontology 2020, 108, 321–330. [Google Scholar] [CrossRef]
- Kumar, V.; Batra, P.; Sharma, K.; Raghavan, S.; Srivastava, A. Comparative assessment of the rate of orthodontic tooth movement in adolescent patients undergoing treatment by first bicuspid extraction and en mass retraction, associated with low-frequency mechanical vibrations in passive self-ligating and conventional brackets: A randomized controlled trial. Int. Orthod. 2020, 18, 696–705. [Google Scholar] [CrossRef] [PubMed]
- Katchooi, M.; Cohanim, B.; Tai, S.; Bayirli, B.; Spiekerman, C.; Huang, G. Effect of supplemental vibration on orthodontic treatment with aligners: A randomized trial. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 336–346. [Google Scholar] [CrossRef] [PubMed]
- DiBiase, A.T.; Woodhouse, N.R.; Papageorgiou, S.N.; Johnson, N.; Slipper, C.; Grant, J.; Alsaleh, M.; Cobourne, M.T. Effect of supplemental vibrational force on orthodontically induced inflammatory root resorption: A multicenter randomized clinical trial. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 918–927. [Google Scholar] [CrossRef] [Green Version]
- Celebi, F.; Turk, T.; Bicakci, A.A. Effects of low-level laser therapy and mechanical vibration on orthodontic pain caused by initial archwire. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Akan, S.; Kocadereli, I.; Aktas, A.; Taşar, F. Effects of maxillary molar intrusion with zygomatic anchorage on the stomatognathic system in anterior open bite patients. Eur. J. Orthod. 2011, 35, 93–102. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Author/ Origin | Sample | Groups | Vibration/ Time | Orthodontic Mechanics | Movement Measurement | Results | Conclusions |
|---|---|---|---|---|---|---|---|
| Pavlin (2015) United States | n = 45 Age: 12–40 | EG: n = 23 CG: n = 22 | AcceleDent (30 Hz, 0.25 N) Until closing space | Canine retraction | Digital caliper in the mouth | The average movement rate was significantly higher for the AcceleDents group at 1.16 mm. | An increase in movement was presented when vibrations were applied as a complement to orthodontic treatment. |
| Woodhouse (2015) United Kingdom, Germany | n = 81; F:41; M:40 Age: 14.06 ± 1.7 | EG: n = 29 NFD = 25 CG: n = 27 | AcceleDent (30 Hz, 0.25 N) 20 min a day for 209 ± 65 days | Alignment of the jaw arch | Plaster Models measured by digital caliper | There were no significant differences. | No evidence that vibrating force can increase alignment rate or reduce the time. |
| Miles (2016) Australia | n = 40 F:26; M:14 Age: 12–13 | EG: n = 20, M:6; F:14 CG: n = 20, M:8; F:12 | AcceleDent (30 Hz, 0.25 N) 20 min a day for 10 weeks | Alignment of jaw front teeth | Plaster models | There were no significant differences. | The device had no effect on increasing the perimeter of the previous arcade, or on reducing irregularity or discomfort. |
| Liao (2017) Australia | n = 13 Age 12–15 | Split-mouth design | Oral B Hamming Bird Vibrating Unit 50 Hz 10 min a day for 28 days | Canine retraction | Digital caliper in the mouth | Canine distalization on the side of vibration was significant | Suggested that the mechanism for OTM acceleration may be more biologically based than mechanically based. |
| Lombardo (2018) Italy | n = 45; F:25; M:20 Age: 14–45 | EG1: n = 15; M:8; F:7 EG2: n = 15; M:4; F:11 CG: n = 15; M:8; F:7 | AcceleDent (30 Hz, 0.25 N) 20 min a day | Aligner treatment | Digital models | There were no significant differences | There were no differences in accuracy between replacing aligners accompanied by low-frequency vibration every 7 days and replacing it every 14 days without vibration. |
| DiBiase (2018) United Kingdom | n = 81 Age: <20 | EG: n = 22; M:11; F:11 NFD: n = 19; M:8; F:11 CG: n = 20; M:11 F:9 | AcceleDent (30 Hz, 0.25 N) 20 min a day throughout treatment | Aligner treatment | Gypsum models | There were no significant differences | Vibratory stimulus combined with fixed appliances does not affect the closure of space, duration of treatment, or occlusal result. |
| Katchooi (2018) U.S.A. | n = 27; F:15; M:12 Age: <18 | EG: n = 13; M:6; F:7 NFD: n = 13; M:6; F:7 | AcceleDent (30 Hz, 0,25 N) 20 min a day for 25 weeks | Aligner treatment | Switching time from aligner to 1 week. | There were no significant differences | The device does not influence the ability to complete a series of aligners. |
| Siriphan (2019) Thailand | n = 60; F:47; M:13 Age: 18–25 | EG (30 Hz): n = M:3; F:17 EG (60 Hz): n = 20; M:5; F:15 CG: n = 20; M:5; F:15. | 30 Hz and 60 Hz in modified toothbrushes. 20 min a day for 3 months. | Canine distalization | Digital models | There were no significant differences | 3 months with vibration of 30 or 60 Hz does not accelerate the movement rate of the canine. |
| Taha (2019) Tokyo | n = 21; F:14; M:7 Age: 11–17 | EG: n = 10; M:3; F:7 CG: n = 11; M:4; F:7 | AcceleDent (30 Hz, 0.25 N) 20 min a day at 7 p.m. for 12 weeks | Canine retraction | Intraoral scanning | There were no significant differences | No statistically significant differences in canine retraction between experimental and control groups. |
| Kumar (2020) India | n = 65; F:35; M:30 Age: 16–17 | LFS: n = 20; M:10; F:10 LFC: n = 20; M:8; F:12 CG: n = 25M:12; F:13 | 30Hz custom-made device by researchers. 20 min a day during space closure | Canine retraction | Digital models | There were no significant differences | Low-frequency vibrations do not increase the rate of dental movement in adolescent patients with early bicuspid extraction or in combination with passive self-linked brackets. |
| Author/ Origin | Sample | Groups | Vibration/ Time | Orthodontic Mechanics | Movement Measurement | Results | Conclusions |
|---|---|---|---|---|---|---|---|
| Miles (2012) Auatralia | n = 66; F:40; M:26 Age: 11–15 | EG: n = 33, M:12; F:21 CG: n = 33 M:4 F:19 | Dental massage device (111 Hz, 0.06 N). 20 min a day for 10 weeks | Alignment of the six jaw anterior teeth | Plaster model | EG = reduction of 65% at 10 weeks, while CG showed a 69% reduction in the same period. | There seems to not be any clinical advantage in the use of the vibratory devices for the early resolution of crowding during initial alignment. |
| Leethanakul (2016) Thailand | n = 15; F:11; M:4 Age: 19–25 | Split-mouth design, (right or left) it was determined randomly | Vibratory Electronic Toothbrush (Colgate) (125 Hz). 15 min a day for 2 months | Retraction of maxillary canines | Plaster Models measured by digital caliper | The amount of movement was greater for the experimental canine than for control, p = 0.001. | Orthodontic force along with vibratory stimuli increased IL-1beta secretion in the gingival crevicular fluid and accelerated movement. |
| Alansari (2018) U.S.A. | n = 60; F:34; M:24 Age: 18–45 | EG2: n = 13; M:5; F:8 EG3: n = 13; M:4; F:9 EG4: n = 13; M:7 F:6 EG5: n = 5; M:2; F:3 CG: n = 13; M:5; F:8 | Vpro5TM (120 Hz)/5 min a day. 5 min a day for four aligners. | Anteroposterior movement rate of a lower anterior | Digital intraoral scans. | There were no significant differences. | Vibration treatment resulted in the significant shortening of time for correction of jaw incisors with transparent aligners. |
| Kannan (2019) India | n = 23; Age: 18–25 | Split-mouth design | Oral B CrossAction Electric Toothbrush ® Dual Power Clean 100–105 Hz. Three times a day for 5 min/3 months | Individual retraction of canines with mini-implants | Gypsum models and digital caliper. | There were no significant differences. | More RCTs are needed to determine whether vibratory devices result in a significant reduction in the duration of orthodontic treatment. |
| Azeem (2019) Pakistan | n = 28; F:10; M:18 Age: 18–24 | Split-mouth design | Oral B Triumph (125 Hz). 20 min day for 60 days. | Canine retraction using a helical spring. Canine distalization | Gypsum models and digital caliper. | There were no significant differences | The application of vibratory stimuli using an electric brush does not accelerate orthodontic tooth movement. |
| Evaluation Period | Study Design | Limitations | Number of Patients | Inconsistency of Results | Indirect Evidence | Other Considerations | Evidence Quality | Feedback |
|---|---|---|---|---|---|---|---|---|
| Tooth movement rate during alignment phase | RCT | Serious limitations. 1,2 | Studies 7 (380) | Serious. 5 | Not serious. | Serious considerations. 6 | --+- Low 7 | There seems not to be any clinical advantage in the use of the vibratory apparatus. |
| Tooth movement rate during canine retraction | RCT | Serious limitations. 3,4 | Studio 8 (270) | Serious. 5 | Not serious. | Serious considerations. 6 | --+- Low 7 | The amount of movement was the same with the use of the vibratory apparatus. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García Vega, M.F.; López Pérez-Franco, L.M.; Dib Kanán, A.; Román Méndez, C.D.; Soto Sainz, J.E.; Reyes Cervantes, E.; Cerda-Cristerna, B.I.; Salas Orozco, M.F.; Casillas Santana, M.A. Are Mechanical Vibrations an Effective Alternative to Accelerate Orthodontic Tooth Movement in Humans? A Systematic Review. Appl. Sci. 2021, 11, 10699. https://doi.org/10.3390/app112210699
García Vega MF, López Pérez-Franco LM, Dib Kanán A, Román Méndez CD, Soto Sainz JE, Reyes Cervantes E, Cerda-Cristerna BI, Salas Orozco MF, Casillas Santana MA. Are Mechanical Vibrations an Effective Alternative to Accelerate Orthodontic Tooth Movement in Humans? A Systematic Review. Applied Sciences. 2021; 11(22):10699. https://doi.org/10.3390/app112210699
Chicago/Turabian StyleGarcía Vega, María Fernanda, Laura Mónica López Pérez-Franco, Alejandro Dib Kanán, Cristian Dionisio Román Méndez, Jesús Eduardo Soto Sainz, Eric Reyes Cervantes, Bernardino Isaac Cerda-Cristerna, Marco Felipe Salas Orozco, and Miguel Angel Casillas Santana. 2021. "Are Mechanical Vibrations an Effective Alternative to Accelerate Orthodontic Tooth Movement in Humans? A Systematic Review" Applied Sciences 11, no. 22: 10699. https://doi.org/10.3390/app112210699
APA StyleGarcía Vega, M. F., López Pérez-Franco, L. M., Dib Kanán, A., Román Méndez, C. D., Soto Sainz, J. E., Reyes Cervantes, E., Cerda-Cristerna, B. I., Salas Orozco, M. F., & Casillas Santana, M. A. (2021). Are Mechanical Vibrations an Effective Alternative to Accelerate Orthodontic Tooth Movement in Humans? A Systematic Review. Applied Sciences, 11(22), 10699. https://doi.org/10.3390/app112210699