A Machine Learning Tool to Predict the Response to Neoadjuvant Chemotherapy in Patients with Locally Advanced Cervical Cancer

 ,
,  ,
, 

 ,
,
Abstract
1. Introduction
2. Materials and Methods
- Accuracy = ,
- Recall (True Positive Rate (TPR)) = ,
- Precision = .
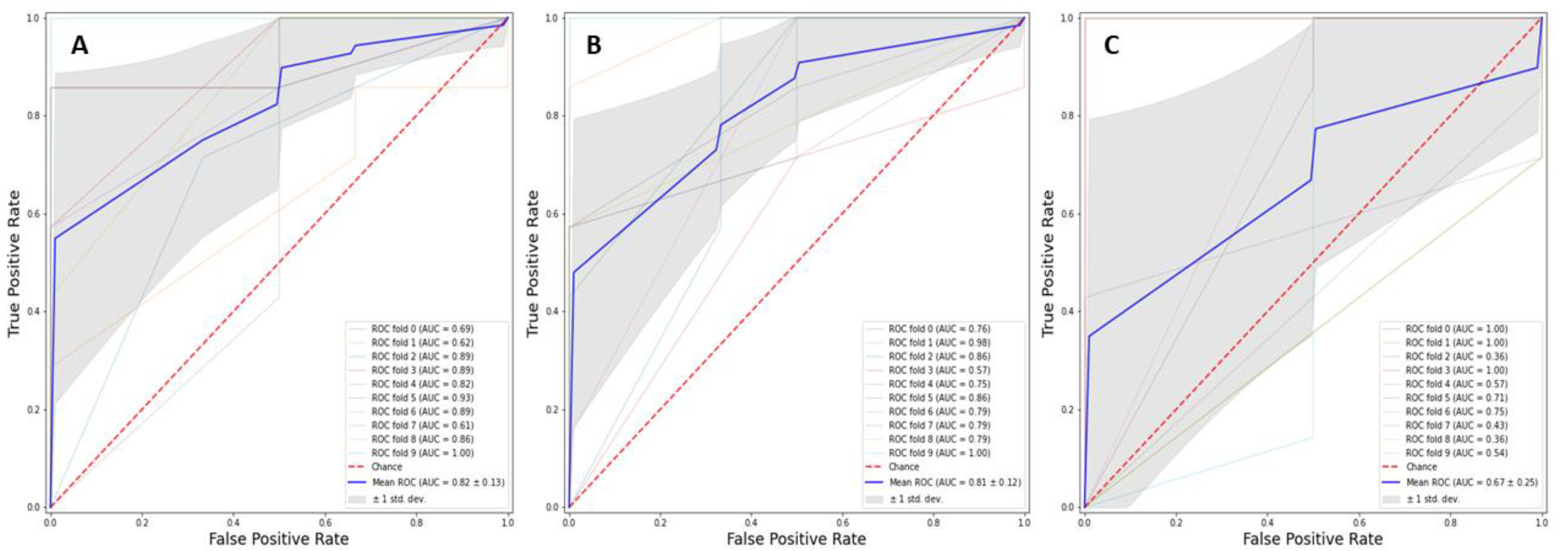
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arbyn, M.; Weiderpass, E.; Bruni, L.; de Sanjose, S.; Saraiya, M.; Ferlay, J.; Bray, F. Estimates of incidence and mortality of cervical cancer in 2018: A worldwide analysis. Lancet Glob. Health 2020, 8, e191–e203. [Google Scholar] [CrossRef]
- Marth, C.; Landoni, F.; Mahner, S.; McCormack, M.; Gonzalez-Martin, A.; Colombo, N. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29 (Suppl. 4), iv262. [Google Scholar] [CrossRef] [PubMed]
- Frumovitz, M.; Sun, C.C.; Schover, L.R.; Munsell, M.F.; Jhingran, A.; Wharton, J.T.; Eifel, P.; Bevers, T.B.; Levenback, C.F.; Gershenson, D.M.; et al. Quality of life and sexual functioning in cervical cancer survivors. J. Clin. Oncol. 2005, 23, 7428–7436. [Google Scholar] [CrossRef] [PubMed]
- Small, W., Jr.; Bacon, M.A.; Bajaj, A.; Chuang, L.T.; Fisher, B.J.; Harkenrider, M.M.; Jhingran, A.; Kitchener, H.; Mileshkin, L.R.; Viswanathan, A.N.; et al. Cervical cancer: A global health crisis. Cancer 2017, 123, 2404–2412. [Google Scholar] [CrossRef] [PubMed]
- Bourgioti, C.; Chatoupis, K.; Moulopoulos, L.A. Current imaging strategies for the evaluation of uterine cervical cancer. World J. Radiol. 2016, 8, 342–354. [Google Scholar] [CrossRef]
- Bhatla, N.; Aoki, D.; Sharma, D.N.; Sankaranarayanan, R. Cancer of the cervix uteri. Int. J. Gynaecol. Obstet. 2018, 143 (Suppl. 2), 22–36. [Google Scholar] [CrossRef]
- Lee, S.I.; Atri, M. 2018 FIGO Staging System for Uterine Cervical Cancer: Enter Cross-sectional Imaging. Radiology 2019, 292, 15–24. [Google Scholar] [CrossRef]
- Balleyguier, C.; Sala, E.; Da Cunha, T.; Bergman, A.; Brkljacic, B.; Danza, F.; Forstner, R.; Hamm, B.; Kubik-Huch, R.; Lopez, C.; et al. Staging of uterine cervical cancer with MRI: Guidelines of the European Society of Urogenital Radiology. Eur. Radiol. 2011, 21, 1102–1110. [Google Scholar] [CrossRef]
- Hameeduddin, A.; Sahdev, A. Diffusion-weighted imaging and dynamic contrast-enhanced MRI in assessing response and recurrent disease in gynaecological malignancies. Cancer Imaging 2015, 15, 3. [Google Scholar] [CrossRef]
- Bipat, S.; Glas, A.S.; van der Velden, J.; Zwinderman, A.H.; Bossuyt, P.M.; Stoker, J. Computed tomography and magnetic resonance imaging in staging of uterine cervical carcinoma: A systematic review. Gynecol. Oncol. 2003, 91, 59–66. [Google Scholar] [CrossRef]
- Chai, Y.; Wang, T.; Wang, J.; Yang, Y.; Gao, Y.; Gao, J.; Gao, S.; Wang, Y.; Zhou, X.; Liu, Z. Radical hysterectomy with adjuvant radiotherapy versus radical radiotherapy for FIGO stage IIB cervical cancer. BMC Cancer 2014, 14, 63. [Google Scholar] [CrossRef] [PubMed]
- Loizzi, V.; Cormio, G.; Vicino, M.; Selvaggi, L. Neoadjuvant chemotherapy: An alternative option of treatment for locally advanced cervical cancer. Gynecol. Obstet. Investig. 2008, 65, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Loizzi, V.; Del Vecchio, V.; Crupano, F.M.; Minicucci, V.; Fumarulo, V.V.; Resta, L.; Vimercati, A.; Bettocchi, S.; Cicinelli, E.; Cormio, G. A phase II study: Dose-dense carboplatin and paclitaxel as neoadjuvant chemotherapy in locally advanced cervical cancer. J. Chemother. 2018, 30, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Benedetti-Panici, P.; Greggi, S.; Colombo, A.; Amoroso, M.; Smaniotto, D.; Giannarelli, D.; Amunni, G.; Raspagliesi, F.; Zola, P.; Mangioni, C.; et al. Neoadjuvant chemotherapy and radical surgery versus exclusive radiotherapy in locally advanced squamous cell cervical cancer: Results from the Italian multicenter randomized study. J. Clin. Oncol. 2002, 20, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Landoni, F.; Maneo, A.; Cormio, G.; Perego, P.; Milani, R.; Caruso, O.; Mangioni, C. Class II versus class III radical hysterectomy in stage IB-IIA cervical cancer: A prospective randomized study. Gynecol. Oncol. 2001, 80, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Neoadjuvant Chemotherapy for Locally Advanced Cervical Cancer Meta-Analysis Collaboration. Neoadjuvant chemotherapy for locally advanced cervical cancer: A systematic review and meta-analysis of individual patient data from 21 randomised trials. Eur. J. Cancer 2003, 39, 2470–2486. [Google Scholar] [CrossRef]
- Venerito, V.; Angelini, O.; Cazzato, G.; Lopalco, G.; Maiorano, E.; Cimmino, A.; Iannone, F. A convolutional neural network with transfer learning for automatic discrimination between low and high-grade synovitis: A pilot study. Intern. Emerg. Med. 2021. ePub ahead of print. [Google Scholar] [CrossRef]
- Johnson, K.W.; Soto, J.T.; Glicksberg, B.S.; Shameer, K.; Miotto, R.; Ali, M.; Ashley, E.; Dudley, J.T. Artificial Intelligence in Cardiology. J. Am. Coll. Cardiol. 2018, 71, 2668–2679. [Google Scholar] [CrossRef]
- Pandit, A.; Radstake, T. Machine learning in rheumatology approaches the clinic. Nat. Rev. Rheumatol. 2020, 16, 69–70. [Google Scholar] [CrossRef]
- Baldini, C.; Ferro, F.; Luciano, N.; Bombardieri, S.; Grossi, E. Artificial neural networks help to identify disease subsets and to predict lymphoma in primary Sjogren’s syndrome. Clin. Exp. Rheumatol. 2018, 36 (Suppl. 112), 137–144. [Google Scholar]
- Rose, P.G.; Java, J.; Whitney, C.W.; Stehman, F.B.; Lanciano, R.; Thomas, G.M.; DiSilvestro, P.A. Nomograms Predicting Progression-Free Survival, Overall Survival, and Pelvic Recurrence in Locally Advanced Cervical Cancer Developed From an Analysis of Identifiable Prognostic Factors in Patients From NRG Oncology/Gynecologic Oncology Group Randomized Trials of Chemoradiotherapy. J. Clin. Oncol. 2015, 33, 2136–2142. [Google Scholar] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.F.; Korevaar, D.A.; Altman, D.G.; Bruns, D.E.; Gatsonis, C.A.; Hooft, L.; Irwig, L.; Levine, D.; Reitsma, J.B.; De Vet, H.C.W.; et al. STARD 2015 guidelines for reporting diagnostic accuracy studies: Explanation and elaboration. BMJ Open 2016, 6, e012799. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD statement. BJOG Int. J. Obstet. Gynaecol. 2015, 122, 434–443. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; Association for Computing Machinery: New York, NY, USA, 2016; pp. 785–794. [Google Scholar]
- Casalino, G.; Vessio, G.; Consiglio, A. (Eds.) Evaluation of Cognitive Impairment in Pediatric Multiple Sclerosis with Machine Learning: An Exploratory Study of miRNA Expressions. In Proceedings of the 2020 IEEE Conference on Evolving and Adaptive Intelligent Systems (EAIS), Bari, Italy, 27–29 May 2020. [Google Scholar]
- Kamel, E.; Sheikh, S.; Huang, X. Data-driven predictive models for residential building energy use based on the segregation of heating and cooling days. Energy 2020, 206, 118045. [Google Scholar] [CrossRef]
- Zeng, X.; Chen, Y.; Tao, C.; Alphen, D. (Eds.) Feature Selection Using Recursive Feature Elimination for Handwritten Digit Recognition. In Proceedings of the 2009 Fifth International Conference on Intelligent Information Hiding and Multimedia Signal Processing, Kyoto, Japan, 12–14 September 2009. [Google Scholar]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Buitinck, L.; Louppe, G.; Blondel, M.; Pedregosa, F.; Mueller, A.; Grisel, O.; Prettenhofer, P.; Gramfort, A.; Grobler, J.; Layton, R.; et al. API Design for Machine Learning Software: Experiences from the Scikit-Learn Project 1 September 2013. arXiv 2013, arXiv:1309.0238. Available online: https://ui.adsabs.harvard.edu/abs/2013arXiv1309.0238B (accessed on 11 November 2020).
- Altukhova, O. Choice of method imputation missing values for obstetrics clinical data. Procedia Comput. Sci. 2020, 176, 976–984. [Google Scholar] [CrossRef]
- Xiao, M.; Yan, C.; Fu, B.; Yang, S.; Zhu, S.; Yang, D.; Lei, B.; Huang, R.; Lei, J. Risk prediction for postpartum depression based on random forest. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2020, 45, 1215–1222. [Google Scholar]
- Rawashdeh, H.; Awawdeh, S.; Shannag, F.; Henawi, E.; Faris, H.; Obeid, N.; Hyett, J. Intelligent system based on data mining techniques for prediction of preterm birth for women with cervical cerclage. Comput. Biol. Chem. 2020, 85, 107233. [Google Scholar] [CrossRef]
- Zhang, H.; Wang, X.; Ding, R.; Shen, L.; Gao, P.; Xu, H.; Xiu, C.; Zhang, H.; Song, D.; Han, B. Characterization and imaging of surgical specimens of invasive breast cancer and normal breast tissues with the application of Raman spectral mapping: A feasibility study and comparison with randomized single-point detection method. Oncol. Lett. 2020, 20, 2969–2976. [Google Scholar] [CrossRef] [PubMed]
- Khalilia, M.; Chakraborty, S.; Popescu, M. Predicting disease risks from highly imbalanced data using random forest. BMC Med. Inform. Decis. Mak. 2011, 11, 51. [Google Scholar] [CrossRef]
- Krstajic, D.; Buturovic, L.J.; Leahy, D.E.; Thomas, S. Cross-validation pitfalls when selecting and assessing regression and classification models. J. Cheminform. 2014, 6, 10. [Google Scholar] [CrossRef] [PubMed]
- Berrar, D. Performance Measures for Binary Classification. In Encyclopedia of Bioinformatics and Computational Biology; Ranganathan, S., Gribskov, M., Nakai, K., Schönbach, C., Eds.; Academic Press: Oxford, UK, 2019; pp. 546–560. [Google Scholar]
- Kuhn, M.; Johnson, K. Applied Predictive Modeling; Springer: New York, NY, US, 2013. [Google Scholar]
- Matsuo, K.; Purushotham, S.; Jiang, B.; Mandelbaum, R.S.; Takiuchi, T.; Liu, Y.; Roman, L.D. Survival outcome prediction in cervical cancer: Cox models vs. deep-learning model. Am. J. Obstet. Gynecol. 2019, 220, 381.e1–381.e14. [Google Scholar] [CrossRef] [PubMed]
- Komagata, H.; Ichimura, T.; Matsuta, Y.; Ishikawa, M.; Shinoda, K.; Kobayashi, N.; Sasaki, A. Feature analysis of cell nuclear chromatin distribution in support of cervical cytology. J. Med. Imaging 2017, 4, 047501. [Google Scholar] [CrossRef] [PubMed]
- Mariarputham, E.J.; Stephen, A. Nominated texture based cervical cancer classification. Comput. Math. Methods Med. 2015, 2015, 586928. [Google Scholar] [CrossRef] [PubMed]
- Kahng, J.; Kim, E.H.; Kim, H.G.; Lee, W. Development of a cervical cancer progress prediction tool for human papillomavirus-positive Koreans: A support vector machine-based approach. J. Int. Med. Res. 2015, 43, 518–525. [Google Scholar] [CrossRef]
- Sato, M.; Horie, K.; Hara, A.; Miyamoto, Y.; Kurihara, K.; Tomio, K.; Yokota, H. Application of deep learning to the classification of images from colposcopy. Oncol. Lett. 2018, 15, 3518–3523. [Google Scholar] [CrossRef]
- Wang, J.; Li, L.; Yang, P.; Chen, Y.; Zhu, Y.; Tong, M.; Hao, Z.; Li, X. Identification of cervical cancer using laser-induced breakdown spectroscopy coupled with principal component analysis and support vector machine. Lasers Med. Sci. 2018, 33, 1381–1386. [Google Scholar] [CrossRef]
- Gu, J.; Fu, C.Y.; Ng, B.K.; Liu, L.B.; Lim-Tan, S.K.; Lee, C.G. Enhancement of early cervical cancer diagnosis with epithelial layer analysis of fluorescence lifetime images. PLoS ONE 2015, 10, e0125706. [Google Scholar] [CrossRef]
- Baltzer, N.; Sundstrom, K.; Nygard, J.F.; Dillner, J.; Komorowski, J. Risk stratification in cervical cancer screening by complete screening history: Applying bioinformatics to a general screening population. Int. J. Cancer 2017, 141, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Torheim, T.; Malinen, E.; Hole, K.H.; Lund, K.V.; Indahl, U.G.; Lyng, H.; Kvaal, K.; Futsæther, C. Autodelineation of cervical cancers using multiparametric magnetic resonance imaging and machine learning. Acta Oncol. 2017, 56, 806–812. [Google Scholar] [CrossRef] [PubMed]
- Mu, W.; Chen, Z.; Liang, Y.; Shen, W.; Yang, F.; Dai, R.; Wu, N.; Tian, J. Staging of cervical cancer based on tumor heterogeneity characterized by texture features on (18)F-FDG PET images. Phys. Med. Biol. 2015, 60, 5123–5139. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.S.; Chang, S.W.; Cheah, P.L.; Yap, H.J. Integrative machine learning analysis of multiple gene expression profiles in cervical cancer. PeerJ 2018, 6, e5285. [Google Scholar] [CrossRef]
- Wilhelm, T. Phenotype prediction based on genome-wide DNA methylation data. BMC Bioinform. 2014, 15, 193. [Google Scholar] [CrossRef]
- Weegar, R.; Kvist, M.; Sundstrom, K.; Brunak, S.; Dalianis, H. Finding Cervical Cancer Symptoms in Swedish Clinical Text using a Machine Learning Approach and NegEx. AMIA Annu. Symp. Proc. 2015, 2015, 1296–1305. [Google Scholar]
- Obrzut, B.; Kusy, M.; Semczuk, A.; Obrzut, M.; Kluska, J. Prediction of 5-year overall survival in cervical cancer patients treated with radical hysterectomy using computational intelligence methods. BMC Cancer 2017, 17, 840. [Google Scholar] [CrossRef]
- Gadducci, A.; Teti, G.; Barsotti, C.; Tana, R.; Fanucchi, A.; Orlandini, C.; Fabrini, M.G.; Genazzani, A.R. Clinicopathological variables predictive of clinical outcome in patients with FIGO stage Ib2-IIb cervical cancer treated with cisplatin-based neoadjuvant chemotherapy followed by radical hysterectomy. Anticancer Res. 2010, 30, 201–208. [Google Scholar]
- Liang, Y.; Lu, B.; Chen, X.; Qin, J.; Cheng, X.; Xie, X.; Lü, W. Prognostic value of pathological response to neoadjuvant chemotherapy in bulky stage Ib2 and IIa cervical squamous cell cancer patients. Virchows Arch. 2016, 468, 329–336. [Google Scholar] [CrossRef]
- Uegaki, K.; Shimada, M.; Sato, S.; Deura, I.; Naniwa, J.; Sato, S.; Oishi, T.; Itamochi, H.; Harada, T.; Kigawa, J. Outcome of stage IB2-IIB patients with bulky uterine cervical cancer who underwent neoadjuvant chemotherapy followed by radical hysterectomy. Int. J. Clin. Oncol. 2014, 19, 348–353. [Google Scholar] [CrossRef]
- Benedetti-Panici, P.; Greggi, S.; Scambia, G.; Amoroso, M.; Salerno, M.G.; Maneschi, F.; Cutillo, G.; Paratore, M.; Scorpiglione, N.; Mancuso, S. Long-term survival following neoadjuvant chemotherapy and radical surgery in locally advanced cervical cancer. Eur. J. Cancer 1998, 34, 341–346. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age at diagnosis (years), mean ± SD | 48.9 ± 11.5 | |
| Parity, median (IQR) | 2 (1–3) | |
| Premenopausal, n. (%) | 50 (54.3%) | |
| FIGO stage, n. (%) | ||
| IB2 | 4/92 (4.3%) | |
| IB3 | 23/92 (25%) | |
| IIA1 | 1/92 (1.1%) | |
| IIA2 | 16/92 (17.4%) | |
| IIB | 29/92 (31.5%) | |
| IIIC1 | 19/92 (20.7%) | |
| Neoadjuvant therapy, n. (%) | n. cycles | |
| Paclitaxel-carboplatin | 46/92 (50%) | 9 |
| Cisplatin-vinorelbine | 39/92 (42.4%) | 3 |
| Topotecan-cisplatin | 6/92 (6.5%) | 2 |
| Paclitaxel-ifosfamide-cisplatin | 1/92 (1.1%) | 3 |
| Pre-treatment MRI | ||
| Largest diameter of lesion (mm), mean ± SD | 44.6 ± 10.5 | |
| Lymph node involvement, n. (%) | 19/92 (20.7%) | |
| Fornix infiltration, n. (%) | 46/92 (50%) | |
| Parametrium infiltration, n (%) | 46/92 (50%) | |
| Vescico-vaginal septum infiltration, n (%) | 1 (1.1%) | |
| Recto-vaginal septum infiltration, n (%) | 1 (1.1%) | |
| Post-treatment MRI | ||
| Largest diameter of lesion (mm), mean± SD | 19.6 ± 12.5 | |
| Lymph node involvement, n. (%) | 4/92 (4.3%) | |
| Fornix infiltration, n. (%) | 5/92 (5.4%) | |
| Parametrium infiltration, n (%) | 4/92 (4.3%) | |
| Vescico-vaginal septum infiltration, n (%) | 0 (0) | |
| Recto-vaginal septum infiltration, n (%) | 0 (0) | |
| Recist criteria | ||
| CR, n. (%) | 19/92 (21%) | |
| PR, n. (%) | 67/92 (73%) | |
| SD, n. (%) | 5/92 (6%) | |
| Histotypes, n. (%) | ||
| Squamous cell carcinoma | 70/92 (76.1%) | |
| Adenocarcinoma | 18/92 (19.6%) | |
| Adenosquamous carcinoma | 4/92 (4.3%) | |
| Grading, n. (%) | ||
| G1 | 13/92 (14%) | |
| G2 | 32/92 (35%) | |
| G3 | 47/92 (51%) | |
| pN0, n. (%) | 76/92 (83%) | |
| pN+, n. (%) | 16/92 (17%) | |
| Persistence of cervix disease after NACT | 73/92 (79%) | |
| Further treatment needed | 25/92 (27%) | |
| Youden’s Index Cut-Off | Accuracy (%) | TPR (%) | Precision (%) | AUROC | |
|---|---|---|---|---|---|
| LR | 0.77 | 77.9 | 96.2 | 80.1 | 0.81 |
| RFF | 0.62 | 82.4% | 96.2 | 83.4 | 0.82 |
| KNN | 0.84 | 73.6 | 96.2 | 76.5 | 0.67 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arezzo, F.; La Forgia, D.; Venerito, V.; Moschetta, M.; Tagliafico, A.S.; Lombardi, C.; Loizzi, V.; Cicinelli, E.; Cormio, G. A Machine Learning Tool to Predict the Response to Neoadjuvant Chemotherapy in Patients with Locally Advanced Cervical Cancer. Appl. Sci. 2021, 11, 823. https://doi.org/10.3390/app11020823
Arezzo F, La Forgia D, Venerito V, Moschetta M, Tagliafico AS, Lombardi C, Loizzi V, Cicinelli E, Cormio G. A Machine Learning Tool to Predict the Response to Neoadjuvant Chemotherapy in Patients with Locally Advanced Cervical Cancer. Applied Sciences. 2021; 11(2):823. https://doi.org/10.3390/app11020823
Chicago/Turabian StyleArezzo, Francesca, Daniele La Forgia, Vincenzo Venerito, Marco Moschetta, Alberto Stefano Tagliafico, Claudio Lombardi, Vera Loizzi, Ettore Cicinelli, and Gennaro Cormio. 2021. "A Machine Learning Tool to Predict the Response to Neoadjuvant Chemotherapy in Patients with Locally Advanced Cervical Cancer" Applied Sciences 11, no. 2: 823. https://doi.org/10.3390/app11020823
APA StyleArezzo, F., La Forgia, D., Venerito, V., Moschetta, M., Tagliafico, A. S., Lombardi, C., Loizzi, V., Cicinelli, E., & Cormio, G. (2021). A Machine Learning Tool to Predict the Response to Neoadjuvant Chemotherapy in Patients with Locally Advanced Cervical Cancer. Applied Sciences, 11(2), 823. https://doi.org/10.3390/app11020823