
Anomalous Origin of the Right Vertebral Artery

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
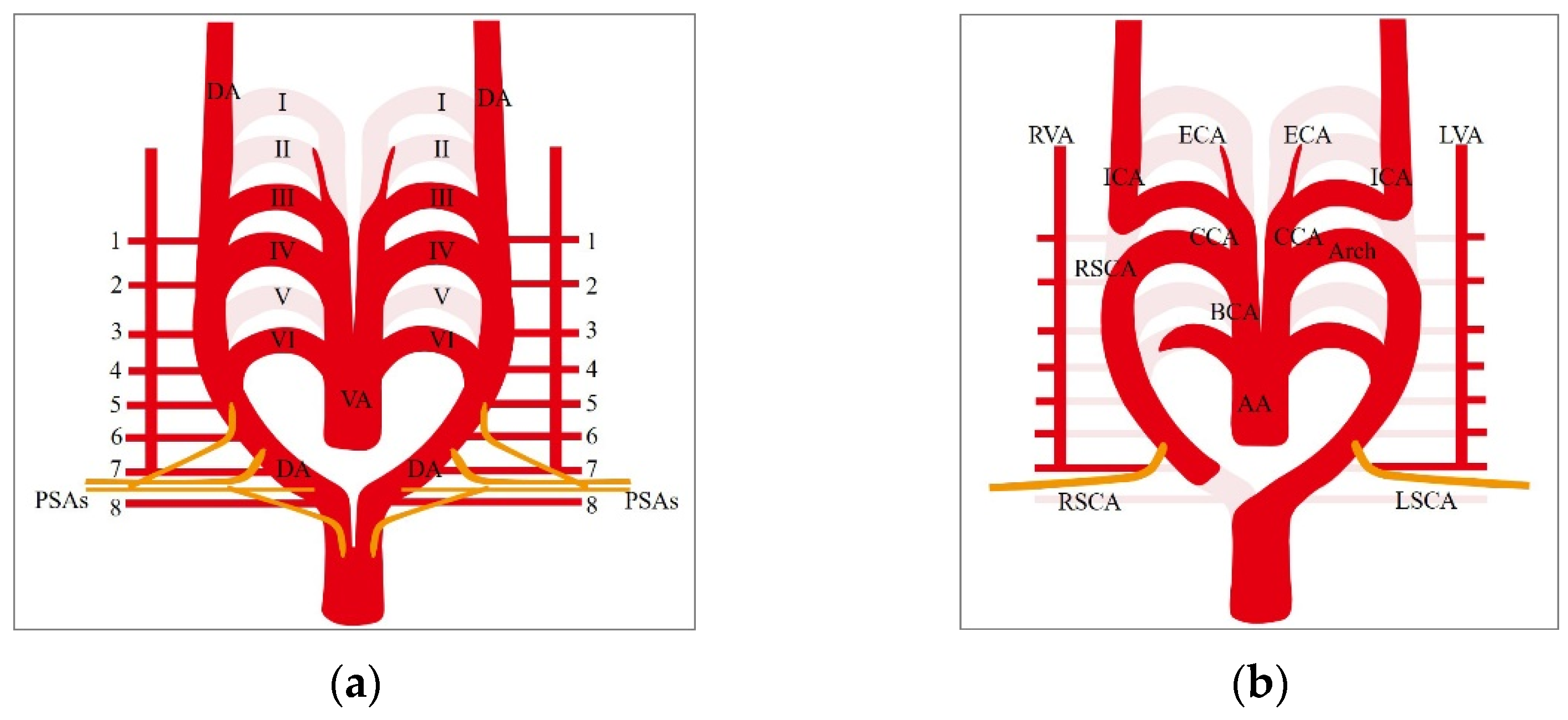
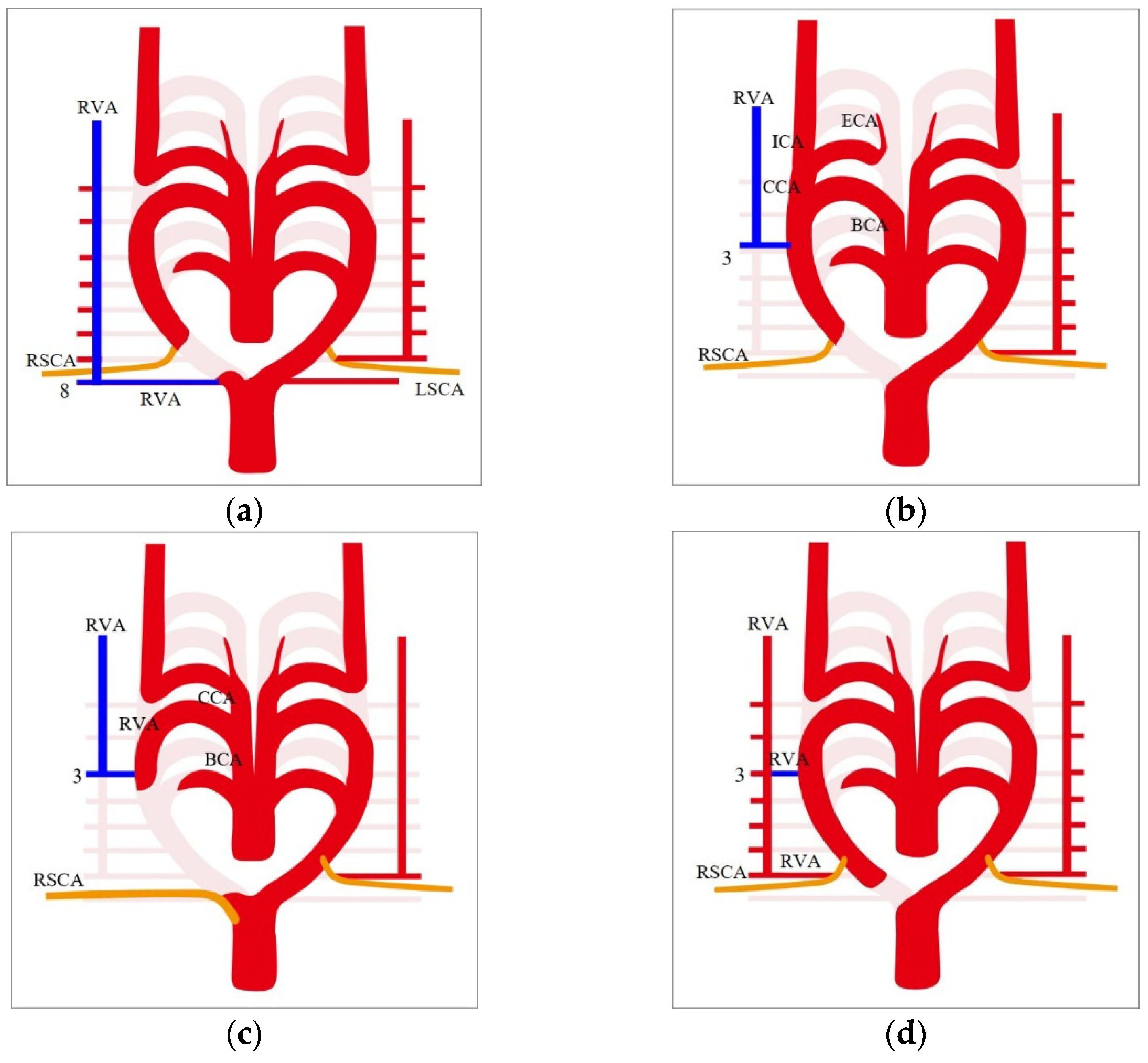
2. Embryological Development and Normal Anatomy of the Proximal Part of the Right Vertebral Artery
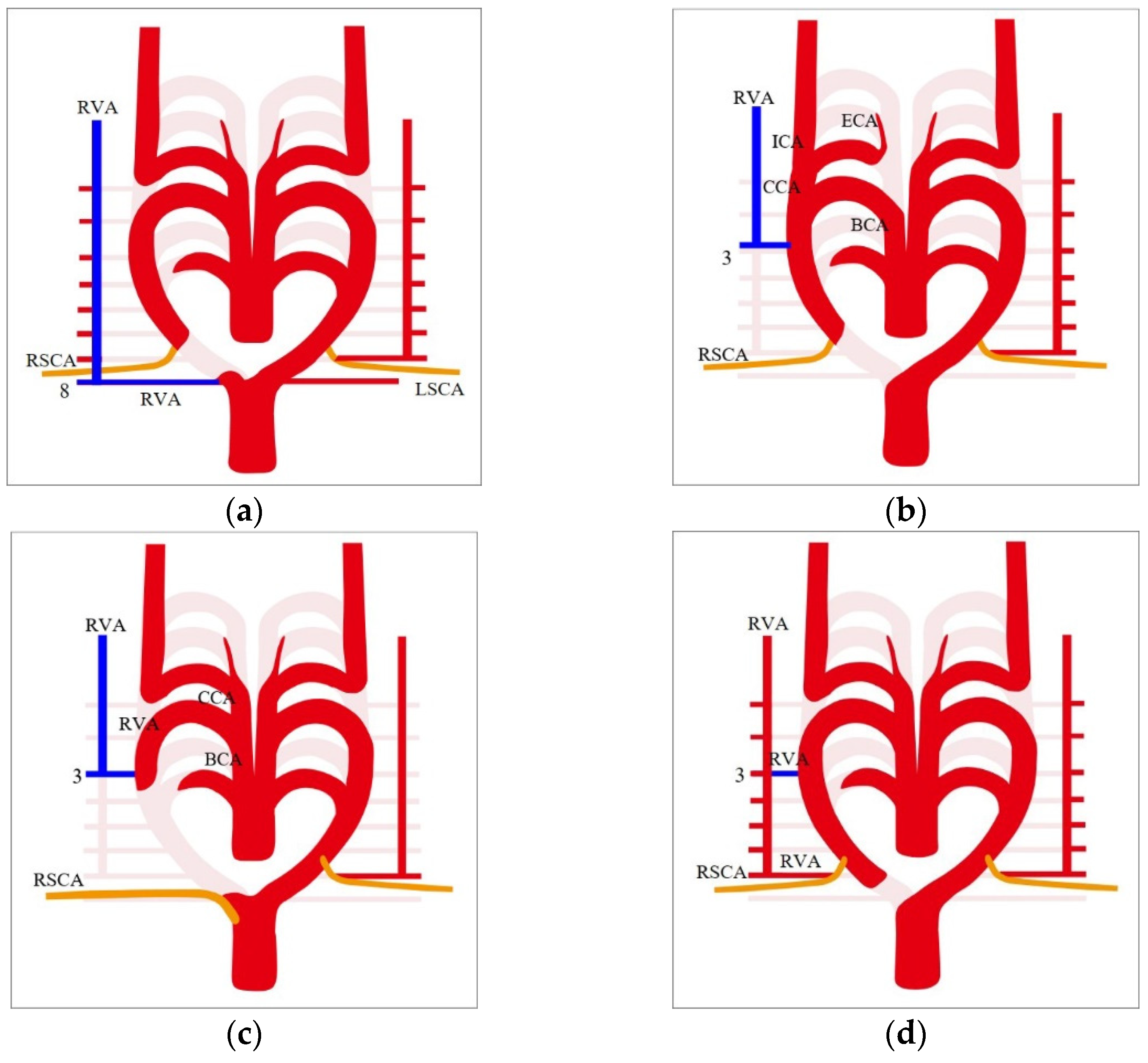
3. Anomalous Origin of the Right Vertebral Artery
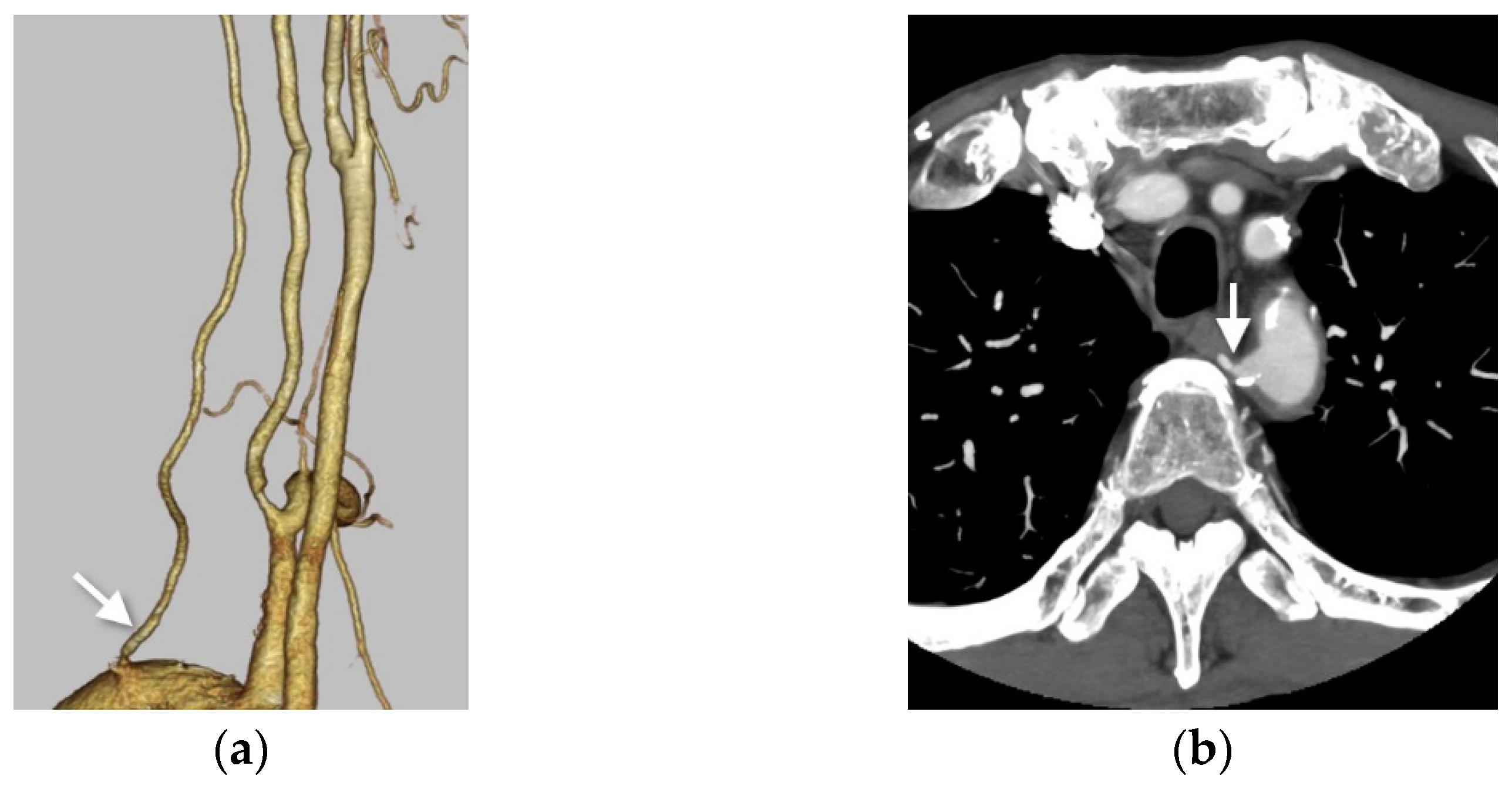
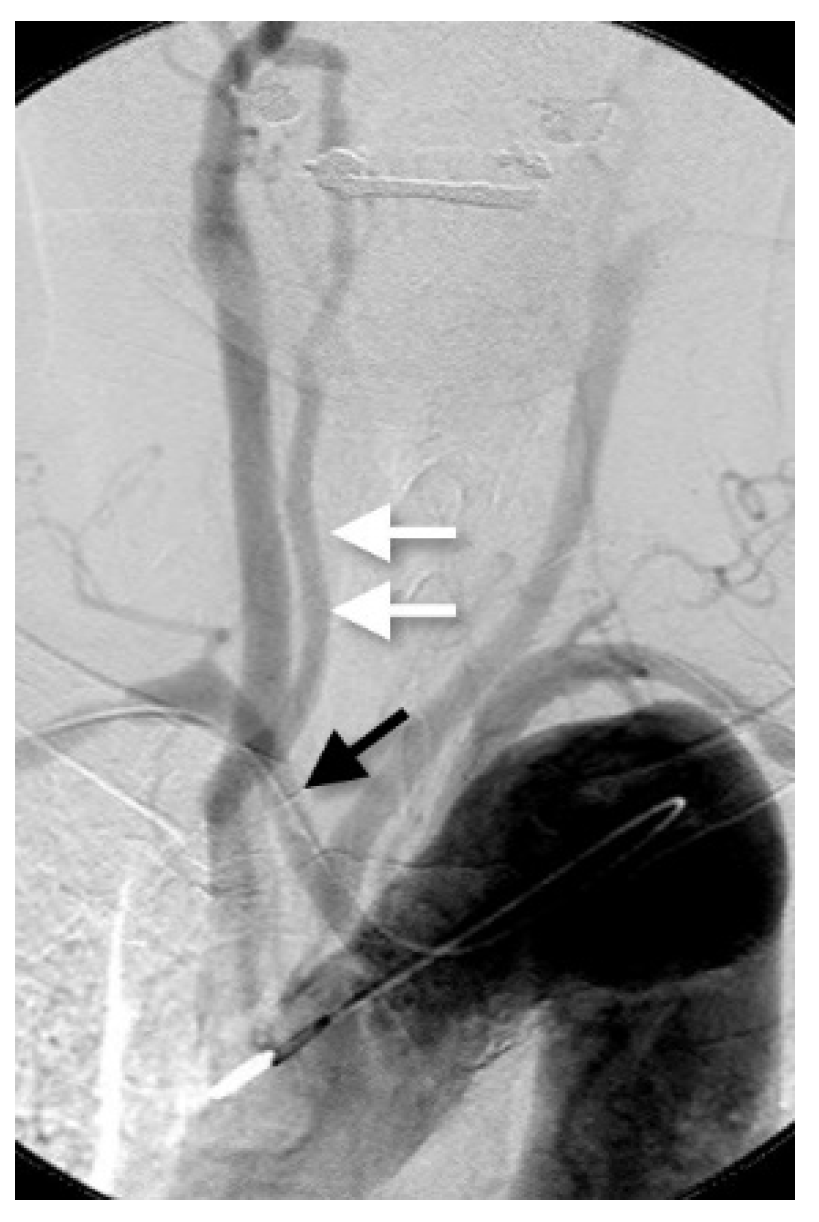
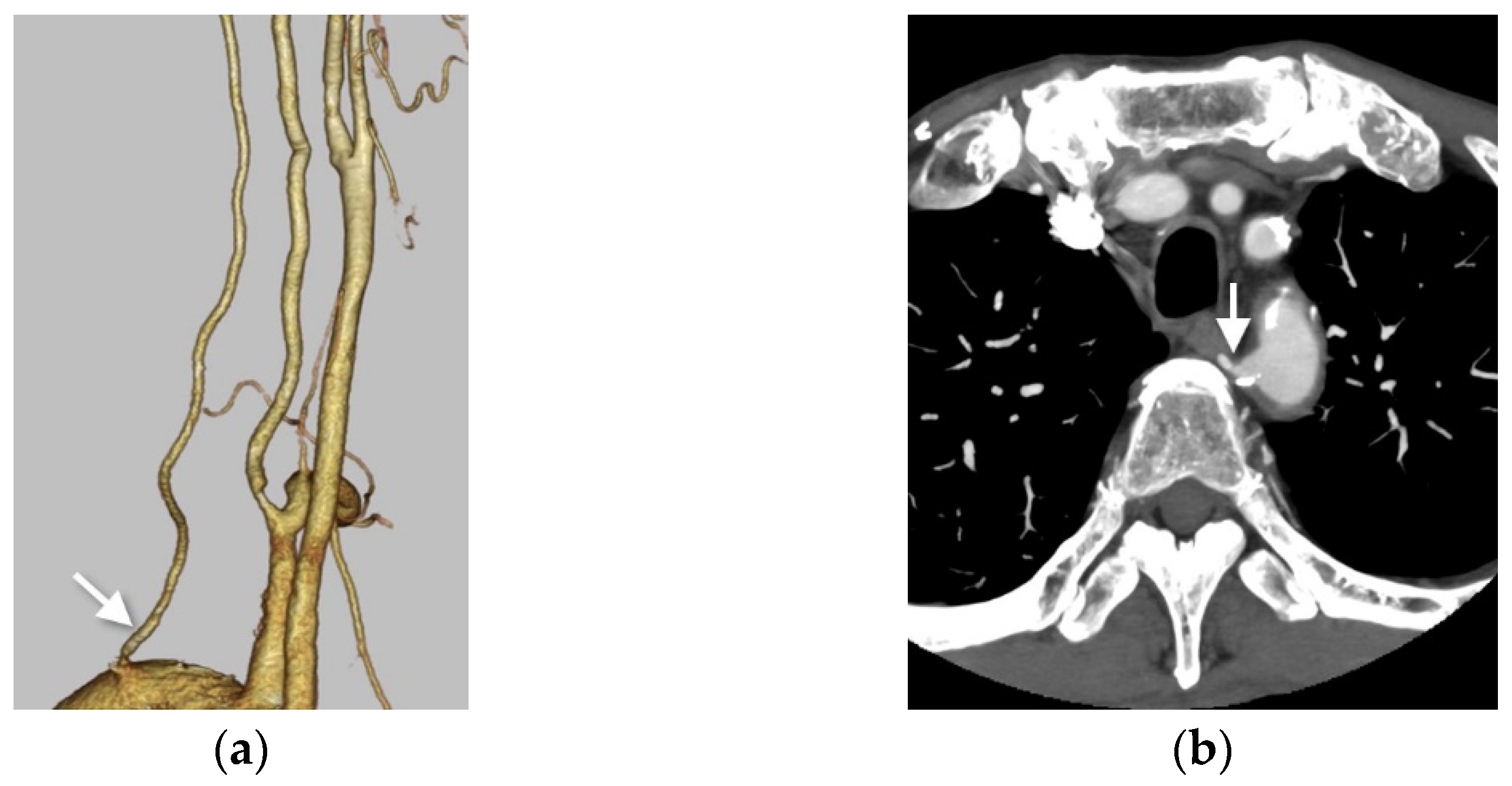
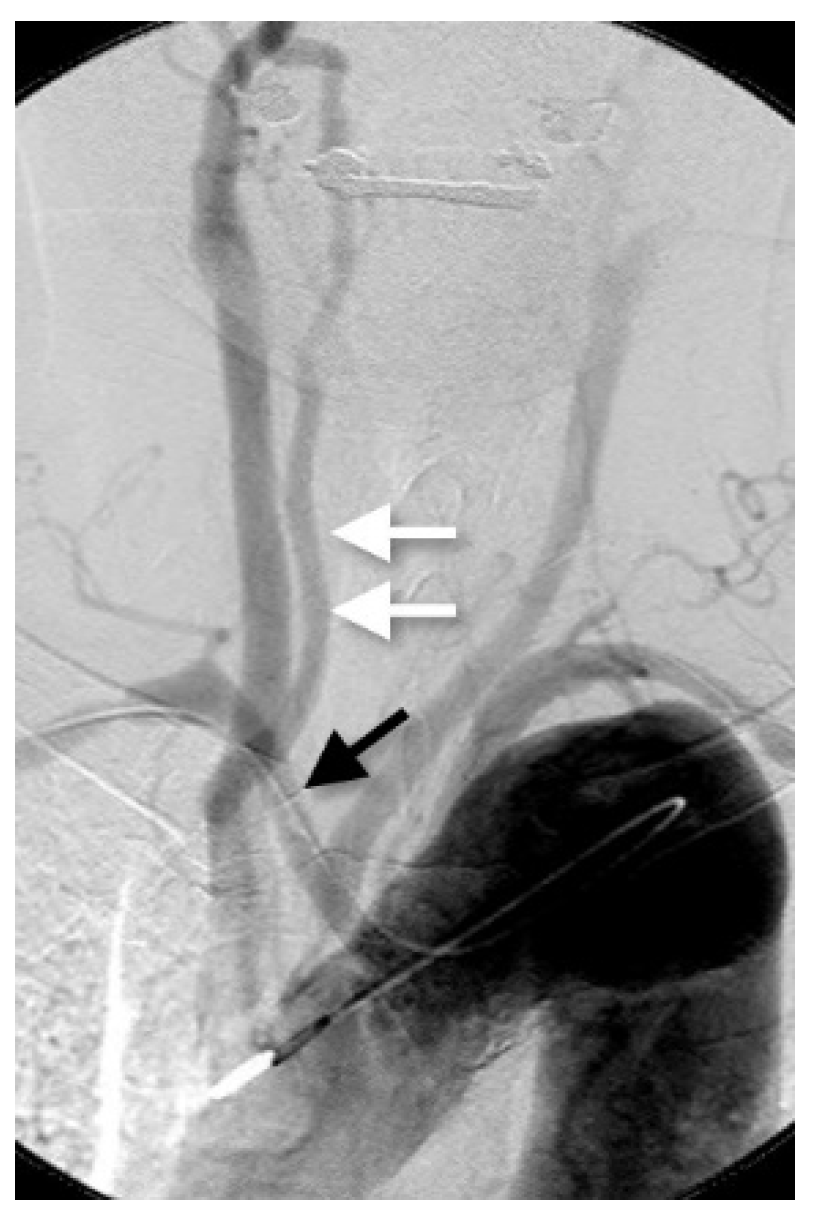
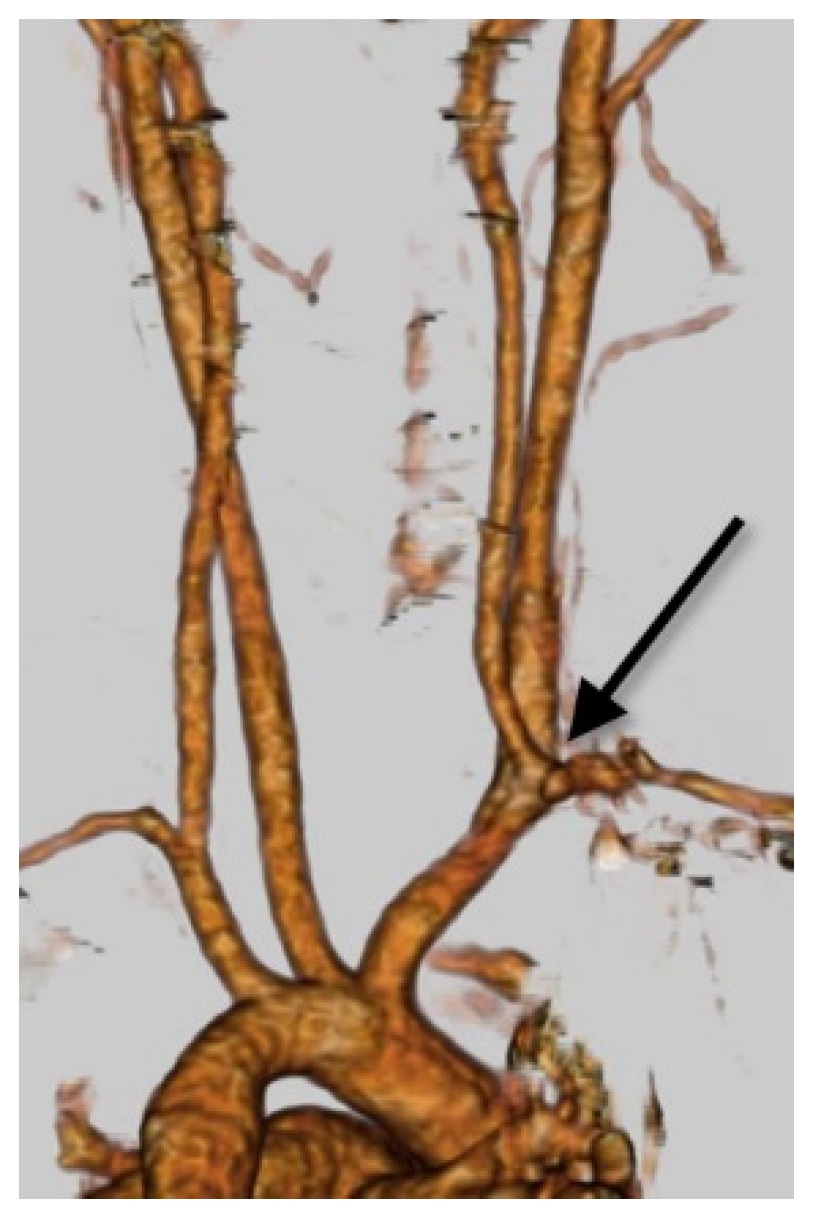
3.1. Right VA Originating from the Aortic Arch (Aortic Origin)
3.2. Right VA Originating from the Common Carotid Artery or the Brachiocephalic Artery
3.3. The Dual Origin of the Right Vertebral Artery
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lazaridis, N.; Piagkou, M.; Loukas, M.; Piperaki, E.T.; Totlis, T.; Noussiou, G.; Natsis, K. A systematic classification of the vertebral artery variable origin: Clinical and surgical implications. Surg. Radiol. Anat. 2018, 40, 779–797. [Google Scholar] [CrossRef] [PubMed]
- Maiti, T.K.; Konar, S.K.; Bir, S.; Nanda, A.; Cuellar, H. Anomalous Origin of the Right Vertebral Artery: Incidence and Significance. World Neurosurg. 2016, 89, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Uchino, A.; Saito, N.; Takahashi, M.; Okada, Y.; Kozawa, E.; Nishi, N.; Mizukoshi, W.; Nakajima, R.; Watanabe, Y. Variations in the origin of the vertebral artery and its level of entry into the transverse foramen diagnosed by CT angiography. Neuroradiology 2013, 55, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Sadler, T.W. Chapter 13 cardiovascular system. In Vascular Development in Langman′s Medical Embryology, 12th ed.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012; pp. 185–191. [Google Scholar]
- Padget, D.H. The development of the cranial arteries in the human embryo. Contrib. Embryol. 1948, 32, 207–261. [Google Scholar]
- Aizawa, Y.; Isogai, S.; Izumiyama, M.; Horiguchi, M. Morphogenesis of the primary arterial trunks of the forelimb in the rat embryos: The trunks originate from the lateral surface of the dorsal aorta independently of the intersegmental arteries. Anat. Embryol. 1999, 200, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Gailloud, P.; Gregg, L.; Pearl, M.S.; San, M.D. Ascending and Descending Thoracic Vertebral Arteries. AJNR Am. J. Neuroradiol. 2017, 38, 327–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemke, A.J.; Benndorf, G.; Liebig, T.; Felix, R. Anomalous origin of the right vertebral artery: Review of the literature and case report of right vertebral artery origin distal to the left subclavian artery. AJNR Am. J. Neuroradiol. 1999, 20, 1318–1321. [Google Scholar] [PubMed]
- Wasserman, B.A.; Mikulis, D.J.; Manzione, J.V. Origin of the right vertebral artery from the left side of the aortic arch proximal to the origin of the left subclavian artery. AJNR Am. J. Neuroradiol. 1992, 13, 355–358. [Google Scholar] [PubMed]
- Akdeniz, B.; Yilmaz, E.; Pekel, N.; Ergul, B.U. Anomalous origin of the right vertebral artery from the ascending aorta in the presence of an aberrant right subclavian artery. Int. J. Cardiovasc. Imaging 2007, 23, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Goldbach, A.; Dass, C.; Surapaneni, K. Aberrant Right Vertebral Artery with a Diverculum of Kommerell: Review of a Rare Aortic Arch Anomaly. J. Radiol. Case Rep. 2018, 12, 19–26. [Google Scholar] [PubMed]
- Vitošević, F.; Vitošević, Z.; Rasulić, L. The right vertebral artery arising from the right common carotid artery: Report of a rare case. Case Reports. Surg. Radiol. Anat. 2020, 42, 1263–1266. [Google Scholar] [CrossRef] [PubMed]
- Kesler, W.W.; Sabat, S.B. Isolated anomalous origin of the vertebral artery from the common carotid artery. Case Reports. Interact. Cardiovasc. Thorac. Surg. 2018, 27, 615–616. [Google Scholar] [CrossRef] [PubMed]
- Baik, J.; Baek, H.J.; Shin, H.S.; Choi, K.H. Duplication of the right vertebral artery: MRA findings and review of the literature. Springerplus 2016, 5, 1123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motomura, M.; Watanabe, K.; Tabira, Y.; Iwanaga, J.; Matsuuchi, W.; Yoshida, D.; Saga, T.; Yamaki, K. A Case of Duplicated Right Vertebral Artery. Kurume. Med. J. 2018, 64, 69–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishijima, M.; Harada, J.; Akai, T.; Endo, S.; Tkaku, A. Operative correction of kinking and coiling at the origin of vertebral artery and stellate ganglionectomy in patients with severe vertigo and dizziness. No Shinkei Geka. 1989, 32, 356–359. [Google Scholar]
- Yuan, S.M. Aberrant Origin of Vertebral Artery and its Clinical Implications. Braz. J. Cardiovasc. Surg. 2016, 31, 52–59. [Google Scholar] [PubMed]
- Le, E.P.V.; Rundo, L.; Tarkin, J.M.; Evans, N.R.; Chowdhury, M.M.; Coughlin, P.A.; Pavey, H.; Wall, C.; Zaccagna, F.; Gallagher, F.A.; et al. Assessing robustness of carotid artery CT angiography radiomics in the identification of culprit lesions in cerebrovascular events. Sci. Rep. 2021, 11, 3499. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Zhang, Q.; Ji, A.; Lv, P.; Zhang, J.; Fu, C.; Lin, J. Identification of high-risk carotid plaque with MRI-based radiomics and machine learning. Eur. Radiol. 2021, 31, 3116–3126. [Google Scholar] [CrossRef] [PubMed]
- Zaccagna, F.; Ganeshan, B.; Arca, M.; Rengo, M.; Napoli, A.; Rundo, L.; Groves, A.M.; Laghi, A.; Carbone, I.; Menezes, L.J. CT texture-based radiomics analysis of carotid arteries identifies vulnerable patients: A preliminary outcome study. Neuroradiology 2021, 63, 1043–1052. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tokuyama, K.; Kiyosue, H.; Baba, H.; Asayama, Y. Anomalous Origin of the Right Vertebral Artery. Appl. Sci. 2021, 11, 8171. https://doi.org/10.3390/app11178171
Tokuyama K, Kiyosue H, Baba H, Asayama Y. Anomalous Origin of the Right Vertebral Artery. Applied Sciences. 2021; 11(17):8171. https://doi.org/10.3390/app11178171
Chicago/Turabian StyleTokuyama, Kohei, Hiro Kiyosue, Hiroshi Baba, and Yoshiki Asayama. 2021. "Anomalous Origin of the Right Vertebral Artery" Applied Sciences 11, no. 17: 8171. https://doi.org/10.3390/app11178171
APA StyleTokuyama, K., Kiyosue, H., Baba, H., & Asayama, Y. (2021). Anomalous Origin of the Right Vertebral Artery. Applied Sciences, 11(17), 8171. https://doi.org/10.3390/app11178171