
Platelet-Rich Fibrin: A Viable Therapy for Endodontic-Periodontal Lesions? A Preliminary Assessment

 ,
,  and
and 
Abstract
:1. Introduction
2. Material and Methods
- P: Patients with endodontic-periodontal lesions
- I: The use of PRF in adjunct to endodontic and periodontal treatment
- C: Open flap debridement or only endodontic treatment
- O: Regenerative potential of PRF in endodontic-periodontal lesions (in terms of probing depth, clinical attachment loss, bleeding on probing, size of periapical lesion)
2.1. Eligibility Criteria
2.2. Literature Search
2.3. Data Extraction
3. Results
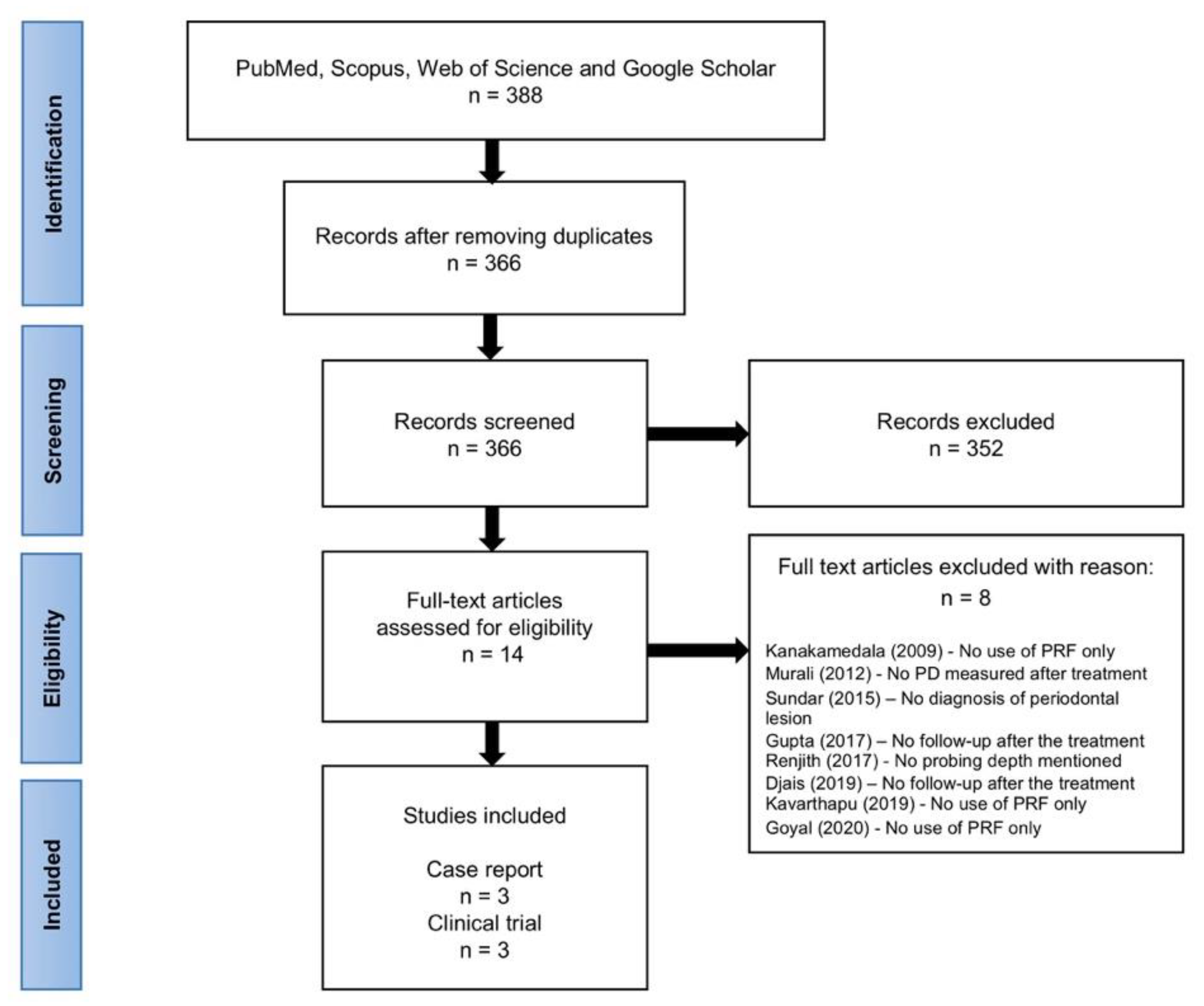
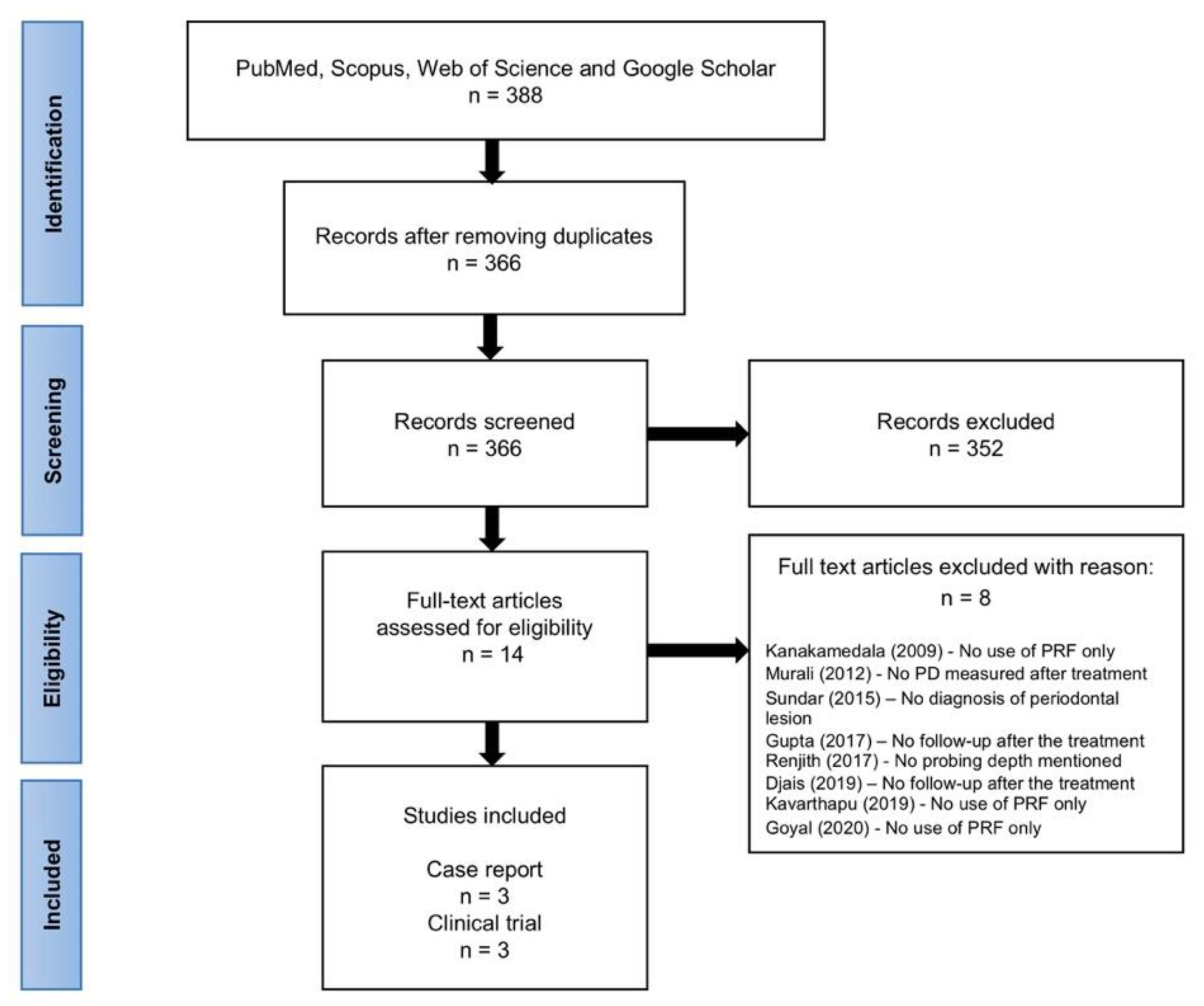
3.1. Search Results
3.2. General Characteristics
3.3. Clinical Assessments for the Diagnosis of Endodontic-Periodontal Lesions
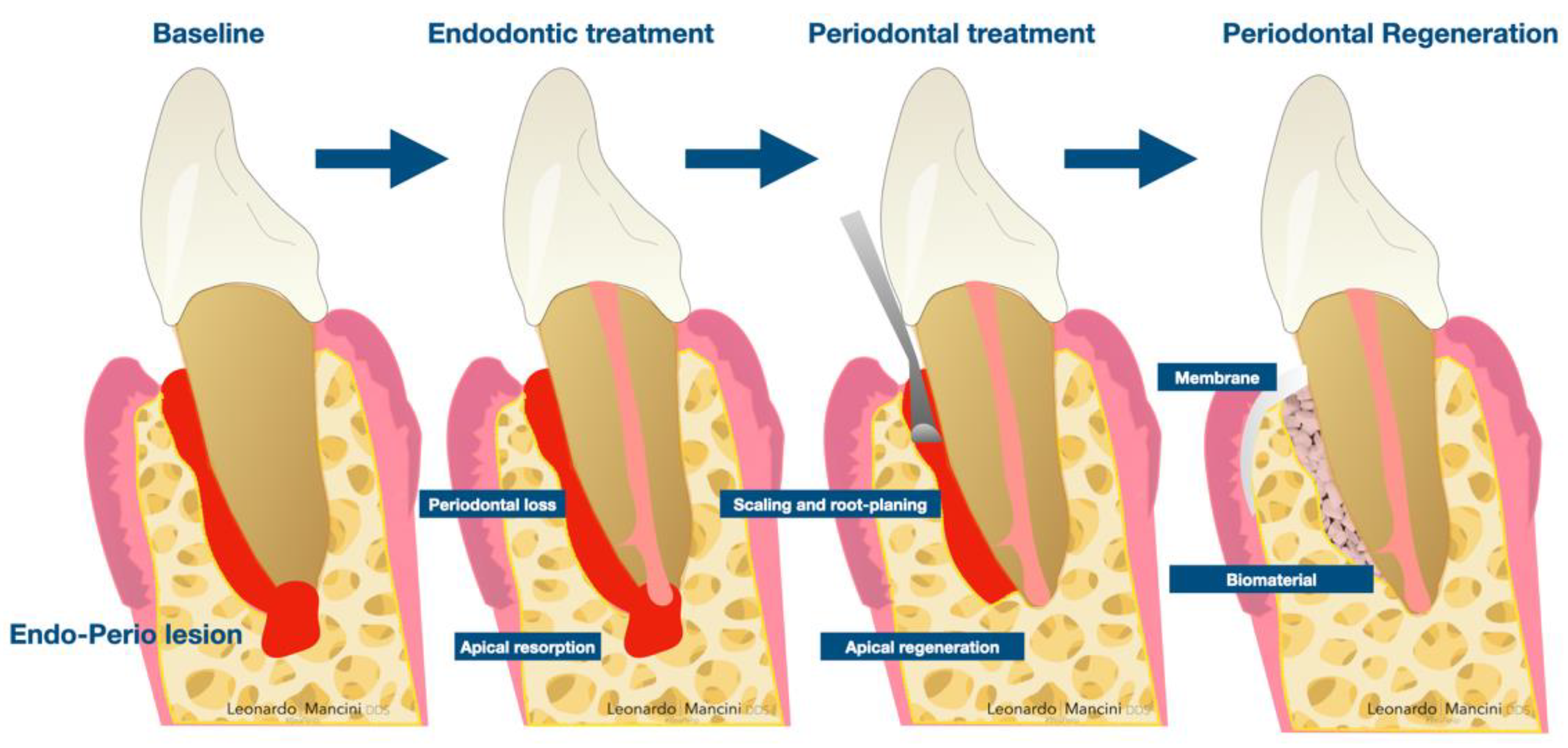
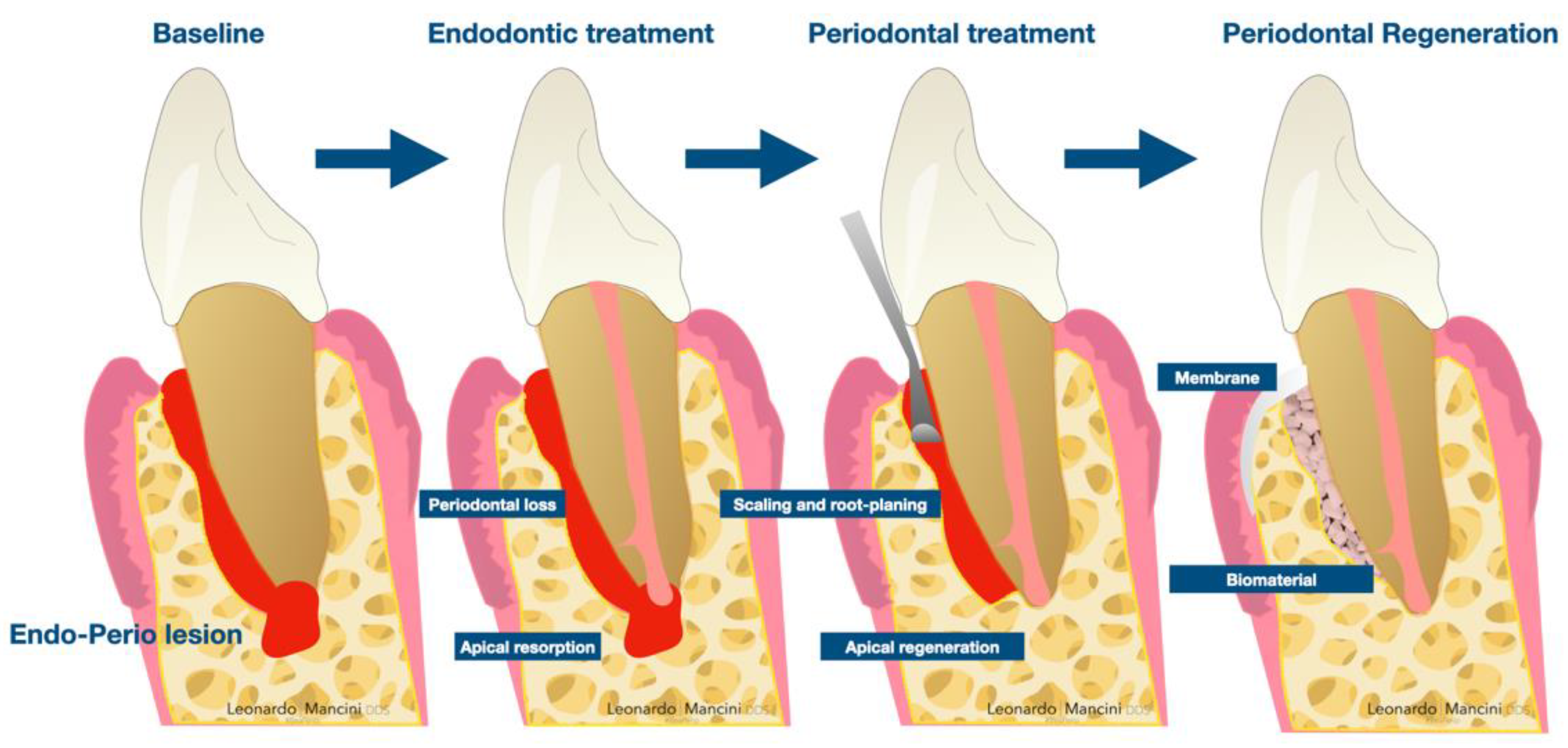
3.4. Treatment of Endodontic-Periodontal Lesions
4. Discussion
5. Conclusion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Rotstein, I.; Simon, J.H.S. Diagnosis, prognosis and decision-making in the treatment of combined periodontal-endodontic lesions. Periodontology 2000 2004, 34, 165–203. [Google Scholar] [CrossRef]
- Simon, J.H.S.; Glick, D.H.; Frank, A.L. The Relationship of Endodontic-Periodontic Lesions. J. Periodontol. 1972, 43, 202–208. [Google Scholar] [CrossRef]
- Newman, M.G.; Takei, H.; Klokkevold, P.R.; Carranza, F.A. Carranza’s Clinical Periodontology, 12th ed.; Elsevier: Philadelphia, PA, USA, 2015. [Google Scholar]
- Walton, R.E.; Torabinejad, M. Principles and Practice of Endodontics, 4th ed.; Elsevier: St. Louis, MO, USA, 2010. [Google Scholar]
- Harrington, G.W.; Steiner, D.R.; Ammons, W.F. The periodontal-endodontic controversy. Periodontol. 2000 2002, 30, 123–130. [Google Scholar] [CrossRef]
- Thorat, M.; Pradeep, A.R.; Pallavi, B. Clinical effect of autologous platelet-rich fibrin in the treatment of intra-bony defects: A controlled clinical trial. J. Clin. Periodontol. 2011, 38, 925–932. [Google Scholar] [CrossRef]
- Murali, K.V.; Shahabe, S.A.; Patil, S.G.; Ahmed, M.N.; Bhandi, S. Periodontal Management of Non Healing Endodontic Lesion—A Case Report. Int. J. Clin. Dent. Sci. 2012, 3, 57931988. [Google Scholar]
- Goyal, L.; Gupta, N.; Gupta, N.D. Autologous platelet-rich derivatives along with alloplastic bone substitute in the management of complex perio-endo cases. J. Indian Soc. Periodontol. 2020, 24, 182–185. [Google Scholar] [CrossRef]
- Marchetti, E.; Mancini, L.; Bernardi, S.; Bianchi, S.; Cristiano, L.; Torge, D.; Marzo, G.; Macchiarelli, G. Evaluation of Different Autologous Platelet Concentrate Biomaterials: Morphological and Biological Comparisons and Considerations. Materials 2020, 13, 2282. [Google Scholar] [CrossRef] [PubMed]
- Miron, R.J.; Chai, J.; Zheng, S.; Feng, M.; Sculean, A.; Zhang, Y. A novel method for evaluating and quantifying cell types in platelet rich fibrin and an introduction to horizontal centrifugation. J. Biomed. Mater. Res. Part A 2019, 107, 2257–2271. [Google Scholar] [CrossRef]
- Choukroun, J.; Diss, A.; Simonpieri, A.; Girard, M.-O.; Schoeffler, C.; Dohan, S.L.; Dohan, A.; Mouhyi, J.; Dohan, D.M. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part IV: Clinical effects on tissue healing. Oral Surgery Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 101, e56–e60. [Google Scholar] [CrossRef] [PubMed]
- Mazzone, N.; Mici, E.; Calvo, A.; Runci, M.; Crimi, S.; Lauritano, F.; Belli, E. Preliminary Results of Bone Regeneration in Oromaxillomandibular Surgery Using Synthetic Granular Graft. BioMed Res. Int. 2018, 2018, 8503427. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part II: Platelet-related biologic features. Oral Surgery Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 101, e45–e50. [Google Scholar] [CrossRef] [PubMed]
- Castro, A.; Cortellini, S.; Temmerman, A.; Li, X.; Pinto, N.; Teughels, W.; Quirynen, M. Characterization of the Leukocyte- and Platelet-Rich Fibrin Block: Release of Growth Factors, Cellular Content, and Structure. Int. J. Oral Maxillofac. Implants 2019, 34, 855–864. [Google Scholar] [CrossRef] [PubMed]
- Kanakamedala, A.; Ari, G.; Sudhakar, U.; Vijayalakshmi, R.; Ramakrishnan, T.; Emmadi, P. Treatment of a Furcation Defect with a Combination of Platelet-Rich Fibrin and Bone Graft-a Case Report. Endod. Pract. Today 2009, 3, 127–135. [Google Scholar]
- Raja, V.S.; Naidu, E.M. Platelet-rich fibrin: Evolution of a second-generation platelet concentrate. Indian J. Dent. Res. 2008, 19, 42. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Sun, X.; Yu, J.; Wang, J.; Zhai, P.; Chen, S.; Liu, M.; Zhou, Y. Platelet-Rich Fibrin as a Bone Graft Material in Oral and Maxillofacial Bone Regeneration: Classification and Summary for Better Application. BioMed Res. Int. 2019, 2019, 1–16. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Jayadev, M.; Shravani, G.S.; Karunakar, P.; Prasanna, J.S. Platelet-rich fibrin, “a faster healing aid” in the treatment of combined lesions: A report of two cases. J. Indian Soc. Periodontol. 2014, 18, 651–655. [Google Scholar] [CrossRef]
- Dhiman, M.; Kumar, S.; Duhan, J.; Sangwan, P.; Tewari, S. Effect of Platelet-rich Fibrin on Healing of Apicomarginal Defects: A Randomized Controlled Trial. J. Endod. 2015, 41, 985–991. [Google Scholar] [CrossRef]
- Nisha, S.; Shashikumar, P. Autologous platelet concentrate as a potential regenerative biomaterial in the treatment of endo-perio lesion. Indian J. Oral Health Res. 2016, 2, 106. [Google Scholar] [CrossRef]
- Betancourt, P.; Elgueta, R.; Fuentes, R. Treatment of endo-periodontal lesion using leukocyte-platelet-rich fibrin. A case report. Colomb. Med. 2017, 48, 204–207. [Google Scholar] [CrossRef] [Green Version]
- Ustaoğlu, G.; Aydin, Z.U.; Özelçi, F. Comparison of GTR, T-PRF and open-flap debridement in the treatment of intrabony defects with endo-perio lesions: A randomized controlled trial. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e117–e123. [Google Scholar] [CrossRef]
- Razi, M.A.; Mahajan, A.; Qamar, S.; Mehra, S.; Roy, T.R.; Kumari, P. A Comparative Study of Platelet-rich Fibrin (PRF) and Titanium-prepared Platelet-rich Fibrin (T-PRF) in Management of Endo-perio Lesions. J. Contemp. Dent. Pract. 2020, 21, 997–1001. [Google Scholar] [CrossRef]
- Sundar, J.S.; Varma, K.M.; Satish, R.K.; Sajjan, G.S.; Tanikonda, R. A Biological Approach in Repair of Damaged Dental Pulp and Periapical Tissues Using Platelet Rich Fibrin, Mineral Trioxide Aggregate and Laser Biostimulation. IJSS Case Rep. Rev. 2015, 1, 44–50. [Google Scholar]
- Renjith, K.P.; Harish Kumar, V.V.; Santhosh, V.C.; Sreekanth, P.; Shabeer, M. PRF and Bonegraft-Magical Tools in Periodontics-A Case Report. Int. J. Periodontol. Implantol. 2017, 2, 23–26. [Google Scholar]
- Gupta, P.; Mittal, S.; Pall, S.; Deswal, H. A Potential Opportunity for Treating Hopeless Tooth with Hemisection and Platelet Rich Fibrin as a Regenerative Tool: A Case Report. IP Int. J. Periodontol. Implantol. 2017, 2, 95–97. [Google Scholar]
- Djais, A.I.; Akbar, F.H.; Adam, M.; Oktawati, S.; Tahir, H.; Gani, A.; Supiaty; Rizki, S.S. Application of Platelet Rich Fibrin (PRF) on Endodontic-Periodontic Lesion in Periodontal Tissue Regereneration: Case Report. J. Int. Dent. Med. Res. 2019, 12, 1189–1195. [Google Scholar]
- Kavarthapu, A.; Malaiappan, S. Management of periodontic-endodontic lesion in aggressive periodontitis-9 months follow-up: Report of a case. Indian J. Dent. Res. 2019, 30, 149–153. [Google Scholar] [PubMed]
- Tsesis, I.; Nemcovsky, C.E.; Nissan, J.; Rosen, E. Endodontic-Periodontal Lesions, 1st ed.; Springer International Publishing: Cham, Switzerland, 2019. [Google Scholar]
- Tanzer, J.M.; Livingston, J.; Thompson, A.M. The Microbiology of Primary Dental Caries in Humans. J. Dent. Educ. 2001, 65, 1028–1037. [Google Scholar] [CrossRef]
- Hirsch, J.-M.; Ahlström, U.; Henrikson, P.-Å.; Heyden, G.; Peterson, L.-E. Periapical surgery. Int. J. Oral Surg. 1979, 8, 173–185. [Google Scholar] [CrossRef]
- Corso, M.D.; Toffler, M.; Ehrenfest, D.M. Use of an Autologous Leukocyte and Plate Let Rich Fibrin (L-PRF) Membrane in Post–Avulsion Sites: An Overview of Choukroun’s PRF. J. Implant Adv. Clin. Dent. 2010, 9, 27–35. [Google Scholar]
- Mise-Omata, S.; Alles, N.; Fukazawa, T.; Aoki, K.; Ohya, K.; Jimi, E.; Obata, Y.; Doi, T. NF-κB RELA-deficient bone marrow macrophages fail to support bone formation and to maintain the hematopoietic niche after lethal irradiation and stem cell transplantation. Int. Immunol. 2014, 26, 607–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michalski, M.N.; Koh, A.J.; Weidner, S.; Roca, H.; McCauley, L.K. Modulation of Osteoblastic Cell Efferocytosis by Bone Marrow Macrophages. J. Cell. Biochem. 2016, 117, 2697–2706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancini, L.; Tarallo, F.; Quinzi, V.; Fratini, A.; Mummolo, S.; Marchetti, E. Platelet-Rich Fibrin in Single and Multiple Coronally Advanced Flap for Type 1 Recession: An Updated Systematic Review and Meta-Analysis. Medicina 2021, 57, 144. [Google Scholar] [CrossRef]
- Tarallo, F.; Mancini, L.; Pitzurra, L.; Bizzarro, S.; Tepedino, M.; Marchetti, E. Use of Platelet-Rich Fibrin in the Treatment of Grade 2 Furcation Defects: Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 2104. [Google Scholar] [CrossRef] [PubMed]
- Bachman, H.; Nicosia, J.; Dysart, M.M.; Barker, T.H. Utilizing Fibronectin Integrin-Binding Specificity to Control Cellular Responses. Adv. Wound Care 2015, 4, 501–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marie, P.J.; Hay, E.; Saidak, Z. Integrin and cadherin signaling in bone: Role and potential therapeutic targets. Trends Endocrinol. Metab. 2014, 25, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Zelzer, E.; McLean, W.; Ng, Y.-S.; Fukai, N.; Reginato, A.M.; Lovejoy, S.; D’Amore, P.A.; Olsen, B.R. Skeletal defects in VEGF120/120 mice reveal multiple roles for VEGF in skeletogenesis. Development 2002, 129, 1893–1904. [Google Scholar] [CrossRef]
- Piché, J.; Graves, D. Study of the growth factor requirements of human bone-derived cells: A comparison with human fibroblasts. Bone 1989, 10, 131–138. [Google Scholar] [CrossRef]
- Hock, J.M.; Centrella, M.; Canalis, E. Insulin-Like Growth Factor I Has Independent Effects on Bone Matrix Formation and Cell Replication. Endocrinology 1988, 122, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Arunachalam, M.; Pulikkotil, S.J.; Sonia, N. Platelet Rich Fibrin in Periodontal Regeneration. Open Dent. J. 2016, 10, 174–181. [Google Scholar] [CrossRef] [Green Version]
- Yajamanya, S.; Chatterjee, A.; Babu, C.; Karunanithi, D. Fibrin network pattern changes of platelet-rich fibrin in young versus old age group of individuals: A cell block cytology study. J. Indian Soc. Periodontol. 2016, 20, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Oktawati, S.; Siswanto, H.; Mardiana, A.; Supiaty; Neormansyah, I.; Basir, I. Endodontic–periodontic lesion management: A systematic review. Med. Clin. Pract. 2020, 3, 100098. [Google Scholar] [CrossRef]
- Mancini, L.; Romandini, M.; Fratini, A.; Americo, L.; Panda, S.; Marchetti, E. Biomaterials for Periodontal and Peri-Implant Regeneration. Materials 2021, 14, 3319. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Product | Protocol | Type of Spin |
|---|---|---|
| PRF | RCF 700 g to 200 g, 12 min | Inclined |
| L-PRF | RCF 700 g, 12 min | Inclined |
| T-PRF | RCF 700 g, 12 min, Titanium tubes | Inclined |
| A-PRF | RCF 200 g, 8 min | Inclined |
| Bio-PRF | RCF700 g, 8 min | Horizontal |
| Author/Ref/Year | n | Age/Sex | Tooth | Diagnosis | Treatment | Before Treatment | Follow-Up after Treatment |
|---|---|---|---|---|---|---|---|
| Case reports | |||||||
| Karunakar et al. [19] 2014 | 2 | 24 years Male: 1 32 years, Female: 1 | Mandibular right first molar Mandibular right first premolar | Primary periodontal lesion with secondary endodontic involvement | Phase I therapy: Root Canal Treatment SRP Phase II therapy: (after 3 months) PRF | PD = 10 mm PD = 8 mm | PD = 4 mm (9 months) PD = 3mm (9 months) |
| Shashikumar and Nisha [21] 2016 | 1 | 52 years Female: 1 | Mandibular left central incisor | Combined endododontic-periodontal lesion | Phase I therapy: SRP + splinting Root Canal Treatment Phase II therapy: (after 3 months) PRF | Grade II mobility PD = 8 mm on DL Sinus tract | Grade I mobility (3 months) PD = 4 mm on DL (12 months) sinus tract healed completely (12 months) |
| Betancourt et al. [22] 2017 | 1 | 52 years Male: 1 | Maxillary left second premolar | Combined endodontic-periodontal lesion | Phase I therapy: Root Canal Treatment Phase II therapy: (after 2 weeks)L-PRF | PD = 11 mm on MB PD = 14 mm on MP No mobility | PD = 3 mm on MB PD = 5 mm on MP (3 months) |
| Clinical studies | |||||||
| Dhiman et al. [20] 2015 | 30 | PRF group Age: 18–45 years Male: 10 Female: 5 Control group Age: 17–42 years Male: 9 Female: 6 | NA | Primary endodontic lesion with secondary periodontal involvement | Phase I therapy: Professional plaque controlPhase II therapy: Root Canal Treatment (MTA) PRF |
PRF group PD = 9.07 CAL = 9.67 GMP = −0.60 SPL = 105.67 Control group PD = 8.67 CAL = 8.80 GMP = −0.07 SPL = 111.73 | PRF group PD = 1.07 CAL = 2.67 GMP = −1.60 SPL = 7.67 (12 months) Control group PD = 1.4 CAL = 2.2 GMP = −0.80 SPL = 6.33 (12 months) |
| Ustaoğlu et al. [23] 2020 | T-PRF group n = 15 GTR group n = 15 OFD alone group n = 15 | Age: 26–59 years Male: 23 Female: 22 | Single rooted teeth | Primary periodontal lesion with secondary endodontic involvement Combined endodontic-periodontal lesion | Phase I therapy: Root Canal Treatment SRP Phase II therapy: (after 6 weeks)a. T-PRF b. GTR (allograft + collagen membrane) c. OFD alone | T-PRF group PD = 9.15 CAL = 9.26 IBD depth = 5.93 GTR group PD = 9.85 CAL = 10.07 IBD depth = 6.76 OFD alone group PD = 9.43 CAL = 9.66 IBD depth = 6.49 | T-PRF group PD = 4.46 CAL = 5.07 IBD depth = 2.95 GTR group PD = 4.17 CAL = 4.57 IBD depth = 2.90 OFD alone group PD = 6.06 CAL = 6.36 IBD depth = 5.59 (9 months) |
| Razi et al. [24] 2020 | 140 | PRF group T-PRF group M = 80, F = 60 18–58 years | Mandibular molars | Primary endodontic lesion with secondary periodontal involvement | Phase I therapy: Root Canal Treatment Phase II therapy: a. PRF b. T-PRF | PRF group PD-mean change: 2.10 (32.68%) (3 months) 2.56 (42.59%) (6 months) RAL-mean change 1.92 (31.20%) (3 months) 2.52 (40.82%) (6 months) | T-PRF group PD-Mean change: 1.91 (33.41%) (3 months) 2.51 (43.90%) (6 months) RAL-mean change: 1.81 (31.60%) (3 months) 2.41 (42.12%) (6 months) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onicas, M.I.; Narita, L.E.; Mester, A.; Onisor, F.; Mancini, L. Platelet-Rich Fibrin: A Viable Therapy for Endodontic-Periodontal Lesions? A Preliminary Assessment. Appl. Sci. 2021, 11, 7081. https://doi.org/10.3390/app11157081
Onicas MI, Narita LE, Mester A, Onisor F, Mancini L. Platelet-Rich Fibrin: A Viable Therapy for Endodontic-Periodontal Lesions? A Preliminary Assessment. Applied Sciences. 2021; 11(15):7081. https://doi.org/10.3390/app11157081
Chicago/Turabian StyleOnicas, Maria Ioana, Laura Elena Narita, Alexandru Mester, Florin Onisor, and Leonardo Mancini. 2021. "Platelet-Rich Fibrin: A Viable Therapy for Endodontic-Periodontal Lesions? A Preliminary Assessment" Applied Sciences 11, no. 15: 7081. https://doi.org/10.3390/app11157081
APA StyleOnicas, M. I., Narita, L. E., Mester, A., Onisor, F., & Mancini, L. (2021). Platelet-Rich Fibrin: A Viable Therapy for Endodontic-Periodontal Lesions? A Preliminary Assessment. Applied Sciences, 11(15), 7081. https://doi.org/10.3390/app11157081