
Will Zirconia Implants Replace Titanium Implants?


Abstract
:Featured Application
Abstract
1. Introduction
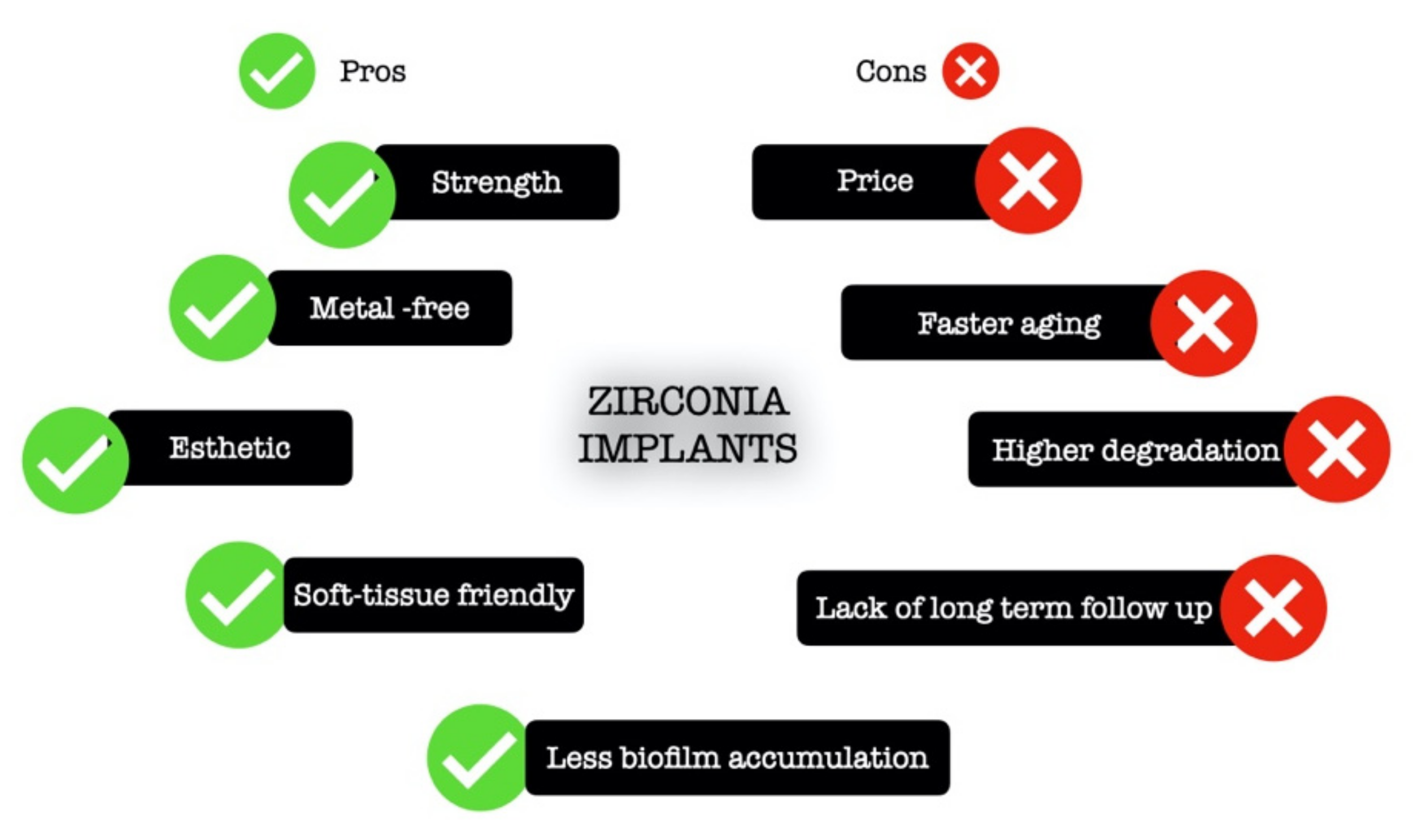
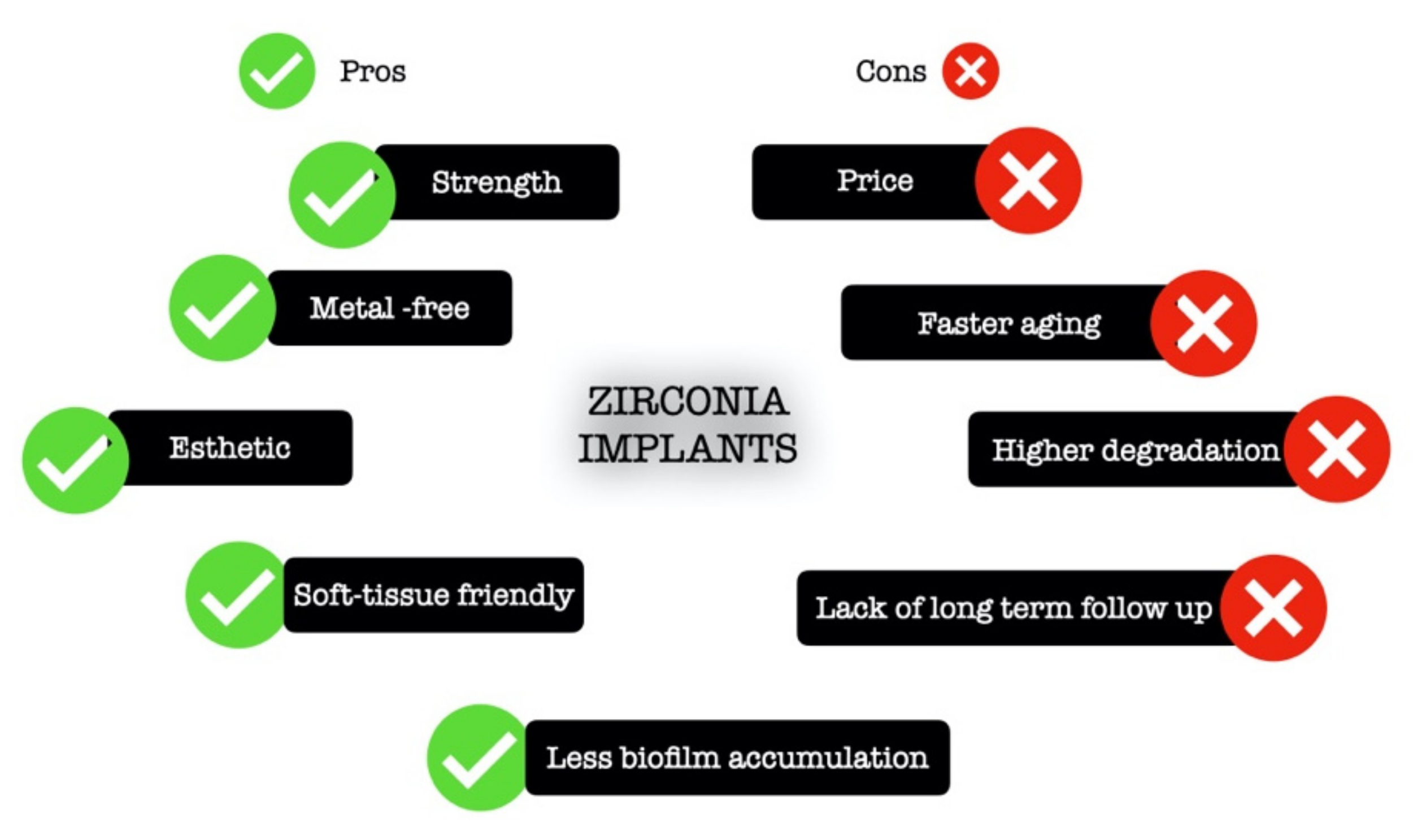
2. What Is a Zirconia Implant?
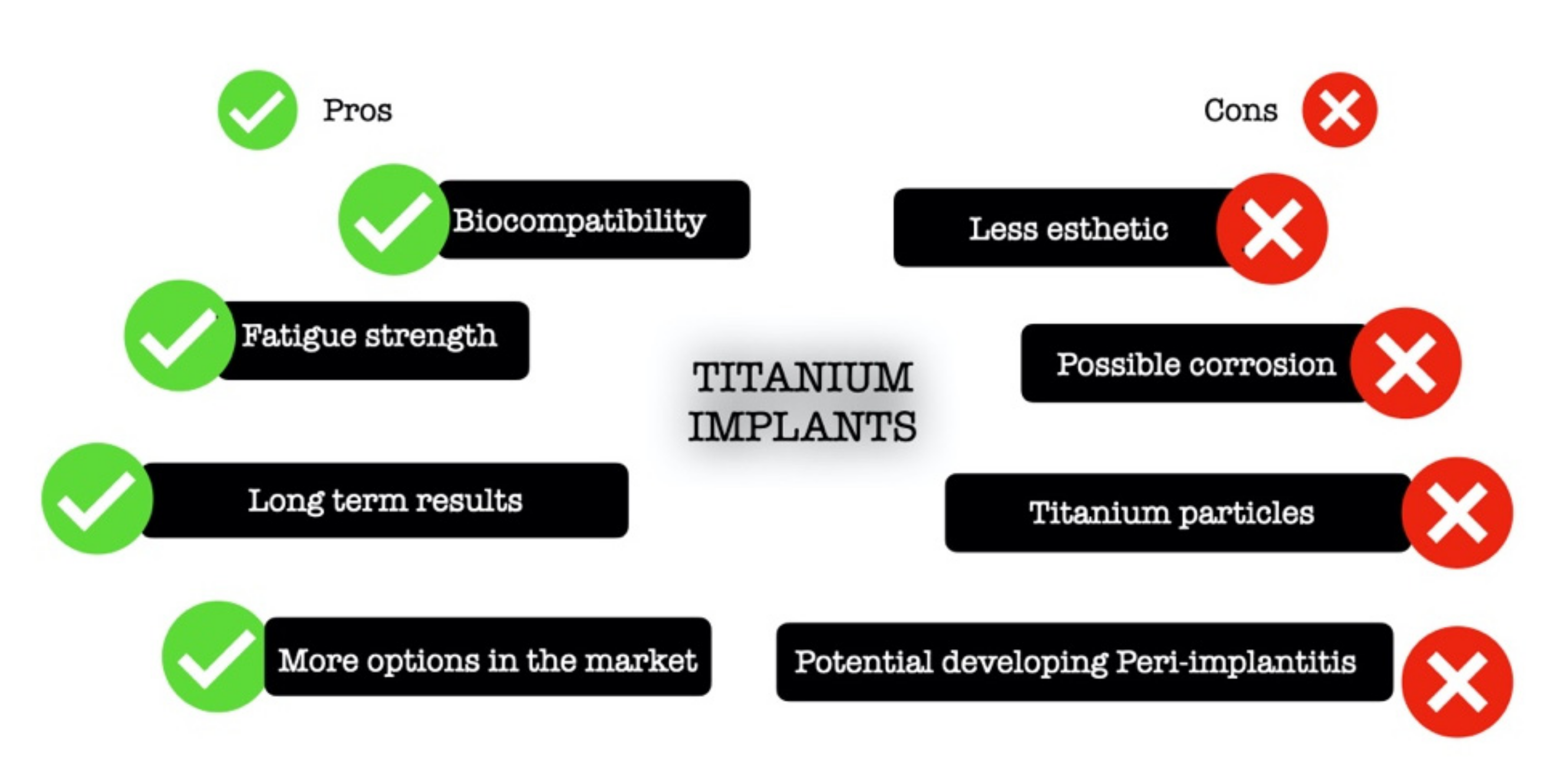
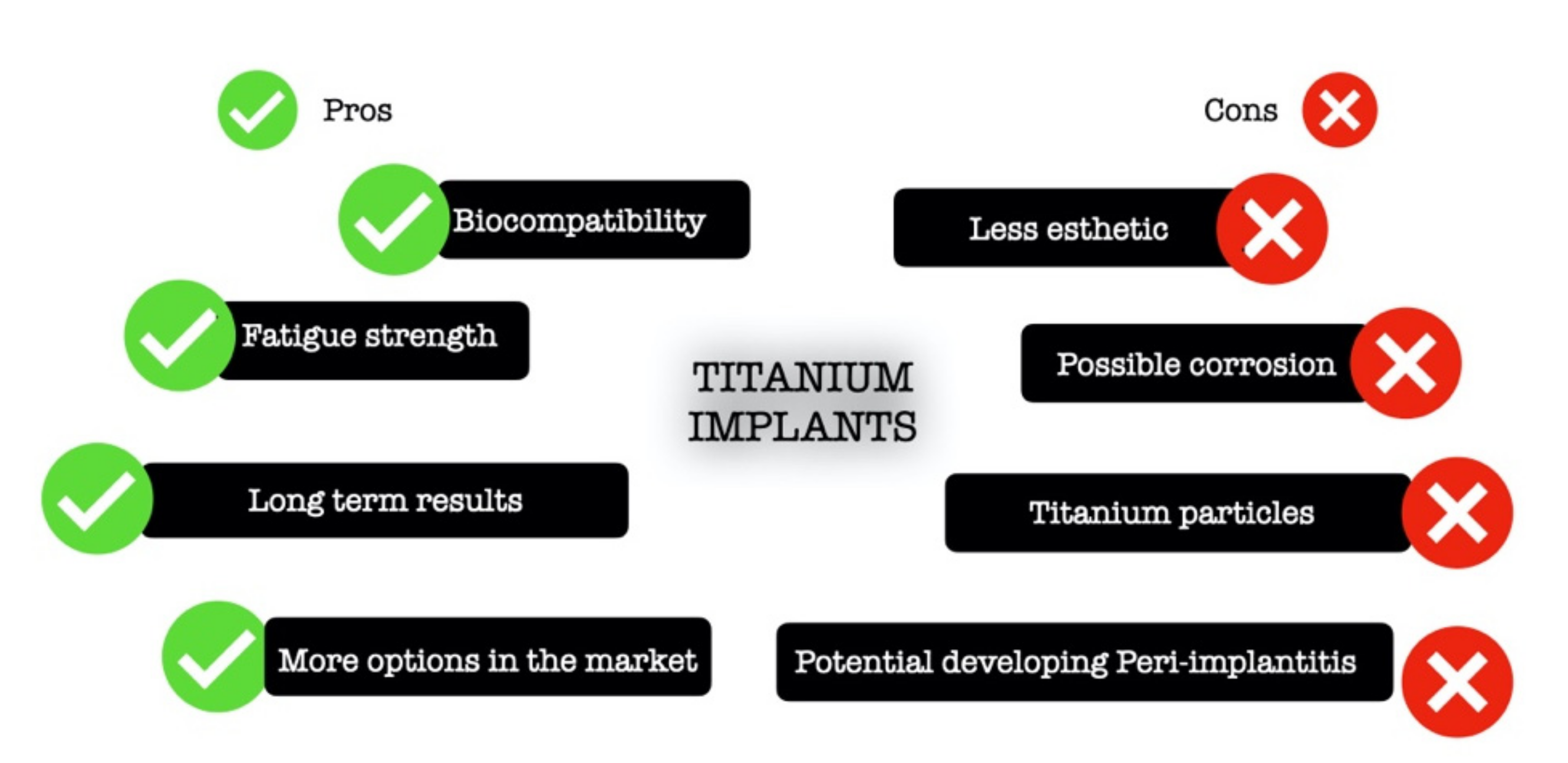
3. What Is a Titanium Implant?
4. Osteointegration
5. Soft Tissue Reaction
6. Microbiota and Peri-Implantitis
7. Long-Term Results
8. Conclusions
- Titanium implants are still the standard material for the replacement of a missing tooth;
- Titanium particles are potentially harmful to the peri-implant tissue; however, more studies are necessary for definitive conclusions;
- Osteointegration of zirconia and titanium implants are similar and are influenced by microstructure and the treatment of the surface;
- Some clinical studies show better soft tissue response with zirconia implants, suggesting that this material can provide a protective effect against inflammation;
- Some studies suggest that zirconia implant seems to be less susceptive to peri-implantitis than titanium implants;
- There is a lack of studies with a long-term follow up of zirconia implants.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S286–S291. [Google Scholar] [CrossRef] [Green Version]
- Kordbacheh Changi, K.; Finkelstein, J.; Papapanou, P.N. Peri-implantitis prevalence, incidence rate, and risk factors: A study of electronic health records at a U.S. dental school. Clin. Oral Implants Res. 2019, 30, 306–314. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, Y.T.; Jeong, S.N.; Kim, N.H.; Lee, D.W. Incidence and pattern of implant fractures: A long-term follow-up multicenter study. Clin. Implant Dent. Relat. Res. 2018, 20, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Vijayaraghavan, V.; Sabane, A.V.; Tejas, K. Hypersensitivity to titanium: A less explored area of research. J. Indian Prosthodont. Soc. 2012, 12, 201–207. [Google Scholar] [CrossRef]
- Kelly, J.R.; Denry, I. Stabilized zirconia as a structural ceramic: An overview. Dent. Mater. 2008, 24, 289–298. [Google Scholar] [CrossRef]
- Wang, T.; Wang, L.; Lu, Q.; Fan, Z. Changes in the esthetic, physical, and biological properties of a titanium alloy abutment treated by anodic oxidation. J. Prosthet. Dent. 2019, 121, 156–165. [Google Scholar] [CrossRef]
- Kim, A.; Campbell, S.D.; Viana, M.A.; Knoernschild, K.L. Abutment Material Effect on Peri-implant Soft Tissue Color and Perceived Esthetics. J. Prosthodont. 2016, 25, 634–640. [Google Scholar] [CrossRef]
- Thoma, D.S.; Ioannidis, A.; Cathomen, E.; Hämmerle, C.H.; Hüsler, J.; Jung, R.E. Discoloration of the Peri-implant Mucosa Caused by Zirconia and Titanium Implants. Int. J. Periodontol. Restor. Dent. 2016, 36, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Cionca, N.; Hashim, D.; Mombelli, A. Zirconia dental implants: Where are we now, and where are we heading? Periodontol. 2000 2017, 73, 241–258. [Google Scholar] [CrossRef]
- Hashim, D.; Cionca, N.; Courvoisier, D.S.; Mombelli, A. A systematic review of the clinical survival of zirconia implants. Clin. Oral Investig. 2016, 20, 1403–1417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koth, D.L.; McKinney, R.V.; Steflik, D.E.; Davis, Q.B. Clinical and statistical analyses of human clinical trials with the single crystal aluminum oxide endosteal dental implant: Five-year results. J. Prosthet. Dent. 1988, 60, 226–234. [Google Scholar] [CrossRef]
- Vagkopoulou, T.; Koutayas, S.O.; Koidis, P.; Strub, J.R. Zirconia in dentistry: Part 1. Discovering the nature of an upcoming bioceramic. Eur. J. Esthet. Dent. 2009, 4, 130–151. [Google Scholar] [PubMed]
- Kunrath, M.F.; Gupta, S.; Lorusso, F.; Scarano, A.; Noumbissi, S. Oral Tissue Interactions and Cellular Response to Zirconia Implant-Prosthetic Components: A Critical Review. Materials 2021, 14, 2825. [Google Scholar] [CrossRef]
- Covacci, V.; Bruzzese, N.; Maccauro, G.; Andreassi, C.; Ricci, G.A.; Piconi, C.; Marmo, E.; Burger, W.; Cittadini, A. In vitro evaluation of the mutagenic and carcinogenic power of high purity zirconia ceramic. Biomaterials 1999, 20, 371–376. [Google Scholar] [CrossRef]
- Piconi, C.; Maccauro, G. Zirconia as a ceramic biomaterial. Biomaterials 1999, 20, 1–25. [Google Scholar] [CrossRef]
- Sivaraman, K.; Chopra, A.; Narayan, A.I.; Balakrishnan, D. Is zirconia a viable alternative to titanium for oral implant? A critical review. J. Prosthodont. Res. 2018, 62, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Lughi, V.; Sergo, V. Low temperature degradation -aging- of zirconia: A critical review of the relevant aspects in dentistry. Dent. Mater. 2010, 26, 807–820. [Google Scholar] [CrossRef] [PubMed]
- Apratim, A.; Eachempati, P.; Krishnappa Salian, K.K.; Singh, V.; Chhabra, S.; Shah, S. Zirconia in dental implantology: A review. J. Int. Soc. Prev. Commun. Dent. 2015, 5, 147–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bornstein, M.M.; Valderrama, P.; Jones, A.A.; Wilson, T.G.; Seibl, R.; Cochran, D.L. Bone apposition around two different sandblasted and acid-etched titanium implant surfaces: A histomorphometric study in canine mandibles. Clin. Oral. Implants Res. 2008, 19, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Roehling, S.; Astasov-Frauenhoffer, M.; Hauser-Gerspach, I.; Braissant, O.; Woelfler, H.; Waltimo, T.; Kniha, H.; Gahlert, M. In Vitro Biofilm Formation on Titanium and Zirconia Implant Surfaces. J. Periodontol. 2017, 88, 298–307. [Google Scholar] [CrossRef]
- Roehling, S.; Schlegel, K.A.; Woelfler, H.; Gahlert, M. Zirconia compared to titanium dental implants in preclinical studies—A systematic review and meta-analysis. Clin. Oral Implants Res. 2019, 30, 365–395. [Google Scholar] [CrossRef]
- Grössner-Schreiber, B.; Teichmann, J.; Hannig, M.; Dörfer, C.; Wenderoth, D.F.; Ott, S.J. Modified implant surfaces show different biofilm compositions under in vivo conditions. Clin. Oral Implants Res. 2009, 20, 817–826. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Piattelli, M.; Caputi, S.; Favero, G.A.; Piattelli, A. Bacterial adhesion on commercially pure titanium and zirconium oxide disks: An in vivo human study. J. Periodontol. 2004, 75, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Barksdale, J. Titanium. In The Encyclopedia of the Chemical Elements; Hampel, C.A., Ed.; Reinhold Book Corporation: New York, NY, USA, 1968; pp. 732–738. [Google Scholar]
- Fage, S.W.; Muris, J.; Jakobsen, S.S.; Thyssen, J.P. Titanium: A review on exposure, release, penetration, allergy, epidemiology, and clinical reactivity. Contact Dermat. 2016, 74, 323–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaur, M.; Singh, K. Review on titanium and titanium based alloys as biomaterials for orthopaedic applications. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 102, 844–862. [Google Scholar] [CrossRef]
- Donachie, M.J. Titanium a Technical Guide; ASM International: Columbus, OH, USA, 1988. [Google Scholar]
- Kotsakis, G.A.; Olmedo, D.G. Peri-implantitis is not periodontitis: Scientific discoveries shed light on microbiome-biomaterial interactions that may determine disease phenotype. Periodontol. 2000 2021, 86, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Koike, M.; Fujii, H. The corrosion resistance of pure titanium in organic acids. Biomaterials 2001, 22, 2931–2936. [Google Scholar] [CrossRef]
- Barão, V.A.; Mathew, M.T.; Assunção, W.G.; Yuan, J.C.; Wimmer, M.A.; Sukotjo, C. The role of lipopolysaccharide on the electrochemical behavior of titanium. J. Dent. Res. 2011, 90, 613–618. [Google Scholar] [CrossRef]
- Barão, V.A.; Mathew, M.T.; Yuan, J.C.; Knoernschild, K.L.; Assunção, W.G.; Wimmer, M.A.; Sukotjo, C. Influence of corrosion on lipopolysaccharide affinity for two different titanium materials. J. Prosthet. Dent. 2013, 110, 462–470. [Google Scholar] [CrossRef]
- Nakagawa, M.; Matsuya, S.; Udoh, K. Effects of fluoride and dissolved oxygen concentrations on the corrosion behavior of pure titanium and titanium alloys. Dent. Mater. J. 2002, 21, 83–92. [Google Scholar] [CrossRef] [Green Version]
- Noguti, J.; de Oliveira, F.; Peres, R.C.; Renno, A.C.; Ribeiro, D.A. The role of fluoride on the process of titanium corrosion in oral cavity. Biometals 2012, 25, 859–862. [Google Scholar] [CrossRef] [PubMed]
- Lindholm-Sethson, B.; Ardlin, B.I. Effects of pH and fluoride concentration on the corrosion of titanium. J. Biomed. Mater. Res. A 2008, 86, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Suárez-López Del Amo, F.; Garaicoa-Pazmiño, C.; Fretwurst, T.; Castilho, R.M.; Squarize, C.H. Dental implants-associated release of titanium particles: A systematic review. Clin. Oral Implants Res. 2018, 29, 1085–1100. [Google Scholar] [CrossRef] [PubMed]
- Stavropoulos, A.; Bertl, K.; Eren, S.; Gotfredsen, K. Mechanical and biological complications after implantoplasty—A systematic review. Clin. Oral Implants Res. 2019, 30, 833–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.X.; Fan, Y.B.; Gao, Y.; Hu, Q.H.; Wang, T.C. TiO2 nanoparticles translocation and potential toxicological effect in rats after intraarticular injection. Biomaterials 2009, 30, 4590–4600. [Google Scholar] [CrossRef] [PubMed]
- Fretwurst, T.; Nelson, K.; Tarnow, D.P.; Wang, H.L.; Giannobile, W.V. Is Metal Particle Release Associated with Peri-implant Bone Destruction? An Emerging Concept. J. Dent. Res. 2018, 97, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Marshall, A.; Ries, M.D.; Paprosky, W. How prevalent are implant wear and osteolysis, and how has the scope of osteolysis changed since 2000? J. Am. Acad. Orthop. Surg. 2008, 16, S1–S6. [Google Scholar] [CrossRef] [PubMed]
- Suárez-López Del Amo, F.; Rudek, I.; Wagner, V.P.; Martins, M.D.; O’Valle, F.; Galindo-Moreno, P.; Giannobile, W.V.; Wang, H.L.; Castilho, R.M. Titanium Activates the DNA Damage Response Pathway in Oral Epithelial Cells: A Pilot Study. Int. J. Oral Maxillofac. Implants 2017, 32, 1413–1420. [Google Scholar] [CrossRef] [Green Version]
- Pettersson, M.; Kelk, P.; Belibasakis, G.N.; Bylund, D.; Molin Thorén, M.; Johansson, A. Titanium ions form particles that activate and execute interleukin-1β release from lipopolysaccharide-primed macrophages. J. Periodont. Res. 2017, 52, 21–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eger, M.; Sterer, N.; Liron, T.; Kohavi, D.; Gabet, Y. Scaling of titanium implants entrains inflammation-induced osteolysis. Sci. Rep. 2017, 7, 39612. [Google Scholar] [CrossRef]
- Okazaki, Y.; Rao, S.; Ito, Y.; Tateishi, T. Corrosion resistance, mechanical properties, corrosion fatigue strength and cytocompatibility of new Ti alloys without Al and V. Biomaterials 1998, 19, 1197–1215. [Google Scholar] [CrossRef]
- Nicholson, J.W. Titanium Alloys for Dental Implants: A Review. Prosthesis 2020, 2, 11. [Google Scholar] [CrossRef]
- Liu, X.; Chen, S.; Tsoi, J.K.H.; Matinlinna, J.P. Binary titanium alloys as dental implant materials—A review. Regen. Biomater. 2017, 4, 315–323. [Google Scholar] [CrossRef] [Green Version]
- Niinomi, M. Mechanical biocompatibilities of titanium alloys for biomedical applications. J. Mech. Behav. Biomed. Mater. 2008, 1, 30–42. [Google Scholar] [CrossRef] [PubMed]
- Klein, G.L. Aluminum toxicity to bone: A multisystem effect? Osteoporos. Sarcopenia 2019, 5, 2–5. [Google Scholar] [CrossRef]
- Thyssen, J.P.; Jakobsen, S.S.; Engkilde, K.; Johansen, J.D.; Søballe, K.; Menné, T. The association between metal allergy, total hip arthroplasty, and revision. Acta Orthop. 2009, 80, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Listgarten, M.A.; Lang, N.P.; Schroeder, H.E.; Schroeder, A. Periodontal tissues and their counterparts around endosseous implants. Clin. Oral Implants Res. 1991, 2, 1–19. [Google Scholar] [CrossRef]
- Bosshardt, D.D.; Chappuis, V.; Buser, D. Osseointegration of titanium, titanium alloy and zirconia dental implants: Current knowledge and open questions. Periodontol. 2000 2017, 73, 22–40. [Google Scholar] [CrossRef] [PubMed]
- Monje, A.; Ravidà, A.; Wang, H.L.; Helms, J.A.; Brunski, J.B. Relationship Between Primary/Mechanical and Secondary/Biological Implant Stability. Int. J. Oral Maxillofac. Implants 2019, 34, s7–s23. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Abrahamsson, I.; Lang, N.P.; Lindhe, J. De novo alveolar bone formation adjacent to endosseous implants. Clin. Oral Implants Res. 2003, 14, 251–262. [Google Scholar] [CrossRef] [Green Version]
- Kazemian, M.; Hoseini, S.H.; Ghorbanzade, S. A brief overview of cellular and molecular mechanisms of osseointegration. Int. J. Contemp. Dent. Med. Rev. 2015. [Google Scholar] [CrossRef]
- Lang, N.P.; Salvi, G.E.; Huynh-Ba, G.; Ivanovski, S.; Donos, N.; Bosshardt, D.D. Early osseointegration to hydrophilic and hydrophobic implant surfaces in humans. Clin. Oral Implants Res. 2011, 22, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.E. Understanding peri-implant endosseous healing. J. Dent. Educ. 2003, 67, 932–949. [Google Scholar] [CrossRef] [PubMed]
- Liñares, A.; Grize, L.; Muñoz, F.; Pippenger, B.E.; Dard, M.; Domken, O.; Blanco-Carrión, J. Histological assessment of hard and soft tissues surrounding a novel ceramic implant: A pilot study in the minipig. J. Clin. Periodontol. 2016, 43, 538–546. [Google Scholar] [CrossRef]
- Buser, D.; Nydegger, T.; Oxland, T.; Cochran, D.L.; Schenk, R.K.; Hirt, H.P.; Snétivy, D.; Nolte, L.P. Interface shear strength of titanium implants with a sandblasted and acid-etched surface: A biomechanical study in the maxilla of miniature pigs. J. Biomed. Mater. Res. 1999, 45, 75–83. [Google Scholar] [CrossRef]
- Buser, D.; Schenk, R.K.; Steinemann, S.; Fiorellini, J.P.; Fox, C.H.; Stich, H. Influence of surface characteristics on bone integration of titanium implants. A histomorphometric study in miniature pigs. J. Biomed. Mater. Res. 1991, 25, 889–902. [Google Scholar] [CrossRef]
- Carmo Filho, L.C.D.; Marcello-Machado, R.M.; Castilhos, E.D.; Del Bel Cury, A.A.; Faot, F. Can implant surfaces affect implant stability during osseointegration? A randomized clinical trial. Braz. Oral Res. 2018, 32, e110. [Google Scholar] [CrossRef] [PubMed]
- López-Valverde, N.; Flores-Fraile, J.; Ramírez, J.M.; Sousa, B.M.; Herrero-Hernández, S.; López-Valverde, A. Bioactive Surfaces vs. Conventional Surfaces in Titanium Dental Implants: A Comparative Systematic Review. J. Clin. Med. 2020, 9, 47. [Google Scholar] [CrossRef]
- Wennerberg, A.; Albrektsson, T.; Chrcanovic, B. Long-term clinical outcome of implants with different surface modifications. Eur. J. Oral Implantol. 2018, 11, S123–S136. [Google Scholar]
- Xue, T.; Attarilar, S.; Liu, S.; Liu, J.; Song, X.; Li, L.; Zhao, B.; Tang, Y. Surface Modification Techniques of Titanium and its Alloys to Functionally Optimize Their Biomedical Properties: Thematic Review. Front. Bioeng. Biotechnol. 2020, 8, 603072. [Google Scholar] [CrossRef]
- Kligman, S.; Ren, Z.; Chung, C.H.; Perillo, M.A.; Chang, Y.C.; Koo, H.; Zheng, Z.; Li, C. The Impact of Dental Implant Surface Modifications on Osseointegration and Biofilm Formation. J. Clin. Med. 2021, 10, 1641. [Google Scholar] [CrossRef] [PubMed]
- Xiropaidis, A.V.; Qahash, M.; Lim, W.H.; Shanaman, R.H.; Rohrer, M.D.; Wikesjö, U.M.; Hall, J. Bone-implant contact at calcium phosphate-coated and porous titanium oxide (TiUnite)-modified oral implants. Clin. Oral Implants Res. 2005, 16, 532–539. [Google Scholar] [CrossRef]
- Roccuzzo, M.; Aglietta, M.; Bunino, M.; Bonino, L. Early loading of sandblasted and acid-etched implants: A randomized-controlled double-blind split-mouth study. Five-year results. Clin. Oral Implants Res. 2008, 19, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Browaeys, H.; Defrancq, J.; Dierens, M.C.; Miremadi, R.; Vandeweghe, S.; Van de Velde, T.; De Bruyn, H. A retrospective analysis of early and immediately loaded osseotite implants in cross-arch rehabilitations in edentulous maxillas and mandibles up to 7 years. Clin. Implant Dent. Relat. Res. 2013, 15, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Hao, C.P.; Cao, N.J.; Zhu, Y.H.; Wang, W. The osseointegration and stability of dental implants with different surface treatments in animal models: A network meta-analysis. Sci. Rep. 2021, 11, 13849. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Ardebili, Y.; Worthington, H.V. Interventions for replacing missing teeth: Different types of dental implants. Cochrane Database Syst. Rev. 2014, Cd003815. [Google Scholar] [CrossRef]
- Goldman, M.; Juodzbalys, G.; Vilkinis, V. Titanium surfaces with nanostructures influence on osteoblasts proliferation: A systematic review. J. Oral Maxillofac. Res. 2014, 5, e1. [Google Scholar] [CrossRef]
- Martins, R.; Cestari, T.M.; Arantes, R.V.N.; Santos, P.S.; Taga, R.; Carbonari, M.J.; Oliveira, R.C. Osseointegration of zirconia and titanium implants in a rabbit tibiae model evaluated by microtomography, histomorphometry and fluorochrome labeling analyses. J. Periodont. Res. 2018, 53, 210–221. [Google Scholar] [CrossRef]
- Hoffmann, O.; Angelov, N.; Zafiropoulos, G.G.; Andreana, S. Osseointegration of zirconia implants with different surface characteristics: An evaluation in rabbits. Int. J. Oral Maxillofac. Implants 2012, 27, 352–358. [Google Scholar] [PubMed]
- Lee, J.; Sieweke, J.H.; Rodriguez, N.A.; Schüpbach, P.; Lindström, H.; Susin, C.; Wikesjö, U.M. Evaluation of nano-technology-modified zirconia oral implants: A study in rabbits. J. Clin. Periodontol. 2009, 36, 610–617. [Google Scholar] [CrossRef]
- Wenz, H.J.; Bartsch, J.; Wolfart, S.; Kern, M. Osseointegration and clinical success of zirconia dental implants: A systematic review. Int. J. Prosthodont. 2008, 21, 27–36. [Google Scholar]
- Pieralli, S.; Kohal, R.J.; Jung, R.E.; Vach, K.; Spies, B.C. Clinical Outcomes of Zirconia Dental Implants: A Systematic Review. J. Dent. Res. 2017, 96, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Pieralli, S.; Kohal, R.J.; Lopez Hernandez, E.; Doerken, S.; Spies, B.C. Osseointegration of zirconia dental implants in animal investigations: A systematic review and meta-analysis. Dent. Mater. 2018, 34, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Borges, H.; Correia, A.R.M.; Castilho, R.M.; de Oliveira Fernandes, G.V. Zirconia Implants and Marginal Bone Loss: A Systematic Review and Meta-Analysis of Clinical Studies. Int. J. Oral Maxillofac. Implants 2020, 35, 707–720. [Google Scholar] [CrossRef] [PubMed]
- Kohal, R.J.; Schwindling, F.S.; Bächle, M.; Spies, B.C. Peri-implant bone response to retrieved human zirconia oral implants after a 4-year loading period: A histologic and histomorphometric evaluation of 22 cases. J. Biomed. Mater. Res. B Appl. Biomater. 2016, 104, 1622–1631. [Google Scholar] [CrossRef]
- Jepsen, S.; Caton, J.G.; Albandar, J.M.; Bissada, N.F.; Bouchard, P.; Cortellini, P.; Demirel, K.; de Sanctis, M.; Ercoli, C.; Fan, J.; et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S237–S248. [Google Scholar] [CrossRef]
- Kennedy, J.E.; Bird, W.C.; Palcanis, K.G.; Dorfman, H.S. A longitudinal evaluation of varying widths of attached gingiva. J. Clin. Periodontol. 1985, 12, 667–675. [Google Scholar] [CrossRef]
- Miyasato, M.; Crigger, M.; Egelberg, J. Gingival condition in areas of minimal and appreciable width of keratinized gingiva. J. Clin. Periodontol. 1977, 4, 200–209. [Google Scholar] [CrossRef]
- Avila-Ortiz, G.; Gonzalez-Martin, O.; Couso-Queiruga, E.; Wang, H.L. The peri-implant phenotype. J. Periodontol. 2020, 91, 283–288. [Google Scholar] [CrossRef]
- Lindhe, J.; Berglundh, T. The interface between the mucosa and the implant. Periodontol. 2000 1998, 17, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Carcuac, O.; Abrahamsson, I.; Albouy, J.P.; Linder, E.; Larsson, L.; Berglundh, T. Experimental periodontitis and peri-implantitis in dogs. Clin. Oral Implants Res. 2013, 24, 363–371. [Google Scholar] [CrossRef]
- Carcuac, O.; Berglundh, T. Composition of human peri-implantitis and periodontitis lesions. J. Dent. Res. 2014, 93, 1083–1088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gharpure, A.S.; Latimer, J.M.; Aljofi, F.E.; Kahng, J.H.; Daubert, D.M. Role of thin gingival phenotype and inadequate keratinized mucosa width (<2 mm) as risk indicators for peri-implantitis and peri-implant mucositis. J. Periodontol. 2021. [Google Scholar] [CrossRef]
- Yamano, S.; Ma, A.K.; Shanti, R.M.; Kim, S.W.; Wada, K.; Sukotjo, C. The influence of different implant materials on human gingival fibroblast morphology, proliferation, and gene expression. Int. J. Oral Maxillofac. Implants 2011, 26, 1247–1255. [Google Scholar] [PubMed]
- Atsuta, I.; Ayukawa, Y.; Kondo, R.; Oshiro, W.; Matsuura, Y.; Furuhashi, A.; Tsukiyama, Y.; Koyano, K. Soft tissue sealing around dental implants based on histological interpretation. J. Prosthodont. Res. 2016, 60, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zheng, M.; Liao, Y.; Zhou, J.; Li, H.; Tan, J. Different behavior of human gingival fibroblasts on surface modified zirconia: A comparison between ultraviolet (UV) light and plasma. Dent. Mater. J. 2019, 38, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Tetè, S.; Mastrangelo, F.; Bianchi, A.; Zizzari, V.; Scarano, A. Collagen fiber orientation around machined titanium and zirconia dental implant necks: An animal study. Int. J. Oral Maxillofac. Implants 2009, 24, 52–58. [Google Scholar] [PubMed]
- Sadid-Zadeh, R.; Willis, J.; Forgo, G.; Haraszthy, V. Comparative Analysis of Biofilm Formation on Materials Used for the Fabrication of Implant-Supported Prostheses. Braz. Dent. J. 2020, 31, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Kniha, K.; Heussen, N.; Modabber, A.; Hölzle, F.; Möhlhenrich, S.C. The effect of zirconia and titanium surfaces on biofilm formation and on host-derived immunological parameters. Int. J. Oral Maxillofac. Surg. 2021. [Google Scholar] [CrossRef]
- Fretwurst, T.; Müller, J.; Larsson, L.; Bronsert, P.; Hazard, D.; Castilho, R.M.; Kohal, R.; Nelson, K.; Iglhaut, G. Immunohistological composition of peri-implantitis affected tissue around ceramic implants—A pilot study. J. Periodontol. 2021, 92, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Wilson, T.G., Jr. Bone loss around implants—Is it metallosis? J. Periodontol. 2021, 92, 181–185. [Google Scholar] [CrossRef]
- Afrashtehfar, K.I.; Del Fabbro, M. Clinical performance of zirconia implants: A meta-review. J. Prosthet. Dent. 2020, 123, 419–426. [Google Scholar] [CrossRef]
- Lorenz, J.; Giulini, N.; Hölscher, W.; Schwiertz, A.; Schwarz, F.; Sader, R. Prospective controlled clinical study investigating long-term clinical parameters, patient satisfaction, and microbial contamination of zirconia implants. Clin. Implant. Dent. Relat. Res. 2019, 21, 263–271. [Google Scholar] [CrossRef]
- Comisso, I.; Arias-Herrera, S.; Gupta, S. Zirconium dioxide implants as an alternative to titanium: A systematic review. J. Clin. Exp. Dent. 2021, 13, e511–e519. [Google Scholar] [CrossRef]
- Buser, D.; Janner, S.F.; Wittneben, J.G.; Brägger, U.; Ramseier, C.A.; Salvi, G.E. 10-year survival and success rates of 511 titanium implants with a sandblasted and acid-etched surface: A retrospective study in 303 partially edentulous patients. Clin. Implant Dent. Relat. Res. 2012, 14, 839–851. [Google Scholar] [CrossRef]
- Andreiotelli, M.; Wenz, H.J.; Kohal, R.J. Are ceramic implants a viable alternative to titanium implants? A systematic literature review. Clin. Oral Implants Res. 2009, 20, 32–47. [Google Scholar] [CrossRef] [PubMed]
- Manzano, G.; Herrero, L.R.; Montero, J. Comparison of clinical performance of zirconia implants and titanium implants in animal models: A systematic review. Int. J. Oral Maxillofac. Implants 2014, 29, 311–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hafezeqoran, A.; Koodaryan, R. Effect of Zirconia Dental Implant Surfaces on Bone Integration: A Systematic Review and Meta-Analysis. Biomed Res. Int. 2017, 2017, 9246721. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, A.; Khan, A.S.; Zafar, S. Thirty Years of Translational Research in Zirconia Dental Implants: A Systematic Review of the Literature. J. Oral Implantol. 2017, 43, 314–325. [Google Scholar] [CrossRef] [PubMed]
- ArRejaie, A.S.; Al-Hamdan, R.S.; Basunbul, G.I.; Abduljabbar, T.; Al-Aali, K.A.; Labban, N. Clinical performance of one-piece zirconia dental implants: A systematic review. J. Investig. Clin. Dent. 2019, 10, e12384. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Reference | Aim | Main Results | Conclusions |
|---|---|---|---|
| Wenz et al., 2008 [73] | SR with seven animals’ studies to report the clinical success of zirconia implants and osseointegration compared with titanium. | The mean bone–implant contact percentage was above 60%. In studies comparing zirconia vs. titanium, the first was comparable to or even better than the second. Surface modifications may further improve initial bone healing and resistance to removal torque. | Zirconia implants may become an alternative to titanium implants, but cannot currently be recommended for routine clinical use, as no long-term clinical data are available. |
| Hashim et al., 2016 [10] | SR with 14 clinical studies and at least 1 year follow up to analyze osseointegration of zirconia implants. | The overall survival rate of zirconia was 92% after one year of function. Early failure of zirconia implants oscillated between 1.8 and 100 %, with 77% of overall early failure rate. | Zirconia ceramics could potentially be the alternative to titanium for a non-metallic implant solution. |
| Pieralli et al., 2017 [74] | SR of two RCTs and seven prospective clinical trials with zirconia implants restored with single crowns and fixed dental prostheses. | The survival rate after 12 months ranged between 85% and 100 with a mean of 95.6%. The mean marginal bone loss after 12 months follow up was 0.79 mm. | The survival rate and marginal bone loss of zirconia dental implants after one year are comparable to available data of two-piece titanium implants. |
| Pieralli et al., 2018 [75] | SR with 54 studies analyzing osseointegration of zirconia implants in animal studies. | Titanium implants showed a bone to implant (BIC) contact of 60.70% after the mean follow-up time. In comparison, zirconia implants showed a reduced BIC of −3.47%. Titanium implants showed a removal torque analysis of 102.71 Ncm after the mean follow-up time. No significant difference was found for zirconia implants (−7.31 Ncm, p = 0.44). In general, smooth implant surfaces (−43.85 Ncm, p = 0.03) and implant loading (+40.78 Ncm, p < 0.01) significantly influenced the removal torque. A roughness of Ra >2 m and Sa > 2 m resulted in a positive effect. | No significant difference of zirconia or titanium on the results analyzed could be found. Moreover, the results might depend on the animal model studied. |
| Borges et al., 2020 [76] | SR with 19 articles regarding survival rate and marginal bone loss (MBL), with a minimum follow-up of 12 months. | The marginal bone remodeling of 0.8 mm and 1.01 mm at 1 year and 2 years post-loading, respectively. Overall failure rate of 6.8% in 2.75 years. Early failure was 3.4%, late failure was 1.7%, and implant fracture was 1.7. | Zirconia presents results similar to titanium. However, the studies demonstrate a short follow-up period. |
| Reference | Aim | Main Results | Conclusions |
|---|---|---|---|
| Andreioitelli et al., 2009 [98] | SR with 25 studies describing clinical animal studies. | Animal studies show similar results between titanium and zirconia implants. Clinical outcomes presented a survival rate from 84% after 21 months to 98% after 1 year for zirconia implants. | No difference was found in the rate of osseointegration between the different implant materials in animal experiments. Regarding the clinical studies, the authors concluded that only cohort investigations with questionable scientific value were found at that time. |
| Manzano et al., 2014 [99] | SR with 16 animal studies comparing the removal torque and bone–implant contact. | Titanium: in rabbits, BIC = 32%, after 3 weeks and 80% in 4 weeks; in minipigs, 24% after 4 weeks and 83% after 12 weeks. Removal torque—in rabbits, 42 Ncm in the tibia after 6 weeks 36 to 74 Ncm in the femur after 6 weeks; in minipigs, 245 Ncm after 4 weeks and 105 Ncm after 12 weeks. Zirconia—in rabbits, 72% after 4 weeks; in minipigs, 71% after 12 weeks. Removal torque—in rabbits, 12 Ncm in the tibia after 6 weeks to 98 Ncm in the femur after 6 weeks; in minipigs, 112 Ncm after 4 weeks and 26 Ncm after 12 weeks. | BIC and removal torque did not show a significant statistical difference between titanium and zirconia implants. |
| Hafezeqoran and Koodaryan 2017 [100] | SR and meta-analysis of 15 preclinical studies analyzing bone to implant contact and removal torque. | The range of BIC was 31.80% to 87.85% for titanium, 33.74% to 84.17% for machined zirconia, 41.35% to 67.4% for blasted zirconia, and 51.1% to 71.4% for surface etched zirconia in the studies. No significant statistical difference in the BIC values between titanium machined zirconia or blasted zirconia implants was found. However, acid-etched zirconia significantly increased BIC compared with titanium implants (𝑝 = 0.032). More favorable removal torque values for untreated zirconia implants than those of machined zirconia implants, which were statistically significant (𝑝 < 0.001). | Acid-etched zirconia implants may present a successful osseointegration. |
| Siddiqi et al., 2017 [101] | SR of 29 animal studies. | Zirconia has shown a similar %BIC to that of Ti implants in most of the studies. Cracks and material fracture have been attributed as the major technical complications related to Zr implants possibly leading to early implant failure. | The use of zirconia implants to restore edentulous area should be carefully evaluated. |
| Sivaraman et al., 2018 [16] | Critical review | The early fracture of a one-piece zirconia implant, especially in the posterior region, is a sensitive and critical factor to be considered regarding its use and acceptance in all clinical situations. As most clinical studies on zirconia implants are short-term, substantial evidence supported by long-term clinical trials is warranted before zirconia-based implant systems can completely replace titanium for prosthetic rehabilitation. | Zirconia implants are a favorable alternative to titanium with greater soft tissue response, biocompatibility, and aesthetics with comparable osseointegration. |
| Roehling et al., 2019 [21] | SR and meta-analysis of 37 preclinical studies comparing titanium and zirconia implants regarding soft and hard tissue. | Outcome measurements: Titanium—BIC = 59.1% Removal torque = 102.6 Ncm Push in = 25.1 N Zirconia—BIC = 55.9% Removal torque = 71.5 Ncm Push in = 22.0 N Similar qualitative soft tissue integration was reported for zirconia and titanium implants. However, faster maturation processes of epithelial and connective tissues around zirconia implants were assumed. Quantitatively, similar bone width dimensions were evaluated for titanium (3.5 mm) and zirconia (3.2 mm), whereas the loading protocol significantly influenced the outcomes. | Zirconia and titanium implants demonstrate a similar soft and hard tissue integration capacity. However, titanium tended to show a faster initial osseointegration process compared with zirconia. Nevertheless, animal species and study protocols can significantly influence the outcomes. |
| ArRejaie et al., 2019 [102] | SR of six studies comparing one-piece titanium vs. one-piece zirconia implants. | Zirconia implants showed higher crestal bone loss compared with titanium. Variable results regarding failure rate were found. | High heterogeneity of results. |
| Comisso et al., 2021 [96] | SR with 15 articles evaluating aesthetic, clinical benefits, and survival rates. | Zirconia implants showed better esthetic outcomes, less plaque accumulation, and less inflammation around the peri-implant mucosa than titanium. Moreover, zirconia presented a lower probing depth and an ideal papilla crown proportion with an increased papillary height. For survival and success rates, no difference was found between the materials. | It seems like zirconia implants present better clinical performance than titanium ones. However, more studies are needed to confirm these data. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Webber, L.P.; Chan, H.-L.; Wang, H.-L. Will Zirconia Implants Replace Titanium Implants? Appl. Sci. 2021, 11, 6776. https://doi.org/10.3390/app11156776
Webber LP, Chan H-L, Wang H-L. Will Zirconia Implants Replace Titanium Implants? Applied Sciences. 2021; 11(15):6776. https://doi.org/10.3390/app11156776
Chicago/Turabian StyleWebber, Liana Preto, Hsun-Liang Chan, and Hom-Lay Wang. 2021. "Will Zirconia Implants Replace Titanium Implants?" Applied Sciences 11, no. 15: 6776. https://doi.org/10.3390/app11156776
APA StyleWebber, L. P., Chan, H.-L., & Wang, H.-L. (2021). Will Zirconia Implants Replace Titanium Implants? Applied Sciences, 11(15), 6776. https://doi.org/10.3390/app11156776