
Transfer Accuracy of Two 3D Printed Trays for Indirect Bracket Bonding—An In Vitro Pilot Study

 ,
, 


Abstract
:1. Introduction
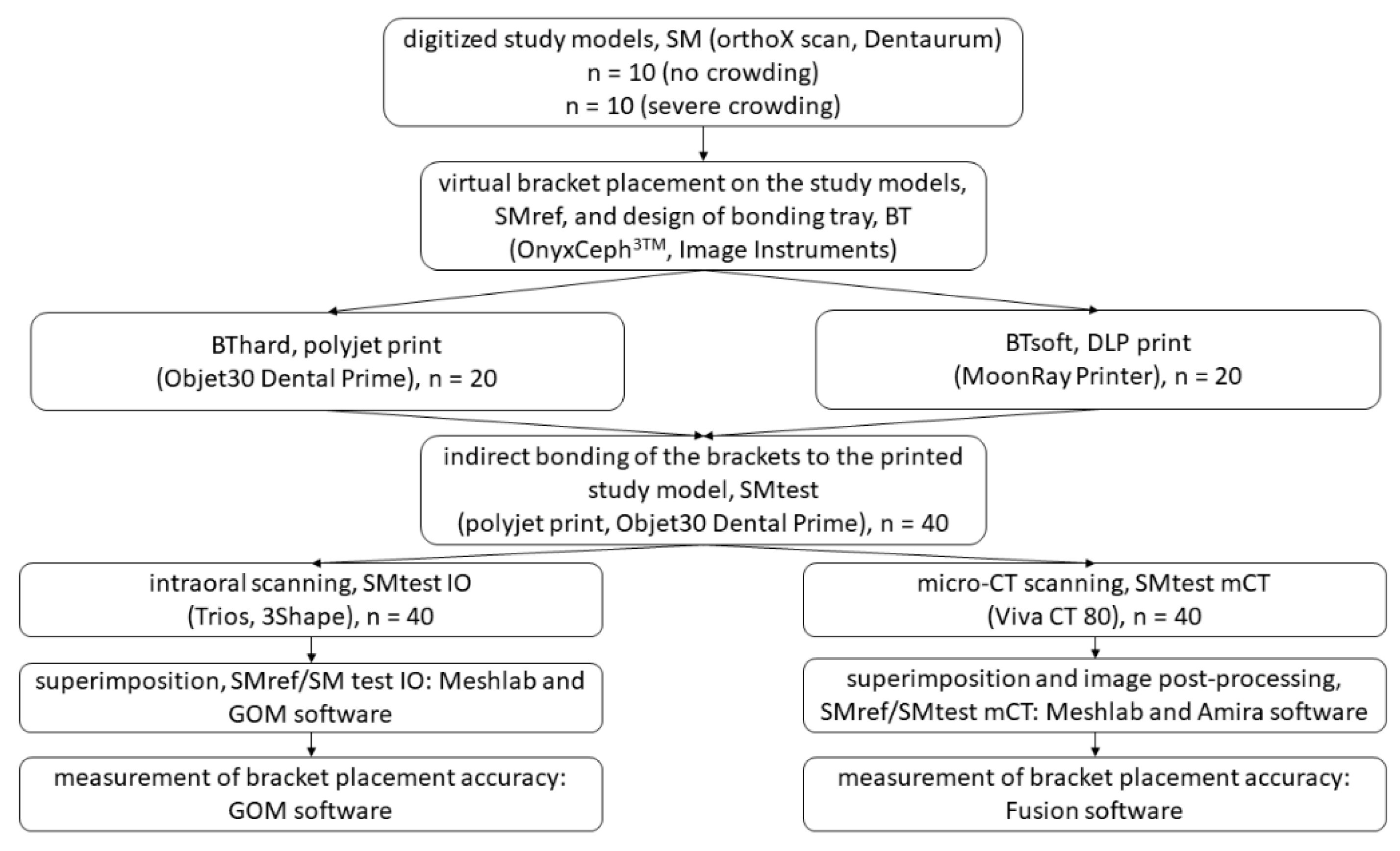
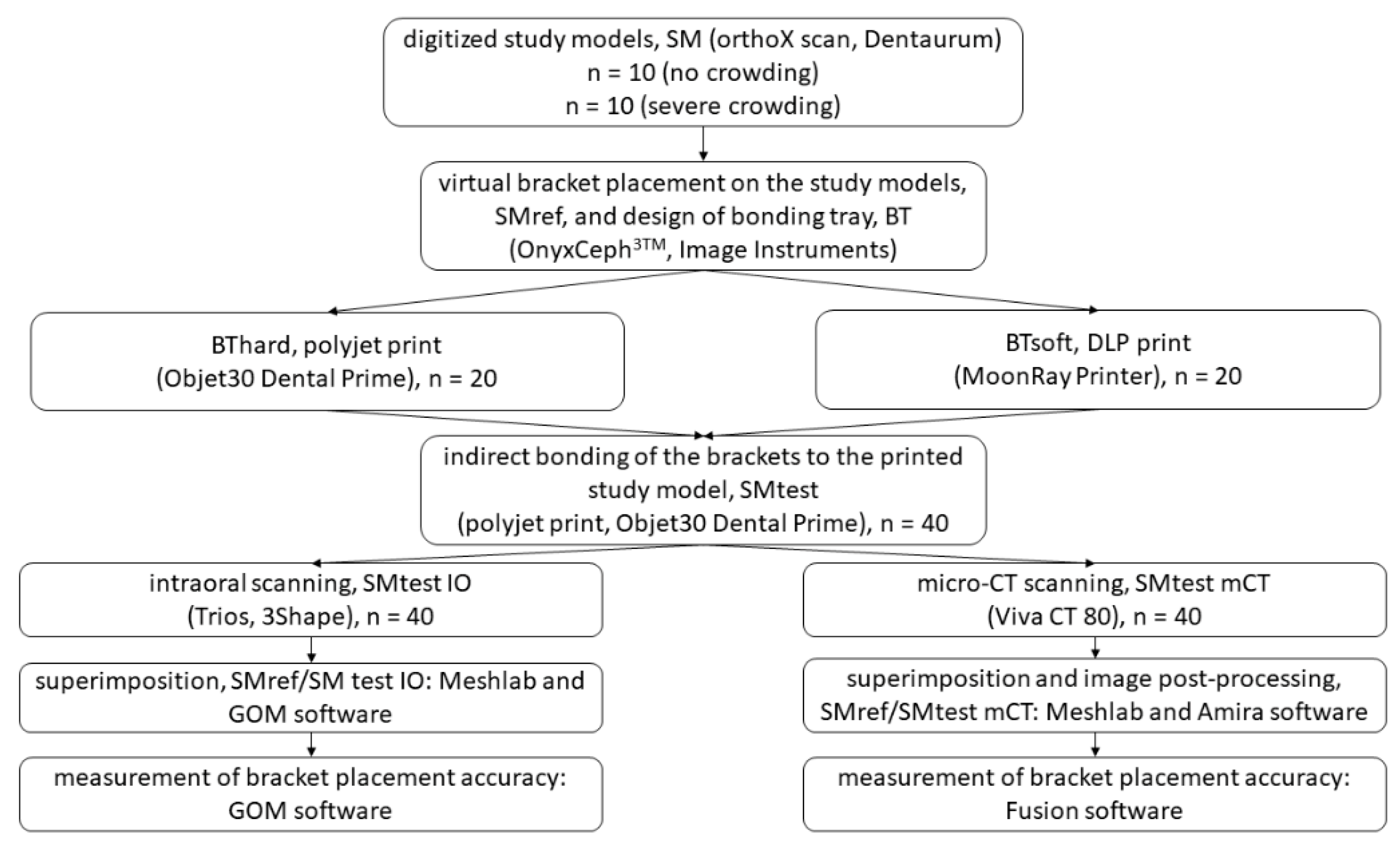
2. Materials and Methods
2.1. Selection of Casts
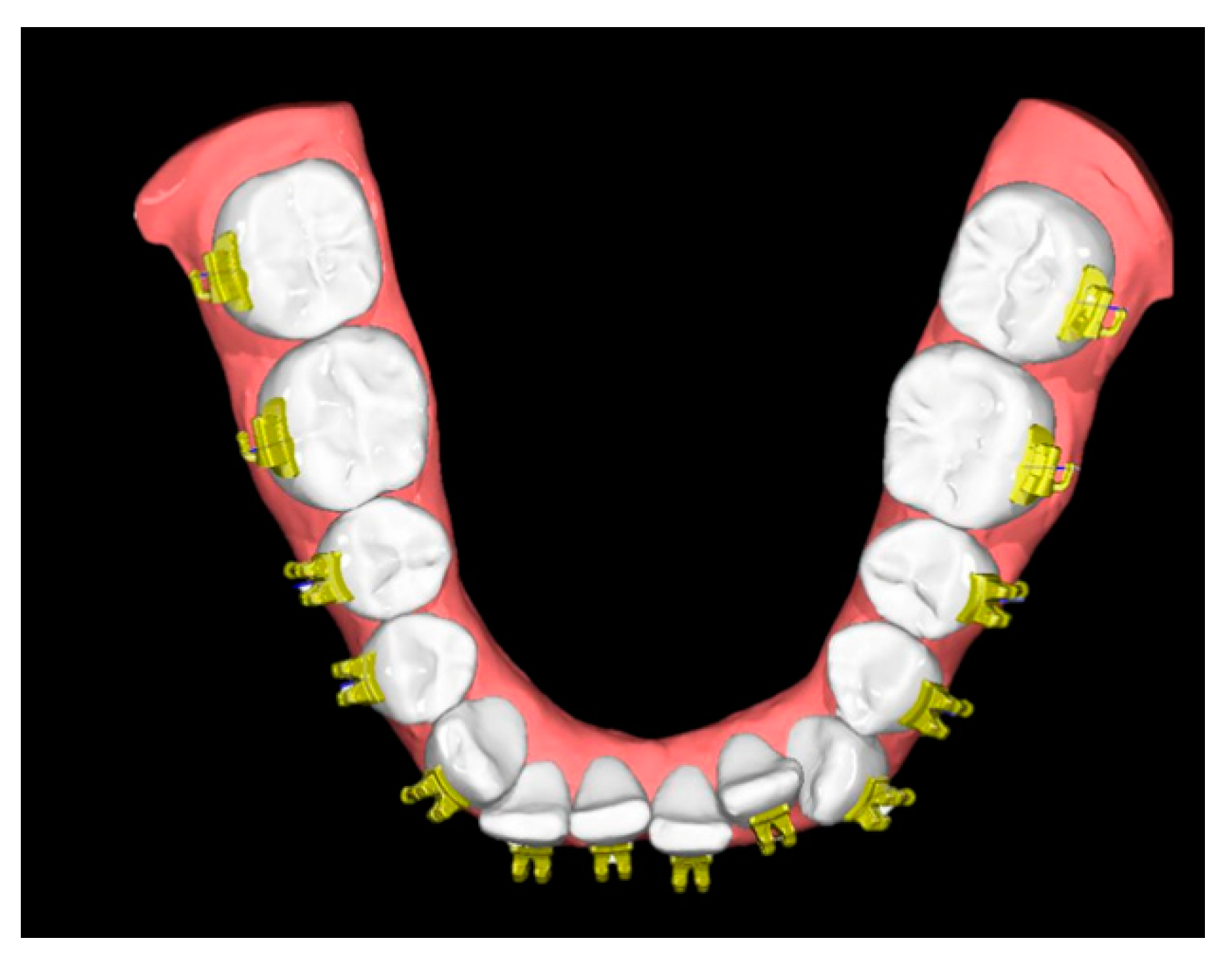
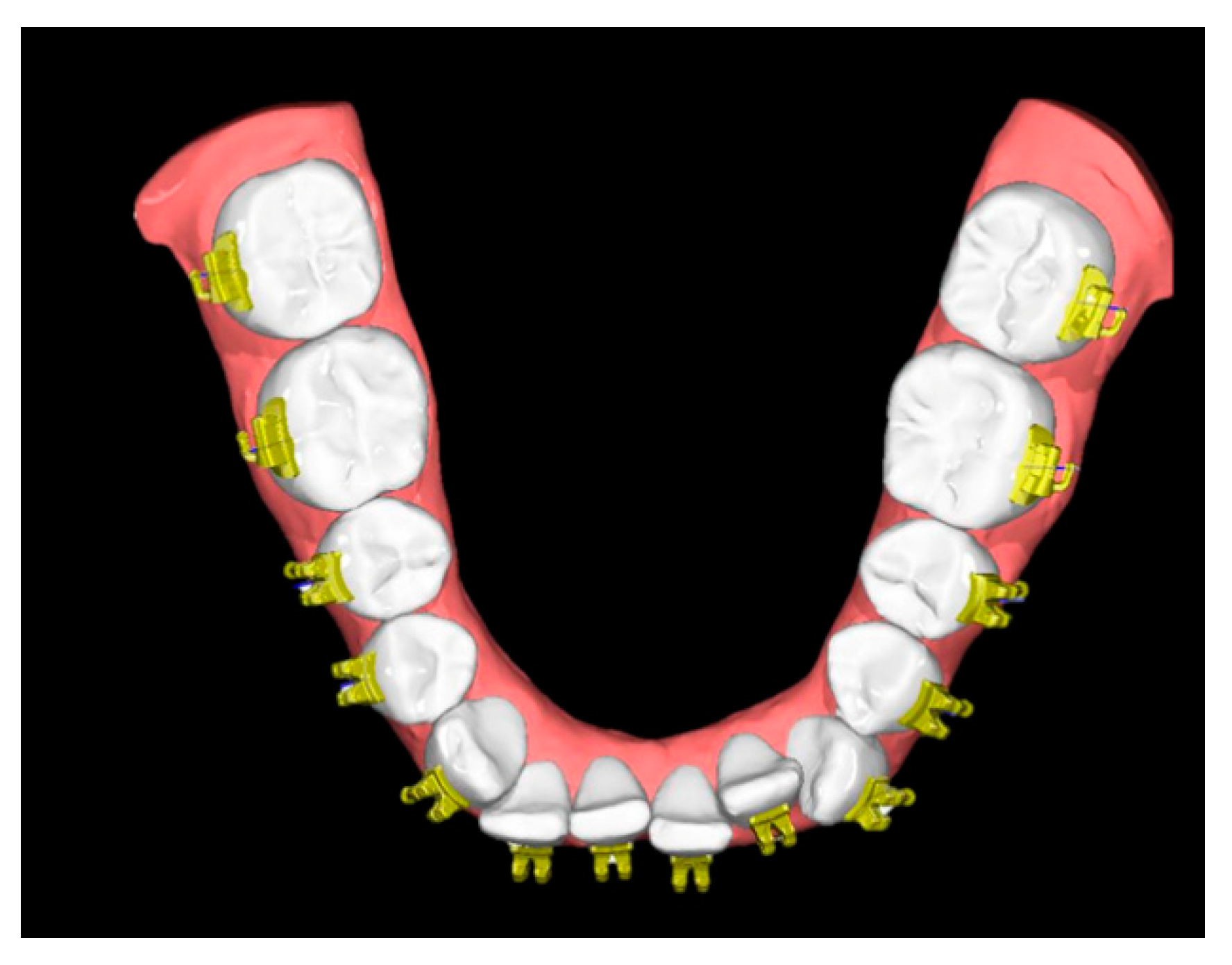
2.2. Model Preparation and Bracket Placement
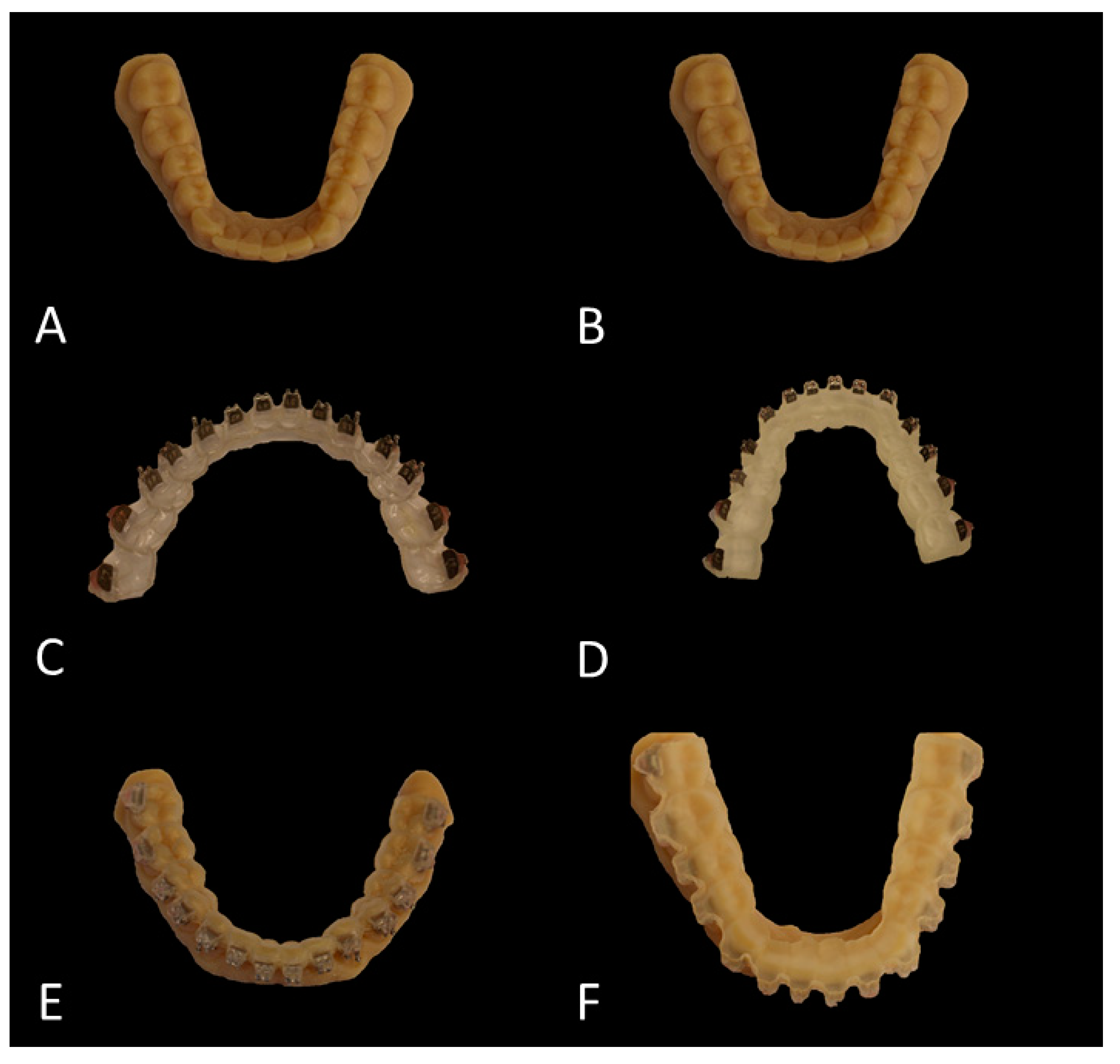
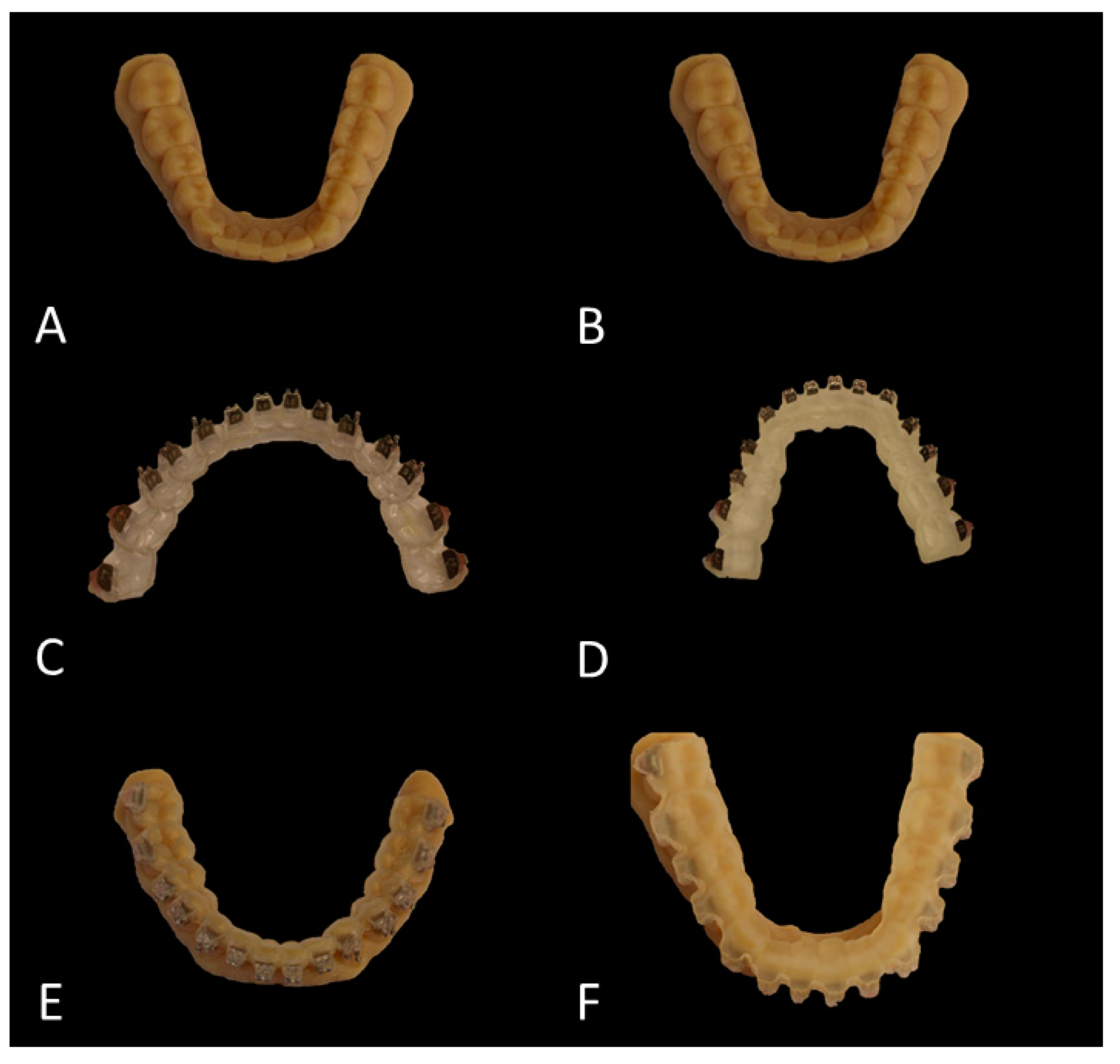
2.3. Planning and Printing of the Transfer Trays
2.4. Bracket Transfer and Bonding
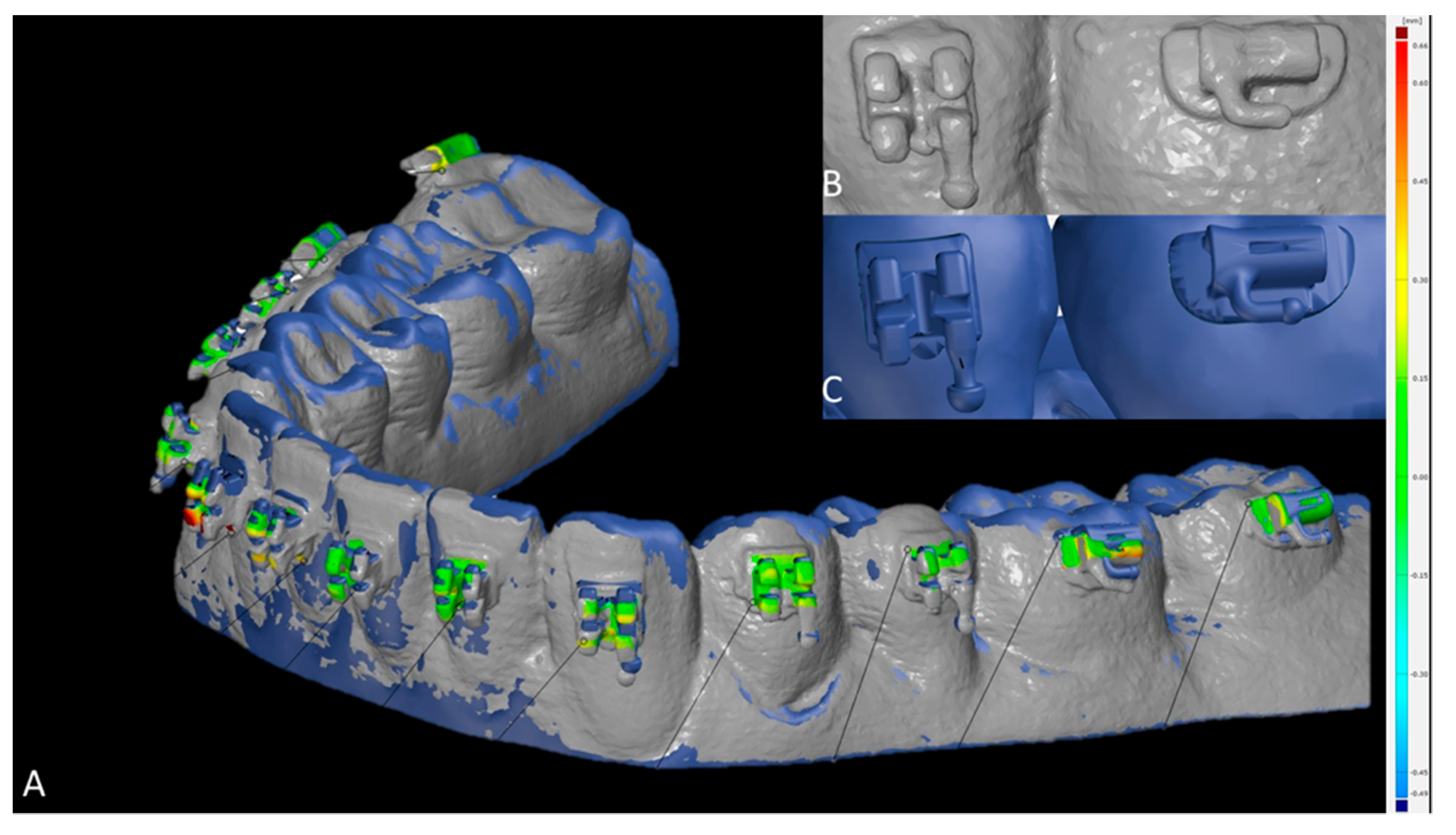
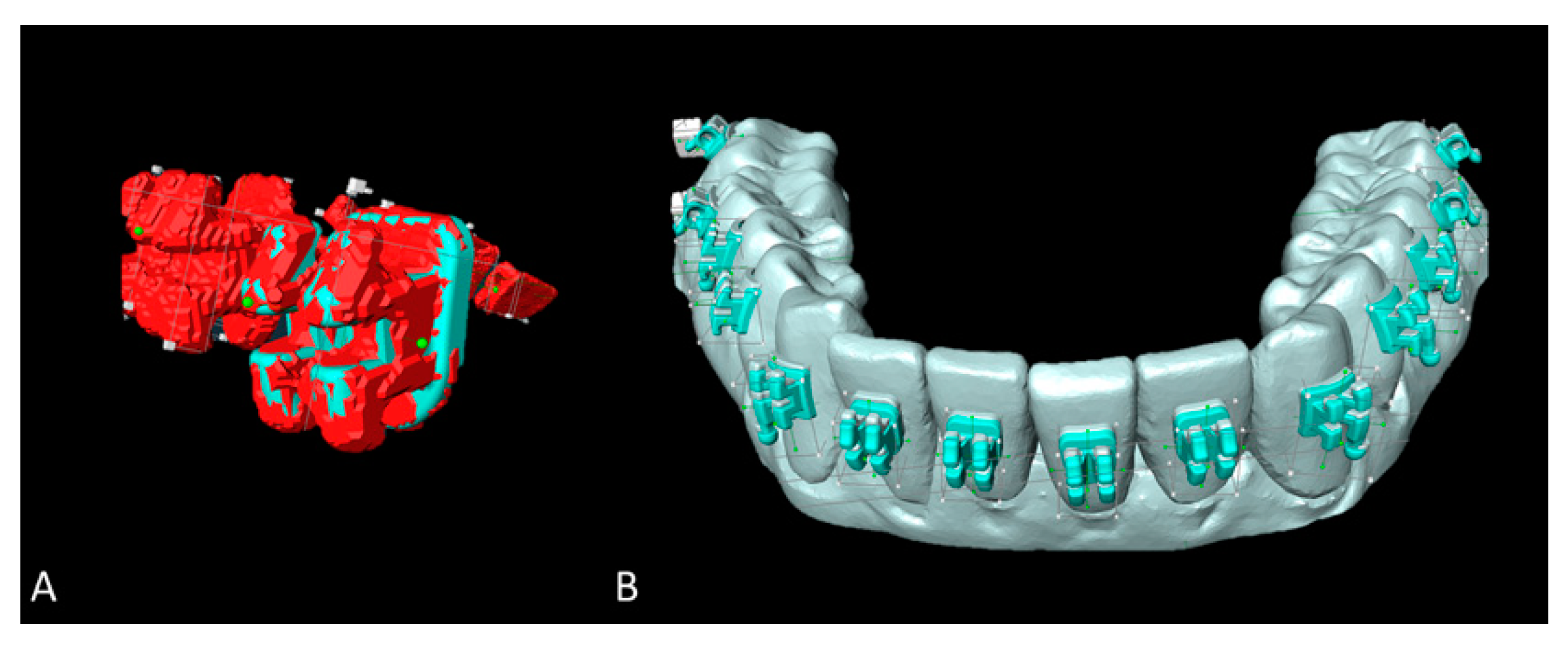
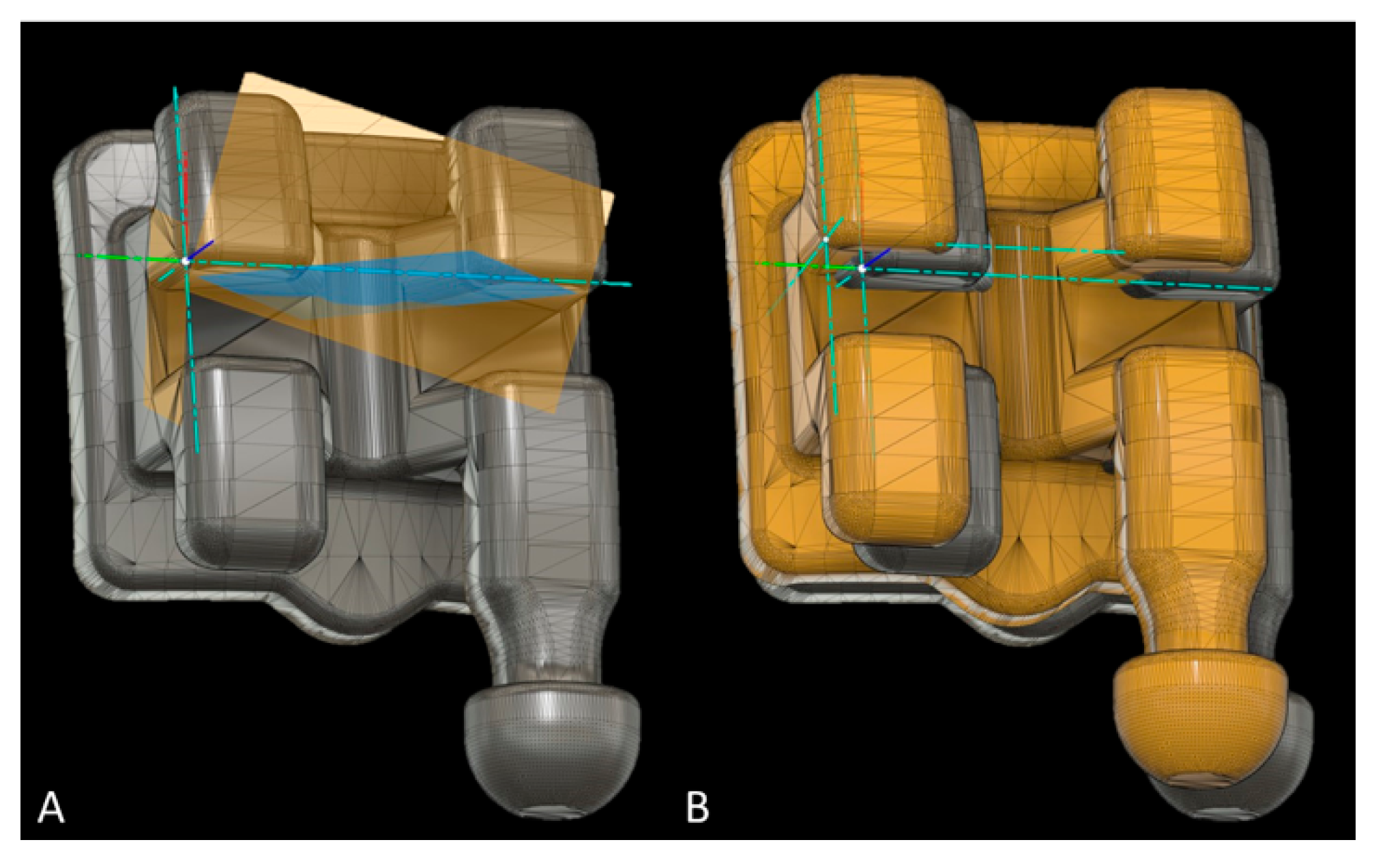
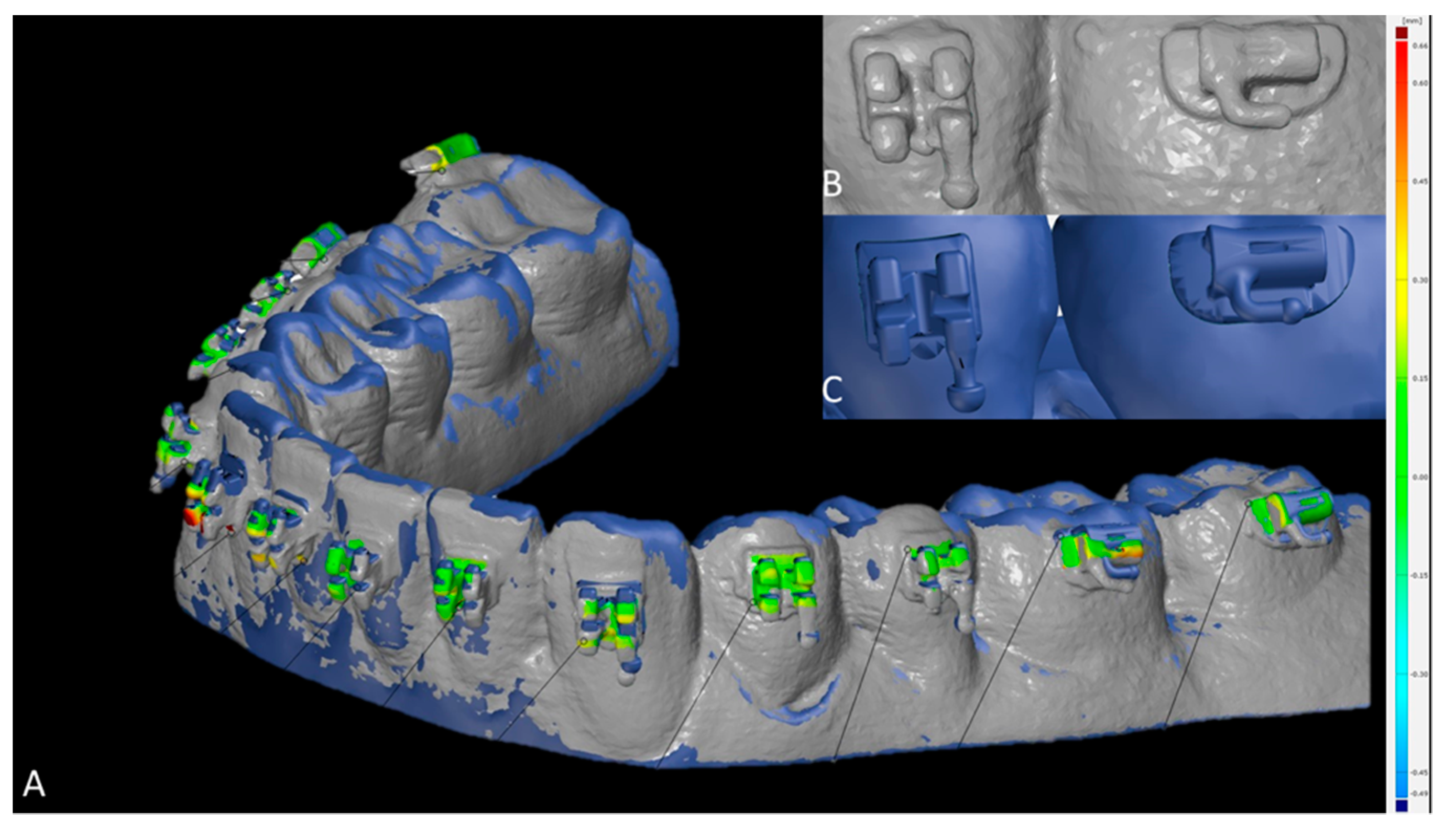
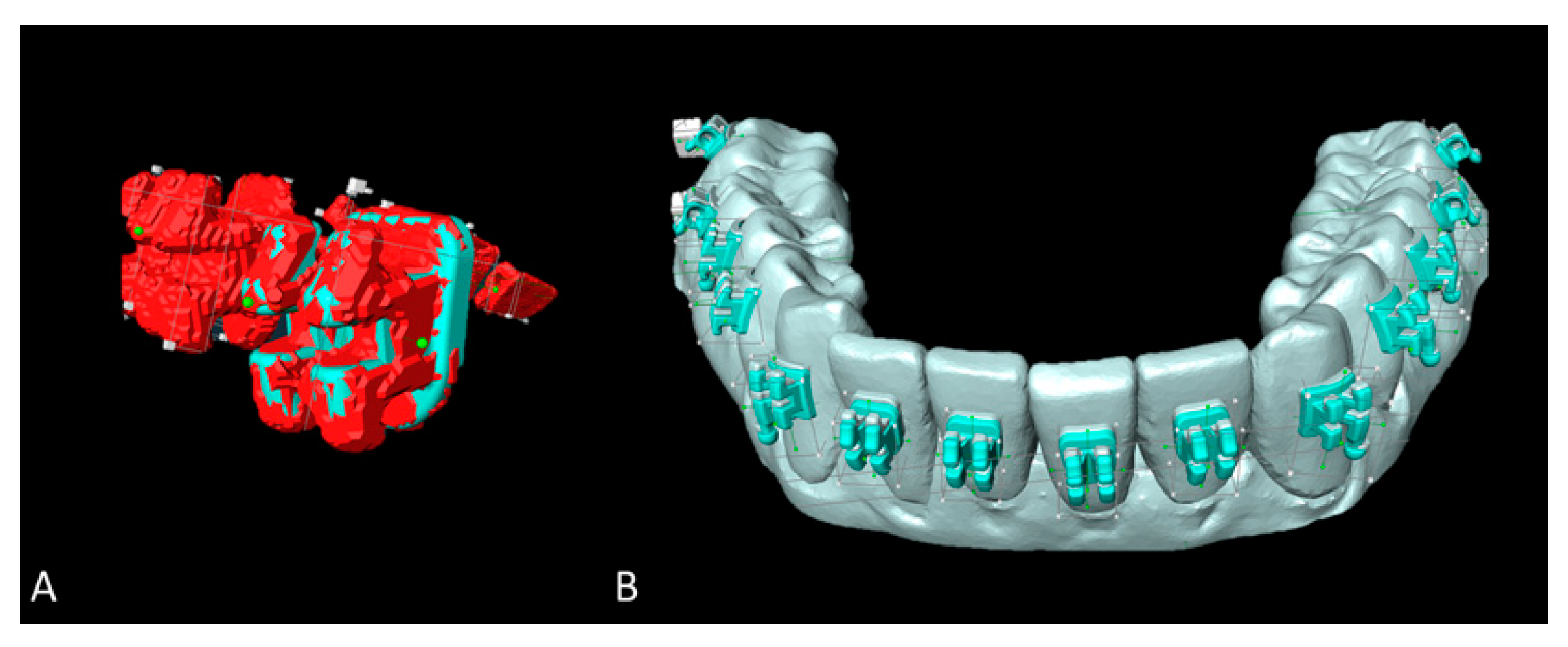
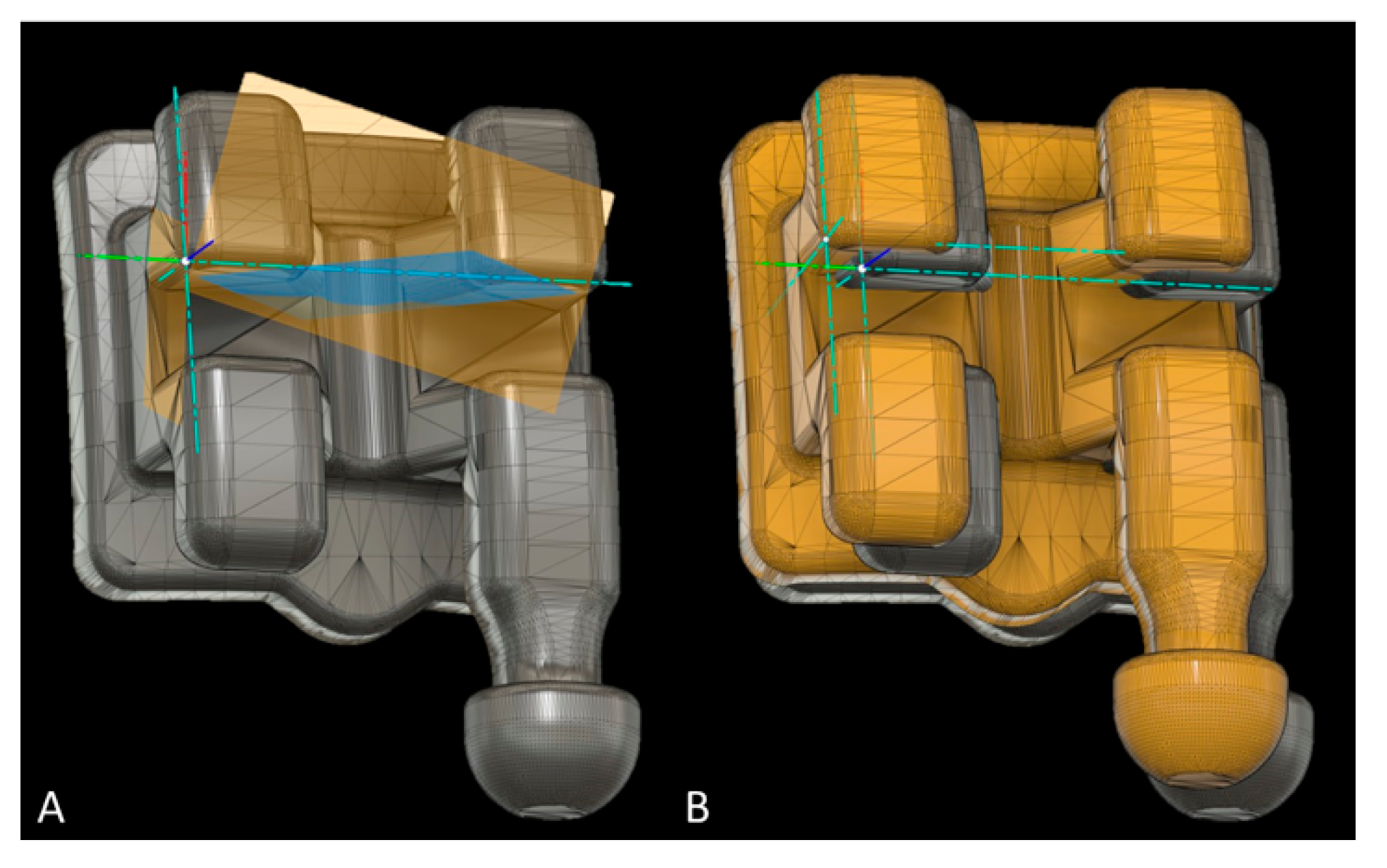
2.5. Digitization, Image Processing and Measurement of Bracket Placement Accuracy
2.5.1. Intraoral Scanning
2.5.2. Micro-CT Scanning (Method Validation)
2.6. Sample Size Calculation
2.7. Reliability of Measurements
2.8. Statistical Analysis
3. Results
3.1. Reliability of Measurements
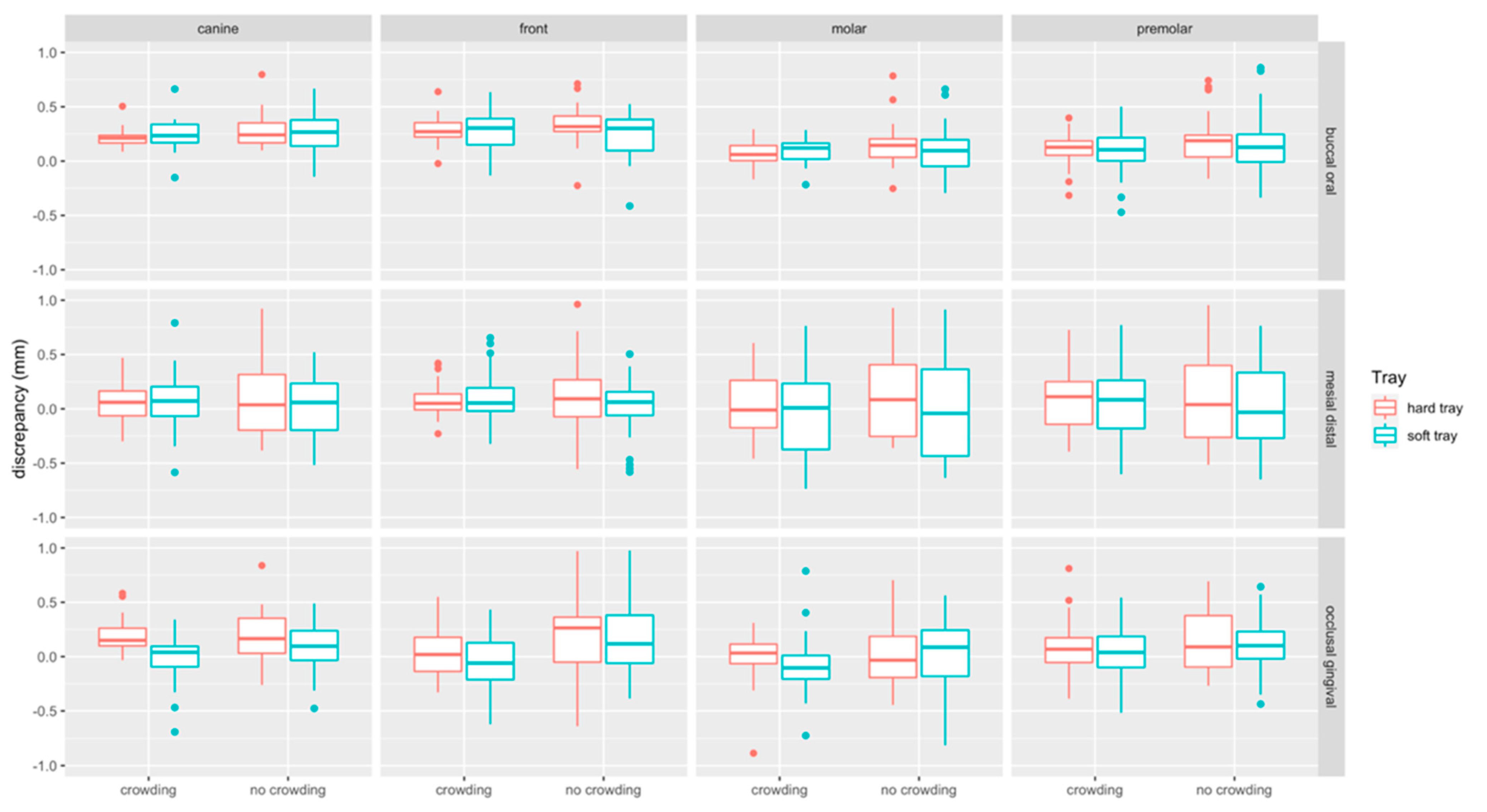
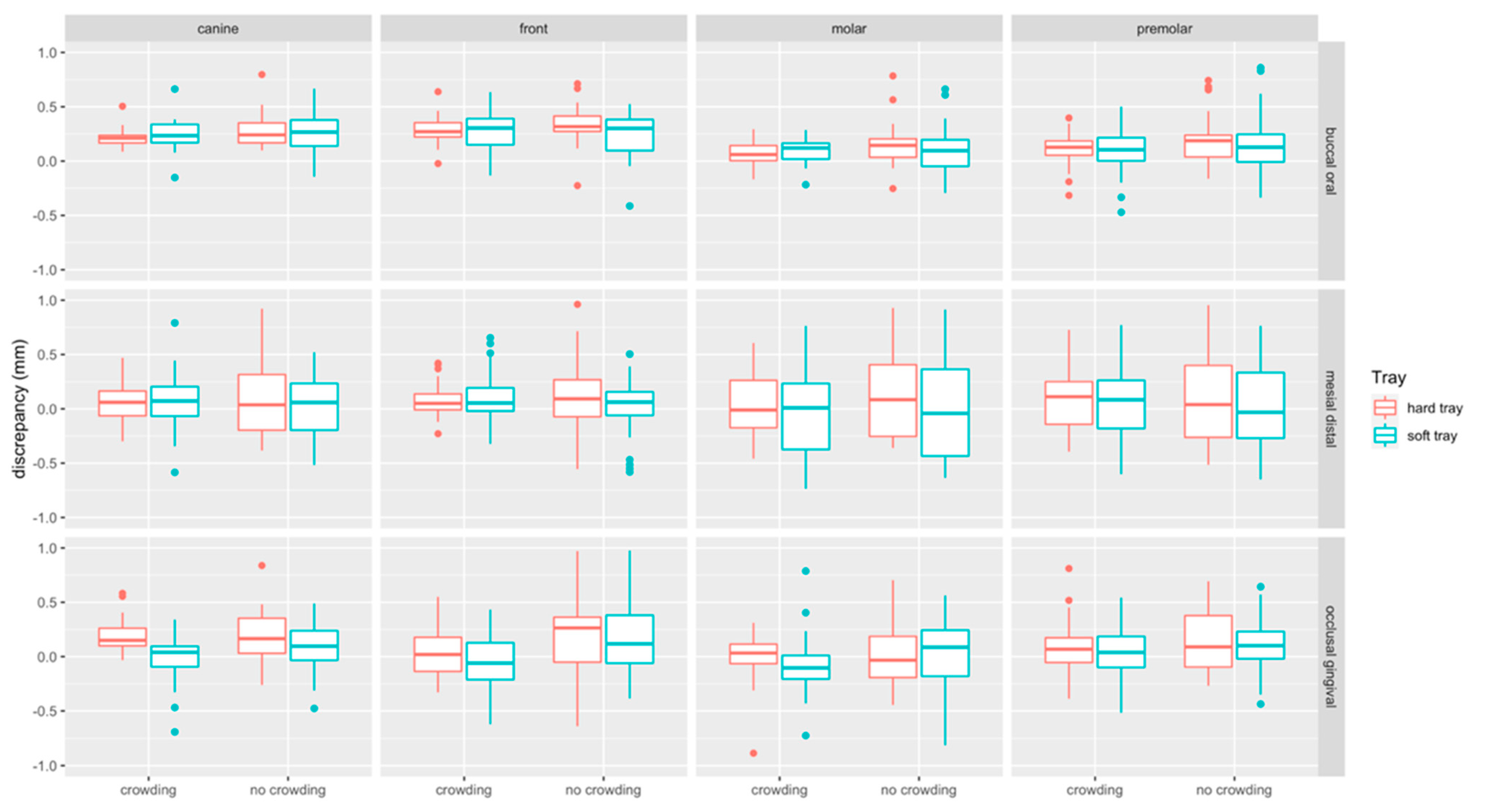
3.2. Bracket Bonding Accuracy (Linear Measurements)
3.2.1. Impact of Crowding
3.2.2. Impact of Tray Type
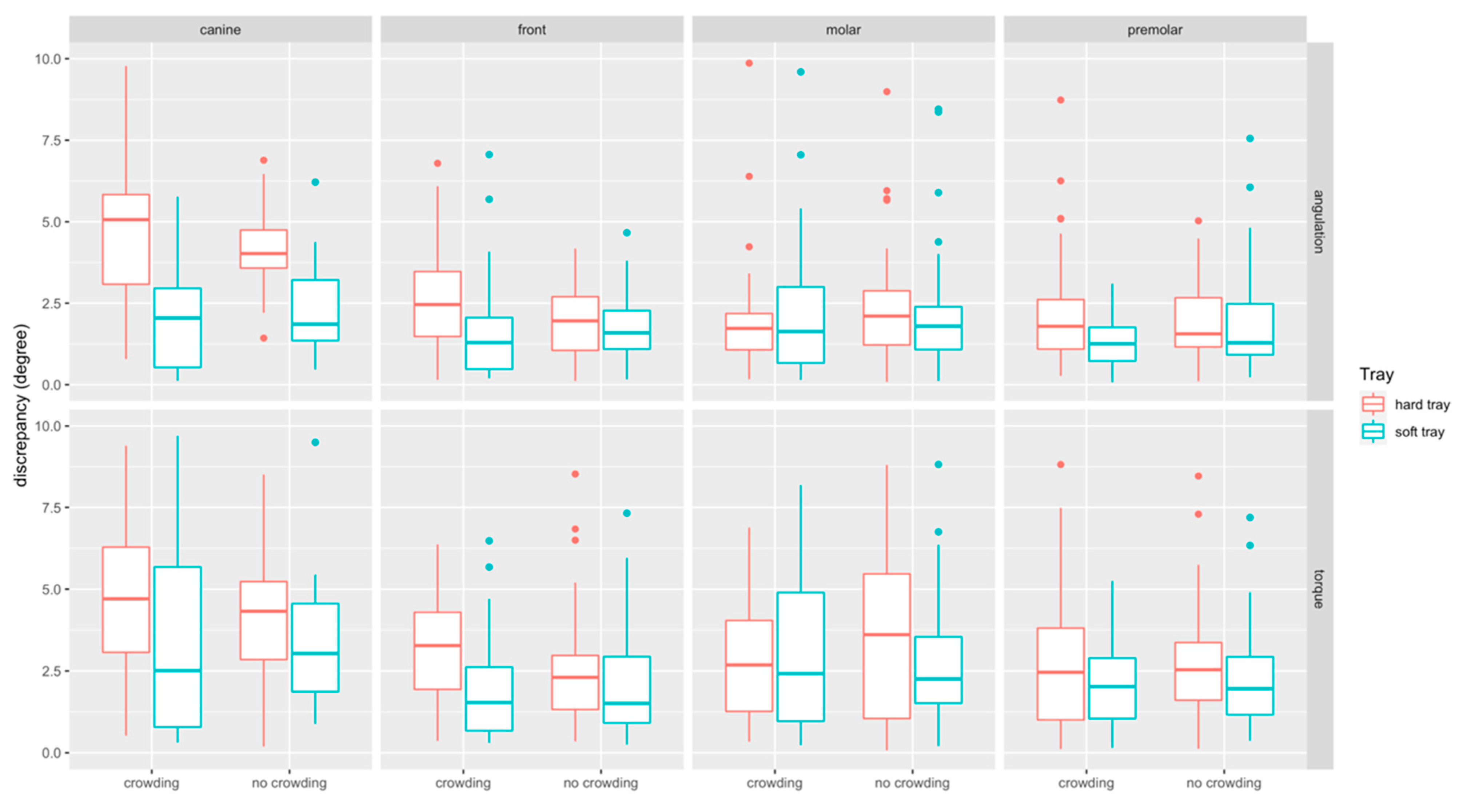
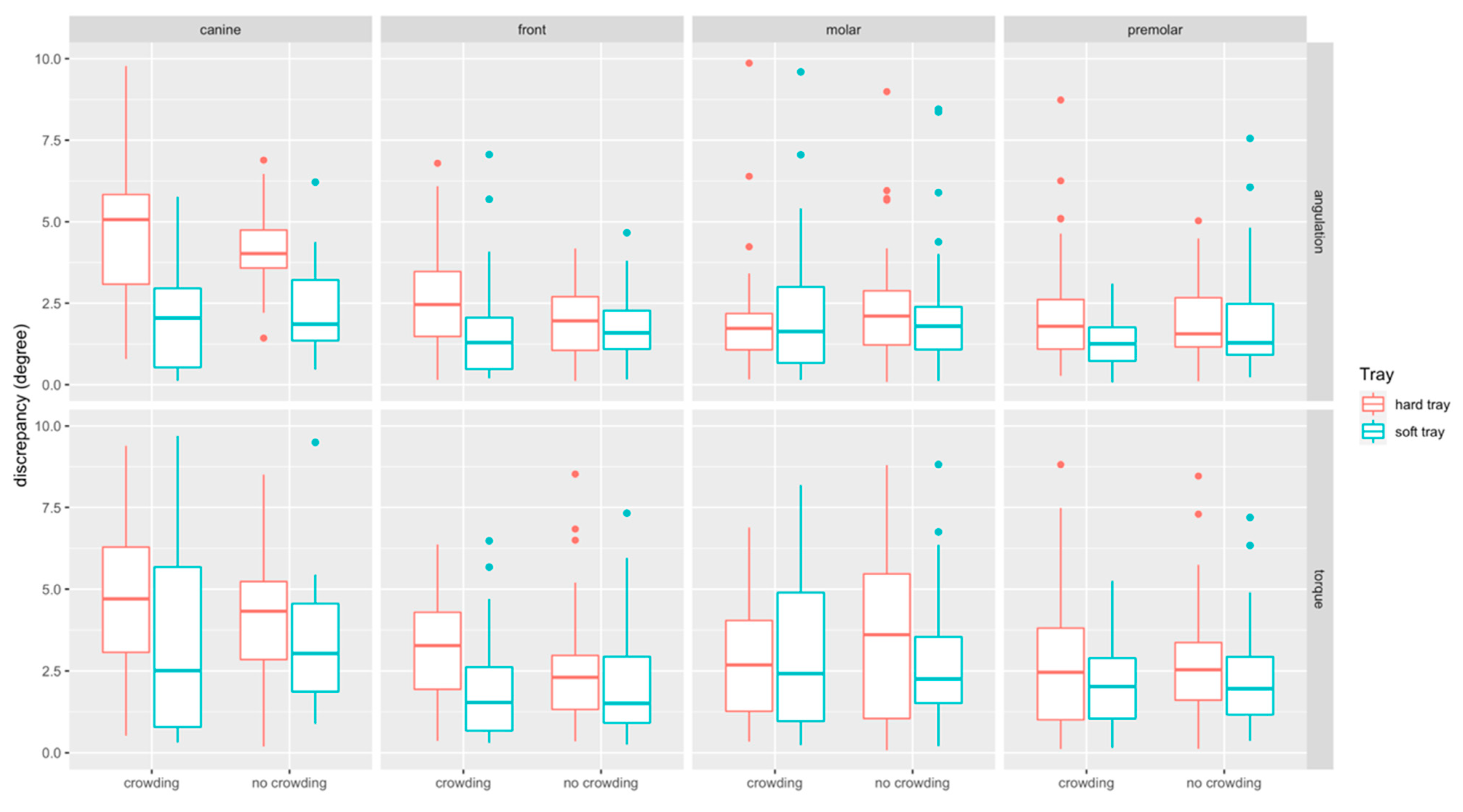
3.3. Bracket Bonding Accuracy (Angular Measurements)
3.3.1. Impact of Crowding
3.3.2. Impact of the Tray Type
4. Discussion
5. Conclusions
- The present study found that intraoral scanning may severely impede measurements to assess the accuracy of bracket transfer, whereas micro-CT was shown to be a highly reliable alternative for in vitro settings.
- We demonstrated that linear discrepancies were below the ABO-range of 0.5 mm, most of the angular discrepancies were not within the clinical acceptable limit of 2°.
- Severe crowding and transfer tray hardness have an impact on transfer tray accuracy, and bonding with the soft transfer tray was more accurate in cases of severe crowding.
- Front teeth were most frequently affected by bonding errors, followed by canines and molars.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Andrews, L.F. The six keys to normal occlusion. Am. J. Orthod. 1972, 62, 296–309. [Google Scholar] [CrossRef]
- Andrews, L.F. The straight-wire appliance, origin, controversy, commentary. J. Clin. Orthod. 1976, 10, 99–114. [Google Scholar]
- Andrews, L.F. The straight-wire appliance. Explained and compared. J. Clin. Orthod. 1976, 10, 174–195. [Google Scholar] [PubMed]
- Andrews, L.F. Straight Wire: The Concept and Appliance; Wells: San Diego, CA, USA, 1989; ISBN 0961625600. [Google Scholar]
- Shpack, N.; Geron, S.; Floris, I.; Davidovitch, M.; Brosh, T.; Vardimon, A.D. Bracket placement in lingual vs labial systems and direct vs indirect bonding. Angle Orthod. 2007, 77, 509–517. [Google Scholar] [CrossRef] [Green Version]
- Silverman, E.; Cohen, M.; Gianelly, A.A.; Dietz, V.S. A universal direct bonding system for both metal and plastic brackets. Am. J. Orthod. 1972, 62, 236–244. [Google Scholar] [CrossRef]
- Sondhi, A. Efficient and effective indirect bonding. Am. J. Orthod. Dentofac. Orthop. 1999, 115, 352–359. [Google Scholar] [CrossRef]
- Yi, G.K.; Dunn, W.J.; Taloumis, L.J. Shear bond strength comparison between direct and indirect bonded orthodontic brackets. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 577–581. [Google Scholar] [CrossRef]
- Linn, B.J.; Berzins, D.W.; Dhuru, V.B.; Bradley, T.G. A comparison of bond strength between direct- and indirect-bonding methods. Angle Orthod. 2006, 76, 289–294. [Google Scholar] [CrossRef]
- Menini, A.; Cozzani, M.; Sfondrini, M.F.; Scribante, A.; Cozzani, P.; Gandini, P. A 15-month evaluation of bond failures of orthodontic brackets bonded with direct versus indirect bonding technique: A clinical trial. Prog. Orthod. 2014, 15, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swetha, M.; Pai, V.S.; Sanjay, N.; Nandini, S. Indirect versus direct bonding—A shear bond strength comparison: An in vitro study. J. Contemp. Dent. Pract. 2011, 12, 232–238. [Google Scholar]
- McLaughlin, R.P.; Bennett, J.C.; Trevisi, H.J. Systemized Orthodontic Treatment Mechanics; Reprinted; Mosby: Edinburgh, UK, 2002; ISBN 0-7234-3171-X. [Google Scholar]
- Ciuffolo, F.; Tenisci, N.; Pollutri, L. Modified bonding technique for a standardized and effective indirect bonding procedure. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 504–509. [Google Scholar] [CrossRef]
- Hickham, J.H. Predictable indirect bonding. J. Clin. Orthod. 1993, 27, 215–217. [Google Scholar]
- Gracco, A.; Tracey, S. The insignia system of customized orthodontics. J. Clin. Orthod. 2011, 45, 442–451. [Google Scholar] [PubMed]
- Kalange, J.T. Ideal appliance placement with APC brackets and indirect bonding. J. Clin. Orthod. 1999, 33, 516–526. [Google Scholar] [PubMed]
- Matsuno, I.; Okuda, S.; Nodera, Y. The hybrid core system for indirect bonding. J. Clin. Orthod. 2003, 37, 160–168. [Google Scholar]
- Castilla, A.E.; Crowe, J.J.; Moses, J.R.; Wang, M.; Ferracane, J.L.; Covell, D.A. Measurement and comparison of bracket transfer accuracy of five indirect bonding techniques. Angle Orthod. 2014, 84, 607–614. [Google Scholar] [CrossRef] [Green Version]
- Duarte, M.E.A.; Gribel, B.F.; Spitz, A.; Artese, F.; Miguel, J.A.M. Reproducibility of digital indirect bonding technique using three-dimensional (3D) models and 3D-printed transfer trays. Angle Orthod. 2020, 90, 92–99. [Google Scholar] [CrossRef] [Green Version]
- Niu, Y.; Zeng, Y.; Zhang, Z.; Xu, W.; Xiao, L. Comparison of the transfer accuracy of two digital indirect bonding trays for labial bracket bonding. Angle Orthod. 2020. [Google Scholar] [CrossRef]
- Pottier, T.; Brient, A.; Turpin, Y.L.; Chauvel, B.; Meuric, V.; Sorel, O.; Brezulier, D. Accuracy evaluation of bracket repositioning by indirect bonding: Hard acrylic CAD/CAM versus soft one-layer silicone trays, an in vitro study. Clin. Oral Investig. 2020, 24, 3889–3897. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Yang, C.; Li, Y.; Xia, D.; Shi, T.; Li, C. Comparison of three-dimensional printing guides and double-layer guide plates in accurate bracket placement. BMC Oral Health 2020, 20, 127. [Google Scholar] [CrossRef]
- Koch, P.J. Measuring the accuracy of a computer-aided design and computer-aided manufacturing-based indirect bonding tray. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 315. [Google Scholar] [CrossRef] [PubMed]
- Little, R.M. The Irregularity Index: A quantitative score of mandibular anterior alignment. Am. J. Orthod. 1975, 68, 554–563. [Google Scholar] [CrossRef]
- Koretsi, V.; Kirschbauer, C.; Proff, P.; Kirschneck, C. Reliability and intra-examiner agreement of orthodontic model analysis with a digital caliper on plaster and printed dental models. Clin. Oral Investig. 2019, 23, 3387–3396. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.; Wilmes, B.; Grandjean, C.; Drescher, D. Impact of manual control point selection accuracy on automated surface matching of digital dental models. Clin. Oral Investig. 2018, 22, 801–810. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Taylor and Francis: Hoboken, NJ, USA, 2013; ISBN 9780805802832. [Google Scholar]
- Xue, C.; Xu, H.; Guo, Y.; Xu, L.; Dhami, Y.; Wang, H.; Liu, Z.; Ma, J.; Bai, D. Accurate bracket placement using a computer-aided design and computer-aided manufacturing-guided bonding device: An in vivo study. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 269–277. [Google Scholar] [CrossRef] [Green Version]
- Süpple, J.; von Glasenapp, J.; Hofmann, E.; Jost-Brinkmann, P.-G.; Koch, P.J. Accurate bracket placement with an indirect bonding method using digitally designed transfer models printed in different orientations—An in vitro study. JCM 2021, 10, 2002. [Google Scholar] [CrossRef] [PubMed]
- Möhlhenrich, S.C.; Alexandridis, C.; Peters, F.; Kniha, K.; Modabber, A.; Danesh, G.; Fritz, U. Three-dimensional evaluation of bracket placement accuracy and excess bonding adhesive depending on indirect bonding technique and bracket geometry: An in-vitro study. Head Face Med. 2020, 16, 17. [Google Scholar] [CrossRef] [PubMed]
- Grünheid, T.; Lee, M.S.; Larson, B.E. Transfer accuracy of vinyl polysiloxane trays for indirect bonding. Angle Orthod. 2016, 86, 468–474. [Google Scholar] [CrossRef] [Green Version]
- Heo, H.; Kim, M. The effects of orthodontic brackets on the time and accuracy of digital impression taking. Int. J. Environ. Res. Public Health 2021, 18, 5282. [Google Scholar] [CrossRef]
- Kim, Y.-K.; Kim, S.-H.; Choi, T.-H.; Yen, E.H.; Zou, B.; Shin, Y.; Lee, N.-K. Accuracy of intraoral scan images in full arch with orthodontic brackets: A retrospective in vivo study. Clin. Oral Investig. 2021. [Google Scholar] [CrossRef]
- Quaas, S.; Loos, R.; Sporbeck, H.; Luthardt, R. Analyse des einflusses der puderapplikation auf die genauigkeit optischer digitalisierungen. Dtsch. Zahnarztl. Z. 2005, 60, 96–99. [Google Scholar]
- Kang, S.-J.; Kee, Y.-J.; Lee, K.C. Effect of the presence of orthodontic brackets on intraoral scans. Angle Orthod. 2021, 91, 98–104. [Google Scholar] [CrossRef]
- Casko, J.S.; Vaden, J.L.; Kokich, V.G.; Damone, J.; James, R.; Cangialosi, T.J.; Riolo, M.L.; Owens, S.E.; Bills, E.D. Objective grading system for dental casts and panoramic radiographs. Am. J. Orthod. Dentofac. Orthop. 1998, 114, 589–599. [Google Scholar] [CrossRef]
- Schmid, J.; Brenner, D.; Recheis, W.; Hofer-Picout, P.; Brenner, M.; Crismani, A.G. Transfer accuracy of two indirect bonding techniques-an in vitro study with 3D scanned models. Eur. J. Orthod. 2018, 40, 549–555. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tooth Type | Tray | Measurement | MD | IQR | MD | IQR | p-Value |
|---|---|---|---|---|---|---|---|
| No crowding (LII < 3) | Crowding (LII > 7) | Crowding vs. no crowding | |||||
| Canine (n = 40) | Hard | Angulation (°) | 4.02 | 1.33 | 5.07 | 2.88 | 0.529 |
| Soft | Angulation (°) | 1.86 | 2.07 | 2.04 | 2.59 | 0.445 | |
| p-value hard vs. soft tray (r) | <0.001 (0.58) *** | <0.001 (0.56) *** | |||||
| Hard | Buccal/oral (mm) | 0.24 | 0.2 | 0.21 | 0.09 | 0.201 | |
| Soft | Buccal/oral (mm) | 0.27 | 0.29 | 0.23 | 0.18 | 0.698 | |
| p-value hard vs. soft tray (r) | 0.968 | 0.327 | |||||
| Hard | Mesial/distal (mm) | 0.04 | 0.54 | 0.06 | 0.24 | 0.989 | |
| Soft | Mesial/distal (mm) | 0.06 | 0.45 | 0.07 | 0.38 | 0.678 | |
| p-value hard vs. soft tray (r) | 0.495 | 0.841 | |||||
| Hard | Occlusal/gingival (mm) | 0.16 | 0.37 | 0.15 | 0.24 | 0.799 | |
| Soft | Occlusal/gingival (mm) | 0.10 | 0.29 | 0.04 | 0.21 | 0.211 | |
| p-value hard vs. soft tray (r) | 0.398 | 0.005 (0.45) ** | |||||
| Hard | Torque (°) | 4.32 | 2.63 | 4.7 | 3.32 | 0.461 | |
| Soft | Torque (°) | 3.52 | 3.04 | 2.51 | 5.04 | 0.341 | |
| p-value hard vs. soft tray. (r) | 0.289 | 0.096 | |||||
| Front (n = 80) | Hard | Angulation (°) | 1.96 | 1.7 | 2.46 | 2.25 | 0.053 |
| Soft | Angulation (°) | 1.59 | 1.19 | 1.29 | 1.64 | 0.178 | |
| p-value hard vs. soft tray (r) | 0.308 | 0.001 (0.39) ** | |||||
| Hard | Buccal/oral (mm) | 0.32 | 0.15 | 0.27 | 0.14 | 0.083 | |
| Soft | Buccal/oral (mm) | 0.30 | 0.30 | 0.3 | 0.24 | 0.722 | |
| p-value hard vs. soft tray (r) | 0.065 | 0.923 | |||||
| Hard | Mesial/distal (mm) | 0.09 | 0.38 | 0.05 | 0.15 | 0.607 | |
| Soft | Mesial/distal (mm) | 0.06 | 0.22 | 0.05 | 0.26 | 0.624 | |
| p-value hard vs. soft tray (r) | 0.384 | 0.769 | |||||
| Hard | Occlusal/gingival (mm) | 0.26 | 0.43 | 0.02 | 0.32 | 0.015 (0.27) * | |
| Soft | Occlusal/gingival (mm) | 0.12 | 0.45 | −0.07 | 0.37 | 0.001 (0.36) * | |
| p-value hard vs. soft tray (r) | 0.554 | 0.068 | |||||
| Hard | Torque (°) | 2.31 | 2.01 | 3.28 | 2.49 | 0.028 (0.25) * | |
| Soft | Torque (°) | 1.64 | 2.34 | 1.54 | 2.07 | 0.439 | |
| p-value hard vs. soft tray (r) | 0.312 | <0.001 (0.41) *** | |||||
| Molar (n= 80) | Hard | Angulation (°) | 2.11 | 2.01 | 1.73 | 1.22 | 0.163 |
| Soft | Angulation (°) | 1.8 | 1.35 | 1.65 | 2.8 | 0.577 | |
| p-value hard vs. soft tray (r) | 0.366 | 0.773 | |||||
| Hard | Buccal/oral (mm) | 0.14 | 0.17 | 0.06 | 0.15 | 0.029 (0.24) * | |
| Soft | Buccal/oral (mm) | 0.10 | 0.25 | 0.12 | 0.15 | 0.6 | |
| p-value hard vs. soft tray (r) | 0.14 | 0.296 | |||||
| Hard | Mesial/distal (mm) | 0.08 | 0.68 | −0.01 | 0.45 | 0.788 | |
| Soft | Mesial/distal (mm) | −0.04 | 0.82 | 0.07 | 0.66 | 0.893 | |
| p-value (hard vs. soft tray) | 0.159 | 0.368 | |||||
| Hard | Occlusal/gingival (mm) | −0.03 | 0.4 | 0.03 | 0.22 | 0.61 | |
| Soft | Occlusal/gingival (mm) | 0.09 | 0.43 | −0.12 | 0.23 | 0.007 (0.30) ** | |
| p-value hard vs. soft tray (r) | 0.583 | 0.002 (0.34) ** | |||||
| Hard | Torque (°) | 3.61 | 4.73 | 2.71 | 3.04 | 0.405 | |
| Soft | Torque (°) | 2.26 | 2.23 | 3.23 | 5.27 | 0.470 | |
| p-value hard vs. soft tray (r) | 0.189 | 0.7 | |||||
| Premolar (n= 80) | Hard | Angulation (°) | 1.59 | 1.7 | 1.79 | 1.66 | 0.707 |
| Soft | Angulation (°) | 1.43 | 1.63 | 1.3 | 1.11 | 0.178 | |
| p-value hard vs. soft tray (r) | 0.441 | 0.009 (0.29) ** | |||||
| Hard | Buccal/oral (mm) | 0.19 | 0.23 | 0.13 | 0.14 | 0.119 | |
| Soft | Buccal/oral (mm) | 0.14 | 0.29 | 0.10 | 0.22 | 0.56 | |
| p-value hard vs. soft tray (r) | 0.242 | 0.14 | |||||
| Hard | Mesial/distal (mm) | 0.04 | 0.67 | 0.11 | 0.41 | 0.9 | |
| Soft | Mesial/distal (mm) | −0.03 | 0.61 | 0.12 | 0.5 | 0.669 | |
| p-value hard vs. soft tray (r) | 0.634 | 0.954 | |||||
| Hard | Occlusal/gingival (mm) | 0.09 | 0.54 | 0.07 | 0.29 | 0.462 | |
| Soft | Occlusal/gingival (mm) | 0.1 | 0.28 | 0.04 | 0.29 | 0.248 | |
| p-value hard vs. soft tray (r) | 0.747 | 0.488 | |||||
| Hard | Torque (°) | 2.60 | 2.03 | 2.46 | 1.94 | 0.476 | |
| Soft | Torque (°) | 1.96 | 1.83 | 2.05 | 2.03 | 0.693 | |
| p-value hard vs. soft tray (r) | 0.057 | 0.163 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jungbauer, R.; Breunig, J.; Schmid, A.; Hüfner, M.; Kerberger, R.; Rauch, N.; Proff, P.; Drescher, D.; Becker, K. Transfer Accuracy of Two 3D Printed Trays for Indirect Bracket Bonding—An In Vitro Pilot Study. Appl. Sci. 2021, 11, 6013. https://doi.org/10.3390/app11136013
Jungbauer R, Breunig J, Schmid A, Hüfner M, Kerberger R, Rauch N, Proff P, Drescher D, Becker K. Transfer Accuracy of Two 3D Printed Trays for Indirect Bracket Bonding—An In Vitro Pilot Study. Applied Sciences. 2021; 11(13):6013. https://doi.org/10.3390/app11136013
Chicago/Turabian StyleJungbauer, Rebecca, Jonas Breunig, Alois Schmid, Mira Hüfner, Robert Kerberger, Nicole Rauch, Peter Proff, Dieter Drescher, and Kathrin Becker. 2021. "Transfer Accuracy of Two 3D Printed Trays for Indirect Bracket Bonding—An In Vitro Pilot Study" Applied Sciences 11, no. 13: 6013. https://doi.org/10.3390/app11136013
APA StyleJungbauer, R., Breunig, J., Schmid, A., Hüfner, M., Kerberger, R., Rauch, N., Proff, P., Drescher, D., & Becker, K. (2021). Transfer Accuracy of Two 3D Printed Trays for Indirect Bracket Bonding—An In Vitro Pilot Study. Applied Sciences, 11(13), 6013. https://doi.org/10.3390/app11136013