
The Effect of Transcutaneous Application of Gaseous CO2 on Diabetic Symmetrical Peripheral Neuropathy—A Double-Blind Randomized Clinical Trial


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Chao, C.C.; Hsieh, S.C.; Yang, W.S.; Lin, Y.H.; Lin, W.M.; Tai, T.Y.; Hsieh, S.T. Glycemic control is related to the severity of impaired thermal sensations in type 2 diabetes. Diabetes Met. Res. Rev. 2007, 23, 612–620. [Google Scholar] [CrossRef]
- Sveen, K.A.; Karimé, B.; Jørum, E.; Mellgren, S.I.; Fagerland, M.W.; Monnier, V.M.; Dahl-Jørgensen, K.; Hanssen, K.F. Small- and large-fiber neuropathy after 40 years of type 1 diabetes: Associations with glycemic control and advanced protein glycation: The Oslo Study. Diabetes Care 2013, 36, 3712–3717. [Google Scholar] [CrossRef] [Green Version]
- Bansal, V.; Kalita, J.; Misra, U.K. Diabetic neuropathy. Postgrad Med. J. 2006, 82, 95–100. [Google Scholar] [CrossRef]
- Tesfaye, S.; Boulton, A.J.; Dyck, P.J.; Freeman, R.; Horowitz, M.; Kempler, P.; Lauria, G.; Malik, R.A.; Spallone, V.; Vinik, A.; et al. Diabetic neuropathies: Update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care 2010, 33, 2285–2293. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 5. Lifestyle Management: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S46–S60. [Google Scholar] [CrossRef] [Green Version]
- Feldman, E.L.; Nave, K.A.; Jensen, T.S.; Bennett, D.L.H. New Horizons in Diabetic Neuropathy: Mechanisms, Bioenergetics, and Pain. Neuron 2017, 93, 1296–1313. [Google Scholar] [CrossRef] [Green Version]
- Callaghan, B.C.; Cheng, H.T.; Stables, C.L.; Smith, A.L.; Feldman, E.L. Diabetic neuropathy: Clinical manifestations and current treatments. Lancet Neurol. 2012, 11, 521–534. [Google Scholar] [CrossRef] [Green Version]
- Hicks, C.W.; Selvin, E. Epidemiology of Peripheral Neuropathy and Lower Extremity Disease in Diabetes. Curr. Diab. Rep. 2019, 19, 86. [Google Scholar] [CrossRef]
- Iqbal, Z.; Azmi, S.; Yadav, R.; Ferdousi, M.; Kumar, M.; Cuthbertson, D.J.; Lim, J.; Malik, R.A.; Alam, U. Diabetic Peripheral Neuropathy: Epidemiology, Diagnosis, and Pharmacotherapy. Clin. Ther. 2018, 40, 828–849. [Google Scholar] [CrossRef] [Green Version]
- Snyder, M.J.; Gibbs, L.M.; Lindsay, T.J. Treating Painful Diabetic Peripheral Neuropathy: An Update. Am. Fam. Phys. 2016, 94, 227–234. [Google Scholar]
- Naderi Nabi, B.; Sedighinejad, A.; Haghighi, M.; Biazar, G.; Hashemi, M.; Haddadi, S.; Fathi, A. Comparison of Transcutaneous Electrical Nerve Stimulation and Pulsed Radiofrequency Sympathectomy for Treating Painful Diabetic Neuropathy. Anesth. Pain Med. 2015, 5, e29280. [Google Scholar] [CrossRef] [Green Version]
- Lavery, L.A.; Murdoch, D.P.; Williams, J.; Lavery, D.C. Does anodyne light therapy improve peripheral neuropathy in diabetes? A double-blind, sham-controlled, randomized trial to evaluate monochromatic infrared photoenergy. Diabetes Care 2008, 31, 316–321. [Google Scholar] [CrossRef] [Green Version]
- Nawfar, S.A.; Yacob, N.B. Effects of monochromatic infrared energy therapy on diabetic feet with peripheral sensory neuropathy: A randomised controlled trial. Singap. Med. J. 2011, 52, 669–672. [Google Scholar]
- Robinson, C.C.; Klahr, P.D.S.; Stein, C.; Falavigna, M.; Sbruzzi, G.; Plentz, R.D.M. Effects of monochromatic infrared phototherapy in patients with diabetic peripheral neuropathy: A systematic review and meta-analysis of randomized controlled trials. Braz. J. Phys. 2017, 21, 233–243. [Google Scholar] [CrossRef]
- Kerstman, E.; Ahn, S.; Battu, S.; Tariq, S.; Grabois, M. Neuropathic pain. Handb Clin. Neurol. 2013, 110, 175–187. [Google Scholar] [CrossRef]
- Macura, M.; Ban Frangez, H.; Cankar, K.; Finžgar, M.; Frangez, I. The effect of transcutaneous application of gaseous CO2 on diabetic chronic wound healing-A double-blind randomized clinical trial. Int. Wound J. 2020, 17, 1607–1614. [Google Scholar] [CrossRef]
- Sakai, Y.; Miwa, M.; Oe, K.; Ueha, T.; Koh, A.; Niikura, T.; Iwakura, T.; Lee, S.Y.; Tanaka, M.; Kurosaka, M. A novel system for transcutaneous application of carbon dioxide causing an “artificial Bohr effect” in the human body. PLoS ONE 2011, 6, e24137. [Google Scholar] [CrossRef]
- Hartmann, B.R.; Bassenge, E.; Hartmann, M. Effects of serial percutaneous application of carbon dioxide in intermittent claudication: Results of a controlled trial. Angiology 1997, 48, 957–963. [Google Scholar] [CrossRef]
- Finzgar, M.; Melik, Z.; Cankar, K. Effect of transcutaneous application of gaseous carbon dioxide on cutaneous microcirculation. Clin. Hemorheol. Microcirc. 2015, 60, 423–435. [Google Scholar] [CrossRef]
- Oda, T.; Iwakura, T.; Fukui, T.; Oe, K.; Mifune, Y.; Hayashi, S.; Matsumoto, T.; Matsushita, T.; Kawamoto, T.; Sakai, Y.; et al. Effects of the duration of transcutaneous CO2 application on the facilitatory effect in rat fracture repair. J. Orthop. Sci. 2020, 25, 886–891. [Google Scholar] [CrossRef]
- Ueha, T.; Oe, K.; Miwa, M.; Hasegawa, T.; Koh, A.; Nishimoto, H.; Lee, S.Y.; Niikura, T.; Kurosaka, M.; Kuroda, R.; et al. Increase in carbon dioxide accelerates the performance of endurance exercise in rats. J. Physiol. Sci. 2018, 68, 463–470. [Google Scholar] [CrossRef]
- Stirban, A. Microvascular dysfunction in the context of diabetic neuropathy. Curr. Diab. Rep. 2014, 14, 541. [Google Scholar] [CrossRef]
- Moghtaderi, A.; Bakhshipour, A.; Rashidi, H. Validation of Michigan neuropathy screening instrument for diabetic peripheral neuropathy. Clin. Neurol. Neurosurg. 2006, 108, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Pop-Busui, R.; Boulton, A.J.; Feldman, E.L.; Bril, V.; Freeman, R.; Malik, R.A.; Sosenko, J.M.; Ziegler, D. Diabetic Neuropathy: A Position Statement by the American Diabetes Association. Diabetes Care 2017, 40, 136–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sosenko, J.M.; Sparling, Y.H.; Hu, D.; Welty, T.; Howard, B.V.; Lee, E.; Robbins, D.C. Use of the Semmes-Weinstein monofilament in the strong heart study. Risk factors for clinical neuropathy. Diabetes Care 1999, 22, 1715–1721. [Google Scholar] [CrossRef] [PubMed]
- Østergaard, L.; Finnerup, N.B.; Terkelsen, A.J.; Olesen, R.A.; Drasbek, K.R.; Knudsen, L.; Jespersen, S.N.; Frystyk, J.; Charles, M.; Thomsen, R.W.; et al. The effects of capillary dysfunction on oxygen and glucose extraction in diabetic neuropathy. Diabetologia 2015, 58, 666–677. [Google Scholar] [CrossRef] [Green Version]
- Tesfaye, S.; Selvarajah, D. Advances in the epidemiology, pathogenesis and management of diabetic peripheral neuropathy. Diabetes Metab Res. Rev. 2012, 28, 8–14. [Google Scholar] [CrossRef]
- Kreska, Z.; Németh, B.; Kiss, I.; Péter, I.; Ajtay, Z.; Hejjel, L. Transcutaneous Carbon Dioxide Treatment Affects Heart Rate Variability—A Pilot Study. In Vivo 2018, 32, 1259–1264. [Google Scholar] [CrossRef] [Green Version]
- Németh, B.; Kiss, I.; Ajtay, B.; Péter, I.; Kreska, Z.; Cziráki, A.; Horváth, I.G.; Ajtay, Z. Transcutaneous Carbon Dioxide Treatment Is Capable of Reducing Peripheral Vascular Resistance in Hypertensive Patients. In Vivo 2018, 32, 1555–1559. [Google Scholar] [CrossRef] [Green Version]
- Nemeth, B.; Kiss, I.; Jencsik, T.; Peter, I.; Kreska, Z.; Koszegi, T.; Miseta, A.; Kustan, P.; Boncz, I.; Laczo, A.; et al. Angiotensin-converting Enzyme Inhibition Improves the Effectiveness of Transcutaneous Carbon Dioxide Treatment. In Vivo 2017, 31, 425–428. [Google Scholar] [CrossRef] [Green Version]
- Green, A.Q.; Krishnan, S.; Finucane, F.M.; Rayman, G. Altered C-fiber function as an indicator of early peripheral neuropathy in individuals with impaired glucose tolerance. Diabetes Care 2010, 33, 174–176. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.G.; Ramachandran, P.; Tripp, S.; Singleton, J.R. Epidermal nerve innervation in impaired glucose tolerance and diabetes-associated neuropathy. Neurology 2001, 57, 1701–1704. [Google Scholar] [CrossRef]
- Vas, P.R.; Green, A.Q.; Rayman, G. Small fibre dysfunction, microvascular complications and glycaemic control in type 1 diabetes: A case-control study. Diabetologia 2012, 55, 795–800. [Google Scholar] [CrossRef] [PubMed]
- Jörneskog, G.; Brismar, K.; Fagrell, B. Skin capillary circulation severely impaired in toes of patients with IDDM, with and without late diabetic complications. Diabetologia 1995, 38, 474–480. [Google Scholar] [CrossRef] [PubMed]
- Stansberry, K.B.; Peppard, H.R.; Babyak, L.M.; Popp, G.; McNitt, P.M.; Vinik, A.I. Primary nociceptive afferents mediate the blood flow dysfunction in non-glabrous (hairy) skin of type 2 diabetes: A new model for the pathogenesis of microvascular dysfunction. Diabetes Care 1999, 22, 1549–1554. [Google Scholar] [CrossRef] [PubMed]
- Finžgar, M.; Frangež, H.B.; Cankar, K.; Frangež, I. Transcutaneous application of the gaseous CO2 for improvement of the microvascular function in patients with diabetic foot ulcers. Microvasc Res. 2021, 133, 104100. [Google Scholar] [CrossRef]
- Shalan, N.; Al-Bazzaz, A.; Al-Ani, I.; Najem, F.; Al-Masri, M. Effect of Carbon Dioxide Therapy on Diabetic Foot Ulcer. J. Diabetes Mellit. 2015, 5, 284–289. [Google Scholar] [CrossRef] [Green Version]
- Abdulhamza, G.R.; Al-Omary, H.I. Physiological Effects of Carbon Dioxide Treatment on Diabetic Foot Ulcer Patients. J. Pharm. Biol. Sci. 2018, 13, 1–7. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Study Group | Control Group | p | |
|---|---|---|---|
| No. of patients | 30 (24 M, 6 F) | 30 (24 M, 6 F) | 1.000 |
| Average age of patients (years ± SD) | 65.3 ± 11.9 | 66.76± 10.6 | 0.640 |
| BMI (mean kg/m2 ± SD) Tobacco smokers yes/no | 29.85 ± 5.0 4/26 | 30.2 ± 4.9 3/27 | 0.756 1.000 |
| HbA1c before therapy (mean% ± SD) | 7.08 ± 0.85 | 7.00 ± 0.90 | 0.736 |
| Diabetes mellitus type (type 1/type 2) | 1/29 | 2/28 | 0.999 |
| Average score on Michigan neuropathy scoring instrument (score ± SD) | 8.23 ± 2.61 | 8.67 ± 2.55 | 0.518 |
| Study Group (N = 30) | Control Group (N = 30) | |||
|---|---|---|---|---|
| Before CO2 Therapies a | After CO2 Therapies b | Before placebo treatment c | After placebo Treatment d | |
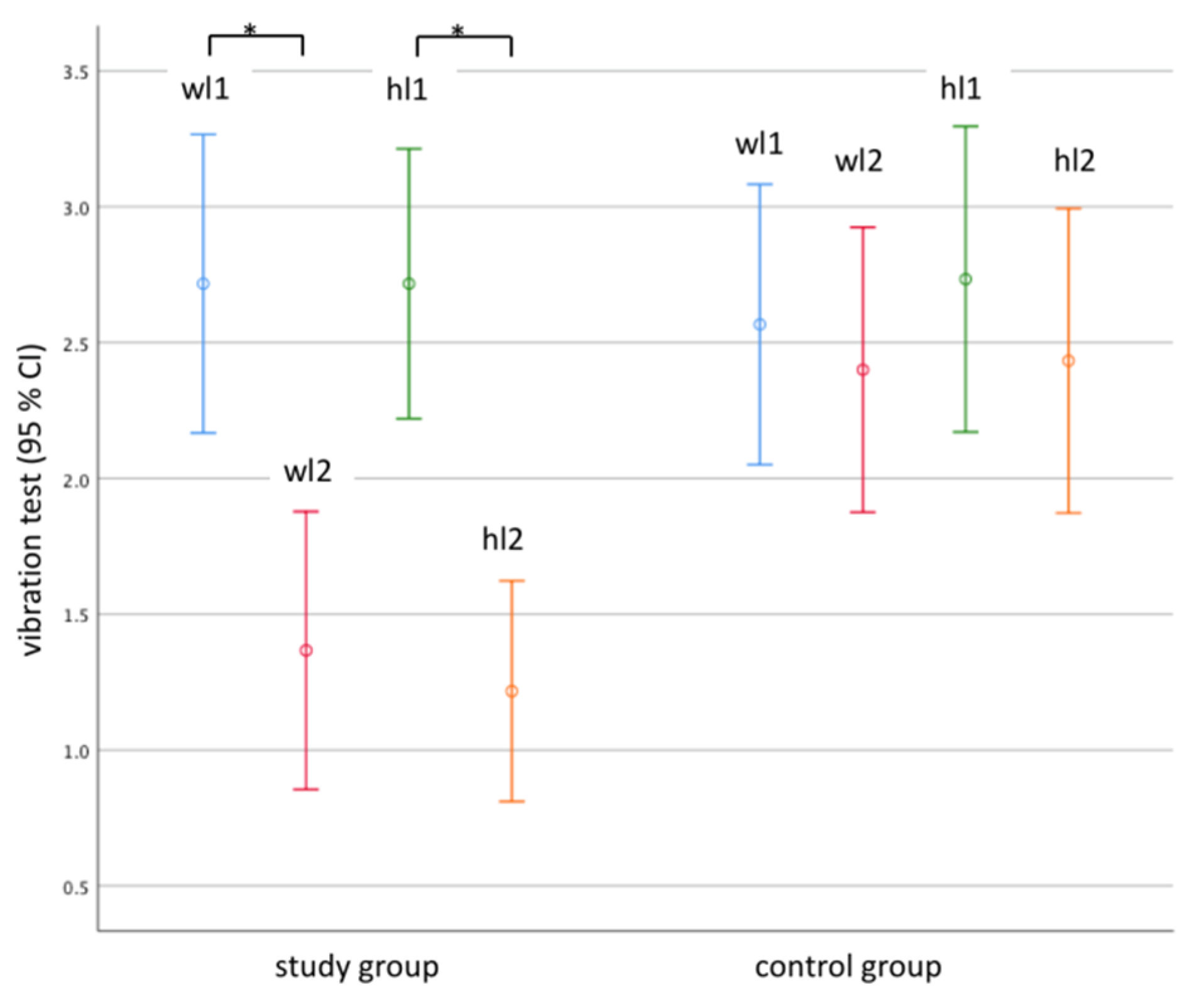
| Vibration sensation score | 5.467 ± 2.573 | 2.583 ± 2.173 | 5.333 ± 2.537 | 4.867 ± 2.596 |
| p vibration ab < 0.001 | p vibration cd = 0.242 | |||
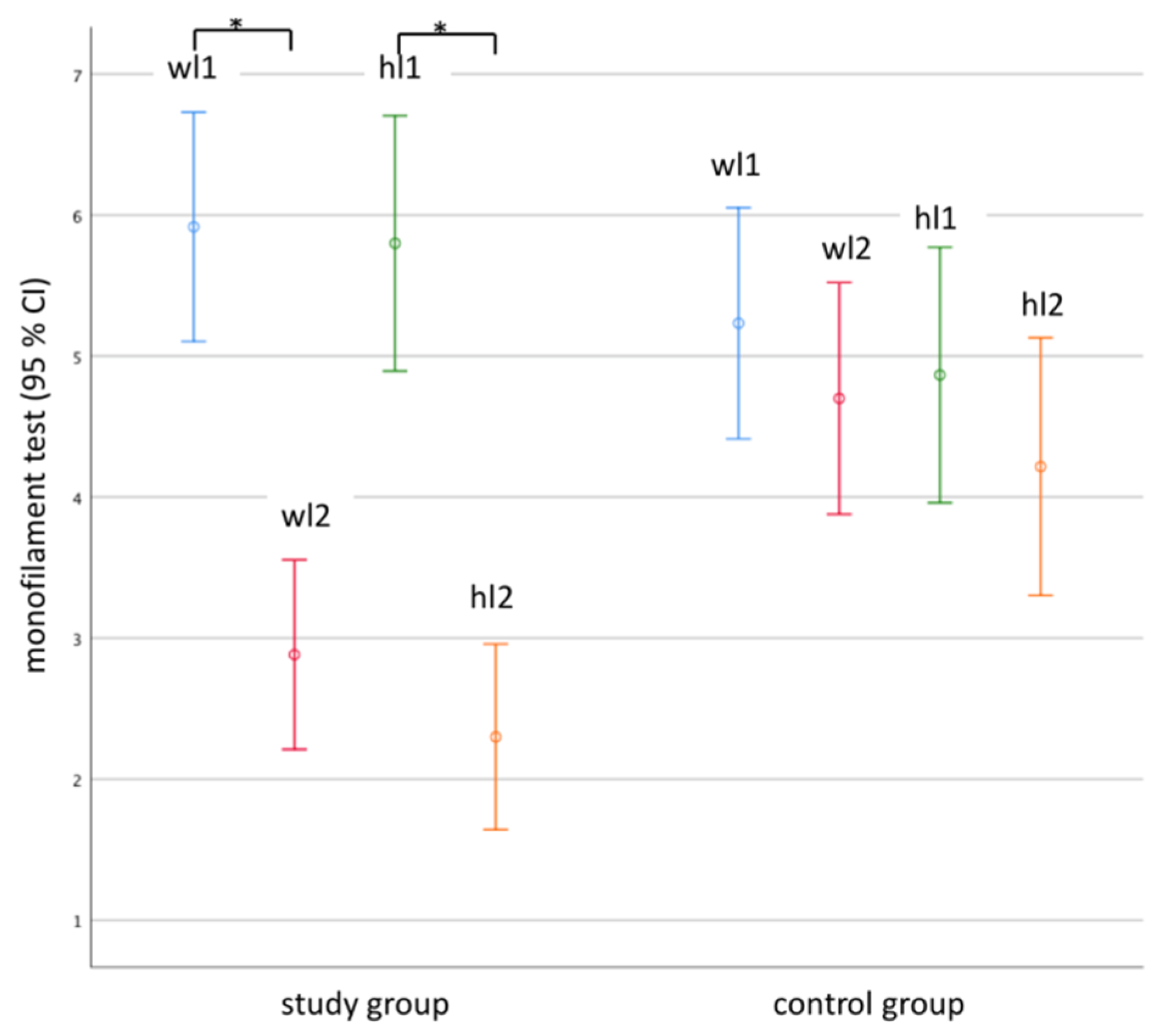
| Monofilament test score | 11.700 ± 4.417 | 5.183 ± 3.244 | 10.083 ± 3.618 | 8.917 ± 4.027 |
| p monofilament ab < 0.001 | p monofilament cd = 0.484 | |||
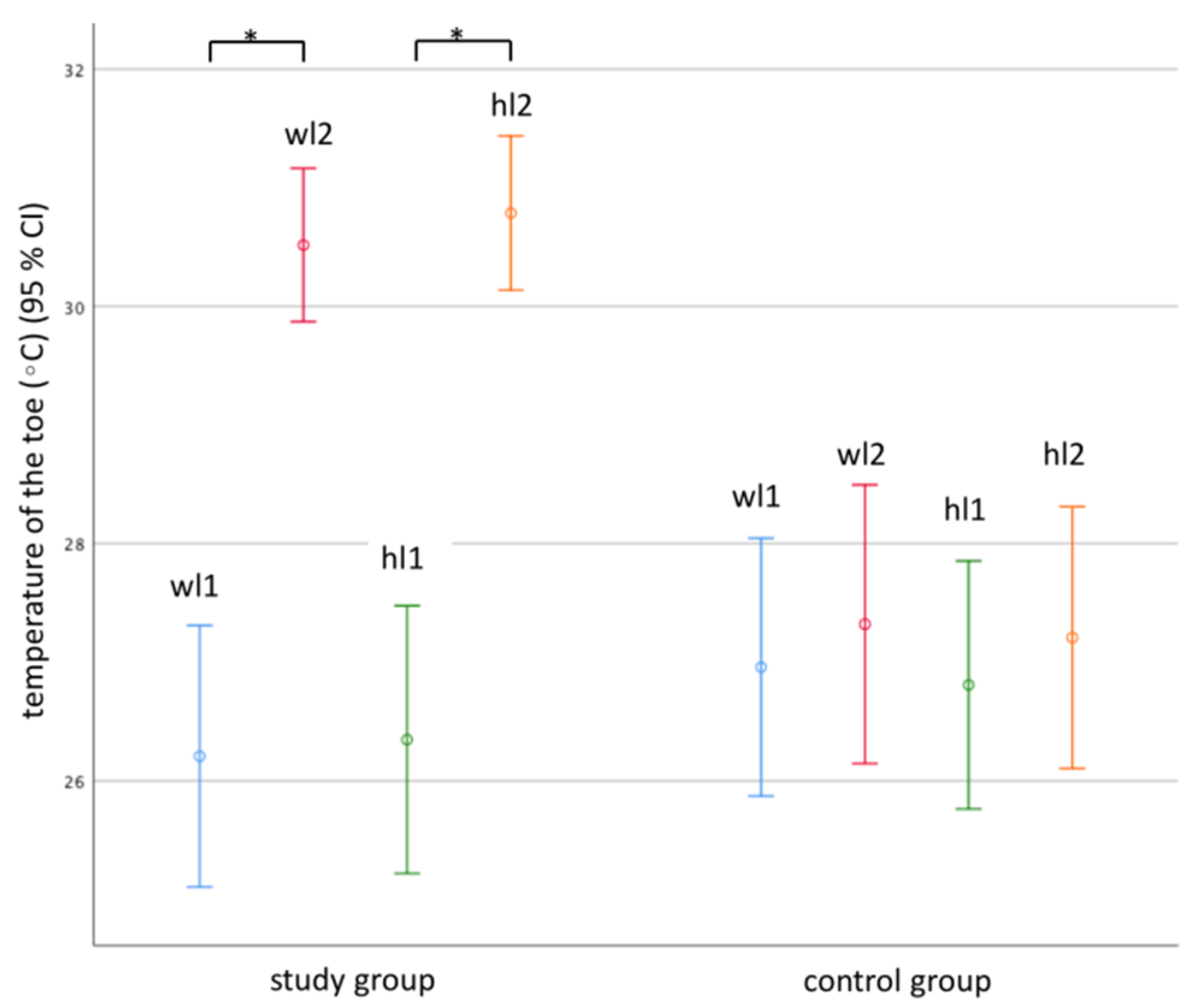
| Temperature in °C on the big toe | 26.277 ± 2.875 | 30.651 ± 1.611 | 26.882 ± 2.828 | 27.263 ± 2.968 |
| p temperature ab < 0.001 | p temperature cd = 0.612 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ban Frangež, H.; Rodi, Z.; Miklavčič, J.; Frangež, I. The Effect of Transcutaneous Application of Gaseous CO2 on Diabetic Symmetrical Peripheral Neuropathy—A Double-Blind Randomized Clinical Trial. Appl. Sci. 2021, 11, 4911. https://doi.org/10.3390/app11114911
Ban Frangež H, Rodi Z, Miklavčič J, Frangež I. The Effect of Transcutaneous Application of Gaseous CO2 on Diabetic Symmetrical Peripheral Neuropathy—A Double-Blind Randomized Clinical Trial. Applied Sciences. 2021; 11(11):4911. https://doi.org/10.3390/app11114911
Chicago/Turabian StyleBan Frangež, Helena, Zoran Rodi, Jana Miklavčič, and Igor Frangež. 2021. "The Effect of Transcutaneous Application of Gaseous CO2 on Diabetic Symmetrical Peripheral Neuropathy—A Double-Blind Randomized Clinical Trial" Applied Sciences 11, no. 11: 4911. https://doi.org/10.3390/app11114911
APA StyleBan Frangež, H., Rodi, Z., Miklavčič, J., & Frangež, I. (2021). The Effect of Transcutaneous Application of Gaseous CO2 on Diabetic Symmetrical Peripheral Neuropathy—A Double-Blind Randomized Clinical Trial. Applied Sciences, 11(11), 4911. https://doi.org/10.3390/app11114911