1. Introduction
Diabetes mellitus (DM) is a metabolic disease caused by the disruption of the glucose metabolism in the body [
1]. DM can cause changes in skin homeostasis resulting in changes in metabolism and several complications, such as vasculopathy and neuropathy [
2]. Diabetes is usually accompanied by the emergence of foot ulcer disease or gangrene, palpable femoral and popliteal pulses, and the absence of foot pulses [
3]. Foot ulcer disease and gangrene are cases of disease that often occur in people with DM and usually begin with the appearance of wounds. In general, there are many ways to treat open wounds in diabetic patients: one of them being the use of ointments as topical medication. Agrawal et al. (2014) reported that wounds can be healed using antibiotics, either used topically, directly on the wound, or orally [
4]. Diabetic wound healing can be disrupted if the patient has poor blood sugar control and therapy, as well as the presence of bacteria on the wound surface that causes infection [
5]. In fact, the problems that occur during the wound-healing process make the wound worsen, e.g., by increasing the reactive oxygen species (ROS) level and oxidative stress. Both of these problems can disrupt the wound-healing process, so the healing takes longer. In normal conditions, ROS such as hydrogen peroxide (H
2O
2) and superoxide act as cellular messengers to stimulate wound healing [
6]. Increasing the level of ROS has a beneficial effect but, in some cases, can also cause tissue damage [
7]. When diabetic complications occur, the ROS level and oxidative stress start causing cell death and tissue damage via several mechanisms [
8]. Disproportion between antioxidants and ROS disturbed by a depletion of antioxidants or an accumulation of ROS causes oxidative stress [
9]. This situation might be resolved through the application of antioxidants. Lobo et al. (2010) reported that antioxidant molecules contribute an electron to make a free radical become neutral, thus reducing its capacity for cellular damage through their free radical scavenging property [
10].
Alginate is a natural polymer that contains β-D-mannuronic acid (M) and α-L-guluronic acid (G) blocks [
11,
12]. The main source of alginate is the various genera of brown seaweed [
12]. Alginate as a topical medicinal material has been chosen because it is considered capable in maintaining the humidity around the wound, minimizing bacterial infections, and easing the wound-healing process [
13]. Alginate has been used in several types of wounds, including pressure, diabetic, venous ulcers, and some open wounds due to its ability as a good absorbent and gel-forming agent [
14,
15].
Mangosteen rind has been a traditional medicine to treat skin trauma and infections for many decades [
16]. Several studies have reported that xanthones (such as α-mangostin) are the main compounds found in mangosteen rind. Xanthone has antibacterial, anti-inflammatory, antioxidant, anticancer, and cardioprotective activities [
17]. In the present paper, the histopathology of wound healing on a diabetic mice model by using a composite of alginate from
S. duplicatum and okra combination extracts is described. Here, we report the wound-healing and antioxidant evaluations of alginate from
S. ilicifolium and mangosteen rind combination extracts on a diabetic mice model.
2. Materials and Methods
2.1. Materials
S. ilicifolium samples were taken from Kei Island, Maluku, Indonesia in July 2018. Identification was performed at the Oceanographic Research Center, LIPI, Jakarta, Indonesia (Approval Reference Number: 1/3/18-id/2018). Mangosteen (Garcinia mangostana) was purchased from the Rungkut district (Surabaya, Indonesia). The species identification was carried out at the Biosystem Laboratory of the Department of Biology of Airlangga University.
2.2. Sodium Alginate Extraction
The S. ilicifolium was dried, cut into pieces, and grounded to powder. The dried S. ilicifolium was added in a Becker in 0.1% KOH, soaked for an hour, and filtered. Then, 1% HCl (1:30 w/v) was added to the sample and stirred for an hour, then it was filtered and washed using water until a neutral pH was reached. The sample was then soaked with 2% Na2CO3 at ±70 °C for two hours and filtered. The filtrate was added with 10% HCl to pH 2.8–3.2 or until a gel was formed and 2% Na2CO3 until neutral pH was added to the gel. Then, 4% NaOCl (1:2 v/v) was added to the mixture. The alginate extract was pipetted into 2-propanol solution in a 1:2 v/v ratio and slowly stirred until a sodium alginate fiber was formed. The sodium alginate fiber was dried and grounded to form sodium alginate powder.
2.3. Analysis of Sodium Alginate
2.3.1. Proton Nuclear Magnetic Resonance (1H NMR) Spectroscopy
1H NMR spectroscopy analyses were conducted on a JEOL JNM-ECS400A spectrometer (JEOL, Peabody, MA, USA) at a frequency of 400 MHz. D2O was used as the NMR solvent if not otherwise detailed. All samples were freeze dried before analysis.
2.3.2. Size Exclusion Chromatography with Multi-Angle Laser Light Scattering (SEC-MALLS) Analysis
The molecular weight of alginate and its classification were analyzed using the gel permeation chromatography technique by using a Shimadzu HPLC system (Shimadzu UK Limited, Milton Keynes, UK) comprising a CBM-20A Controller, LC-20AD Pump with degasser, SIL-20A Autosampler, and SPD-20A detector; HELEOS-II light-scattering and Optilab rEx refractive index detectors were provided by Wyatt. A PL aquagel-OH mixed column (7.5 × 300 mm, 8 μm particle size; Agilent Technologies, Santa Clara, CA, USA) and a PL aquagel-OH mixed guard column (7.5 × 50 mm, 8 μm particle size; Agilent Technologies, Santa Clara, CA, USA) were used as the stationary phase. The mobile phase was a 50 mM sodium nitrate solution with a flow rate of 0.5 mL/min [
11]. The alginate solution (1.5 mg mL
−1), dissolved in deionized water, was filtered through a nylon membrane (Whatman, UK) before analysis. The value of 0.165 was used as the dn dc
−1 grade [
18].
2.3.3. Thermogravimetric Analysis (TGA)
TGA was carried out on a PL Thermal Sciences STA 625 thermal analyzer (PL Thermal Science Limited, Surrey, UK). A total of 10 mg of accurately weighed sample in an aluminum sample cup was placed into the furnace with a N2 flow of 100 mL min−1 and heated from room temperature to 625 °C at a heating rate of 10 °C min−1. From the TGA profiles, the temperatures at 10% and 50% mass loss (TD10 and TD50, respectively) were analyzed afterwards.
2.4. Extraction of Mangosteen Rind
The dry mangosteen rinds were mashed into small fragments. The fragments were then macerated using 96% ethanol for three days. Samples were filtered and concentrated under vacuum. The extract was freeze dried and kept in 4 °C for the next step.
2.5. Antioxidant Assay and Analysis of Total Phenolic Content
Antioxidant assays were performed on alginate from S. ilicifolium, mangosteen rind extract, and a combination of alginate–mangosteen rind extracts by the 2,2-diphenyl-1-picryl-hydrazyl-hydrate (DPPH) free radical method. The concentration of DPPH and stock solutions were 50.0 and 1000.0 μg/mL, respectively. The extracts were diluted in concentration variations of 200.0, 150.0, 125.0, 100.0, 75.0, 50.0, 35.0, 25.0, 15.0, 10.0, and 6.0 μg/mL of sample solution in methanol (200 μL) and 50 μL of DPPH was added into 96-well plates. Subsequently, the mixtures were incubated for 30 min in a dark chamber and the absorbance was measured at 517 nm on an ELISA plate reader.
The total phenolic content of alginate and mangosteen rind extract was determined by the colorimetric method, referring to the procedure of Malik et al. (2015) with some modifications and with gallic acid as standard [
19]. The standard solutions and samples with concentrations of 10, 20, 30, 40, and 50 ppm were added with 0.4 mL of Folin–Ciocalteau reagent. After 4–8 min, 4.0 mL of 7% Na
2CO
3 solution was added and aquabidestilata was added to 10 mL, and then it was allowed to stand for 2 h at room temperature. The absorbance of solution was analyzed at a maximum wavelength of 744.8 nm; a calibration curve was made for the relationship between the concentration of gallic acid (μg/mL) and the absorbance.
2.6. Induction of Diabetic Mice
The BALB/c strains of adult male mice (Mus musculus) were obtained from the Faculty of Pharmacy, Airlangga University, Surabaya. The mice were 3–4 months old with a weight range of 20–35 g. Ethical clearance for treating animals was obtained from the Faculty of Veterinary Medicine, Airlangga University, Surabaya, Indonesia with License Reference Number: 2. KE. 049.04.2019.
The mice were treated in a 12 h light and 12 h dark lighting system for a couple of weeks. During acclimatization for the experiment, the mice were fed (oral dose of 0.3 mL) with lard three times per week during 3 weeks in order to achieve a high fat diet. Streptozotocin (STZ) was injected for 8 days by using the 30 mg/kg body weight using multiple low dose method of 0.15 mL intraperitoneally (i.p) to induce type II diabetes mellitus [
20]. The mice were weighed before and after treatment. The level of blood glucose was measured after STZ induction at 3, 7, and 14 days of treatment.
2.7. Animal Grouping and Treatment
The group of mice (12 groups) were separated: (a) three groups for no treatment as normal (N) and (b) nine diabetic groups for treatment (D), consisting of three mice in each group for 3, 7, and 14 days of treatment [
20]. The nine treatment groups were classified into three categories: (1) three groups for diabetic control (DC3, DC7, and DC14); (2) three groups for alginate treatment (DA3, DA7, and DA14); and (3) three groups for alginate–mangosteen rind extract treatment (DAM3, DAM7, and DAM14). A centimeter wound on the mice’s
glutea (buttocks) was generated. Each group was smeared with Vaseline (untreated and DC), vaseline–alginate (DA), and vaseline–alginate–mangosteen rind extract ointments (DAM). A single dose of 50 mg/kg body weight ointment was generated for treatment. The animal number replication was referred to the Federer formula (1967) [
21].
2.8. Histopathology Analysis of Wound Healing
The histopathology experiments of wound healing were conducted at the Pathology Laboratory of the Faculty of Veterinary Medicine, Airlangga University. A microscope at 400 times magnification was used for the observation of fibroblasts, fibrocytes, macrophages, neutrophils, and collagen density. The width of the wound was analyzed using 40 times magnification under an optical microscope.
2.9. Statistical Analysis
The wound-healing measurements are illustrated as a mean ± standard error mean (SEM). The wound-healing data analysis was conducted by a normality and homogeneity test, one-way ANOVA, and Duncan test. If the results of normality and homogeneity were not qualified (α = 0.05), non-parametric tests such as the Kruskal–Wallis and Mann–Whitney tests were applied. All the statistical analyses were calculated using an IBM with SPSS 20.0 software.
4. Discussion
Sodium alginate was extracted from
S. ilicifolium to give a pale-yellow solid with a 14.36% yield. The obtained yield is very similar to the one reported by Latifi et al. (2015), who reported yields ranging from 12% to 16.5% [
28]. Davis et al. (2004) extracted
S. fluitans and
S. oligocystum using high temperature and base conditions to obtain 21.1–22.8% and 18.9–20.5% yields, respectively [
29]. Mushollaeni (2011) reported that alginate from several species of
Sargassum sp. had 16.93 to 30.50% yields [
30]. Based on this study, the yield of the extracted alginate not only depends on the extraction method and the
Sargassum species used but also on the seasonal variation. It is in fact well known that there are marked seasonal variations of polysaccharide contents in seaweeds, as polysaccharides are stored in winter as a food source and therefore a harvest at the end of summer will give higher polysaccharide levels than in the spring.
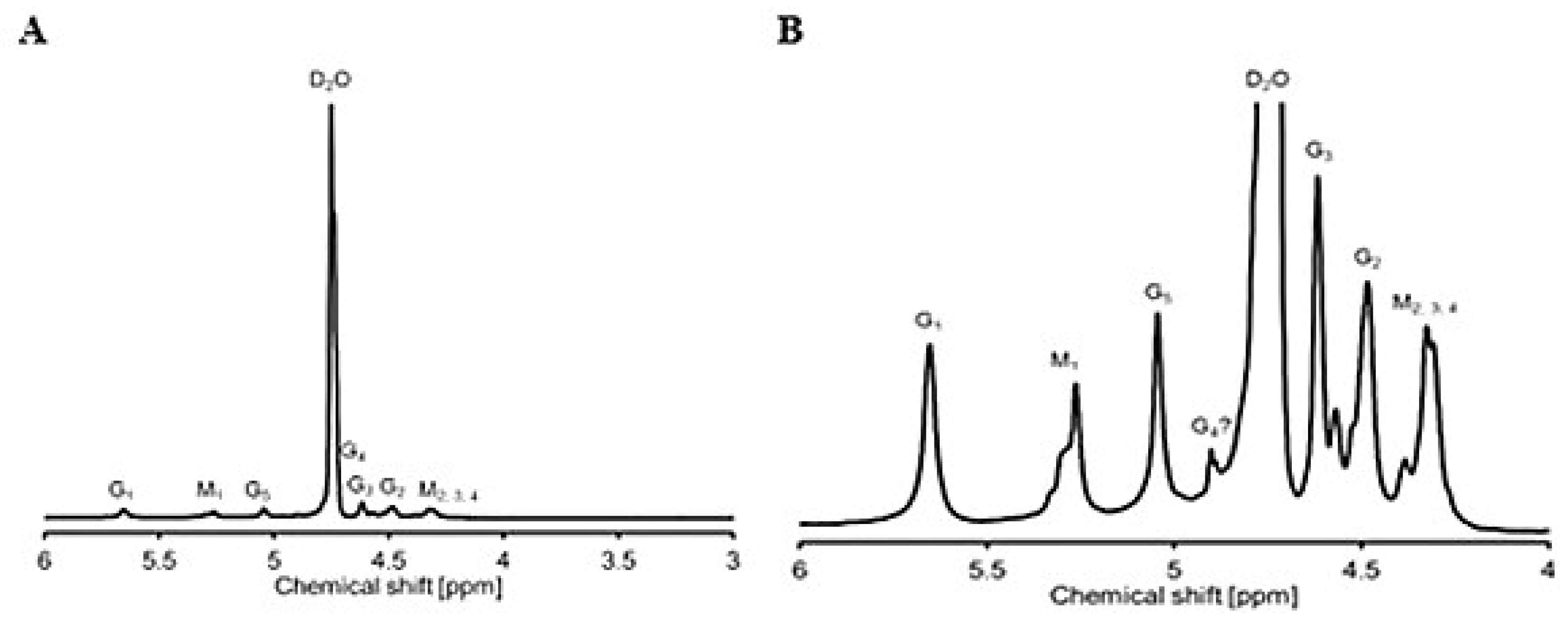
The
1H NMR analysis of
S. ilicifolium alginate showed that the signals in the range 4–4.8 ppm belong to protons from the β-glycosidic bond, whereas the signals between 5.1 and 5.8 ppm are resonances of protons from the α-glycosidic bond. The identification was performed by comparison with the
1H NMR spectrum of alginate from Llanes et al. (1997) [
31]. The structure of alginate from
S. ilicifolium consists of β-D-mannuronic acid (4.3–4.8 ppm) and α-L-guluronic acid (5.1–5.8 ppm). The M/G ratio of alginate was determined by the integration of each proton with their monomers. The M/G ratio of alginate was 0.77, indicating that
S. ilicifolium alginate has a higher guluronic acid monomer than mannuronic acid. The protons G
1 and M
1 are the most de-shielded protons (δ 5.1–5.8 and 5.1–5.5, respectively). M
1 is more shielded than G
1, because G
1 is located at an equatorial position in comparison to an axial one in M
1. In fact, Llanes et al. performed a pretreatment to partly hydrolyze the alginate before
1H NMR analysis, while in our case we decided to work with non-hydrolyzed alginate as it was fully soluble in the NMR solvent. This can be an explanation for the slightly more structured peaks and possibly also for the small shifts downfield we observed.
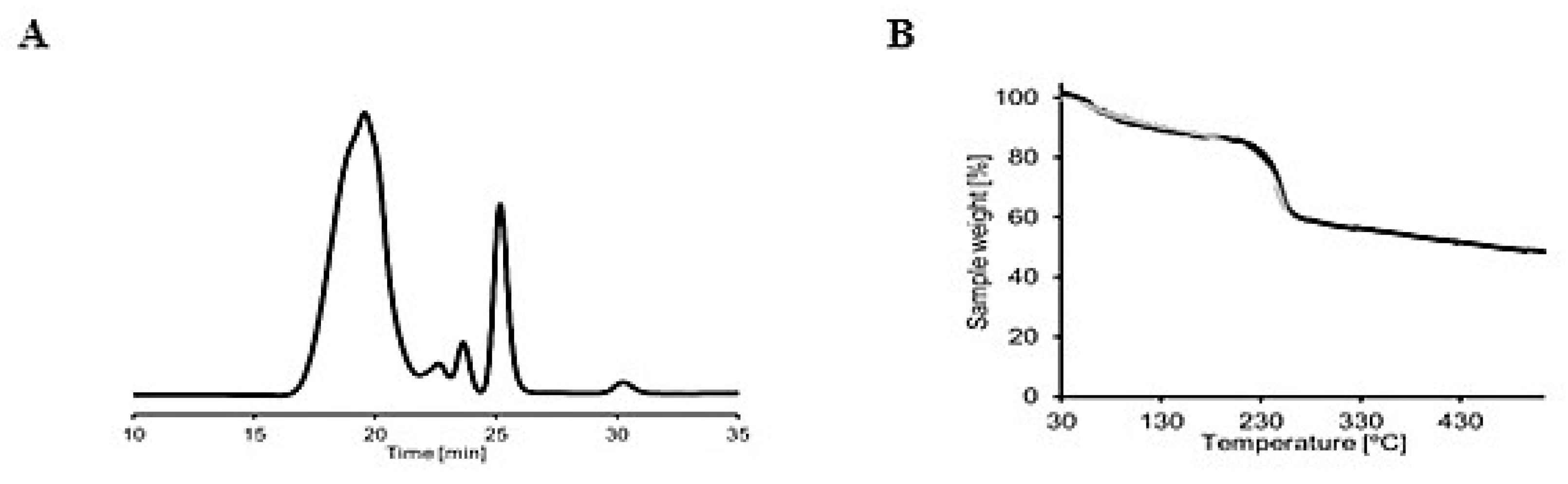
The number of M
n and M
w of alginate were 1.49 × 10
4 and 2.77 × 10
4 Dalton, respectively. Furthermore, the M
n and M
w obtained were used in the calculation of the dispersity index (Ð) using the following equation:
The dispersity index (Ð) was 1.73. The Ð value of alginate from
S. ilicifolium was below 2, indicating that the extracted alginate showed good homogeneity and was classified as chain-growth polymerization. Chain-growth polymerization is a process in which the high molecular weight polymer is generated at the beginning of the polymerization process and the polymer yield (the percentage conversion of the monomer into the polymer) gradually increases with time [
32]. Based on TGA, alginate from
S. ilicifolium had a single-stage decomposition curve (
Figure 2B).
The antioxidant assay showed that the IC
50 of alginate, mangosteen rind, and alginate–mangosteen rind extract combination was 297.60, 29.60, and 52.0 µg/mL, respectively. The results indicated that alginate was a weak antioxidant and mangosteen rind was a powerful antioxidant, and when combined they produced a material with excellent antioxidant properties. These observations could be linked to the fact that mangosteen rind contains xanthones, such as α-mangostin and γ-mangostin, which have been reported to exhibit anti-inflammatory, antioxidant, and radical scavenging activity [
33,
34,
35]. According to Thong et al. (2015), xanthones can capture free radicals in two ways: through hydrogen atom transfer (HAT) to explain the antioxidant activity in the gas phase and the single electron transfer–proton transfer (SETPT) mechanism that is thermodynamically favored in water [
36]. Strong antioxidant activity observed in the combination of alginate and mangosteen rind extract could possibly overcome ROS that occur in hyperglycemic conditions, thus enhancing wound repair in diabetic mice.
The total phenolic content in mangosteen rind extract tends to be low due to several factors, such as the type of mangosteen fruit, storage time, and the hardness of the rind. According to Dangcham et al. (2008), the total phenolic content of mangosteen fruit will decrease throughout the storage time [
37]. Another study reported that the lignin content and density of the damaged pericarp tissue would increase as a result of the hardening of the fruit skin, while the total phenolic content decreased [
38]. Mangosteen rind is an essential, natural phenolic antioxidant source; at least ten phenolic acids have been characterized in mangosteen rind [
39,
40]. Mangosteen rind contains bioactive substances, such as phenolic acids, flavonoids, anthocyanins, proanthocyanidins, (-)-epicatechin, and xanthones, which have biological, medical, and antioxidant properties.
The administration of lard can significantly increase the body weight of mice. This condition indicated increasing hyperglycemia and insulin resistance, and it will cause type II DM [
20]. Husen et al. (2019) reported that obesity caused by excessive fat accumulation can induce various chronic diseases and complications such as diabetes mellitus [
23]. The administration of STZ was performed to increase the condition of hyperglycemia (increased blood sugar level) [
20]. The increase of blood sugar levels in three diabetic groups, namely diabetic non-treated (DC), diabetic treated with alginate ointment (DA), and diabetic treated in alginate–mangosteen rind extract ointment (DAM), of up to 250 mg/dL indicated that the mice were in a diabetic condition. Based on experiments, the combination of alginate and mangosteen rind extract proved able to reduce blood sugar levels (
Table 2). Lee et al. (2018) reported that mangosteen was able to increase insulin secretion in pancreatic B-cells and protected cells from apoptosis, due to the presence of α-mangostin in mangosteen fruit [
41]. Jariyapongskul et al. (2015) reported that daily α-mangostin supplementation in diabetic rats shows remarkable hypoglycemic and insulinotropic effects, a reduction in plasma glycated hemoglobin, and a decrease in serum triglycerides and cholesterol [
42].
It was expected that the administration of a topical combination of alginate and mangosteen rind extract in diabetic wounds could reduce blood sugar levels by entering the systemic circulation through the bloodstream. The entry of compounds found in topical drugs through the bloodstream can enhance the host insulin level and the sensitivity of somatic cells [
43]. Therefore, the topical combination of alginate and mangosteen rind extract can be classified as diadermic ointment. A diadermic ointment is a drug that is able to enter the deepest skin tissue and enter the systemic circulation [
44]. However, further investigation is required to confirm whether the compounds responsible for reducing the blood sugar levels are a combination of alginate and mangosteen rind extract or the presence of other active compounds that have not been separated from the alginate during extraction given the number of weak proton signals observed in the
1HNMR. In addition, it is necessary to confirm the exact mechanism concerning how blood glucose levels can be decreased by administering a topical combination of alginate and mangosteen rind extract.
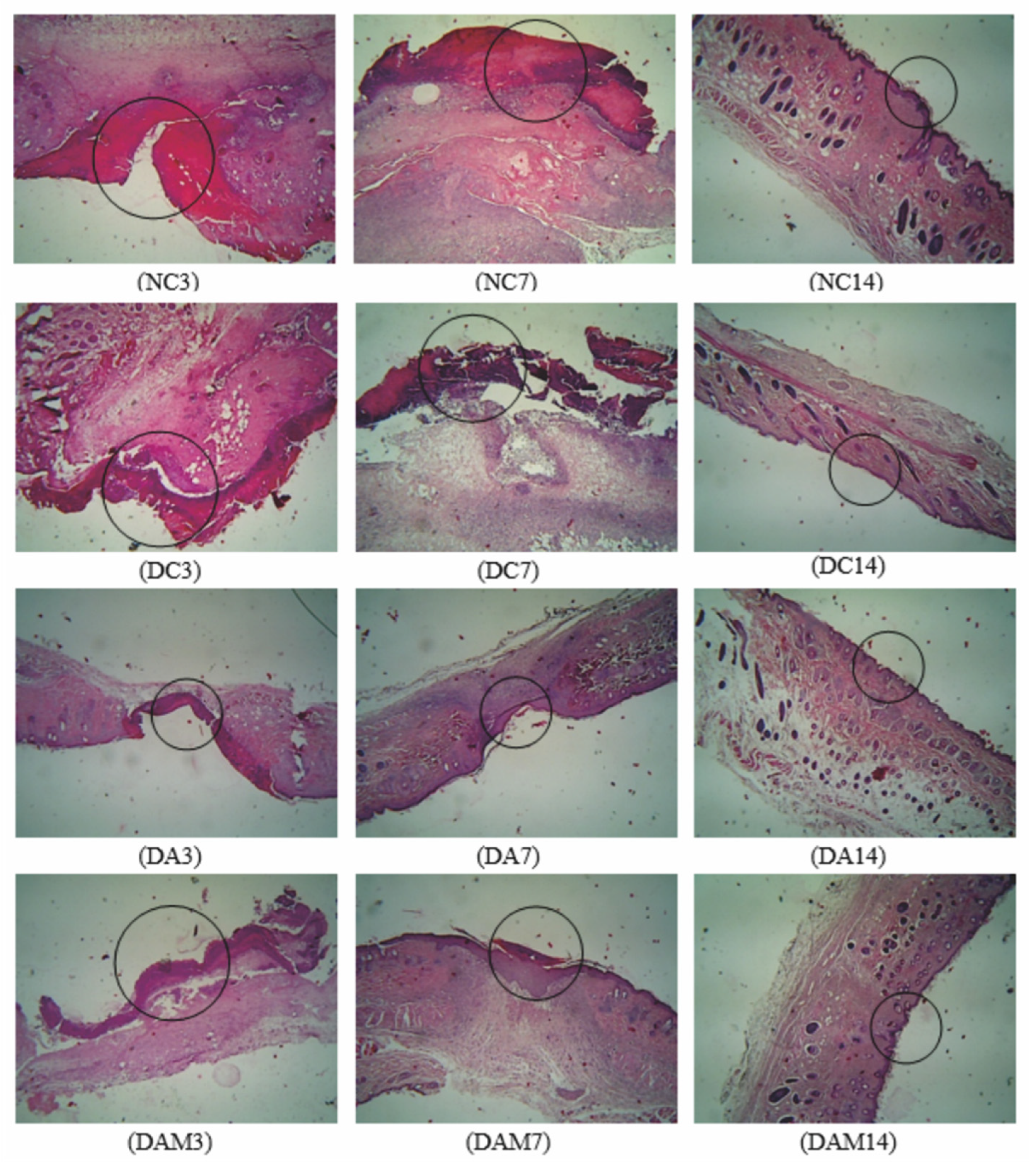
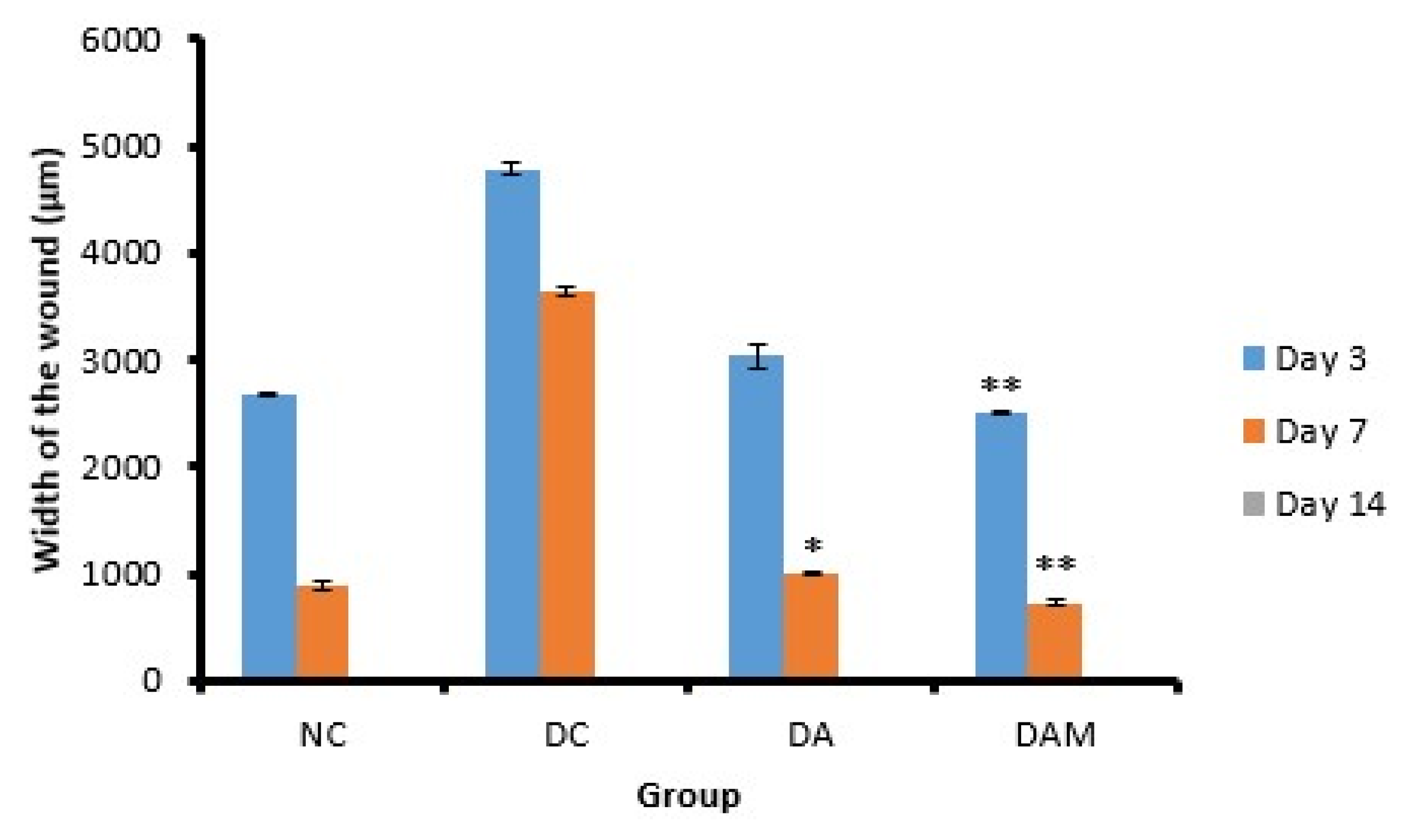
The DAM group, which was treated by alginate–mangosteen rind extract combination, showed a very significant decrease on Days 3 and 7, 2502.0 ± 10.4 and 726.0 ± 29.7, respectively, compared to other groups (
Table 3). On Day 14, all groups showed that the wound had closed. The wound width of diabetic mice in the DAM group showed the best activity when compared to the other tested conditions. This happened due to the combination of alginate and mangosteen rind extract providing strong antioxidant activity and thus decreasing ROS and increasing wound contraction and wound healing.
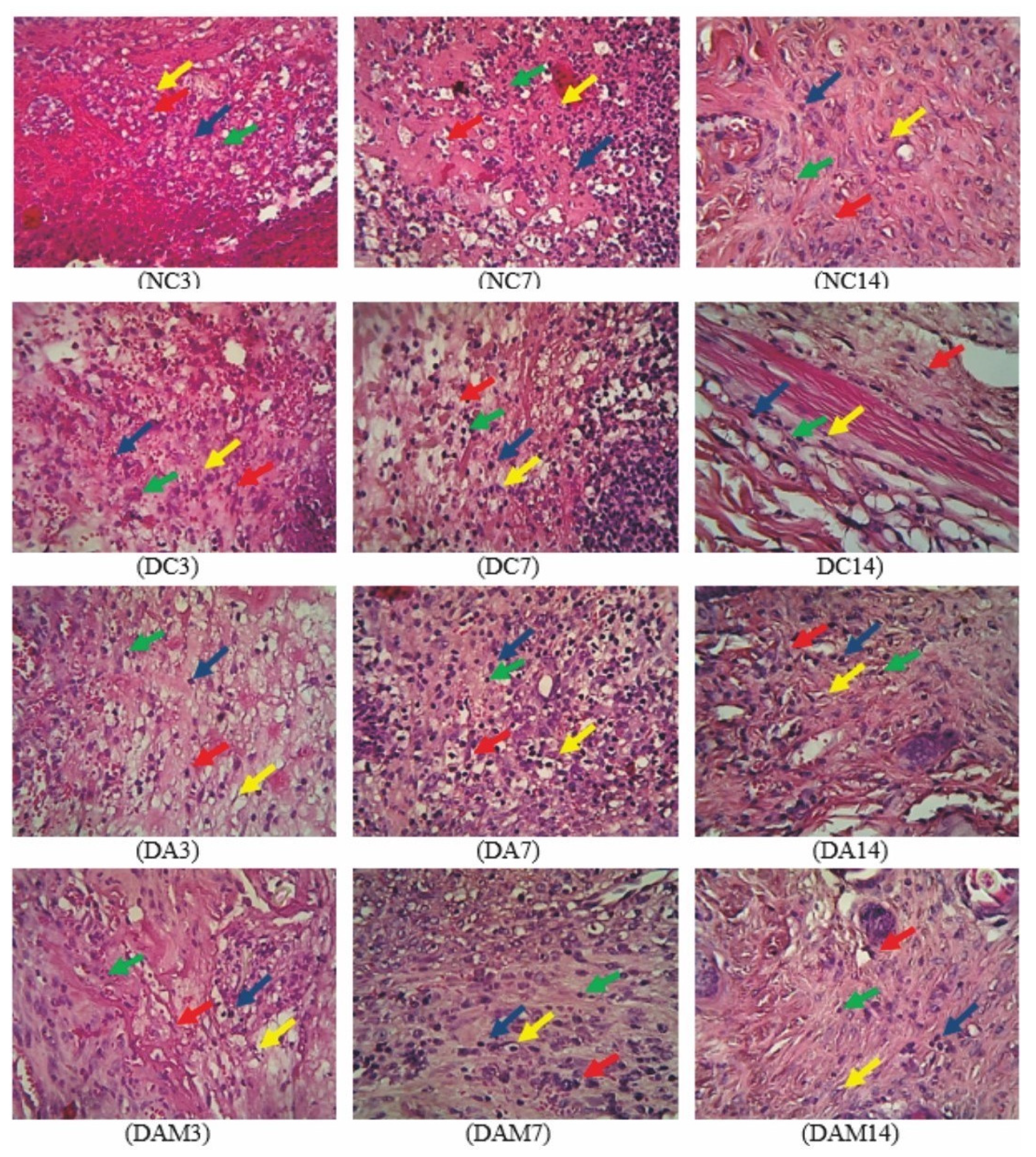
The diabetic group (DC) showed the greatest increase in the number of neutrophils in comparison to other groups. Administration of the combined alginate and mangosteen rind extracts (DAM) demonstrated that the neutrophil count in open wounds on diabetic mice increased in the first 24–48 h and then decreased until Day 14 (55.0 ± 0.9 on Day 3 to 14.0 ± 0.2 cells/mm² on Day 14), thus indicating that DAM could ease the process of wound healing (
Table 4). The decrease in the neutrophil count in the DAM group occurred due to the presence of phenolic compounds from the mangosteen rind extract that acted as antioxidants. Phenolic compounds are able to reduce the secretion of human neutrophil elastase (HNE), which is an enzyme that can break down the components of the extracellular matrix by reducing the number of neutrophils [
45].
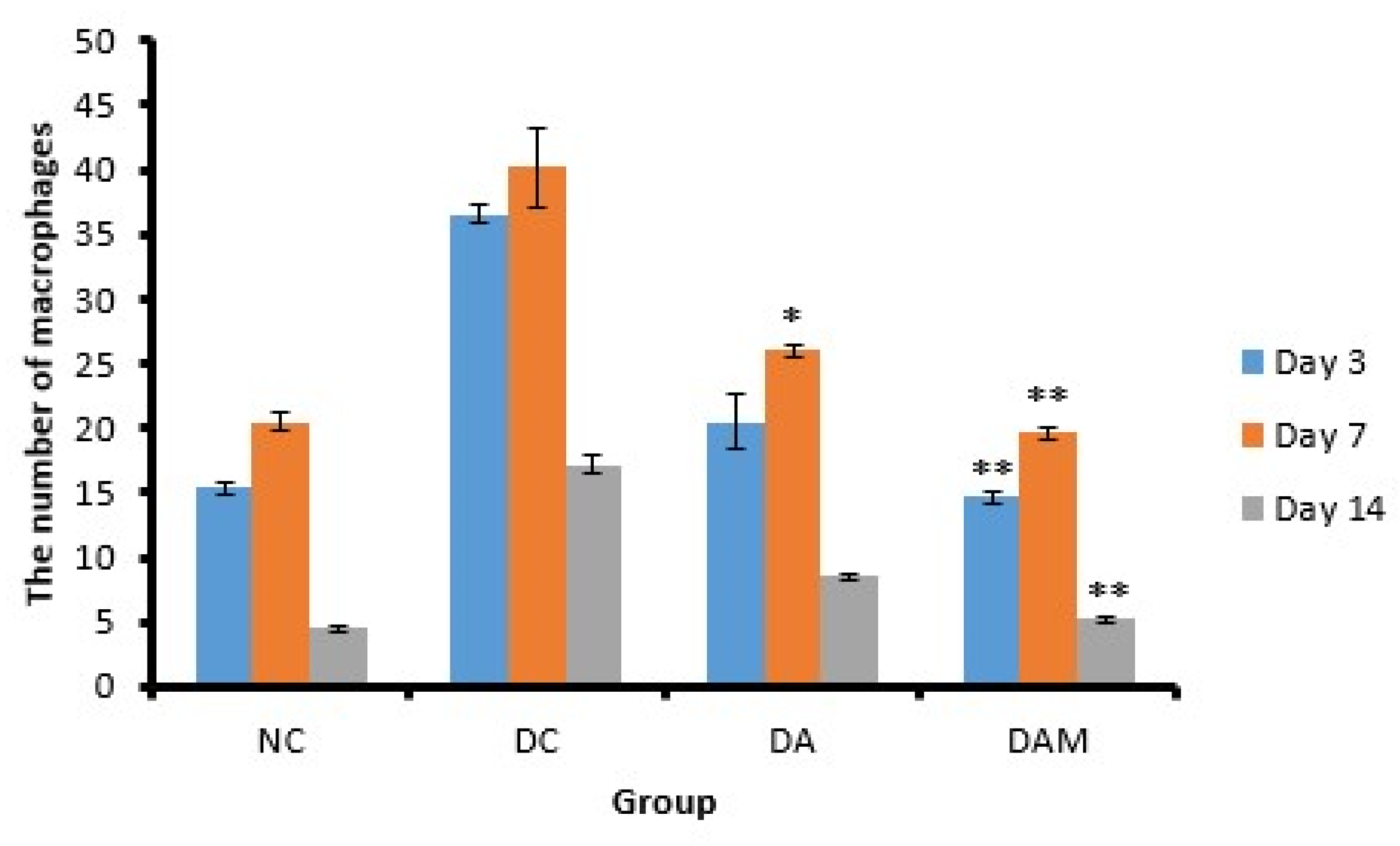
The macrophage count in the DC group showed a slight decrease on Day 14 compared to the other groups, thus implying that the inflammation phase in the open wounds of diabetic mice occurred for a longer duration than the normal group. Persistent inflammatory conditions inhibit wound healing [
46]. The presence of hyperglycemia and oxidative stress (increased blood sugar levels and ROS) can affect the modulation and polarization of macrophages, which could inhibit the healing process [
27,
47]. Therefore, the administration of alginate and mangosteen rind extracts to diabetic wounds could reduce the number of macrophages in the wound almost as well as non-diabetic wounds (
Table 5).
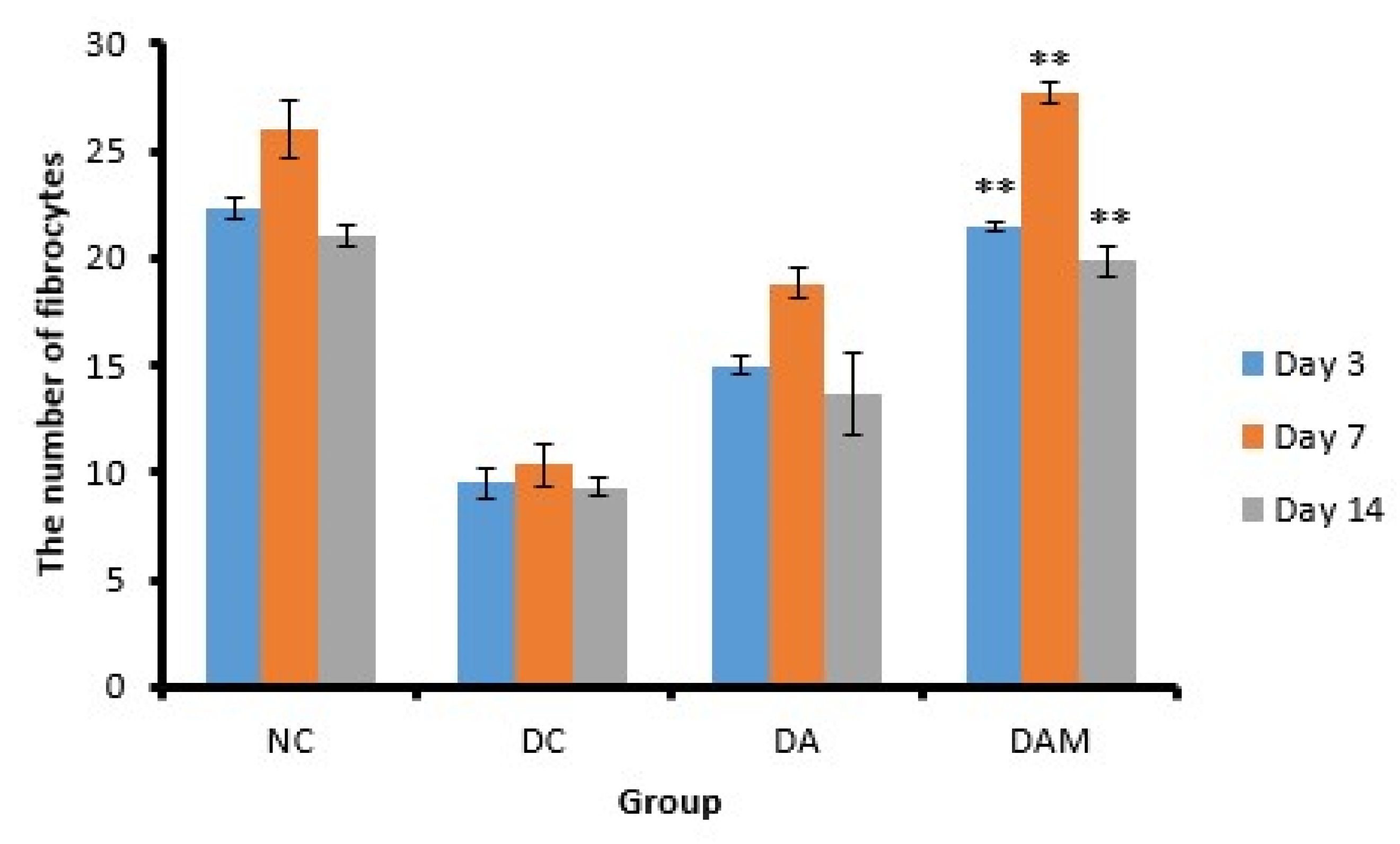
An increase in the fibrocyte count leads to an increase in collagen V production, while lowering collagen I, III, and IV levels [
48]. Fibrocyte differentiation can reduce inflammatory conditions and tissue damage as well as improve the wound-healing and tissue-remodeling process. The number of fibrocytes will increase with the increasing age of the wound, and more than 15 fibrocytes indicated the age of the wound was between 9 and 14 days [
27]. The administration of a topical combination of alginate and mangosteen rind extract in the DAM group can increase the number of fibrocyte cells in diabetic open wounds between Day 3 and Day 7, thus accelerating the process of angiogenesis. On the other hand, the fibrocyte count decreased by Day 14, as shown in
Table 6; this condition indicated the wound had healed.
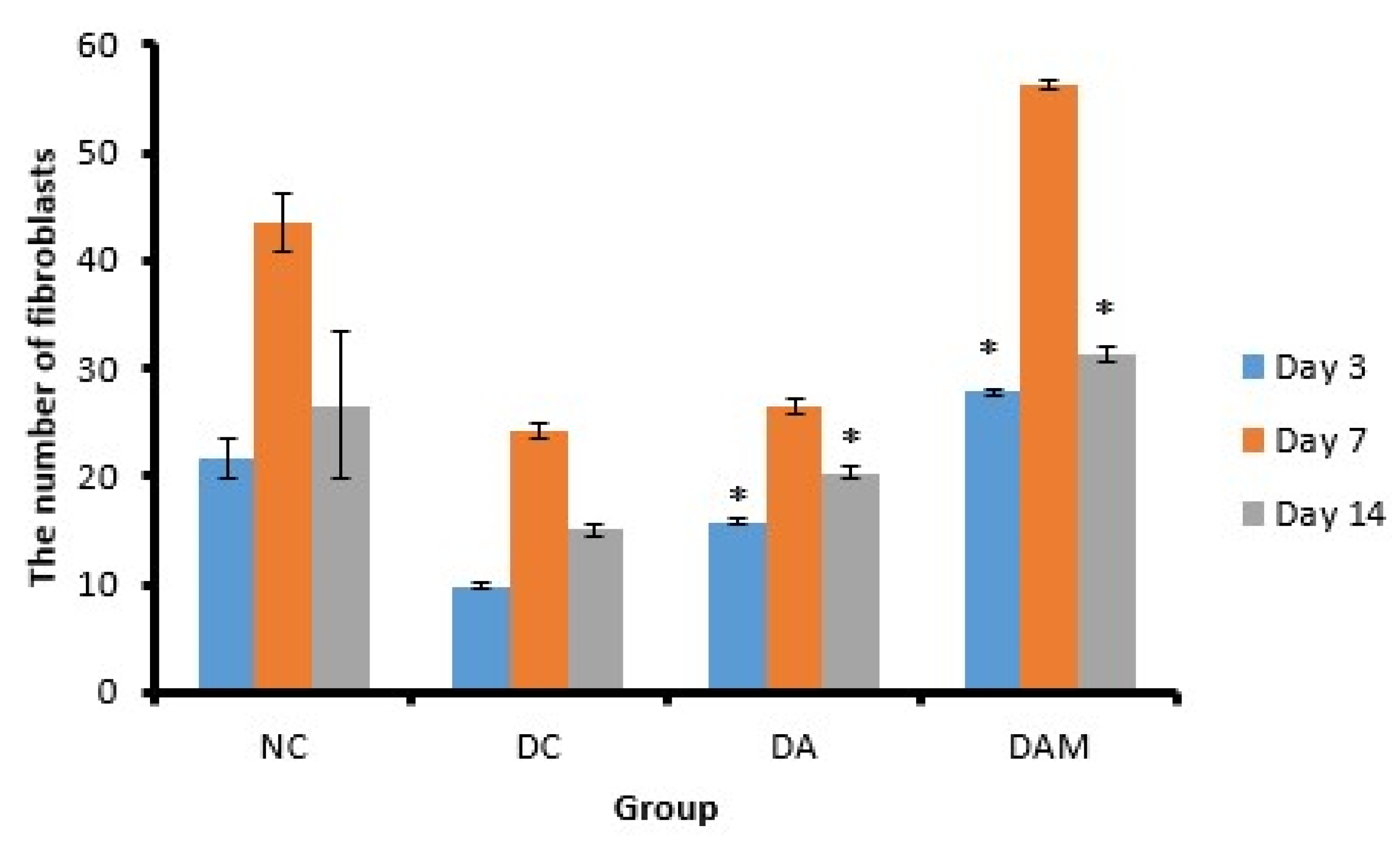
Fibroblasts are cells that have a role in the proliferation phase. These cells have the function to regulate collagen, glycosaminoglycan, proteoglycan, fibronectin, and elastin as the extracellular matrix components [
49,
50]. In addition, fibroblasts also play a role in collagen. The presence of an increase and decrease in the number of fibroblasts is the same as observed in the measurement of the number of fibrocytes in the wound. All groups showed an increase in the number of fibroblasts on Day 7 and a decline on Day 14. A decrease in the number of fibroblasts on Day 14 in all groups indicates that the healing phase is at the remodeling stage (
Table 7). The remodeling phase can be identified by decreasing proliferation and inflammation, reorganization of the extracellular matrix, and regression of newly formed capillary vessels [
51]. The fibroblast count in the DAM group was almost the same as the fibroblast count of the NC or normal group. This result indicated that the administration of alginate–mangosteen rind extract combination was effective to heal the open wound.
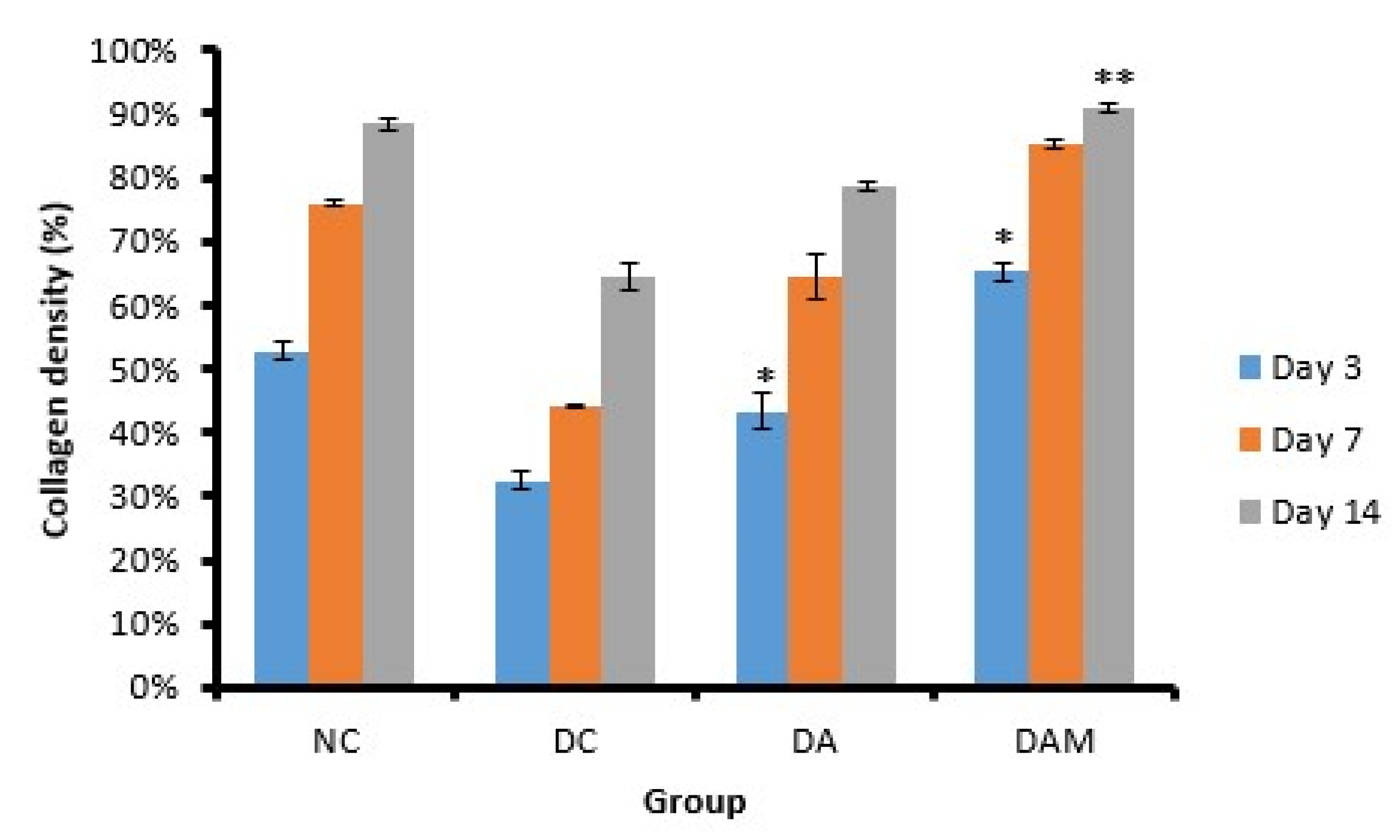
The treatment group of alginate and mangosteen rind extract of DAM showed significant results at each observation on Days 3, 7, and 14 with 65.0 ± 1.4%, 85.0 ± 0.7%, and 91.0 ± 0.7%, respectively (
Table 8). The DAM group showed the highest percentage of collagen density compared to other groups. The diabetic conditions increase the production of ROS/RNS, which decreases the collagen synthesis [
52]. An increase in the percentage of collagen density in the DAM indicated an increase in collagen synthesis.
Achievement of the wound-healing process that occurred in DAM could be due to compounds possessing antioxidant activity from the combined mangosteen peel. Moreover, Kataria et al. (2014) reported that alginate is a good absorbent and gel formation agent that has homeostatic properties [
15]. Alginate has been used in several types of wounds, including pressure wounds, diabetic wounds, and venous ulcers such as cavities and multiple bleeding sores [
14]. In addition, alginate acts as an antioxidant that can capture free radicals and absorbs wound exudate.



 ,
, 














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}