1. Annus Mirabilis
Sometimes it seems that, at certain moments, the lines of history converge in determining radical changes in scientific thought and practice. The year 1882 was certainly one of these for the history of infectious diseases. On March 24 of that year, Robert Koch announced the isolation and identification of
Mycobacterium tuberculosis as the causative agent of tuberculosis. The session of the Berlin Physiological Society, during which the German medical doctor gave the report on the discovery of this new microorganism, was one of the most dramatic moments in the history of medicine: finally, the elusive nature of one of the main 19
th-century scourges found a unitary etiological explanation. Paul Ehrlich (who would be awarded the Nobel Prize for medicine in 1908), present at the time of the conference, always remembered that evening as “the most important scientific experience of my life” [
1]. Against all those who still rejected the contagious nature of tuberculosis, invoking constitutional, degenerative, food or toxic explanations, Koch advanced his overwhelming evidence. When the work was published a few weeks later, it quickly became a source of methodological inspiration for new microbiological investigations.
The year 1882 was also a milestone in the history of tuberculosis for a second important contribution, the publication of a revolutionary therapeutic proposal for the cure of pulmonary phthisis, that would have great importance until the discovery of the treatment of the disease with streptomycin: the “therapeutic” or “artificial pneumothorax” conceived by the Italian medical doctor Carlo Forlanini [
2,
3,
4,
5] in
Figure 1.
Formulated at first only as a theoretical hypothesis (one of the few cases in medicine in which the public hypothetical prediction precedes the practical realization), it would go on to become, in the hands of its proponents during the first half of the twentieth century, an invention generally applied to treat many selected cases of phthisis, the wasting disease due to tuberculosis of the lungs. The method was also destined to be depicted by an important literary figure. In Thomas Mann’s “Magic Mountain”, set in the years immediately preceding the First World War, the group of patients who underwent this treatment—which was at the time the main effective direct therapy—consider themselves as part of a special club. In Mann’s words: “They have formed a group, for of course a thing like the pneumothorax brings people together. They call themselves the Half-Lung Club” [
6,
7]. The novel by the Scottish doctor-writer Archibald Cronin, “The Citadel”, also dedicates, from a descriptive point of view, an important and precise space to the treatment with artificial pneumothorax.
The cure continued to be the primary one until the discovery of streptomycin, the first effective antibiotic therapy for tuberculosis infection, introduced in 1943 by the microbiologists Selman Abraham Waksman, Albert Schatz and Elizabeth Bugie. However, pneumothorax did not immediately disappear from the therapeutic possibilities and continued to be used until the 1970s, in those cases where the presence of large lung cavities made patients easily susceptible to stagnation of infectious processes.
2. The Path to an Invention
Born in Milan on 11 June 1847, Carlo Forlanini, as the son of a doctor, had breathed medicine since childhood. Tuberculosis was also present early in his life, because his mother was killed by pulmonary phthisis. After high school studies, Forlanini enrolled in the medical faculty of the University of Pavia in 1864 as a pupil of the prestigious Borromeo College. It was a time of great scientific and political enthusiasm because the University of Pavia was at the forefront in the applications of new theories on diseases based on Rudolf Virchow’s book “Die Cellularpathologie” and, at the same time, the young students were enthusiastic about the revolutionary movements led by Giuseppe Garibaldi, who in a few years would have brought about the unification of Italy. In 1866 Forlanini was a voluntary fighter in the Garibaldi ranks, in the battles of Monte Suello and Bezzecca. Back in Pavia he published his first scientific work in 1868 and linked himself to a fraternal friendship with Camillo Golgi, who was at the beginning of his stellar scientific career [
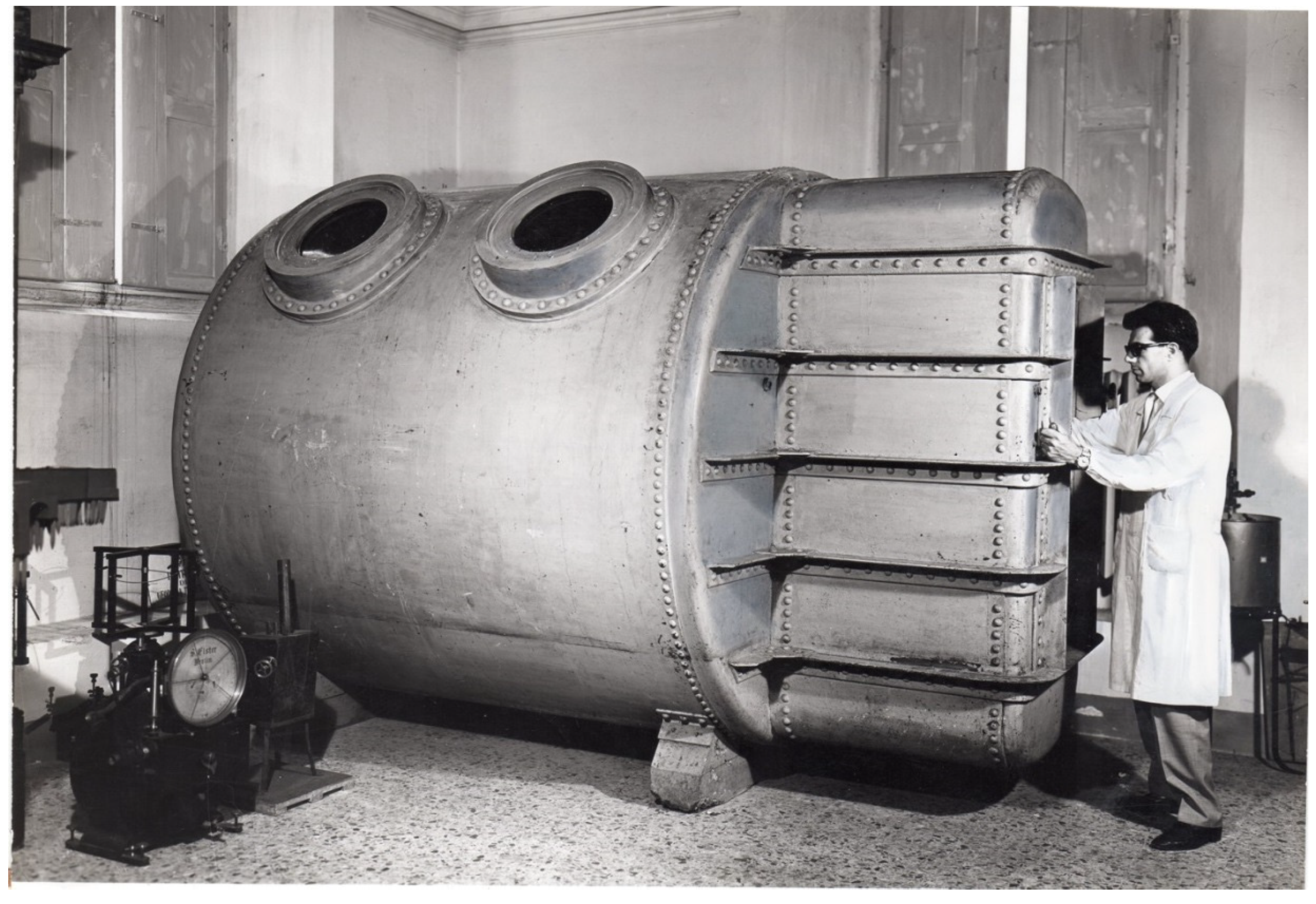
8]. In 1870 he graduated in medicine under the guidance of the ophthalmologist Antonio Quaglino; the following year, Forlanini was at work in the chronically ill division of the Ospedale Maggiore in Milan. Meanwhile, he began to develop a great interest in the study of lung diseases by starting to conceive devices that could increase lung ventilation. In these endeavors he found help from his younger brother, Enrico, a gifted engineer who was one of the pioneers of air flight (the Milan Linate airport of 1937 is named after him). In 1875, Carlo Forlanini founded the Pneumotherapy Society and the Pneumatic Institute of Milan, and from 1881, he was also chief physician for skin diseases. Meanwhile, he began a series of attempts to treat tuberculosis and lung diseases with forced respiratory movements and with aerotherapy to increase blood flow and air supply to the lung. With the scientific collaboration of his brother Enrico, he would also build some of the first hyperbaric chambers in
Figure 2.
He observed some positive results in the treatment of pulmonary emphysema and also some mild improvement in phthisis. Soon, however, Forlanini began to develop opposite therapeutic considerations for pulmonary tuberculosis. It was not the respiratory act of advantage to the sick lung, but rest. In fact, a lesion in the pulmonary tissue, as in the case of tuberculosis, could have worsened with its movements up to the formation and the subsequent development of the cavities, which then became continuously enlarged during each respiratory act. From this consideration, he was convinced that the proper therapy to stop and block the progress of pulmonary disease was to put the lungs to rest through their artificial collapse. In fact, there had already been occasional previous observations that correlated the blockage of the movement of a lung, due to a spontaneous pneumothorax, with the improvement of a tuberculous process there.
In 1822, a British doctor, James Carson, after some experiments on rats, had also made attempts to cure pulmonary tuberculosis by causing pneumothorax on humans, but the attempt had failed [
9]. However, other doctors, such as the French physicians Emile Toussaint in 1880 and Hippolyte Hérard in 1881, had reported improvement of the pulmonary tuberculosis process after lung collapse following spontaneous pneumothorax or hydro-pneumothorax [
4,
10,
11]. Forlanini’s studies on the mechanism of development of the tuberculosis process in the lung and the careful reading of previous studies, in particular Toussaint’s observations, made him think of an articulated therapeutic suggestion: to make a gas penetrate the pleural cavity (interpleural space), causing the collapse of the lung below. In July 1882, Forlanini proposed his method [
10], which he applied only in 1888 with his first intervention of artificial pneumothorax. Two years later, in an article by two of his collaborators, we find the first reference to four patients treated with the method [
12]. Forlanini’s great merit was to propose a technology through which to achieve the purpose of resting a collapsed lung, allowing the drainage and obliteration of tubercular cavity and then the scarring of the underlying lesions. The improvement of the patient became not only local, but also general, because the lung mechanical constriction of artificial pneumothorax reduced the pulmonary inflammatory source of the disease state, and perhaps could improve the body’s overall immune reaction to the pathological process. It was also proposed that the method decreased the absorption of toxic factors released by the tuberculosis lesion. Forlanini observed a reduction and disappearance of the cough; the reduction and disappearance of sputum; the fall of fever and sweating; and the disappearance of asthenia. The patient became euphoric, increased his state of nutrition and had the reduction or the disappearance of the toxic-infectious state. Forlanini also noted favorable effects on the other lung, if affected by phthisis, as a consequence of the general improvement [
13]. Finally, he argued that there was also an indirect therapeutic effect on initial laryngeal and intestinal tuberculosis.
To develop the appropriate technique for a repetitive injection of a small amount of gas into the pleural cavity (200–250 mL) through a large hypodermic needle, he asked for help and advice from his brother Enrico. Thus, medical expertise combined with the technological skills of the creative engineer, and the result was the new apparatus. At first, Forlanini made several attempts with atmospheric air, but then he realized that the oxygen component of this gas was being reabsorbed too quickly and so he switched to nitrogen [
14,
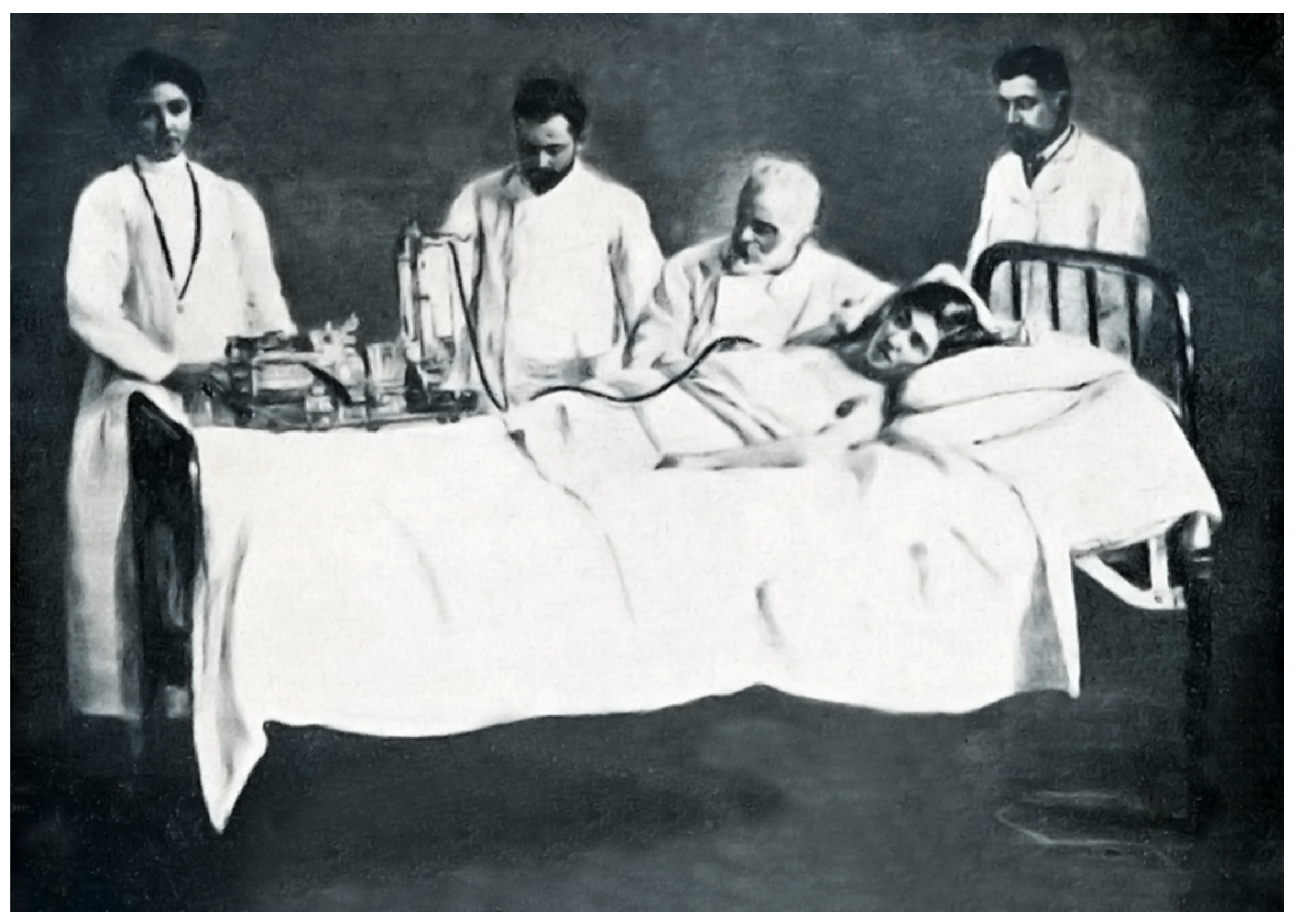
15]. In this way, the lung was immobilized for longer. To carry out the pneumothorax, Forlanini made use of two apparatuses, one for the production of nitrogen, the second for administering under pressure (controlled by a pressure gauge) the gas in the interpleural space. The production of nitrogen in the first apparatus took place through a chemical reaction by means of pyrogallic-acid which avidly absorbs the oxygen of the air. The nitrogen was then transferred to the second apparatus connected to a needle, which was introduced very slowly into the previously selected intercostal space in
Figure 3. With preliminary experiments on animals and corpses, Forlanini had come to the conclusion that, once the parietal pleura was perforated, as soon as the tip of the needle touched the visceral pleura, the underlying elastic tissue retracted, dragging the visceral pleura with it, while the gas entered the interpleural space. In this way, if the introduction was slow, the visceral pleura and the underlying lung were not pierced. Forlanini usually started the treatment by introducing around 200 cc, and never more than 400 cc (to avoid the risk of subcutaneous emphysema, i.e., the passage of gas into the tissues of the chest wall) or less than 100 cc. [
14]. After a few days, nitrogen was administered again to achieve a complete lung collapse. Then, pneumothorax was repeated every 15–20 days and continued for many months, usually up to two years or more.
3. Success and Difficulty
In 1884, Forlanini began his university career at the University of Turin and obtained the position of “extraordinarius” professor of “Clinica medica preparatoria” (preparatory medical clinic). Soon after, he reached the peak of his university career, becoming full professor of special medical pathology. Among Forlanini’s pupils at the University of Turin, the most important was Scipione Riva Rocci, who, under the supervision of the master, developed the pneumatic cuff sphygmomanometer, which soon became a worldwide symbol of practical medicine. In 1898, Forlanini returned to Pavia, first on a provisional teaching of special medical demonstrative pathology and, from 1900, in the prestigious position of full professor of medical clinic. Here a school of talented doctors gathered around him, like Riva Rocci, who moved to Pavia from Turin, Umberto Carpi De Resmini and Eugenio Morelli [
5].
Meanwhile, Forlanini made his operation known in
Figure 4 with a report held on 2 April 1894 to the eleventh international medical congress of Rome [
16] and, the following year, with a lecture to the Italian congress of internal medicine [
17]. However, the reaction by the medical community was not very lively and artificial pneumothorax also found oppositions and objections. With the spread of the operation and its application by physicians who did not know the method very well, and who used inadequate criteria for the selection of candidate patients, the number of serious and even fatal complications greatly increased [
18]. This is despite the fact that the security of the method steadily improved in the first decades of the new century. Among the complications, those reported and also discussed by Forlanini included empyema, emphysema and cerebral embolism, especially gaseous. A further complication was pleural eclampsia, i.e., a syncope whose symptoms Forlanini described in this way: “the patient falls, suddenly, in abandonment on the bed, unconscious, with his head bent to one side, or back; the eye wide open, the bulbs fixed at the front or rotated up or to one side; the pupil of maximum amplitude, rigid; the face of an extreme pallor, sometimes cyanotic, cold, with bluish streaks in the neck, chest, limbs; clenched teeth; stiff trunk and limbs; breathless and imperceptible pulse rhythm;-in short, an impressive syndrome, for the real impotence of the symptoms, for the suddenness, for the thought that the accident follows an operational act and can be fatal” [
14]. Moreover, artificial pneumothorax was sometimes ineffective due to pleural adhesions that prevented lung collapse. To overcome these difficulties, the Swedish physician Hans Christian Jacobaeus introduced the section of endopleural adhesions using a thoracoscope and a cautery [
19]. Some alternative methods to artificial pneumothorax for treatment of pulmonary tuberculosis were also developed. An attempt to put the lung at rest to limit diaphragm excursions was made in 1913 by Ernst Sauerbruch, who introduced phrenicotomy [
20]. In the years preceding the First World War, the foundations of pulmonary tuberculosis surgery were also laid. Already in 1891, Theodore Tuffier removed the pulmonary apex in a case of cavitated tuberculosis; in 1893 David Lawson introduced pneumonectomy; and two years later, William Macewen removed a left lung for tuberculosis (the patient was still alive in 1940). In 1908 Ludolph Brauer published the first radical thoracoplasty and in the following twenty years, lung surgery for pulmonary tuberculosis continuously developed [
21,
22,
23,
24]. However, artificial pneumothorax remained the first choice when an intervention to treat the disease had to be considered.
4. Disputes and Diffusion
A bad surprise caught Forlanini when, in 1906, he read an article by Ludolph Brauer of Marburg, published in an authoritative German journal, in which the invention of the method was attributed to the important American surgeon John Benjamin Murphy [
25]. The latter had developed a version of the operation, presumably without knowing the work of the Italian, and had described it in 1898 at the meeting of the American Medical Association [
26,
27,
28]. Murphy was the first to adopt the new x-ray technology (Wilhelm Roentgen had discovered x-ray in 1895) to control pneumothorax therapy results. Forlanini immediately reacted to Brauer’s article and published in another authoritative German journal the results obtained by him in 25 cases of pulmonary tuberculosis, also to claim the priority of the invention [
29]. Moreover he criticized Murphy’s treatment modalities, as they involved an incision of the skin and the chest muscles (and not a single puncture as he did) and again the large amount of nitrogen introduced (1000–3000 mL) by the American surgeon, which led to excessive compression of the lung. Forlanini’s article contributed to the diffusion of his invention in the German medical world and therefore in transalpine Europe. From this moment on, Forlanini promoted the method, also with conferences for doctors. In 1906–1907, there was a technological development that made the apparatus more applicable, when Christian Saugman, of the Vejlefjord sanatorium in Denmark, perfected it by inserting in the pneumothorax instrument a water pressure monitor, which allowed a precise control of the gas introduced. Moreover, in 1912, Maurizio Ascoli proposed a partial collapse therapy that allowed a bilateral pneumothorax to treat cases of involvement of the two lungs in the pathological process.
On April 1912, Forlanini held a memorable lecture in Rome entitled “Artificial pneumothorax in the treatment of pulmonary phthisis”, at the seventh international congress on tuberculosis [
30]. The presentation obtained a great ovation and, after thirty years of studies on pneumothorax, Forlanini at last obtained full international recognition.
In England, the method was not used before 1911; subsequently, it achieved considerable success. In 1917, the doctor Clive Riviere wrote in his textbook “The pneumothorax treatment of pulmonary tuberculosis”: “No more hopeful ray of sunshine has ever come to illuminate the dark kingdoms of disease than that introduced into the path of the consumptive through the discovery of artificial pneumothorax” [
31]. Riviere confirmed this judgment ten years later in the “British Journal of Tuberculosis” [
32]. Other British doctors expressed an overall positive opinion on the treatment [
33,
34,
35,
36,
37,
38,
39,
40,
41,
42,
43,
44,
45,
46,
47], which was also applied to children [
48]. Its level of popularization is also demonstrated by the fact that one of the important episodes in the novel “The Citadel” (1937) by the Scottish writer Archibald Joseph Cronin concerns precisely the description of an artificial pneumothorax operation. However, the spread of the method, after 1912, reached all European countries and, with some delay, also the United States. In Imperial Russia, the therapeutic pneumothorax was already used in 1910 by Arkadij N. Rubel who, two years later, published the first monograph on the topic, contributing to its knowledge in the country [
18,
49]. In the 1930s, in Stalinist Russia, the application of this method took on political connotations. The treatment was considered an “aristocratic therapy”, therefore counter-revolutionary, and in the end the pneumothorax device was attacked by propaganda as a “killing machine”. One of the leading Russian physicians advocating pneumothorax therapy, Volf S. Kholtsman, director of the Moscow Oblast Tuberculosis Institute, was arrested in 1939 during the Stalinist purges and then executed two years later.
5. The Battle and the War
In 1912, with the success at the Seventh International Congress of Rome, Forlanini became a famous scientist worldwide. In that same year he was proposed for the first time to the Nobel Prize for Medicine and, over the following years, Forlanini was unsuccessfully nominated for this award at least twenty times. His friend and fellow professor at the University of Pavia, Camillo Golgi (Nobel Prize winner for 1906), proposed him three times with the motivation that the invention of pneumothorax was “of great benefit to humanity”, a phrase that underlined the consonance of the candidate’s merits with the will of Alfred Nobel. However, the Nobel Prize was not awarded in the years of the First World War between 1915 and 1918, and in this last year Forlanini died. The Italian doctor thus had the possibility of winning the prize only in the three years between 1912 and 1914. There were, however, some reasons analyzed in detail by Hansson and Polianski [
18] that probably prevented him from being awarded in this short period of time. In fact, all the nominations came from Italian scientists; the method had not yet reached the safety standards that it would obtain a few years later; and there were other alternative surgical operations, less successful, but used in the treatment of pulmonary tuberculosis.
In 1913, Forlanini was nominated senator of the kingdom and member of the council of public education in
Figure 5. During the years of the First World War, his health gradually declined. However, he had the satisfaction of seeing his invention widely used in clinics all over the world. Forlanini died in Nervi, on the Ligurian Riviera, on 25 May 1918. Immediately after his death, Golgi published a very heartfelt obituary [
50].
This great physician won his battle against tuberculosis, the first of a series that will follow with other protagonists. His invention has not completely disappeared from medical practice and is still used in special cases, for example in pre-thoracoscopic artificial pneumothorax [
51], a fact that would have pleased Forlanini. Unfortunately, however, the war against tuberculosis is still going on and the final victory has not yet been achieved.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




