SoundFields: A Virtual Reality Game Designed to Address Auditory Hypersensitivity in Individuals with Autism Spectrum Disorder


Abstract
1. Introduction
1.1. Current Interventions for Auditory Hypersensitivity
1.2. Virtual Reality and ASD Therapy
1.3. The Use of Binaural-Based Spatial Audio
1.4. This Study
2. Materials and Methods
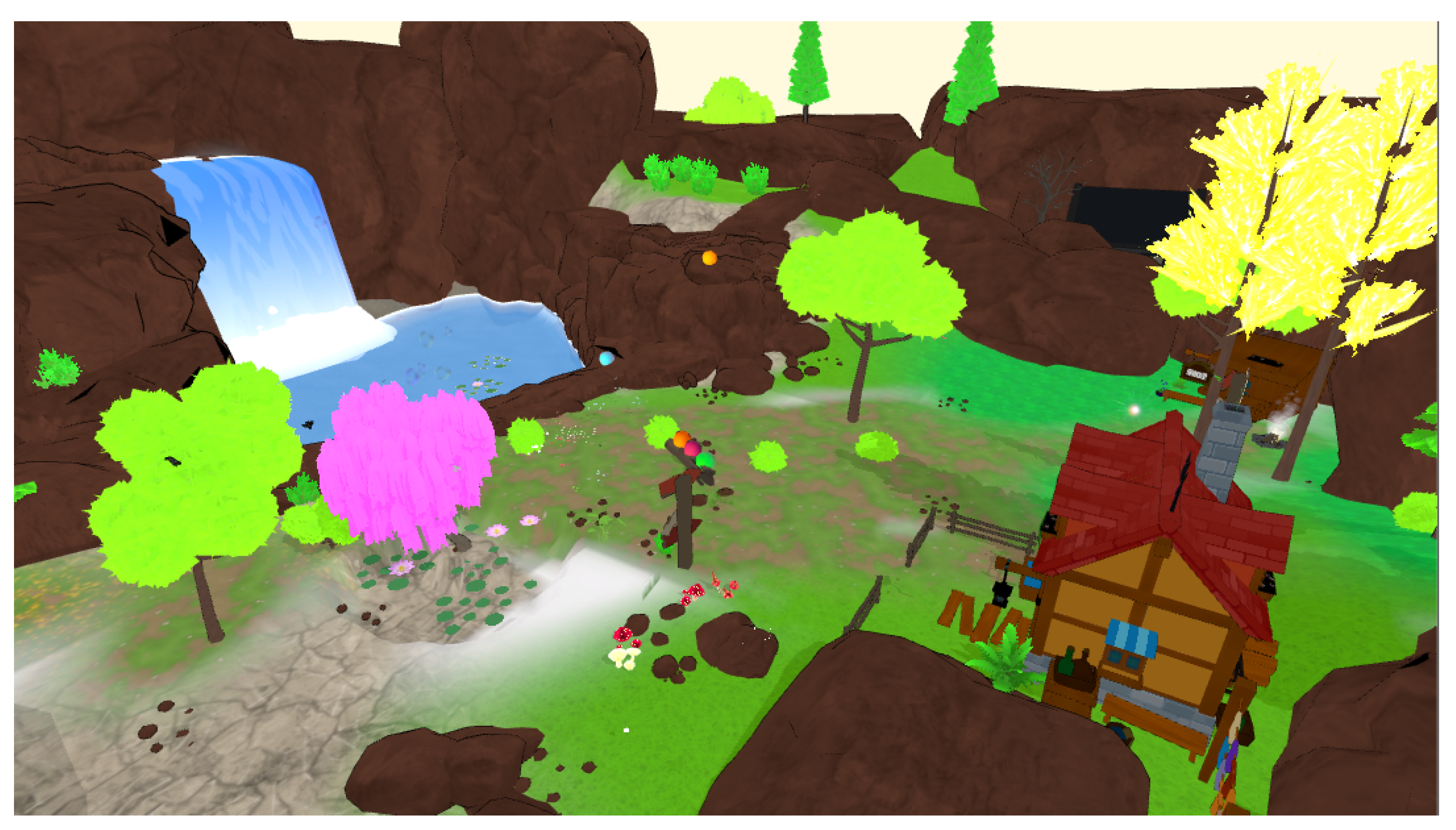
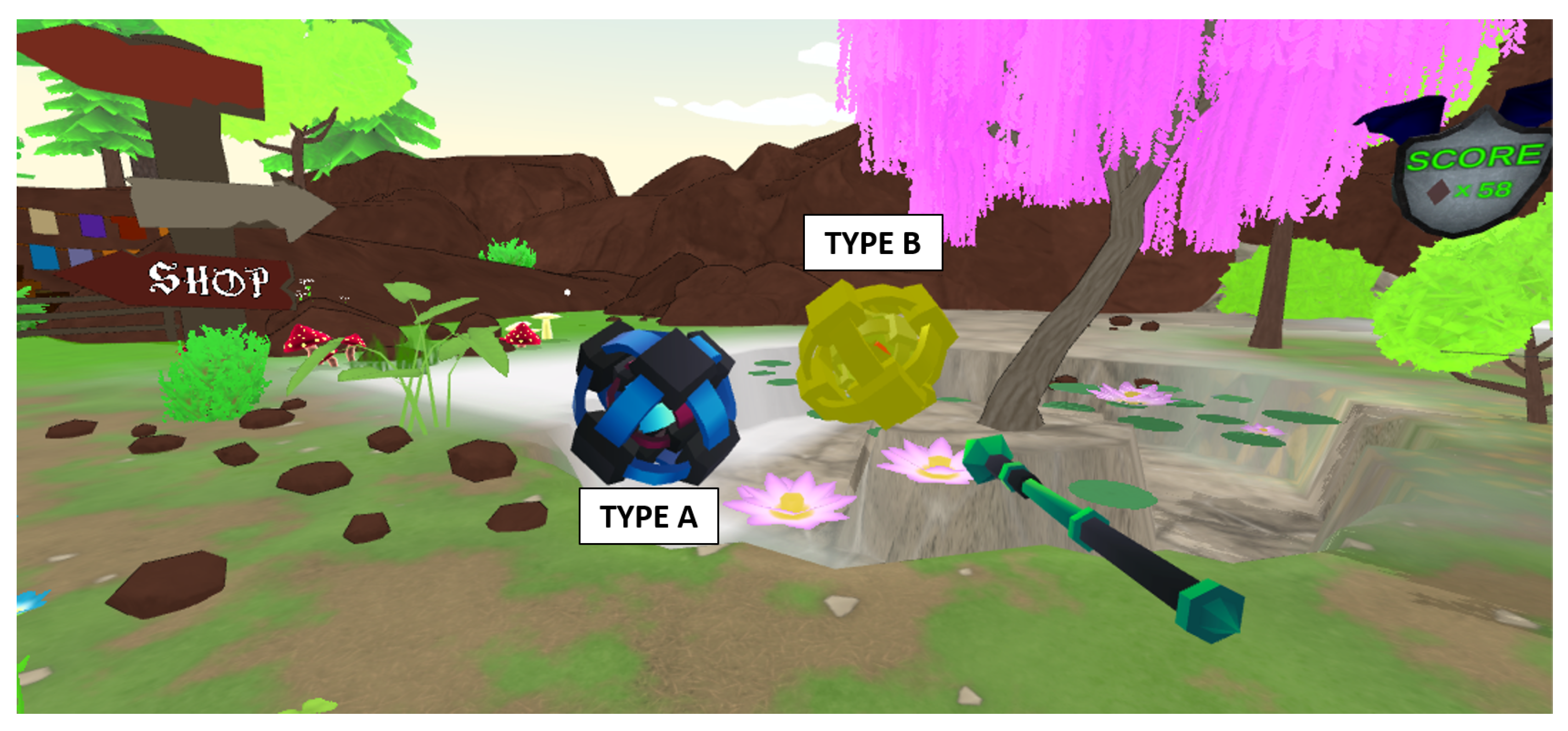
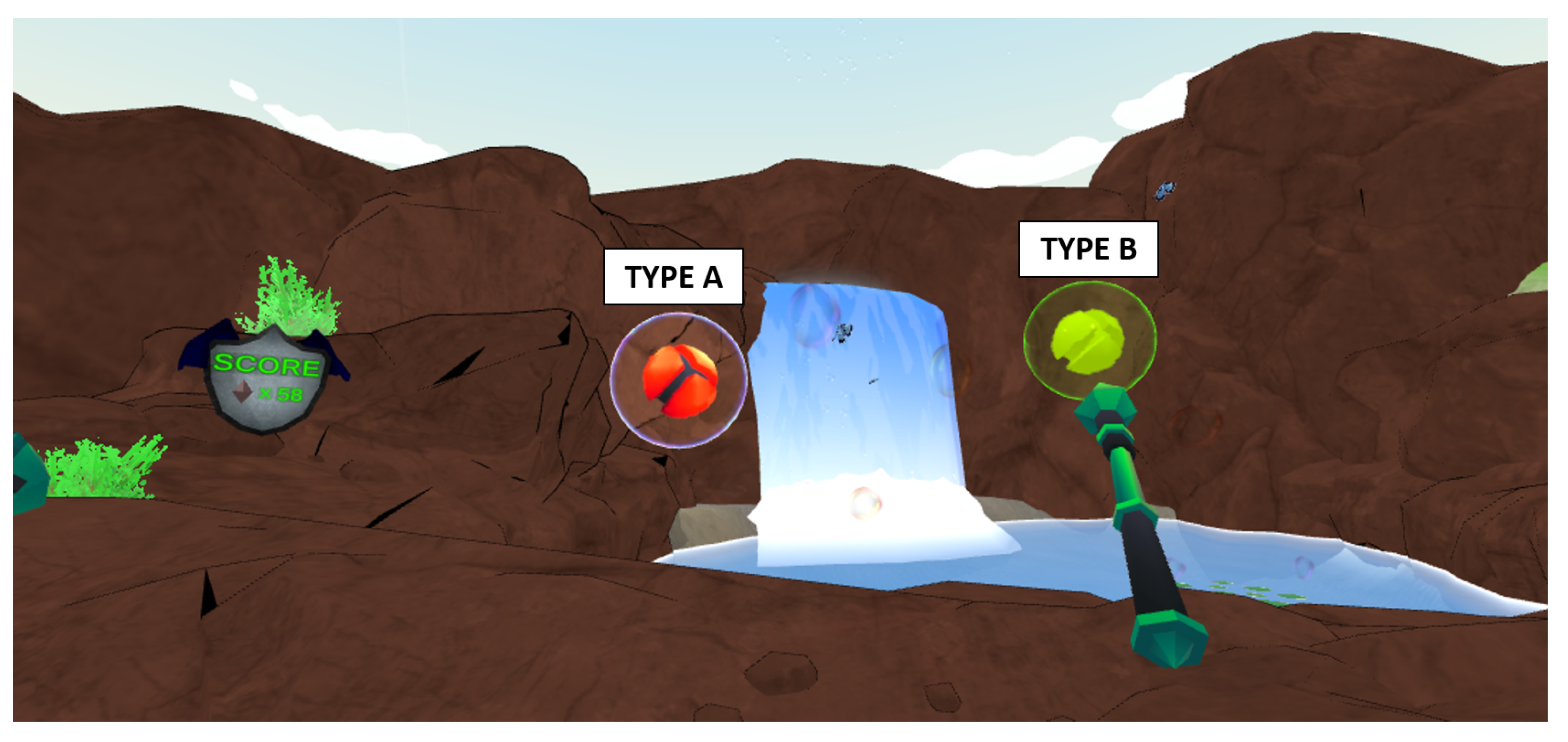
2.1. SoundFields: Game Description
2.2. Participants
2.3. Intervention Protocol
2.3.1. Baseline
2.3.2. Session Procedure
2.4. Equipment Setup
2.5. Assessments
2.5.1. Primary Outcome
2.5.2. Secondary Outcome
3. Results
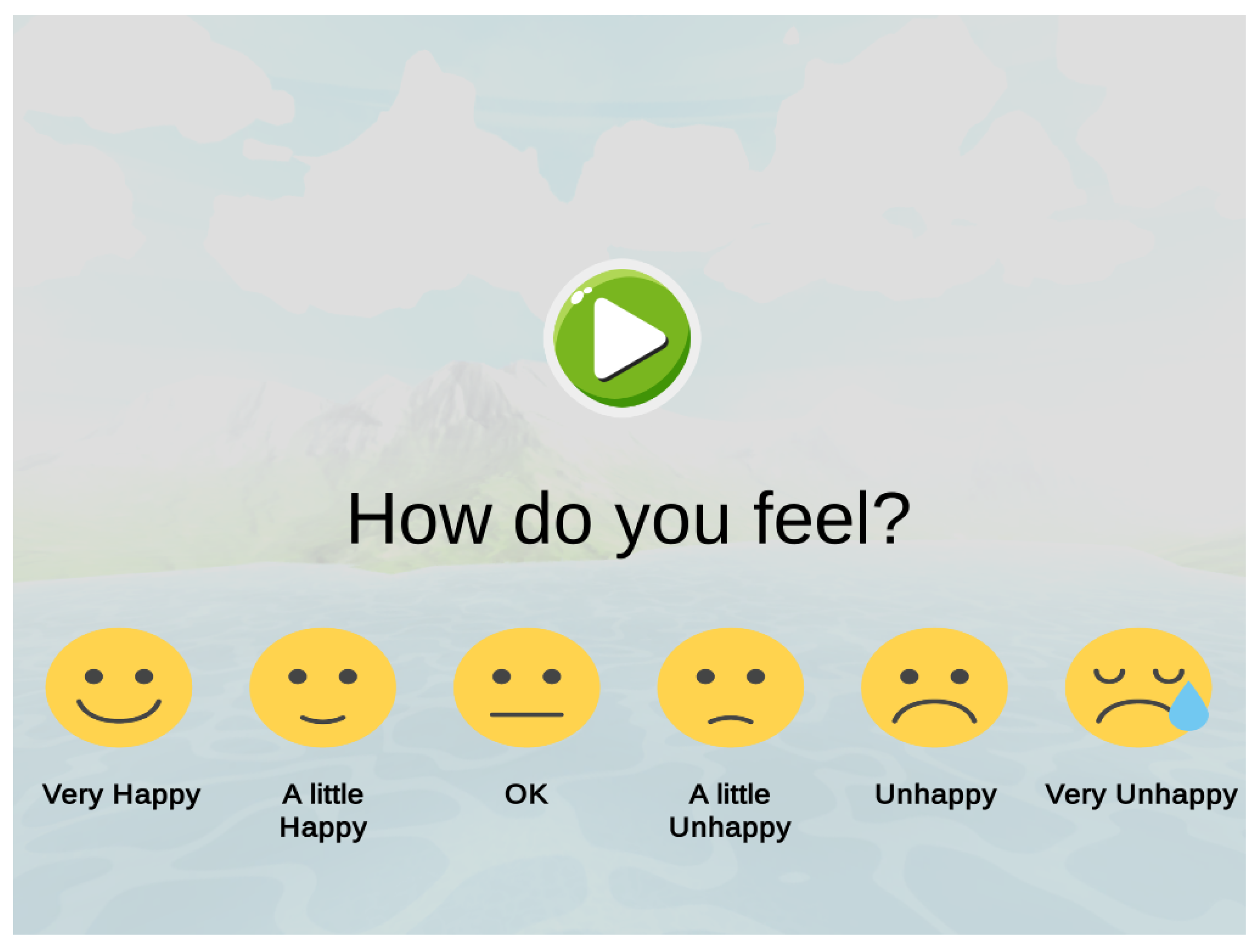
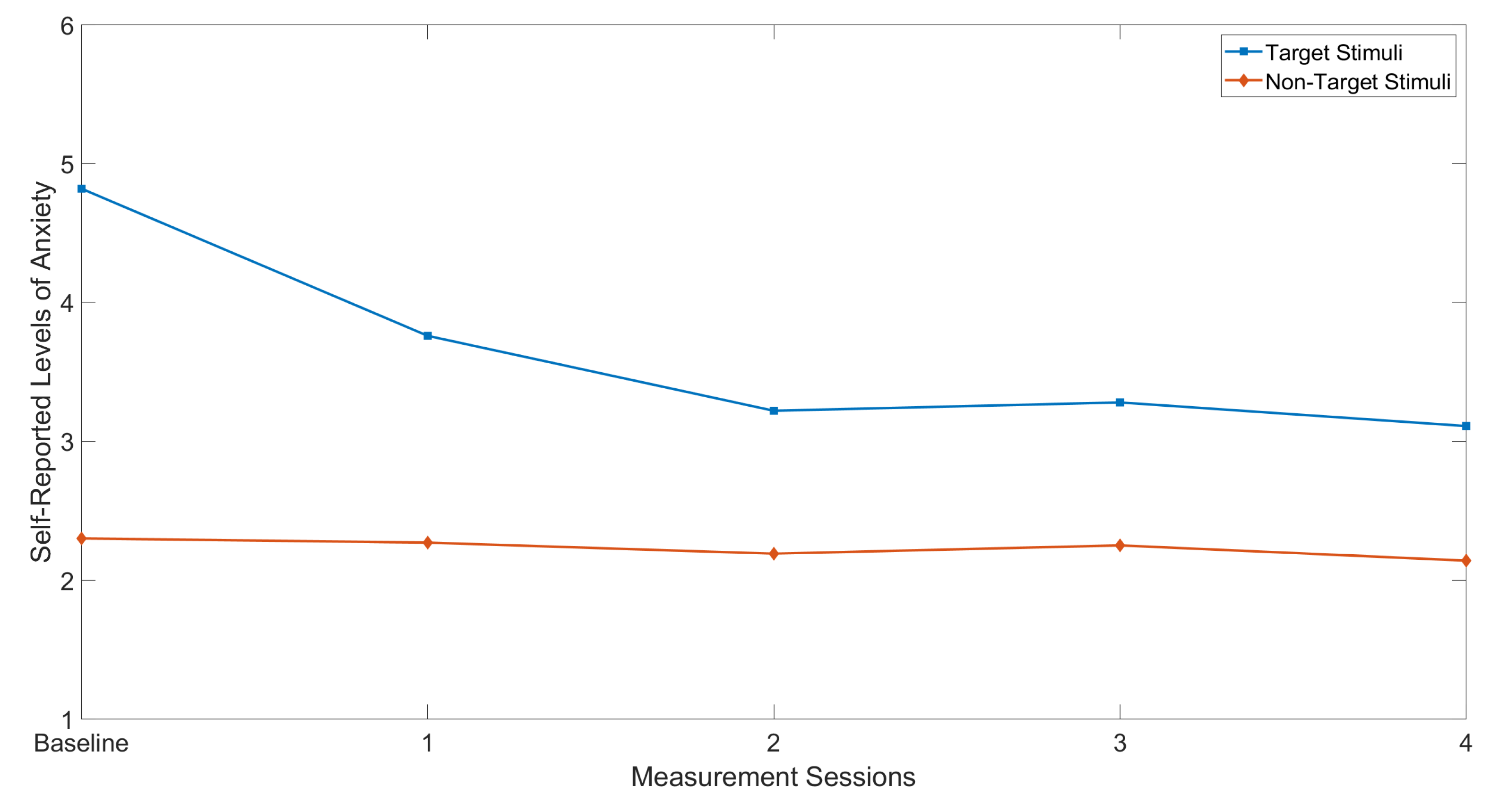
3.1. Modified Smiley-Face Assessment Scale
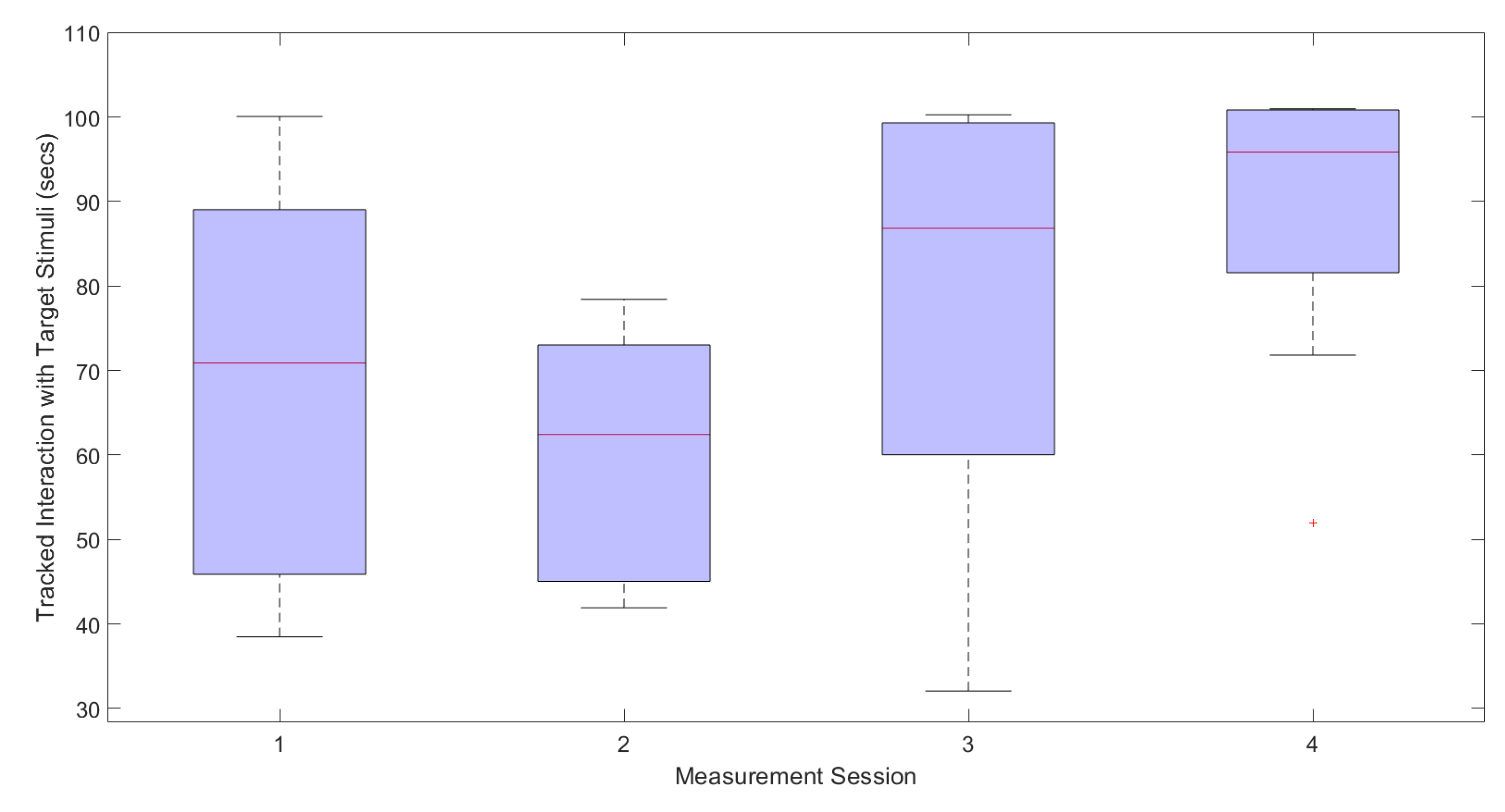
3.2. Tracked Interaction Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ASD | Autism Spectrum Disorders |
| HMD | Head Mounted Display |
| NPC | Non-Playable Character |
| SG | Serious Game |
| VE | Virtual Environment |
| VR | Virtual Reality |
| VRET | Virtual Reality Exposure Therapy |
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Kanner, L. Autistic disturbances of affective contact. Nerv. Child 1943, 2, 217–250. [Google Scholar]
- Frith, U.; Mira, M. Autism and Asperger syndrome. Focus Autistic Behav. 1992, 7, 13–15. [Google Scholar] [CrossRef]
- Bettison, S. The long-term effects of auditory training on children with autism. J. Autism Dev. Disord. 1996, 26, 361–374. [Google Scholar] [CrossRef]
- Edelson, S.M.; Arin, D.; Bauman, M.; Lukas, S.E.; Rudy, J.H.; Sholar, M.; Rimland, B. Auditory integration training: A double-blind study of behavioral and electrophysiological effects in people with autism. Focus Autism Other Dev. Disabil. 1999, 14, 73–81. [Google Scholar] [CrossRef]
- Rimland, B.; Edelson, S.M. Brief report: A pilot study of auditory integration training in autism. J. Autism Dev. Disord. 1995, 25, 61–70. [Google Scholar] [CrossRef]
- Rogers, S.J.; Hepburn, S.; Wehner, E. Parent reports of sensory symptoms in toddlers with autism and those with other developmental disorders. J. Autism Dev. Disord. 2003, 33, 631–642. [Google Scholar] [CrossRef]
- Baranek, G.T.; Boyd, B.A.; Poe, M.D.; David, F.J.; Watson, L.R. Hyperresponsive sensory patterns in young children with autism, developmental delay, and typical development. Am. J. Ment. Retard. 2007, 112, 233–245. [Google Scholar] [CrossRef]
- Stiegler, L.N.; Davis, R. Understanding sound sensitivity in individuals with autism spectrum disorders. Focus Autism Other Dev. Disabil. 2010, 25, 67–75. [Google Scholar] [CrossRef]
- Gomes, E.; Pedroso, F.S.; Wagner, M.B. Auditory hypersensitivity in the autistic spectrum disorder. Pró-Fono Revista de Atualizaç Ao Científica 2008, 20, 279–284. [Google Scholar] [CrossRef]
- Chang, M.C.; Parham, L.D.; Blanche, E.I.; Schell, A.; Chou, C.P.; Dawson, M.; Clark, F. Autonomic and behavioral responses of children with autism to auditory stimuli. Am. J. Occup. Ther. 2012, 66, 567–576. [Google Scholar] [CrossRef]
- Kargas, N.; López, B.; Reddy, V.; Morris, P. The relationship between auditory processing and restricted, repetitive behaviors in adults with autism spectrum disorders. J. Autism Dev. Disord. 2015, 45, 658–668. [Google Scholar] [CrossRef] [PubMed]
- Lucker, J.R. Auditory hypersensitivity in children with autism spectrum disorders. Focus Autism Other Dev. Disabil. 2013, 28, 184–191. [Google Scholar] [CrossRef]
- Gomes, E.; Rotta, N.T.; Pedroso, F.S.; Sleifer, P.; Danesi, M.C. Auditory hypersensitivity in children and teenagers with autistic spectrum disorder. Arq. De Neuro Psiquiatr. 2004, 62, 797–801. [Google Scholar] [CrossRef]
- Rosenhall, U.; Nordin, V.; Brantberg, K.; Gillberg, C. Autism and auditory brain stem responses. Ear Hear. 2003, 24, 206–214. [Google Scholar] [CrossRef]
- Jones, C.R.; Happé, F.; Baird, G.; Simonoff, E.; Marsden, A.J.; Tregay, J.; Phillips, R.J.; Goswami, U.; Thomson, J.M.; Charman, T. Auditory discrimination and auditory sensory behaviours in autism spectrum disorders. Neuropsychologia 2009, 47, 2850–2858. [Google Scholar] [CrossRef]
- Koegel, R.L.; Openden, D.; Koegel, L.K. A systematic desensitization paradigm to treat hypersensitivity to auditory stimuli in children with autism in family contexts. Res. Pract. Pers. Sev. Disabil. 2004, 29, 122–134. [Google Scholar] [CrossRef]
- Steigner, J.; Ruhlin, S.U. Systematic Desensitization of Hyperacusis and Vocal Pitch Disorder Treatment in a Patient with Autism. Internet J. Allied Health Sci. Pract. 2014, 12, 6. [Google Scholar]
- Jolliffe, T.; Lansdown, R.; Robinson, C. Autism: A Personal Account; EduCare, National Bureau for Handicapped Students: London, UK, 1993; 8p. [Google Scholar]
- Grandin, T. A personal perspective of autism. Handb. Autism Pervasive Dev. Disord. 2005, 2, 1276–1286. [Google Scholar]
- O’Donohue, W.T. Cognitive Behavior Therapy: Core Principles for Practice; Wiley: Hoboken, NJ, USA, 2012; pp. 75–97. [Google Scholar]
- Marshall, J.; Hill, R.J.; Dodrill, P. A survey of practice for clinicians working with children with autism spectrum disorders and feeding difficulties. Int. J. Speech Lang. Pathol. 2013, 15, 279–285. [Google Scholar] [CrossRef]
- Marshall, J.; Ware, R.; Ziviani, J.; Hill, R.; Dodrill, P. Efficacy of interventions to improve feeding difficulties in children with autism spectrum disorders: A systematic review and meta-analysis. Child Care Health Dev. 2015, 41, 278–302. [Google Scholar] [CrossRef]
- Tyner, S.; Brewer, A.; Helman, M.; Leon, Y.; Pritchard, J.; Schlund, M. Nice Doggie! Contact Desensitization Plus Reinforcement Decreases Dog Phobias for Children with Autism. Behav. Anal. Pract. 2016, 9, 54–57. [Google Scholar] [CrossRef]
- McMullen, V.; Mahfood, S.L.; Francis, G.L.; Bubenik, J. Using Prediction and Desensitization Techniques to Treat Dental Anxiety: A Case Example. Behav. Interv. 2017, 32, 91–100. [Google Scholar] [CrossRef]
- Van Steensel, F.; Bögels, S. CBT for anxiety disorders in children with and without ASD. J. Consult. Clin. Psychol. 2015, 83, 512–523. [Google Scholar] [CrossRef]
- Wijnhoven, L.A.; Creemers, D.H.; Engels, R.C.; Granic, I. The effect of the video game Mindlight on anxiety symptoms in children with an Autism Spectrum Disorder. BMC Psychiatry 2015, 15, 138. [Google Scholar] [CrossRef]
- Silver, M.; Oakes, P. Evaluation of a new computer intervention to teach people with autism or Asperger syndrome to recognize and predict emotions in others. Autism 2001, 5, 299–316. [Google Scholar] [CrossRef]
- White, S.W.; Oswald, D.; Ollendick, T.; Scahill, L. Anxiety in children and adolescents with autism spectrum disorders. Clin. Psychol. Rev. 2009, 29, 216–229. [Google Scholar] [CrossRef]
- Ince, P.; Haddock, G.; Tai, S. A systematic review of the implementation of recommended psychological interventions for schizophrenia: Rates, barriers, and improvement strategies. Psychol. Psychother. Theory Res. Pract. 2016, 89, 324–350. [Google Scholar] [CrossRef]
- Van Der Krieke, L.; Wunderink, L.; Emerencia, A.C.; De Jonge, P.; Sytema, S. E–mental health self-management for psychotic disorders: State of the art and future perspectives. Psychiatr. Serv. 2014, 65, 33–49. [Google Scholar] [CrossRef]
- Zakari, H.M.; Poyade, M.; Simmons, D. Sinbad and the Magic Cure: A Serious Game for Children with ASD and Auditory Hypersensitivity. In Proceedings of the International Conference on Games and Learning Alliance, Lisbon, Portugal, 5–7 December 2017; Springer: Cham, Switzerland, 2017; pp. 54–63. [Google Scholar]
- Newbutt, N.; Sung, C.; Kuo, H.J.; Leahy, M.J.; Lin, C.C.; Tong, B. Brief report: A pilot study of the use of a virtual reality headset in autism populations. J. Autism Dev. Disord. 2016, 46, 3166–3176. [Google Scholar] [CrossRef]
- Parsons, S.; Cobb, S. State-of-the-art of virtual reality technologies for children on the autism spectrum. Eur. J. Spec. Needs Educ. 2011, 26, 355–366. [Google Scholar] [CrossRef]
- Fino, R.; Lin, M.J.; Caballero, A.; Balahadia, F.F. Disaster Awareness Simulation for Children with Autism Spectrum Disorder Using Android Virtual Reality. J. Telecommun. Electron. Comput. Eng. (JTEC) 2017, 9, 59–62. [Google Scholar]
- Cox, D.J.; Brown, T.; Ross, V.; Moncrief, M.; Schmitt, R.; Gaffney, G.; Reeve, R. Can youth with autism spectrum disorder use virtual reality driving simulation training to evaluate and improve driving performance? An exploratory study. J. Autism Dev. Disord. 2017, 47, 2544–2555. [Google Scholar] [CrossRef]
- Lamash, L.; Klinger, E.; Josman, N. Using a virtual supermarket to promote independent functioning among adolescents with Autism Spectrum Disorder. In Proceedings of the IEEE 2017 International Conference on Virtual Rehabilitation (ICVR), Montreal, QC, Canada, 19–22 June 2017; pp. 1–7. [Google Scholar]
- Miller, H.L.; Bugnariu, N.L. Level of immersion in virtual environments impacts the ability to assess and teach social skills in autism spectrum disorder. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 246–256. [Google Scholar] [CrossRef]
- Lorenzo, G.; Lledó, A.; Pomares, J.; Roig, R. Design and application of an immersive virtual reality system to enhance emotional skills for children with autism spectrum disorders. Comput. Educ. 2016, 98, 192–205. [Google Scholar] [CrossRef]
- Strickland, D.C.; McAllister, D.; Coles, C.D.; Osborne, S. An evolution of virtual reality training designs for children with autism and fetal alcohol spectrum disorders. Top. Lang. Disord. 2007, 27, 226. [Google Scholar] [CrossRef]
- Charitos, D.; Karadanos, G.; Sereti, E.; Triantafillou, S.; Koukouvinou, S.; Martakos, D. Employing virtual reality for aiding the organisation of autistic children behaviour in everyday tasks. In Proceedings of the ICDVRAT, Alghero, Italy, 23–25 September 2000; pp. 147–152. [Google Scholar]
- Wang, M.; Anagnostou, E. Virtual reality as treatment tool for children with autism. In Comprehensive Guide to Autism; Springer: New York, NY, USA, 2014; pp. 2125–2141. [Google Scholar]
- Maples-Keller, J.L.; Bunnell, B.E.; Kim, S.J.; Rothbaum, B.O. The Use of Virtual Reality Technology in the Treatment of Anxiety and Other Psychiatric Disorders. Harv. Rev. Psychiatry 2017, 25, 103–113. [Google Scholar] [CrossRef]
- Diemer, J.; Alpers, G.W.; Peperkorn, H.M.; Shiban, Y.; Mühlberger, A. The impact of perception and presence on emotional reactions: A review of research in virtual reality. Front. Psychol. 2015, 6, 26. [Google Scholar] [CrossRef]
- Price, M.; Anderson, P. The role of presence in virtual reality exposure therapy. J. Anxiety Disord. 2007, 21, 742–751. [Google Scholar] [CrossRef]
- Brinkman, W.P.; Hoekstra, A.R.; van EGMOND, R. The effect of 3D audio and other audio techniques on virtual reality experience. In Annual Review Of Cybertherapy and Telemedicine 2015; IOS Press: Amsterdam, The Netherlands, 2015; pp. 44–49. [Google Scholar]
- Argo, J. Immersive Soundscapes to Elicit Anxiety in Exposure Therapy: Physical Desensitization and Mental Catharsis. Ph.D. Thesis, University of Glasgow, Glasgow, UK, 2017. [Google Scholar]
- Begault, D.R.; Trejo, L.J. 3-D Sound for Virtual Reality and Multimedia; NASA: Hanovcr, MD, USA, 2000.
- Potisk, T. Head-Related Transfer Function; Seminar Ia; Faculty of Mathematics and Physics, University of Ljubljana: Ljubljana, Slovenia, 2015. [Google Scholar]
- Cheng, C.I.; Wakefield, G.H. Introduction to head-related transfer functions (HRTFs): Representations of HRTFs in time, frequency, and space. In Proceedings of the 107th Audio Engineering Society Convention, New York, NY, USA, 24–27 September 1999; Audio Engineering Society: New York, NY, USA, 1999. [Google Scholar]
- Morris, R. Managing Sound Sensitivity in Autism Spectrum Disorder: New Technologies for Customized Intervention. Master’s Thesis, Massachusetts Institute of Technology, Cambridge, MA, USA, 2009. [Google Scholar]
- Whyte, E.M.; Smyth, J.M.; Scherf, K.S. Designing serious game interventions for individuals with autism. J. Autism Dev. Disord. 2015, 45, 3820–3831. [Google Scholar] [CrossRef]
- Kerns, K.A.; Macoun, S.; MacSween, J.; Pei, J.; Hutchison, M. Attention and working memory training: A feasibility study in children with neurodevelopmental disorders. Appl. Neuropsychol. Child 2017, 6, 120–137. [Google Scholar] [CrossRef]
- Tsikinas, S.; Xinogalos, S. Designing effective serious games for people with intellectual disabilities. In Proceedings of the 2018 IEEE Global Engineering Education Conference (EDUCON), Tenerife, Spain, 17–20 April 2018; pp. 1896–1903. [Google Scholar]
- Algazi, V.R.; Duda, R.O. Headphone-based spatial sound. IEEE Signal Process. Mag. 2011, 28, 33–42. [Google Scholar] [CrossRef]
- Kwon, J.; Lee, Y. Serious games for the job training of persons with developmental disabilities. Comput. Educ. 2016, 95, 328–339. [Google Scholar] [CrossRef]
- Iovannone, R.; Dunlap, G.; Huber, H.; Kincaid, D. Effective educational practices for students with autism spectrum disorders. Focus Autism Other Dev. Disabil. 2003, 18, 150–165. [Google Scholar] [CrossRef]
- Unity3D—Game Engine. Available online: https://unity3d.com (accessed on 17 April 2020).
- AudioKinetic-Wwise. Available online: https://www.audiokinetic.com/products/wwise (accessed on 17 April 2020).
- Green, M.; Murphy, D. EigenScape: A database of spatial acoustic scene recordings. Appl. Sci. 2017, 7, 1204. [Google Scholar] [CrossRef]
- Daffern, H.; Camlin, D.; Egermann, H.; Gully, A.J.; Kearney, G.; Neale, C.; Rees-Jones, J. Exploring the potential of virtual reality technology to investigate the health and well being benefits of group singing. Int. J. Perform. Arts Digit. Media 2019, 15, 1–22. [Google Scholar] [CrossRef]
- Freesound—Audio Database. Available online: https://freesound.org/home/ (accessed on 17 April 2020).
- Google Resonance—Spatial Audio SDK. Available online: https://developers.google.com/resonance-audio/ (accessed on 17 April 2020).
- Oculus Rift Head Mounted Display. Available online: https://www.oculus.com/rift/ (accessed on 17 April 2020).
- Wilcoxon, F. Individual comparisons by ranking methods. In Breakthroughs in Statistics; Springer: New York, NY, USA, 1992; pp. 196–202. [Google Scholar]
- Maskey, M.; Rodgers, J.; Grahame, V.; Glod, M.; Honey, E.; Kinnear, J.; Labus, M.; Milne, J.; Minos, D.; McConachie, H.; et al. A Randomised Controlled Feasibility Trial of Immersive Virtual Reality Treatment with Cognitive Behaviour Therapy for Specific Phobias in Young People with Autism Spectrum Disorder. J. Autism Dev. Disord. 2019, 49, 1912–1927. [Google Scholar] [CrossRef]
- Sim oes, M.; Bernardes, M.; Barros, F.; Castelo-Branco, M. Virtual travel training for autism spectrum disorder: Proof-of-concept interventional study. JMIR Serious Games 2018, 6, e5. [Google Scholar] [CrossRef]
- Poyade, M.; Morris, G.; Taylor, I.; Portela, V. Using mobile virtual reality to empower people with hidden disabilities to overcome their barriers. In Proceedings of the 19th ACM International Conference on Multimodal Interaction, Glasgow, UK, 13–17 November 2017; pp. 504–505. [Google Scholar]
- Krijn, M.; Emmelkamp, P.M.; Olafsson, R.P.; Biemond, R. Virtual reality exposure therapy of anxiety disorders: A review. Clin. Psychol. Rev. 2004, 24, 259–281. [Google Scholar] [CrossRef]
- Kuo, M.H.; Orsmond, G.I.; Cohn, E.S.; Coster, W.J. Friendship characteristics and activity patterns of adolescents with an autism spectrum disorder. Autism 2013, 17, 481–500. [Google Scholar] [CrossRef]
- Orsmond, G.I.; Kuo, H.Y. The daily lives of adolescents with an autism spectrum disorder: Discretionary time use and activity partners. Autism 2011, 15, 579–599. [Google Scholar] [CrossRef]
- Li, K.H.; Lou, S.J.; Tsai, H.Y.; Shih, R.C. The Effects of Applying Game-Based Learning to Webcam Motion Sensor Games for Autistic Students’ Sensory Integration Training. Turk. Online J. Educ. Technol. TOJET 2012, 11, 451–459. [Google Scholar]
- Bernardini, S.; Porayska-Pomsta, K.; Smith, T.J. ECHOES: An intelligent serious game for fostering social communication in children with autism. Inf. Sci. 2014, 264, 41–60. [Google Scholar] [CrossRef]
- Almeida, L.M.; da Silva, D.P.; Theodório, D.P.; Silva, W.W.; Rodrigues, S.C.M.; Scardovelli, T.A.; da Silva, A.P.; Bissaco, M.A.S. ALTRIRAS: A Computer Game for Training Children with Autism Spectrum Disorder in the Recognition of Basic Emotions. Int. J. Comput. Games Technol. 2019, 2019, 4384896. [Google Scholar] [CrossRef]
- Tsikinas, S.; Xinogalos, S. Design guidelines for serious games targeted to people with autism. In Smart Education and e-Learning 2019; Springer: Singapore, 2019; pp. 489–499. [Google Scholar]
- Maskey, M.; Lowry, J.; Rodgers, J.; McConachie, H.; Parr, J.R. Reducing specific phobia/fear in young people with autism spectrum disorders (ASDs) through a virtual reality environment intervention. PLoS ONE 2014, 9, e100374. [Google Scholar] [CrossRef]
- Mayes, S.D.; Calhoun, S.L.; Aggarwal, R.; Baker, C.; Mathapati, S.; Molitoris, S.; Mayes, R.D. Unusual fears in children with autism. Res. Autism Spectr. Disord. 2013, 7, 151–158. [Google Scholar] [CrossRef]
- Tomchek, S.D.; Dunn, W. Sensory processing in children with and without autism: A comparative study using the short sensory profile. Am. J. Occup. Ther. 2007, 61, 190–200. [Google Scholar] [CrossRef]
- Berry, J.O.; Jones, W.H. The parental stress scale: Initial psychometric evidence. J. Soc. Pers. Relatsh. 1995, 12, 463–472. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | Gender | Age | Stimulus |
|---|---|---|---|
| A | M | 18 | Group Singing, Baby Crying |
| B | M | 18 | Group Singing, Children Screaming/Shouting |
| C | F | 17 | Children Screaming/Shouting |
| D | M | 16 | Sirens, Children Screaming/Shouting |
| E | F | 19 | Children Screaming/Shouting |
| F | M | 18 | Children Screaming/Shouting, Baby Crying |
| Exposure Level | Virtual Distance between Player and Stimulus |
|---|---|
| 1 | 25 m |
| 2 | 15 m |
| 3 | 5 m |
| 4 | 2.5 m |
| Participant | Stimulus | Baseline SUD Score | Final Score SUD Score |
|---|---|---|---|
| A | Group Singing | 5 | 3 |
| Baby Crying | 6 | 4 | |
| B | Group Singing | 5 | 3 |
| Children Screaming/Shouting | 4 | 3 | |
| C | Children Screaming/Shouting | 6 | 5 |
| D | Sirens | 5 | 3 |
| Children Screaming/Shouting | 5 | 3 | |
| E | Children Screaming/Shouting | 5 | 4 |
| F | Children Screaming/Shouting | 4 | 3 |
| Baby Crying | 6 | 3 |
| Participant | Stimulus | Session 1 | Session 2 | Session 3 | Session 4 |
|---|---|---|---|---|---|
| A | Group Singing | 71.45 | 44.39 | 68.13 | 100.98 |
| Baby Crying | 43.00 | 57.74 | 89.45 | 81.57 | |
| B | Group Singing | 92.00 | 75.03 | 60.03 | 84.26 |
| Children Screaming / Shouting | 71.45 | 44.39 | 68.13 | 100.98 | |
| C | Children Screaming / Shouting | 65.84 | 61.31 | 23.06 | 71.82 |
| D | Sirens | 70.32 | 41.91 | 93.87 | 100.53 |
| Children Screaming / Shouting | 89.02 | 63.55 | 84.20 | 100.87 | |
| E | Children Screaming / Shouting | 38.46 | 45.04 | 53.19 | 51.93 |
| F | Children Screaming / Shouting | 100.07 | 73.03 | 99.30 | 99.15 |
| Baby Crying | 82.21 | 78.41 | 99.95 | 92.55 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johnston, D.; Egermann, H.; Kearney, G. SoundFields: A Virtual Reality Game Designed to Address Auditory Hypersensitivity in Individuals with Autism Spectrum Disorder. Appl. Sci. 2020, 10, 2996. https://doi.org/10.3390/app10092996
Johnston D, Egermann H, Kearney G. SoundFields: A Virtual Reality Game Designed to Address Auditory Hypersensitivity in Individuals with Autism Spectrum Disorder. Applied Sciences. 2020; 10(9):2996. https://doi.org/10.3390/app10092996
Chicago/Turabian StyleJohnston, Daniel, Hauke Egermann, and Gavin Kearney. 2020. "SoundFields: A Virtual Reality Game Designed to Address Auditory Hypersensitivity in Individuals with Autism Spectrum Disorder" Applied Sciences 10, no. 9: 2996. https://doi.org/10.3390/app10092996
APA StyleJohnston, D., Egermann, H., & Kearney, G. (2020). SoundFields: A Virtual Reality Game Designed to Address Auditory Hypersensitivity in Individuals with Autism Spectrum Disorder. Applied Sciences, 10(9), 2996. https://doi.org/10.3390/app10092996