3.2. Registration Phase
In the second phase, two roles, namely patients and remote hospital doctors or clinics, need to register at the CA. We describe these two roles separately in the following subsections.
3.2.1. Patients Registration Phase
Patients must register the first time with the CA in the prior EPRS registration phase and create patient accounts on the EPRS in the following three stages.
Stage 1. Pi keys in onsite his/her identity IDPi and imprints the fingerprint Bi; then, the CA obtains {IDPi, H (Bi)}.
Stage 2. The CA receives the message {IDPi, H (Bi)} from Pi and then calculates the secret token Vi = IDPi ⊕ H (Bi), generates a random number RPi, computes secret token STi = IDPi ⊕ RPi, computes secret token Si = RPi ⊕ h (TCA), and M1 = RPi ⊕ h (IDe ⊕ TCA). Then, the CA stores {Vi, STi, Si} to the smart card and stores the patient ID IDPi to its ID list table. The CA then sends the smart card back to the Pi through the secure channel and sends {STi, M1} to the EPRS over the public channel.
Stage 3. The EPRS receives the message {STi, M1} from the CA and then computes RPi = M1 ⊕ EC, IDPi = STi ⊕ RPi, creates a new patient record EPR {Ri} for IDPi, encrypts Ri using RPi {ERPi (Ri)}, and stores IDPi, ERPi (Ri) to EPRS’s database.
3.2.2. Remote Hospital Doctors or Clinics Registration Phase
The hospital doctors or clinics must also register the first time with the CA in the prior patient’s registration phase by the following two stages.
Stage 1. Doctor Dj registers on-site the first time with a CA. The CA generates the identifier IDj for the Dj and then computes DCj = h (h (IDj) ⊕ TCA), stores DCj to a medical card of doctor Dj, and then sends back to the doctor Dj via a secure channel.
Stage 2. Dj receives the personal medical card from the CA and keeps the medical card on hand.
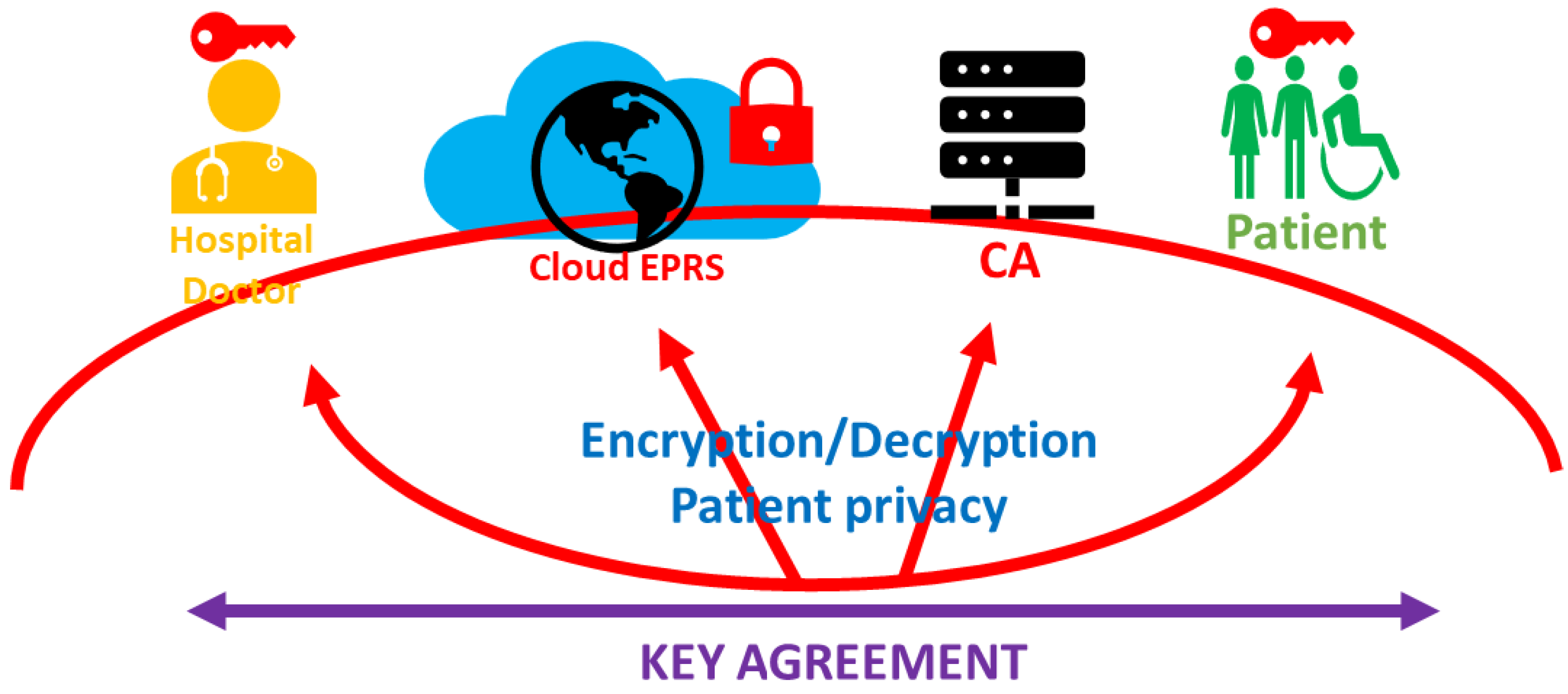
3.3. Secure Electronic Patient Record Storing, Sharing, and Updating Communication Phase
This phase involves the stages of health medical privacy creation, sharing, and storage. In our iPatient access control model, doctors or clinics have read and updated permissions, while authorized professionals have only read permissions. Only patients themselves can access the encrypted personal privacy of the cloud server. Additionally, all data stored in the cloud are also protected by the patient’s private key. All decrypted data must be transmitted in a secure tunnel established through a key agreement. Below, we show six strategies in the iPatient access control model and show the strategy diagram in
Figure 3.
The privacy of all patients is protected and stored in a cloud database via the patient’s private key.
Anyone who wants to access patient privacy records must obtain the patient’s authorization and obtain the records of the patient via patient downloading from the cloud database.
In the case of protecting the privacy of the cloud database, only patients can access via key agreement to establish a secure tunnel. After the tunnel is established, the transmitted data still need to be encrypted with the session key before it can be transmitted securely.
Doctors modify, update patient records, and send them to the patient via the session key. After the patient decrypts the updated patient records, s/he will use the personal private key to encrypt them, and then encrypt them with the session key to upload them to the cloud database server. Once the cloud data server receives and decodes them with the session key, it will update them to the patient records database.
Other authorized professionals excluding doctors can only read the patient records transmitted by the patient through the secure tunnel after they have been authenticated by the key agreement. They cannot modify or update patient records.
Our design for iPatient is personally led and we want to establish a privacy sharing mechanism that is completely patient-led.
Below, we introduce the steps we designed. First, we perform the three-party key agreement process in order to build a secure tunnel, and then decrypt, add, and modify the medical records in a secure tunnel.
Stage 1. Pi imprints the biometric Bi and then deciphers his/her identity by IDPi = Vi ⊕ H (Bi), deciphers RPiold = STi ⊕ IDPi, NIDPi = IDPi ⊕ RPinew, and generates a new random number RPinew, M1 = RPiold ⊕ Si ⊕ RPinew. Pi then sends message {NIDPi, NIDDj, M1} to the CA via a public channel.
Stage 2. After receiving the message from the Pi, the CA deciphers RPinew = M1 ⊕h (TCA), IDPi = NIDPi ⊕ RPinew, and checks the patient identity IDPi from the CA’s ID table. If the legal list cannot find the IDPi, the request is terminated. Then, the CA calculates IDDj = NIDDj ⊕ RPinew, computes M2 = RPinew ⊕ h (IDe ⊕ TCA), M3 = RPinew ⊕ h (IDDj ⊕ TCA), and then sends a request of message and parameters tuple {NIDPi, NIDDj, M2} to the EPRS through the public channel. Then, the CA sends {NIDPi, M3} to the doctor Dj via a public channel.
Stage 3. After receiving the message {NIDPi, NIDDj, M2} from the CA, the EPRS computes RPinew = M2 ⊕ EC, IDPi = NIDPi ⊕ RPinew, and checks IDPi from the EPRS database. Then, the EPRS generates a random number REPRS, generates secret token M4 = RPinew ⊕ REPRS, and then sends M4 to doctor Dj via a public channel.
Stage 4. After receiving the message {NIDPi, M3} from the CA and M4 from the EPRS, Dj computes RPinew = M3 ⊕ DC, IDPi = NIDPi ⊕ RPinew, generates a random number RD, computes REPRS = M4 ⊕ RPinew, M5 = RD ⊕ REPRS, and then sends {M5, NIDPi} to the CA and {M5} to the EPRS via a public channel. Then, Dj owns the session key SK = h (RPinew ⊕ REPRS ⊕ RD).
Stage 5. The EPRS receives the message {M5} from Dj, computes RD = M5 ⊕ REPRS, and then computes session key SK = h (RPinew ⊕REPRS ⊕ RD).
Stage 6. The CA receives the message {M5, NIDPi} from doctor Dj and then sends M5 to Pi by checking NIDPi.
Stage 7. After receiving the message from the CA, Pi computes session key SK = h (RPinew ⊕ M5), updates secret tokens STi = STi ⊕ RPinew ⊕ RPiold and Si = Si ⊕ RPinew ⊕ RPiold, and then finishes key agreement.
After the key agreement process is done, the secure tunnel among Pi, the EPRS, and Dj is established. The three roles can use the same one-time session key for secure communication. Next, the patient privacy history update process under the secure channel is detailed in Stage 8 to Stage 12.
Stage 8. The EPRS uses the secret session key SK to encrypt the privacy record of the IDpi patient, M6 = {ESK (EK (Ri))}, and then sends M6 to patient Pi.
Stage 9. Pi receives the encrypted electronic patient record {ESK (EK (Ri))} and decrypts ESK (EK (Ri)) using session key SK to obtain EK (Ri). Then, Pi applies RPiold to decipher the original Ri = DRPiold (EK (Ri)) and then enciphers the original Ri with session key SK to message M7 = ESK (Ri). Then, Pi sends M7 to doctor Dj.
Stage 10. The doctor Dj receives the message M7 from Pi and deciphers the original record Ri using SK, Ri = DSK (M7). When the telehealth service is done, the doctor generates a new record Rinew and then enciphers the new record Rinew using session key SK to obtain message M8 = ESK (Rinew). Then, the doctor Dj sends encrypted privacy record M8 to Pi.
Stage 11. Pi receives the message from Dj and uses session key SK to obtain Rinew = DSK (M8). Then, Pi enciphers himself the privacy record to obtain M9 = ESK (ERPinew (Rinew)) and sends M9 to the EPRS.
Stage 12. The EPRS receives the message M9 from Pi and then computes M10 = DSK (M9). The EPRS updates IDPi’s electronic patient record using M10 {ERPinew (Rinew)} and then finishes the data sharing and data update phase.







{kind=link}
{kind=link}
{kind=link}
{kind=link}