Three-Dimensional CAD in Skull Reconstruction: A Narrative Review with Focus on Cranioplasty and Its Potential Relevance to Brain Sciences




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Rationale to Remove (Decompressive Craniectomy) and Replace (Cranioplasty) the Skull Bone
3. Brief Outline of Materials Used for Cranioplasty
4. Aesthetics of Cranioplasty—Not Solely Limited to the Function of Bone Replacement
5. Three-Dimensional CAD/CAM Models in the Reconstruction of Skull Defects
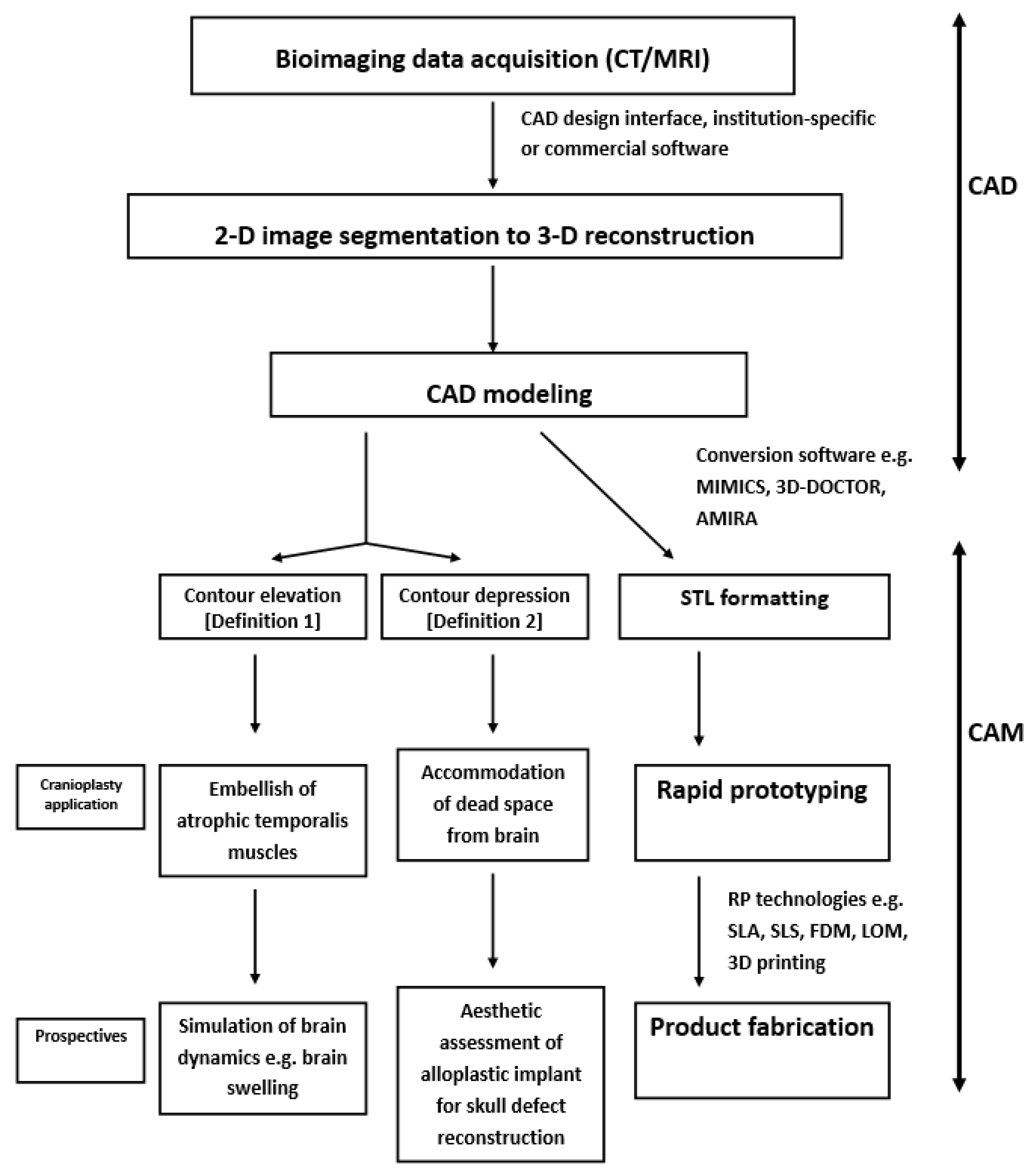
6. Brief Overview of the CAD Modeling Process for the Reconstruction of Cranial Defects
7. Demonstration of Editing the 2-D Images of Brain CT Scans Using Commercial Software
- PD surrounding points in image D,PD+1 surrounding points in image D + 1,Adjacent point in image D + 1 of the sth point in image L is the (s* PD + 1 /PD)th point in image D + 1.Let n = (s*PD + 1 /PD), for the sth point in image D, triangles are formed by connectingthe sth and (s + 1)th points in image D and the nth point in image D + 1the (s + 1)th point in image D and the nth and (n + 1)th points in image D + 1
8. Brief Overview of CAM Processing for Reconstruction of Cranial Defects
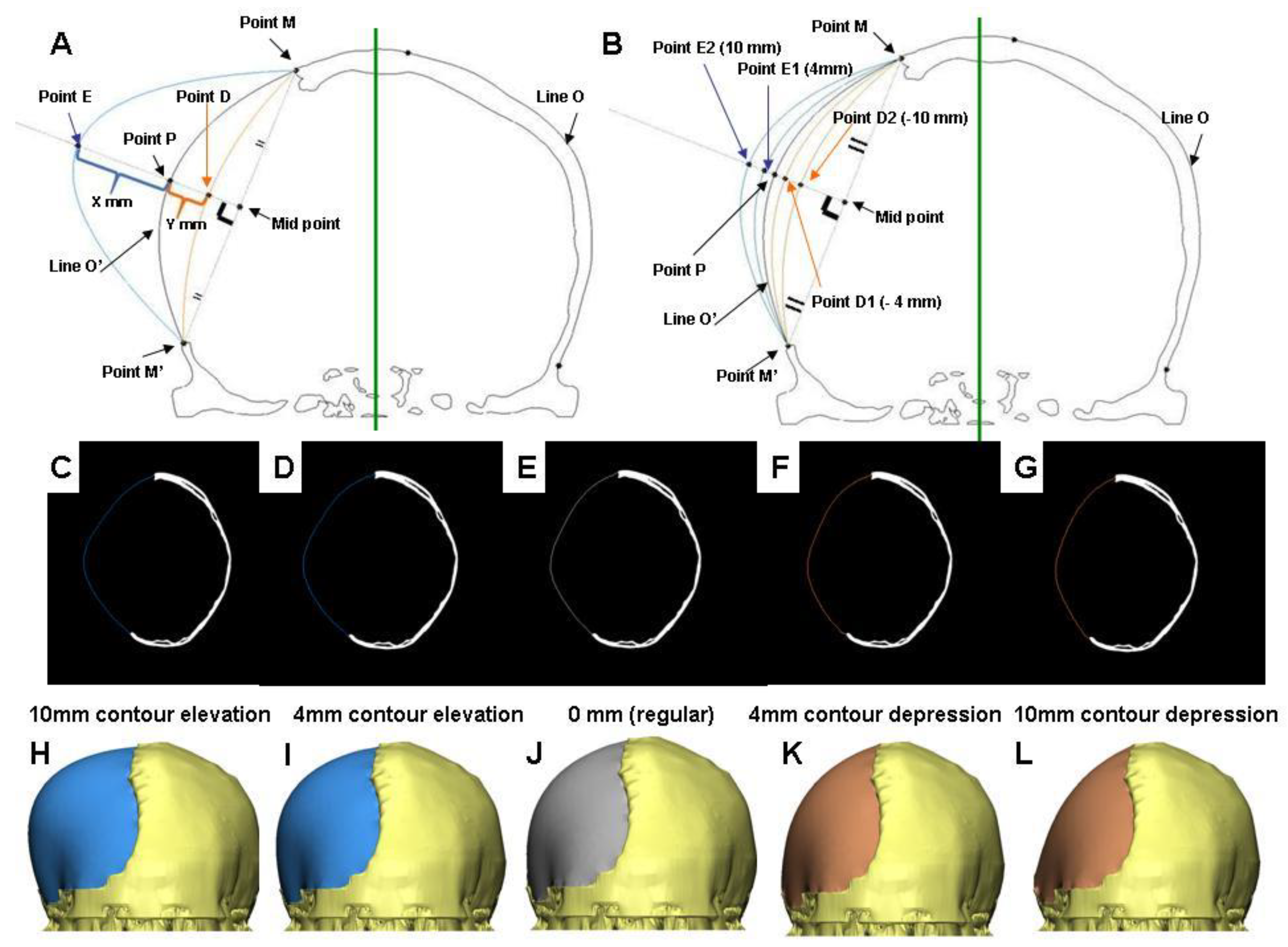
9. Clinical Consideration of CAD Algorithms for Adjusting Contours
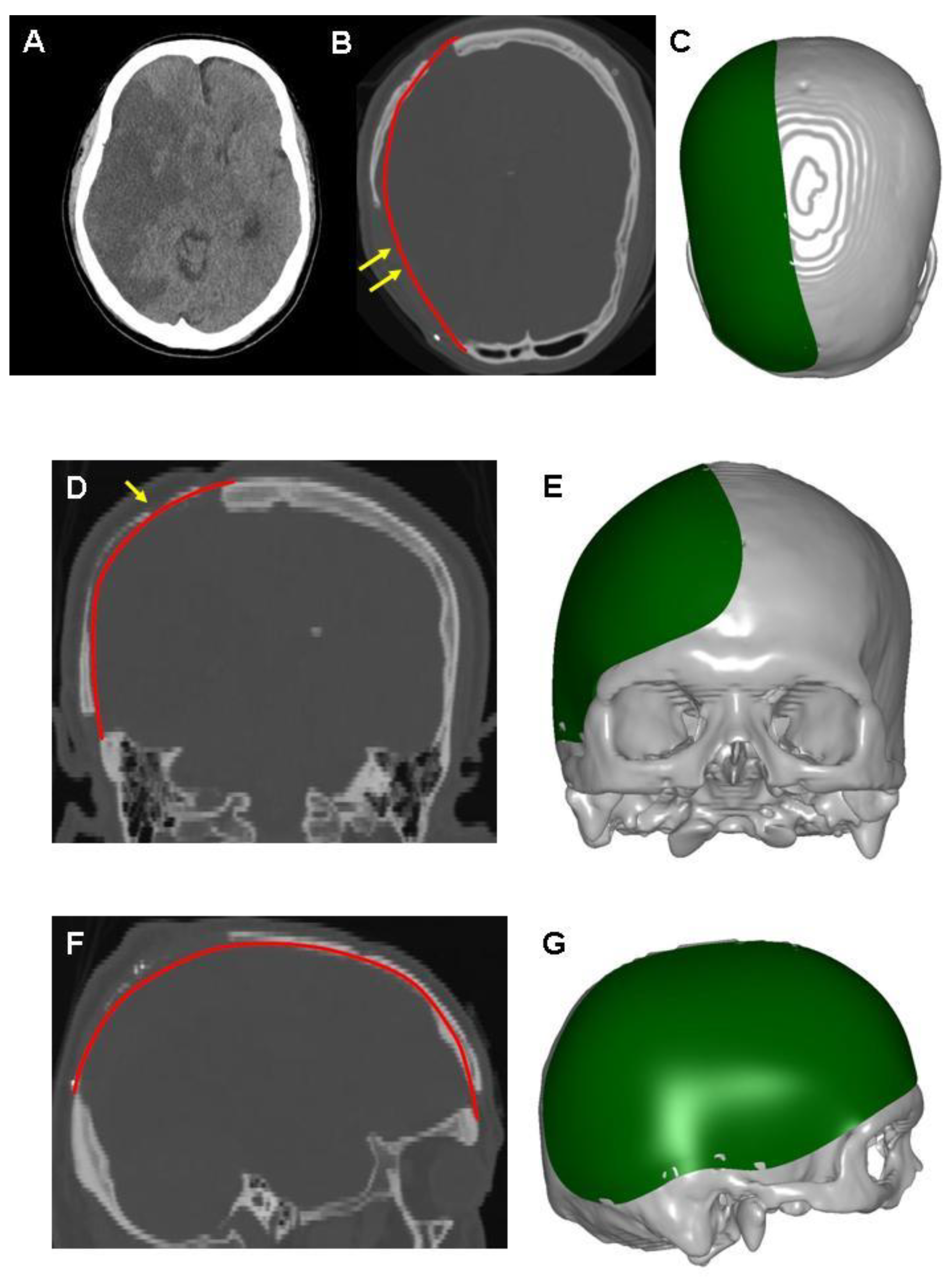
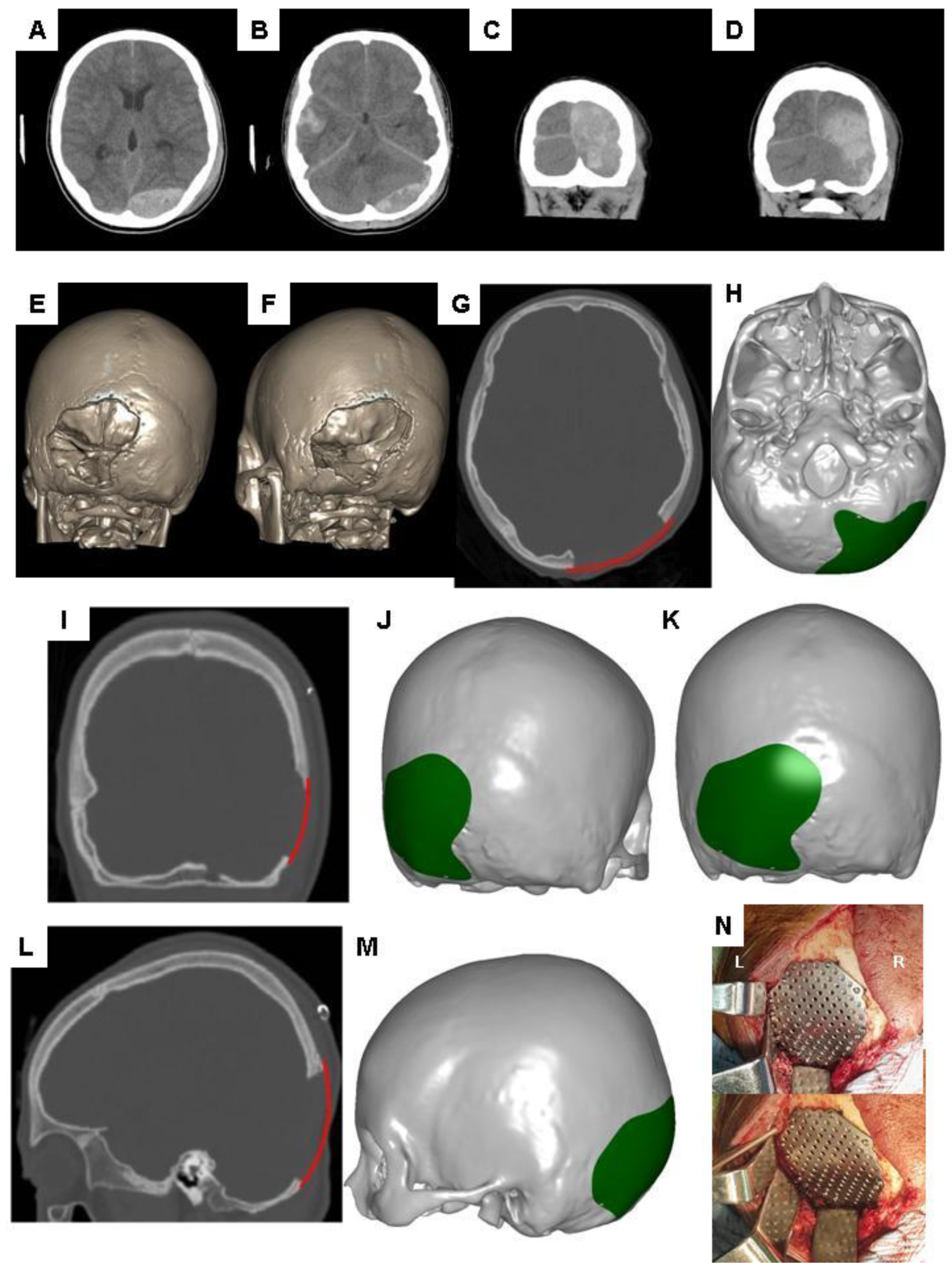
10. Demonstration of Adjusting Contours for the Reconstruction of Skull Defects in CAD Modeling
11. Potential Application of CAD Models with Adjusting Contours in Prospective Brain Sciences
12. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Shah, S.; Kimberly, W.T. Today’s Approach to Treating Brain Swelling in the Neuro Intensive Care Unit. Semin. Neurol. 2016, 36, 502–507. [Google Scholar] [CrossRef]
- Stokum, J.A.; Kurland, D.B.; Gerzanich, V.; Simard, J.M. Mechanisms of astrocyte-mediated cerebral edema. Neurochem. Res. 2015, 40, 317–328. [Google Scholar] [CrossRef]
- Klatzo, I. Presidental address. Neuropathological aspects of brain edema. J. Neuropathol. Exp. Neurol. 1967, 26, 1–14. [Google Scholar] [CrossRef]
- Simard, J.M.; Kent, T.A.; Chen, M.; Tarasov, K.V.; Gerzanich, V. Brain oedema in focal ischaemia: Molecular pathophysiology and theoretical implications. Lancet Neurol. 2007, 6, 258–268. [Google Scholar] [CrossRef]
- Bouzat, P.; Sala, N.; Payen, J.F.; Oddo, M. Beyond intracranial pressure: Optimization of cerebral blood flow, oxygen, and substrate delivery after traumatic brain injury. Ann. Intensive Care 2013, 3, 23. [Google Scholar] [CrossRef]
- Stokum, J.A.; Gerzanich, V.; Simard, J.M. Molecular pathophysiology of cerebral edema. J. Cereb. Blood Flow Metab. 2016, 36, 513–538. [Google Scholar] [CrossRef]
- Marbacher, S.; Andres, R.H.; Fathi, A.R.; Fandino, J. Primary reconstruction of open depressed skull fractures with titanium mesh. J. Craniofac. Surg. 2008, 19, 490–495. [Google Scholar] [CrossRef]
- Chang, S.; Harrington, T.R.; Petersen, S.R. Craniectomy for traumatic brain injury. Barrow. Q. 2003, 61, 744–752. [Google Scholar]
- Huang, X.; Wen, L. Technical considerations in decompressive craniectomy in the treatment of traumatic brain injury. Int. J. Med. Sci. 2010, 7, 385–390. [Google Scholar] [CrossRef]
- Kolias, A.G.; Kirkpatrick, P.J.; Hutchinson, P.J. Decompressive craniectomy: Past, present and future. Nat. Rev. Neurol. 2013, 9, 405–415. [Google Scholar] [CrossRef]
- Bor-Seng-Shu, E.; Figueiredo, E.G.; Fonoff, E.T.; Fujimoto, Y.; Panerai, R.B.; Teixeira, M.J. Decompressive craniectomy and head injury: Brain morphometry, ICP, cerebral hemodynamics, cerebral microvascular reactivity, and neurochemistry. Neurosurg. Rev. 2013, 36, 361–370. [Google Scholar] [CrossRef]
- Schirmer, C.M.; Ackil, A.A., Jr.; Malek, A.M. Decompressive Craniectomy. Neurocrit. Care 2008, 8, 456–470. [Google Scholar] [CrossRef]
- Adamo, M.A.; Drazin, D.; Waldman, J.B. Decompressive craniectomy and postoperative complication management in infants and toddlers with severe traumatic brain injuries. J. Neurosurg. Pediatr. 2009, 3, 334–339. [Google Scholar] [CrossRef]
- Joseph, V.; Reilly, P. Syndrome of the trephined. J. Neurosurg. 2009, 111, 650–652. [Google Scholar] [CrossRef]
- Segal, D.H.; Oppenheim, J.S.; Murovic, J.A. Neurological recovery after cranioplasty. Neurosurgery 1994, 34, 729–731. [Google Scholar]
- Schaller, B.; Graf, R.; Sanada, Y.; Rosner, G.; Wienhard, K.; Heiss, W.D. Hemodynamic and metabolic effects of decompressive hemicraniectomy in normal brain. An experimental PET-study in cats. Brain Res. 2003, 982, 31–37. [Google Scholar] [CrossRef]
- Bandyopadhyay, T.K.; Thapliyal, G.K.; Dubey, A.K. Reconstruction of Cranial Defects in Armed Forces Personnel—Our Experience. Med. J. Armed. Forces. India 2005, 61, 36–40. [Google Scholar] [CrossRef]
- Chang, V.; Hartzfeld, P.; Langlois, M.; Mahmood, A.; Seyfried, D. Outcomes of cranial repair after craniectomy. J. Neurosurg. 2010, 112, 1120–1124. [Google Scholar] [CrossRef]
- Prolo, D.J.; Oklund, S.A. The use of bone grafts and alloplastic materials in cranioplasty. Clin. Orthop. Relat Res. 1991, 268, 270–278. [Google Scholar]
- Marchac, D.; Greensmith, A. Long-term experience with methylmethacrylate cranioplasty in craniofacial surgery. J. Plast. Reconstr. Aesthet. Surg. 2008, 61, 744–752. [Google Scholar] [CrossRef]
- Cabraja, M.; Klein, M.; Lehmann, T.N. Long-term results following titanium cranioplasty of large skull defects. Neurosurg. Focus 2009, 26, E10. [Google Scholar] [CrossRef]
- Staffa, G.; Nataloni, A.; Compagnone, C.; Servadei, F. Custom made cranioplasty prostheses in porous hydroxy-apatite using 3D design techniques: 7 years experience in 25 patients. Acta Neurochir. 2007, 149, 161–170. [Google Scholar] [CrossRef]
- Janecka, I.P. New reconstructive technologies in skull base surgery: Role of titanium mesh and porous polyethylene. Arch. Otolaryngol. Head Neck Surg. 2000, 126, 396–401. [Google Scholar] [CrossRef]
- Lakhani, R.S.; Shibuya, T.Y.; Mathog, R.H.; Marks, S.C.; Burgio, D.L.; Yoo, G.H. Titanium mesh repair of the severely comminuted frontal sinus fracture. Arch. Otolaryngol. Head Neck Surg. 2001, 127, 665–669. [Google Scholar] [CrossRef]
- Azmi, A.; Latiff, A.Z.; Johari, A. Methyl methacrylate cranioplasty. Med. J. Malaysia 2004, 59, 418–421. [Google Scholar]
- Kung, W.M.; Lin, F.H.; Hsiao, S.H.; Chiu, W.T.; Chyau, C.C.; Lu, S.H.; Hwang, B.; Lee, J.H.; Lin, M.S. New reconstructive technologies after decompressive craniectomy in traumatic brain injury: The role of three-dimensional titanium mesh. J. Neurotrauma 2012, 29, 2030–2037. [Google Scholar] [CrossRef]
- Brommeland, T.; Rydning, P.N.; Pripp, A.H.; Helseth, E. Cranioplasty complications and risk factors associated with bone flap resorption. Scand. J. Trauma Resusc. Emerg. Med. 2015, 23, 75. [Google Scholar] [CrossRef]
- Dunisch, P.; Walter, J.; Sakr, Y.; Kalff, R.; Waschke, A.; Ewald, C. Risk factors of aseptic bone resorption: A study after autologous bone flap reinsertion due to decompressive craniotomy. J. Neurosurg. 2013, 118, 1141–1147. [Google Scholar] [CrossRef]
- Honeybul, S.; Morrison, D.A.; Ho, K.M.; Lind, C.R.; Geelhoed, E. A randomized controlled trial comparing autologous cranioplasty with custom-made titanium cranioplasty. J. Neurosurg. 2017, 126, 81–90. [Google Scholar] [CrossRef]
- Schoekler, B.; Trummer, M. Prediction parameters of bone flap resorption following cranioplasty with autologous bone. Clin. Neurol. Neurosurg. 2014, 120, 64–67. [Google Scholar] [CrossRef]
- Park, S.P.; Kim, J.H.; Kang, H.I.; Kim, D.R.; Moon, B.G.; Kim, J.S. Bone Flap Resorption Following Cranioplasty with Autologous Bone: Quantitative Measurement of Bone Flap Resorption and Predictive Factors. J. Korean Neurosurg. Soc. 2017, 60, 749–754. [Google Scholar] [CrossRef]
- Matic, D.B.; Manson, P.N. Biomechanical analysis of hydroxyapatite cement cranioplasty. J. Craniofac. Surg. 2004, 15, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, A.; Illi, O.E.; Sailer, H.F.; Stauffer, U.G. Cranioplasties for congenital and acquired skull defects in children--comparison of new concepts with conventional methods. Eur. J. Pediatr. Surg. 1993, 3, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Grant, G.A.; Jolley, M.; Ellenbogen, R.G.; Roberts, T.S.; Gruss, J.R.; Loeser, J.D. Failure of autologous bone-assisted cranioplasty following decompressive craniectomy in children and adolescents. J. Neurosurg. 2004, 100, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Kung, W.M.; Lin, M.S. A simplified technique for polymethyl methacrylate cranioplasty: Combined cotton stacking and finger fracture method. Brain Inj. 2012, 26, 1737–1742. [Google Scholar] [CrossRef]
- Chen, S.T.; Chang, C.J.; Su, W.C.; Chang, L.W.; Chu, I.H.; Lin, M.S. 3-D titanium mesh reconstruction of defective skull after frontal craniectomy in traumatic brain injury. Injury 2015, 46, 80–85. [Google Scholar] [CrossRef]
- Davidowitz, G.; Kotick, P.G. The use of CAD/CAM in dentistry. Dent. Clin. North Am. 2011, 55, 559–570. [Google Scholar] [CrossRef]
- Leeson, D. The digital factory in both the modern dental lab and clinic. Dent. Mater. 2020, 36, 43–52. [Google Scholar] [CrossRef]
- Jiao, T.; Zhang, F.; Huang, X.; Wang, C. Design and fabrication of auricular prostheses by CAD/CAM system. Int. J. Prosthodont. 2004, 17, 460–463. [Google Scholar]
- Bramlet, M.; Olivieri, L.; Farooqi, K.; Ripley, B.; Coakley, M. Impact of Three-Dimensional Printing on the Study and Treatment of Congenital Heart Disease. Circ. Res. 2017, 120, 904–907. [Google Scholar] [CrossRef]
- Malis, L.I. Titanium mesh and acrylic cranioplasty. Neurosurgery 1989, 25, 351–355. [Google Scholar] [CrossRef]
- Scholz, M.; Wehmoller, M.; Lehmbrock, J.; Schmieder, K.; Engelhardt, M.; Harders, A.; Eufinger, H. Reconstruction of the temporal contour for traumatic tissue loss using a CAD/CAM-prefabricated titanium implant-case report. J. Craniomaxillofac. Surg. 2007, 35, 388–392. [Google Scholar] [CrossRef]
- Sun, W.; Darling, A.; Starly, B.; Nam, J. Computer-aided tissue engineering: Overview, scope and challenges. Biotechnol. Appl. Biochem. 2004, 39, 29–47. [Google Scholar] [CrossRef] [PubMed]
- Kung, W.M.; Chen, S.T.; Lin, C.H.; Lu, Y.M.; Chen, T.H.; Lin, M.S. Verifying three-dimensional skull model reconstruction using cranial index of symmetry. PLoS ONE 2013, 8, e74267. [Google Scholar] [CrossRef] [PubMed]
- Zonenshayn, M.; Kronberg, E.; Souweidane, M.M. Cranial index of symmetry: An objective semiautomated measure of plagiocephaly. Technical note. J. Neurosurg. 2004, 100, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Nayar, S.; Bhuminathan, S.; Bhat, W.M. Rapid prototyping and stereolithography in dentistry. J. Pharm. Bioallied Sci. 2015, 7, S216–S219. [Google Scholar] [CrossRef] [PubMed]




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kung, W.-M.; Tzeng, I.-S.; Lin, M.-S. Three-Dimensional CAD in Skull Reconstruction: A Narrative Review with Focus on Cranioplasty and Its Potential Relevance to Brain Sciences. Appl. Sci. 2020, 10, 1847. https://doi.org/10.3390/app10051847
Kung W-M, Tzeng I-S, Lin M-S. Three-Dimensional CAD in Skull Reconstruction: A Narrative Review with Focus on Cranioplasty and Its Potential Relevance to Brain Sciences. Applied Sciences. 2020; 10(5):1847. https://doi.org/10.3390/app10051847
Chicago/Turabian StyleKung, Woon-Man, I-Shiang Tzeng, and Muh-Shi Lin. 2020. "Three-Dimensional CAD in Skull Reconstruction: A Narrative Review with Focus on Cranioplasty and Its Potential Relevance to Brain Sciences" Applied Sciences 10, no. 5: 1847. https://doi.org/10.3390/app10051847
APA StyleKung, W.-M., Tzeng, I.-S., & Lin, M.-S. (2020). Three-Dimensional CAD in Skull Reconstruction: A Narrative Review with Focus on Cranioplasty and Its Potential Relevance to Brain Sciences. Applied Sciences, 10(5), 1847. https://doi.org/10.3390/app10051847