Evaluation of Commercial Ropes Applied as Artificial Tendons in Robotic Rehabilitation Orthoses

 , , , and
, , , and
Abstract
Featured Application
Abstract
1. Introduction
2. Methodology
2.1. Device
2.2. Volunteers
2.3. Artificial Tendons Design and Selection
2.3.1. Applied Loads Determination
2.3.2. Tensile Strength Test
2.3.3. Pilot Test
3. Results
3.1. Applied Loads Determination
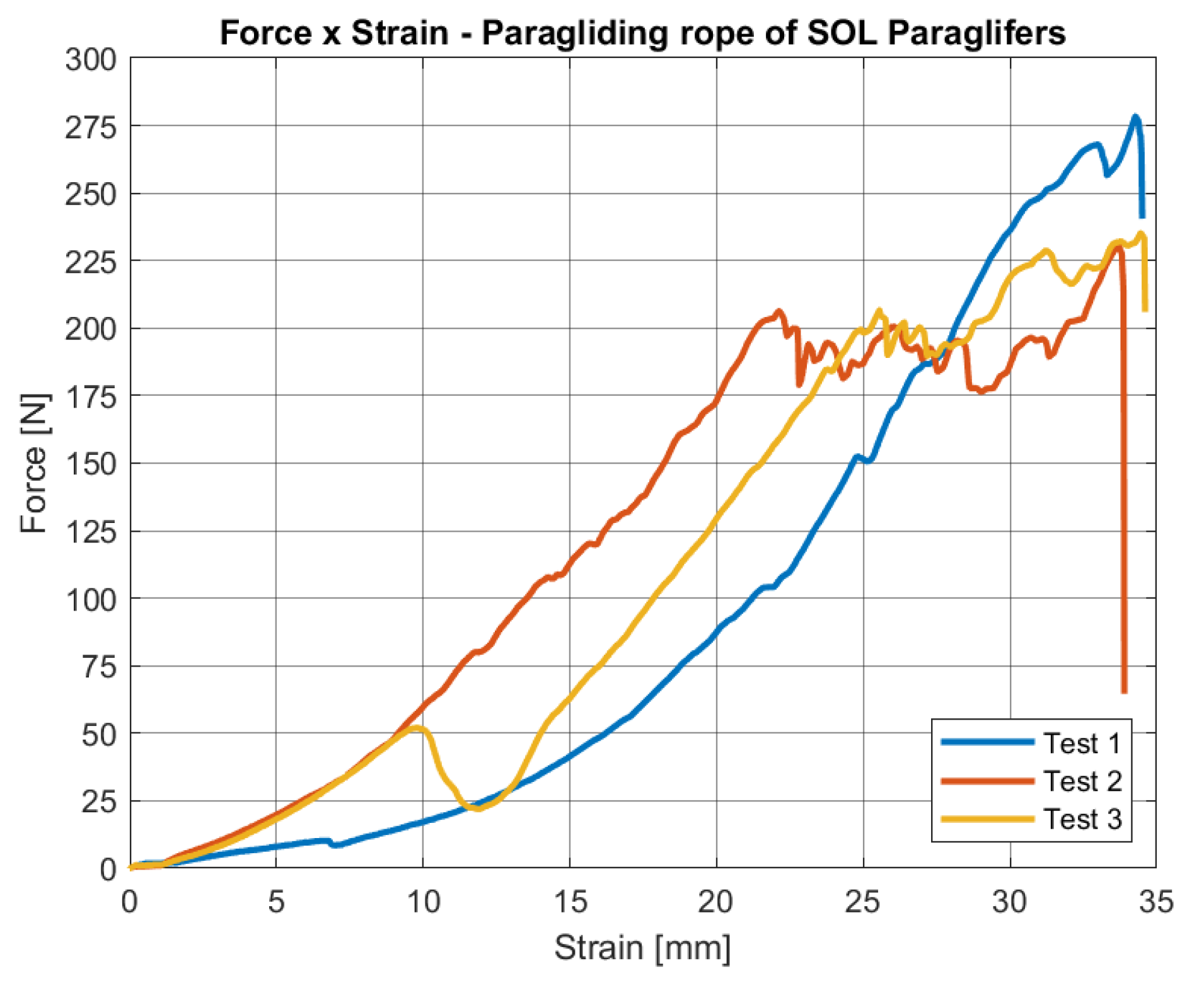
3.2. Tensile Strength Test
3.3. Pilot Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- GBD 2015 Neurological Disorders Collaborator Group. Global, regional, and national burden of neurological disorders during 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Neurol. 2017, 16, 877–897. [Google Scholar] [CrossRef]
- WHO. Health Statistics and Information Systems—Projections of Mortality and Causes of Death, 2015 and 2030. 2013. Available online: http://www.who.int/healthinfo/global_burden_disease/projections/em (accessed on 22 November 2018).
- WHO. The top 10 causes of death. 2014. Available online: http://www.who.int/mediacentre/factsheets/fs310/em (accessed on 22 November 2018).
- Royal College of Physicians. National Clinical Guidelines for Stroke, 5th ed.; Intercollegiate Stroke Working: London, UK, 2016. [Google Scholar]
- Mayo, N.E.; Wood-Dauphinee, S.; Côté, R.; Durcan, L.; Carlton, J. Activity, participation, and quality of life 6 months poststroke. Arch. Phys. Med. Rehabil. 2002, 83, 1035–1042. [Google Scholar] [CrossRef]
- O’Sullivan, S.B.; Schmitz, T.J. Physical Rehabilitation, 5th ed.; F.A. Davis Company: Philadelphia, PA, USA, 2006; p. 1383. [Google Scholar]
- Chang, K.V.; Wu, W.T.; Huang, K.C.; Han, D.S. Segmental body composition transitions in stroke patients: Trunks are different from extremities and strokes are as important as hemiparesis. Clin. Nutr. 2019. [Google Scholar] [CrossRef]
- Poli, P.; Morone, G.; Rosati, G.; Masiero, S. Robotic Technologies and Rehabilitation: New Tools for Stroke Patients’ Therapy. BioMed Res. Int. 2013, 2013, 1–8. [Google Scholar] [CrossRef]
- Liepert, J.; Uhde, I.; Graf, S.; Leidner, O.; Weiller, C. Motor cortex plasticity during forced-use therapy in stroke patients: A preliminary study. J. Neurol. 2001, 248, 315–321. [Google Scholar] [CrossRef]
- Maciejasz Pawełand Eschweiler, J.; Gerlach-Hahn, K.; Jansen-Troy, A.; Leonhardt, S.; Maciejasz, P.; Eschweiler, J.; Gerlach-Hahn, K.; Jansen-Troy, A.; Leonhardt, S. A survey on robotic devices for upper limb rehabilitation. J. NeuroEng. Rehabil. 2014, 11, 3. [Google Scholar] [CrossRef]
- Duret, C.; Grosmaire, A.G.; Krebs, H.I. Robot-Assisted Therapy in Upper Extremity Hemiparesis: Overview of an Evidence-Based Approach. Front. Neurol. 2019, 10. [Google Scholar] [CrossRef]
- Kwakkel, G.; Kollen, B.J.; Krebs, H.I. Effects of Robot-Assisted Therapy on Upper Limb Recovery After Stroke: A Systematic Review. Neurorehabil. Neural Repair 2008, 22, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Yozbatiran, N.; Francisco, G.E. Robot-assisted Therapy for the Upper Limb after Cervical Spinal Cord Injury. Phys. Med. Rehabil. Clin. North Am. 2019, 30, 367–384. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, F.M.R.M.; Chaves, M.E.A.; Oliveira, V.C.; Van Petten, A.M.V.N.; Vimieiro, C.B.S. Effectiveness of robot therapy on body function and structure in people with limited upper limb function: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0200330. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Pohl, M.; Platz, T.; Kugler, J.; Elsner, B. Electromechanical and robot-assisted arm training for improving activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef] [PubMed]
- Norouzi-Gheidari, N.; Archambault, P.S.; Fung, J. Effects of robot-assisted therapy on stroke rehabilitation in upper limbs: Systematic review and meta-analysis of the literature. J. Rehabil. Res. Develop. 2012, 49, 479. [Google Scholar] [CrossRef] [PubMed]
- Prange, G.B.; Jannink, M.J.A.; Groothuis-Oudshoorn, C.G.M.; Hermens, H.J.; IJzerman, M.J. Systematic review of the effect of robot-aided therapy on recovery of the hemiparetic arm after stroke. J. Rehabil. Res. Develop. 2006, 43, 171. [Google Scholar] [CrossRef] [PubMed]
- Veerbeek, J.M.; Langbroek-Amersfoort, A.C.; van Wegen, E.E.H.; Meskers, C.G.M.; Kwakkel, G. Effects of Robot-Assisted Therapy for the Upper Limb After Stroke. Neurorehabil. Neural Repair 2017, 31, 107–121. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Mukae, N.; Arata, J.; Iihara, K.; Hashizume, M. Comparison of Feature Vector Compositions to Enhance the Performance of NIRS-BCI-Triggered Robotic Hand Orthosis for Post-Stroke Motor Recovery. Appl. Sci. 2019, 9, 3845. [Google Scholar] [CrossRef]
- Krebs, H.; Hogan, N.; Aisen, M.; Volpe, B. Robot-aided neurorehabilitation. IEEE Trans. Rehabil. Eng. 1998, 6, 75–87. [Google Scholar] [CrossRef]
- Klamroth-Marganska, V.; Blanco, J.; Campen, K.; Curt, A.; Dietz, V.; Ettlin, T.; Felder, M.; Fellinghauer, B.; Guidali, M.; Kollmar, A.; et al. Three-dimensional, task-specific robot therapy of the arm after stroke: A multicentre, parallel-group randomised trial. Lancet Neurol. 2014, 13, 159–166. [Google Scholar] [CrossRef]
- Lum, P.; Burgar, C.; Van Der Loos, M.; Shor, P.; Majumbar, M.; Yap, R. MIME robotic device for upper-limb neurorehabilitation in subacute stroke subjects: A follow-up study. J. Rehabil. Res. Dev. 2006, 45, 631, 642. [Google Scholar] [CrossRef]
- Hesse, S.; Schulte-Tigges, G.; Konrad, M.; Bardeleben, A.; Werner, C. Robot-assisted arm trainer for the passive and active practice of bilateral forearm and wrist movements in hemiparetic subjects. Arch. Phys. Med. Rehabil. 2003, 84, 915–920. [Google Scholar] [CrossRef]
- Kahn, L.; Lum, P.; Rymer, W.; Reinkensmeyer, D. Robot-assisted movement training for the stroke-impaired arm: Does it matter what the robot does? J. Rehabil. Res. Dev. 2006, 43, 619–630. [Google Scholar] [CrossRef]
- Masiero, S.; Celia, A.; Rosati, G.; Armani, M.; Masieiro, S.; Celia, A.; Rosati, G.; Armani, M. Robotic-Assisted Rehabilitation of the Upper Limb After Acute Stroke. Arch. Phys. Med. Rehabil. 2007, 88, 142–149. [Google Scholar] [CrossRef]
- Araújo, R.C.D. Desenvolvimento e Avaliação de Sistema de Auxílio à Reabilitação Motora do Membro Superior Após Acidente VasculaR EncefáLico. Doctoral Dissertation, Universidade Federal de Minas Gerais, Belo Horizonte, MG, Brazil, 2011. [Google Scholar]
- Rúbio, G.P.; Ferreira, F.; de Lisboa Brandão, F.H.; Machado, V.; Tonelli, L.; Kozan, R.F.; Vimieiro, C. Design of Actuators Applied to a Upper Limb Orthosis. In Proceedings of the 25th International Congress of Mechanical Engineering, ABCM, Uberlandia, MG, Brazil, 20–25 October 2019. [Google Scholar] [CrossRef]
- Radder, B.; Prange-Lasonder, G.B.; Kottink, A.I.R.; Holmberg, J.; Sletta, K.; van Dijk, M.; Meyer, T.; Melendez-Calderon, A.; Buurke, J.H.; Rietman, J.S. Home rehabilitation supported by a wearable soft-robotic device for improving hand function in older adults: A pilot randomized controlled trial. PLoS ONE 2019, 14, e0220544. [Google Scholar] [CrossRef]
- Cherian, B.; Dominic, C.; G, V.; Vishakh, K.R. Exo-Glove: A Soft Wearable Robotic Hand for Stroke Survivors. Inte. Res. J. Eng. Technol. 2018, 5, 3358–3364. [Google Scholar]
- Xiloyannis, M.; Galli, L.; Chiaradia, D.; Frisoli, A.; Braghin, F.; Masia, L. A Soft Tendon-Driven Robotic Glove: Preliminary Evaluation. In Converging Clinical and Engineering Research on Neurorehabilitation III. ICNR 2018. Biosystems & Biorobotics; Masia, L., Micera, S., Akay, M., Pons, J.L., Eds.; Springer: Cham, Switzerland, 2019; pp. 329–333. [Google Scholar] [CrossRef]
- Xiloyannis, M.; Cappello, L.; Khanh, D.B.; Yen, S.C.; Masia, L. Modelling and design of a synergy-based actuator for a tendon-driven soft robotic glove. In Proceedings of the 2016 6th IEEE International Conference on Biomedical Robotics and Biomechatronics (BioRob), Singapore, 26–29 June 2016; pp. 1213–1219. [Google Scholar] [CrossRef]
- Yurkewich, A.; Hebert, D.; Wang, R.H.; Mihailidis, A. Hand Extension Robot Orthosis (HERO) Glove: Development and Testing With Stroke Survivors With Severe Hand Impairment. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 916–926. [Google Scholar] [CrossRef] [PubMed]
- Rocha, D.N. Desenvolvimento de um sistema de controle para a órtese funcional de mão da UFMG. Master’s Thesis, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil, 2007. [Google Scholar]
- Wechsler, L.R.; Bates, D.; Stroemer, P.; Andrews-Zwilling, Y.S.; Aizman, I. Cell Therapy for Chronic Stroke. Stroke 2018, 49, 1066–1074. [Google Scholar] [CrossRef] [PubMed]
- Freitas, P.P. Reabilitação da Mão, 1st ed.; Atheneu: São Paulo, Brazil, 2006; p. 578. [Google Scholar]
- Fugl-Meyer, A.; Jaasko, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient: 1. A method for evaluation of physical performance. Scand. J. Rehab. Med. 1975, 7, 13–31. [Google Scholar]
- Bohannon, R.W.; Smith, M.B. Interrater Reliability of a Modified Ashworth Scale of Muscle Spasticity. Phys. Ther. 1987, 67, 206–207. [Google Scholar] [CrossRef] [PubMed]
- Bertolucci, P.H.; Brucki, S.M.; Campacci, S.R.; Juliano, Y. O Mini-Exame do Estado Mental em uma população geral: Impacto da escolaridade. Arquivos de Neuro-Psiquiatria 1994, 52, 1–7. [Google Scholar] [CrossRef]
- Raghavan, P. Upper Limb Motor Impairment After Stroke. Phys. Med. Rehabil. Clin. North Am. 2015, 26, 599–610. [Google Scholar] [CrossRef]
- Thompson, A.J.; Jarrett, L.; Lockley, L.; Marsden, J.; Stevenson, V. Clinical management of spasticity. J. Neurol. Neurosurg. Psychiatry 2005, 76, 459–463. [Google Scholar] [CrossRef]
- Chagas, H.M.A. Determinação de valores de referência para a força de preensão palmar e força muscular respiratória em adultos saudáveis. Master’s Thesis, Universidade de São Paulo, São Paulo, Brazil, 2018. [Google Scholar]
- Bohannon, R. Muscle strength and muscle training after stroke. J. Rehabil. Med. 2007, 39, 14–20. [Google Scholar] [CrossRef]
- Wu, W.T.; Chang, K.V.; Mezian, K.; Naňka, O.; Lin, C.P.; Özçakar, L. Basis of Shoulder Nerve Entrapment Syndrome: An Ultrasonographic Study Exploring Factors Influencing Cross-Sectional Area of the Suprascapular Nerve. Front. Neurol. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.T.; Chang, K.V.; Mezian, K.; Naňka, O.; Yang, Y.C.; Hsu, Y.C.; Hsu, P.C.; Özçakar, L. Ulnar Wrist Pain Revisited: Ultrasound Diagnosis and Guided Injection for Triangular Fibrocartilage Complex Injuries. J. Clin. Med. 2019, 8, 1540. [Google Scholar] [CrossRef] [PubMed]
- Faria-Fortini, I.; Michaelsen, S.M.; Cassiano, J.G.; Teixeira-Salmela, L.F. Upper Extremity Function in Stroke Subjects: Relationships between the International Classification of Functioning, Disability, and Health Domains. J. Hand Ther. 2011, 24, 257–265. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | Sex | Age | Dominance | Post Stroke Time | Finger Spasticity Level * |
|---|---|---|---|---|---|
| 1 | Male | 73 | Right | 53 months | 1 |
| 2 | Male | 38 | Right | 113 months | 2 |
| 3 | Female | 25 | Left | 48 months | 2 |
| 4 | Female | 48 | Right | 24 months | 1 |
| Manufacturer | Product | Material | Diameter [mm] |
|---|---|---|---|
| D’Addarío | Guitar String | Brass | 0.64 |
| D (85/15) | |||
| D’Addarío | Guitar String | Brass | 0.23 |
| E (85/15) | |||
| D’Addarío | Guitar String | Brass | 0.30 |
| B (85/15) | |||
| D’Addarío | Guitar String | Brass | 0.89 |
| A (85/15) | |||
| D’Addarío | Guitar String | Brass | 0.38 |
| G (85/15) | |||
| D’Addarío | Guitar String | Brass | 1.14 |
| E (85/15) | |||
| TufLine XP | Fishing line | Spectra | 0.48 |
| SOL Paragliders | Paragliding rope | DuPont™ Kevlar | 1.00 |
| Participant | Measured | Average | Standard Deviation | |||
|---|---|---|---|---|---|---|
| Unaffected | Affected | Unaffected | Affected | Unaffected | Affected | |
| [kgf] | [kgf] | [kgf] | [kgf] | [kgf] | [kgf] | |
| 1 | 36 | 9 | 38.67 | 11.00 | 2.52 | 1.73 |
| 39 | 12 | |||||
| 41 | 12 | |||||
| 2 | 54 | 18 | 49 | 17.83 | 5 | 0.29 |
| 49 | 18 | |||||
| 44 | 17.5 | |||||
| 3 | 38 | 15 | 38.67 | 13.33 | 1.15 | 2.89 |
| 38 | 10 | |||||
| 40 | 15 | |||||
| 4 | 34.5 | 6 | 33.83 | 7.33 | 3.55 | 1.53 |
| 37 | 9 | |||||
| 30 | 7 | |||||
| Average | 40.04 | 12.38 | 6.45 | 4.28 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rúbio, G.d.P.; Martins Ferreira, F.M.R.; Brandão, F.H.d.L.; Machado, V.F.; Tonelli, L.G.; Martins, J.S.R.; Kozan, R.F.; Vimieiro, C.B.S. Evaluation of Commercial Ropes Applied as Artificial Tendons in Robotic Rehabilitation Orthoses. Appl. Sci. 2020, 10, 920. https://doi.org/10.3390/app10030920
Rúbio GdP, Martins Ferreira FMR, Brandão FHdL, Machado VF, Tonelli LG, Martins JSR, Kozan RF, Vimieiro CBS. Evaluation of Commercial Ropes Applied as Artificial Tendons in Robotic Rehabilitation Orthoses. Applied Sciences. 2020; 10(3):920. https://doi.org/10.3390/app10030920
Chicago/Turabian StyleRúbio, Guilherme de Paula, Fernanda Márcia Rodrigues Martins Ferreira, Fabrício Henrique de Lisboa Brandão, Victor Flausino Machado, Leandro Gonzaga Tonelli, Jordana Simões Ribeiro Martins, Renan Fernandes Kozan, and Claysson Bruno Santos Vimieiro. 2020. "Evaluation of Commercial Ropes Applied as Artificial Tendons in Robotic Rehabilitation Orthoses" Applied Sciences 10, no. 3: 920. https://doi.org/10.3390/app10030920
APA StyleRúbio, G. d. P., Martins Ferreira, F. M. R., Brandão, F. H. d. L., Machado, V. F., Tonelli, L. G., Martins, J. S. R., Kozan, R. F., & Vimieiro, C. B. S. (2020). Evaluation of Commercial Ropes Applied as Artificial Tendons in Robotic Rehabilitation Orthoses. Applied Sciences, 10(3), 920. https://doi.org/10.3390/app10030920