Pre-Cancerous Stomach Lesion Detections with Multispectral-Augmented Endoscopic Prototype

 ,
,  ,
,  and
and
Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Preclinical Study on Mice’s Stomach
| Algorithm 1: Pseudo code of the wavelengths clustering algorithm |
 |
| Algorithm 2: Classification pipeline |
 |
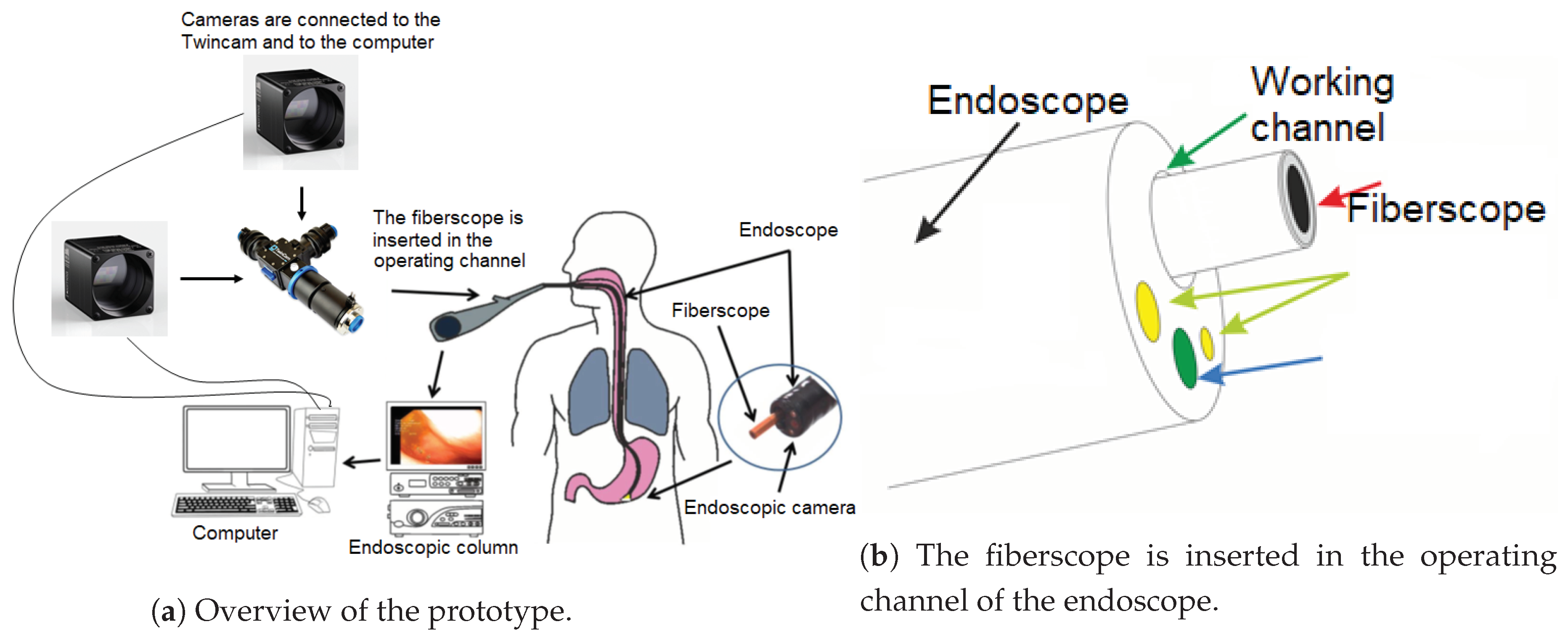
2.2. Description of the Prototype
2.3. Data Acquisition and Preprocessing
3. Results
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Bergman, J.J.; Goda, K.; Kato, M.; Messmann, H.; Alsop, B.R.; Gupta, N.; Vennalaganti, P.; Hall, M.; Konda, V.; et al. Development and validation of a classification system to identify high-grade dysplasia and esophageal adenocarcinoma in Barrett’s esophagus using narrow-band imaging. Gastroenterology 2016, 150, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Bansal, A.; Ulusarac, O.; Mathur, S.; Sharma, P. Correlation between narrow band imaging and nonneoplastic gastric pathology: A pilot feasibility trial. Gastrointest. Endosc. 2008, 67, 210–216. [Google Scholar] [CrossRef] [PubMed]
- FICE Fuji Intelligent Chromo Endoscopy. Available online: http://www.sfed.org/files/documents_sfed/partenaires/fujinon/pdf/fice.pdf (accessed on 27 May 2019).
- Burgos, H.; Porras, M.; Brenes, F.; Izquierdo, E. Fujinon FICE electronic chromovideoendoscopy helps differentiate the type of metaplasia in patients with chronic atrophic gastritis. Gastrointest. Endosc. 2007, 65, AB353. [Google Scholar] [CrossRef]
- Song, L.M.W.K.; Adler, D.G.; Conway, J.D.; Diehl, D.L.; Farraye, F.A.; Kantsevoy, S.V.; Kwon, R.; Mamula, P.; Rodriguez, B.; Shah, R.J.; et al. Narrow band imaging and multiband imaging. Gastrointest. Endosc. 2008, 67, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Weigt, J.; Malfertheiner, P.; Canbay, A.; Haybaeck, J.; Bird-Lieberman, E.; Link, A. Blue Light Imaging and Linked Color Imaging for the Characterization of Mucosal Changes in Chronic Gastritis: A Clinicians View and Brief Technical Report. Dig. Dis. 2020, 38, 9–14. [Google Scholar] [CrossRef]
- Dohi, O.; Yagi, N.; Onozawa, Y.; Kimura-Tsuchiya, R.; Majima, A.; Kitaichi, T.; Horii, Y.; Suzuki, K.; Tomie, A.; Okayama, T.; et al. Linked color imaging improves endoscopic diagnosis of active Helicobacter pylori infection. Endosc. Int. Open 2016, 4, E800–E805. [Google Scholar] [CrossRef]
- Gono, K. An Introduction to High-Resolution Endoscopy and Narrowband Imaging. In Comprehensive Atlas of High-Resolution Endoscopy and Narrowband Imaging; Wiley Online Library: Hoboken, NJ, USA, 2017; pp. 7–15. [Google Scholar]
- Bruno, M. Magnification endoscopy, high resolution endoscopy, and chromoscopy; towards a better optical diagnosis. Gut 2003, 52, iv7–iv11. [Google Scholar] [CrossRef]
- Uedo, N.; Ishihara, R.; Iishi, H.; Yamamoto, S.; Yamada, T.; Imanaka, K.; Takeuchi, Y.; Higashino, K.; Ishiguro, S.; Tatsuta, M. A new method of diagnosing gastric intestinal metaplasia: Narrow-band imaging with magnifying endoscopy. Endoscopy 2006, 38, 819–824. [Google Scholar] [CrossRef]
- Gu, X.; Yao, L.; Zhong, Y.; Han, Z.; Shi, Q.; Fu, Y.; Liu, C.; Wang, X.; Xie, T. Image enhancement based on in vivo hyperspectral gastroscopic images: A case study. J. Biomed. Opt. 2016, 21, 101412. [Google Scholar] [CrossRef]
- Kiyotoki, S.; Nishikawa, J.; Okamoto, T.; Hamabe, K.; Saito, M.; Goto, A.; Fujita, Y.; Hamamoto, Y.; Takeuchi, Y.; Satori, S.; et al. New method for detection of gastric cancer by hyperspectral imaging: A pilot study. J. Biomed. Opt. 2013, 18, 026010. [Google Scholar] [CrossRef] [PubMed]
- Hohmann, M.; Kanawade, R.; Klämpfl, F.; Douplik, A.; Mudter, J.; Neurath, M.; Albrecht, H. In-vivo multispectral video endoscopy towards in-vivo hyperspectral video endoscopy. J. Biophotonics 2017, 10, 553–564. [Google Scholar] [CrossRef] [PubMed]
- Makhlouf, H.; Gmitro, A.F.; Tanbakuchi, A.A.; Udovich, J.A.; Rouse, A.R. Multispectral confocal microendoscope for in vivo and in situ imaging. J. Biomed. Opt. 2008, 13, 044016. [Google Scholar] [CrossRef] [PubMed]
- Grosberg, L.E.; Radosevich, A.J.; Asfaha, S.; Wang, T.C.; Hillman, E.M. Spectral characterization and unmixing of intrinsic contrast in intact normal and diseased gastric tissues using hyperspectral two-photon microscopy. PLoS ONE 2011, 6, e19925. [Google Scholar] [CrossRef]
- Bergholt, M.S.; Zheng, W.; Ho, K.Y.; Teh, M.; Yeoh, K.G.; So, J.B.Y.; Shabbir, A.; Huang, Z. Fiber-optic Raman spectroscopy probes gastric carcinogenesis in vivo at endoscopy. J. Biophotonics 2013, 6, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Herrera, S.E.; Benezeth, Y.; Boffety, M.; Emile, J.F.; Marzani, F.; Lamarque, D.; Goudail, F. Multispectral endoscopy to identify precancerous lesions in gastric mucosa. In Proceedings of the International Conference on Image and Signal Processing, Cherburg, France, 30 June–2 July 2014; Springer: Berlin/Heidelberg, Germany, 2014; pp. 43–51. [Google Scholar]
- Reddymasu, S.C.; Sharma, P. Advances in endoscopic imaging of the esophagus. Gastroenterol. Clin. 2008, 37, 763–774. [Google Scholar] [CrossRef] [PubMed]
- Namikawa, T.; Sato, T.; Hanazaki, K. Recent advances in near-infrared fluorescence-guided imaging surgery using indocyanine green. Surg. Today 2015, 45, 1467–1474. [Google Scholar] [CrossRef]
- Li, Y.; Xie, X.; Yang, X.; Guo, L.; Liu, Z.; Zhao, X.; Luo, Y.; Jia, W.; Huang, F.; Zhu, S.; et al. Diagnosis of early gastric cancer based on fluorescence hyperspectral imaging technology combined with partial-least-square discriminant analysis and support vector machine. J. Biophotonics 2019, 12, e201800324. [Google Scholar] [CrossRef]
- Kobayashi, M.; Tajiri, H.; Seike, E.; Shitaya, M.; Tounou, S.; Mine, M.; Oba, K. Detection of early gastric cancer by a real-time autofluorescence imaging system. Cancer Lett. 2001, 165, 155–159. [Google Scholar] [CrossRef]
- Krebs, A.; Camilo, V.; Touati, E.; Benezeth, Y.; Michel, V.; Jouvion, G.; Yang, F.; Lamarque, D.; Marzani, F. Detection of H. pylori Induced Gastric Inflammation by Diffuse Reflectance Analysis. In Proceedings of the 18th International Conference on Bioinformatics and Bioengineering (BIBE), Taichung, Taiwan, 29–31 October 2018; pp. 287–292. [Google Scholar]
- Neuhauser, M. Nonparametric Statistical Tests: A Computational Approach; Chapman and Hall/CRC: Boca Raton, FL, USA, 2011. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- USB3 Vision Compliant Cameras-xiQ. Available online: https://www.ximea.com/en/products/usb3-vision-standard-designed-cameras-xiq (accessed on 27 May 2019).
- ITConcepts microFlex. Available online: http://www.itconceptsworld.com/index.html (accessed on 27 May 2019).
- TwinCam. Available online: https://www.cairn-research.co.uk/product/twincam/ (accessed on 25 May 2019).
- Zenteno, O.; Krebs, A.; Treuillet, S.; Lucas, Y.; Benezeth, Y.; Marzani, F. Spatial and Spectral Calibration of a Multispectral-Augmented Endoscopic Prototype. In Proceedings of the International Joint Conference on Computer Vision, Imaging and Computer Graphics, Funchal-Madeira, Portugal, 27–29 January 2018; Springer: Berlin/Heidelberg, Germany, 2018; pp. 262–280. [Google Scholar]
- Ximea API. Available online: https://www.ximea.com/support/wiki/apis/xiAPINET (accessed on 21 January 2020).
- Cetin, A.E.; Tofighi, M. Projection-based wavelet denoising [lecture notes]. Signal Process. Mag. 2015, 32, 120–124. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthy | Chronic Gastritis | Intestinal Metaplasia |
|---|---|---|
| 4 | 7 | 5 |
| Optimal Hyperparameter | Class | Precision | Recall | F1-Score | |
|---|---|---|---|---|---|
| Reduced Bands | c = 0.0001 k = 1 | Healthy | 0.98 | 1.00 | 0.99 |
| Chronic gastritis | 0.58 | 0.99 | 0.73 | ||
| Intestinal metaplasia | 0.00 | 0.00 | 0.00 | ||
| Average | 0.52 | 0.66 | 0.57 | ||
| Divisions | c = 0.0001 k = 1 | Healthy | 1.00 | 1.00 | 1.00 |
| Chronic gastritis | 0.58 | 1.00 | 0.74 | ||
| Intestinal metaplasia | 0.00 | 0.00 | 0.00 | ||
| Average | 0.53 | 0.67 | 0.58 | ||
| Subtractions | c = 0.0001 k = 1 | Healthy | 1.00 | 1.00 | 1.00 |
| Chronic gastritis | 0.58 | 1.00 | 0.74 | ||
| Intestinal metaplasia | 0.00 | 0.00 | 0.00 | ||
| Average | 0.53 | 0.67 | 0.58 |
| Optimal Hyperparameter | Class | Precision | Recall | F1-Score | |
|---|---|---|---|---|---|
| Reduced Bands | c = 0.001 k = 1 | Healthy | 0.88 | 0.51 | 0.64 |
| Chronic gastritis | 0.59 | 0.94 | 0.73 | ||
| Intestinal metaplasia | 0.73 | 0.37 | 0.49 | ||
| Average | 0.73 | 0.61 | 0.62 | ||
| Divisions | c = 0.001 k = 1 | Healthy | 0.87 | 0.56 | 0.68 |
| Chronic gastritis | 0.87 | 0.96 | 0.91 | ||
| Intestinal metaplasia | 0.69 | 0.78 | 0.73 | ||
| Average | 0.80 | 0.80 | 0.80 | ||
| Subtractions | c = 0.001 k = 1 | Healthy | 0.86 | 0.57 | 0.69 |
| Chronic gastritis | 0.86 | 0.96 | 0.91 | ||
| Intestinal metaplasia | 0.69 | 0.76 | 0.73 | ||
| Average | 0.80 | 0.77 | 0.77 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krebs, A.; Benezeth, Y.; Bazin, T.; Marzani, F.; Lamarque, D. Pre-Cancerous Stomach Lesion Detections with Multispectral-Augmented Endoscopic Prototype. Appl. Sci. 2020, 10, 795. https://doi.org/10.3390/app10030795
Krebs A, Benezeth Y, Bazin T, Marzani F, Lamarque D. Pre-Cancerous Stomach Lesion Detections with Multispectral-Augmented Endoscopic Prototype. Applied Sciences. 2020; 10(3):795. https://doi.org/10.3390/app10030795
Chicago/Turabian StyleKrebs, Alexandre, Yannick Benezeth, Thomas Bazin, Franck Marzani, and Dominique Lamarque. 2020. "Pre-Cancerous Stomach Lesion Detections with Multispectral-Augmented Endoscopic Prototype" Applied Sciences 10, no. 3: 795. https://doi.org/10.3390/app10030795
APA StyleKrebs, A., Benezeth, Y., Bazin, T., Marzani, F., & Lamarque, D. (2020). Pre-Cancerous Stomach Lesion Detections with Multispectral-Augmented Endoscopic Prototype. Applied Sciences, 10(3), 795. https://doi.org/10.3390/app10030795