Effect of Mat Pilates on Body Fluid Composition, Pelvic Stabilization, and Muscle Damage during Pregnancy



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Pilates Exercise Protocols
2.3. Pelvic Stabilization Muscle Strength Test
2.4. Body Composition
2.5. Blood Collection and Biochemical Analyses
2.6. Statistical Analysis
3. Results
3.1. Effect of Pilates on the Body Compositions and Lipid Profiles
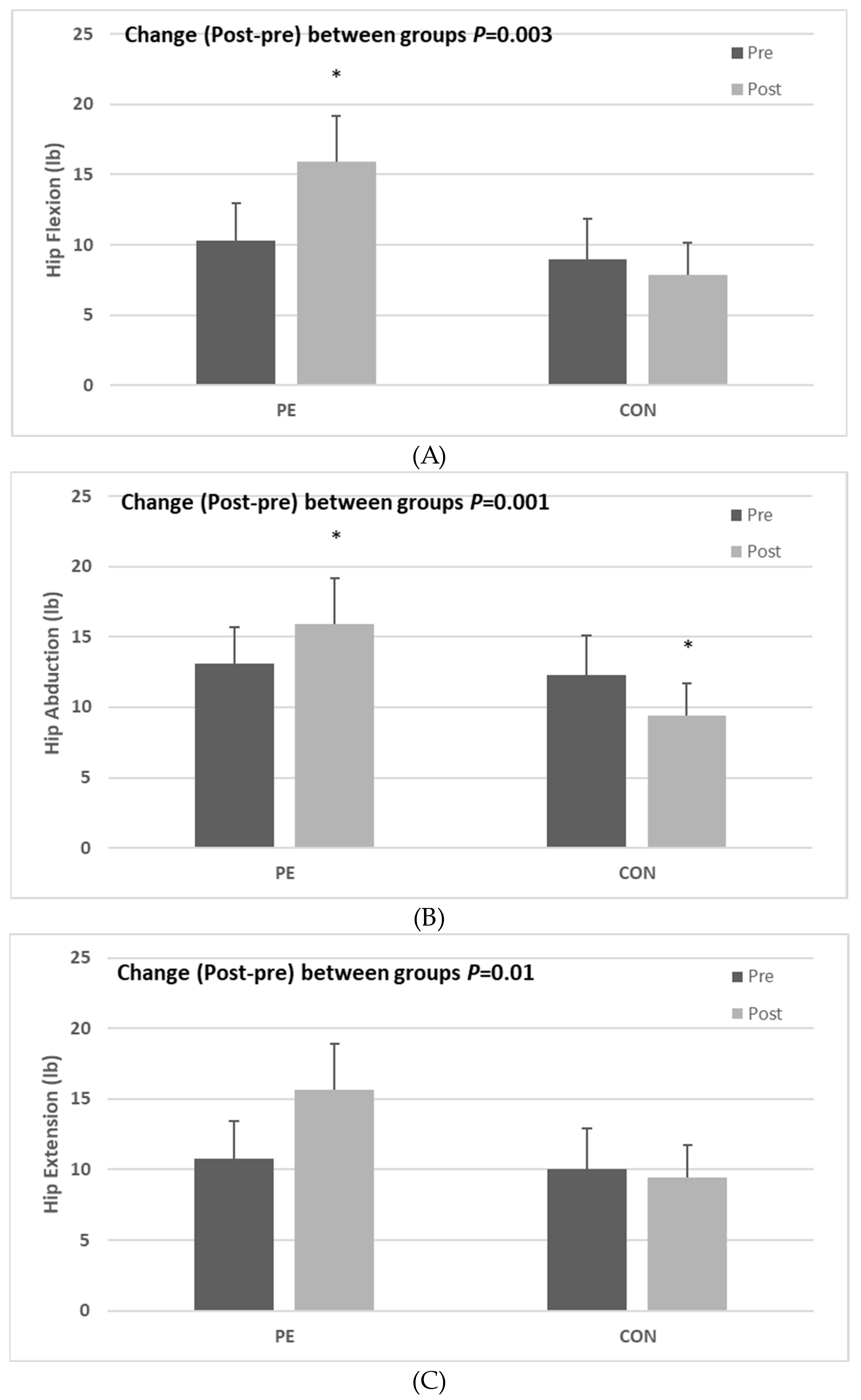
3.2. Effect of Pilates on the Pelvic Stabilization Muscle Strength
3.3. Muscle Damage and Stress Markers
4. Discussion
4.1. Effect of Pilates on Body Compositions and Lipid Profiles
4.2. Effect of Pilates on the Pelvic Stabilization Muscle Strength
4.3. Muscle Damage and Stress Markers
5. Conclusions
6. Ethics Approval and Informed Consent
Author Contributions
Funding
Conflicts of Interest
References
- Dastenaei, B.M.; Aein, F.; Safdari, F.; Karimiankakolaki, Z. Designing an intervention program over the effects of Pilates on pregnancy outcomes among the pregnant women: A protocol study. Int. J. Surg. Protoc. 2020, 24, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Santos-Rocha, R.; Branco, M.; Aguiar, L.; Vieira, F.; Veloso, A.P. Biomechanical Adaptations of Gait in Pregnancy: Implications for Physical Activity and Exercise. In Exercise and Sporting Activity During Pregnancy; Springer: Cham, Switzerland, 2019; pp. 95–134. [Google Scholar] [CrossRef]
- Güder, D.S.; Yalvaç, M.; Vural, G. The effect of pregnancy Pilates-assisted childbirth preparation training on childbirth fear and neonatal outcomes: A quasi-experimental/quantitative research. Qual. Quant. 2018, 52, 2667–2679. [Google Scholar] [CrossRef]
- Barakat, R.; Pelaez, M.; Cordero, Y.; Perales, M.; Lopez, C.; Coteron, J.; Mottola, M.F. Exercise during pregnancy protects against hypertension and macrosomia: Randomized clinical trial. Am. J. Obs. Gynecol. 2016, 214, 649.e1–649.e8. [Google Scholar] [CrossRef] [PubMed]
- Coll, C.D.V.N.; Domingues, M.R.; Stein, A.; Da Silva, B.G.C.; Bassani, D.G.; Hartwig, F.P.; Da Silva, I.C.M.; Da Silveira, M.F.; Da Silva, S.G.; Bertoldi, A.D. Efficacy of regular exercise during pregnancy on the prevention of postpartum depression: The PAMELA randomized clinical trial. JAMA Netw. Open 2019, 2, e186861. [Google Scholar] [CrossRef] [PubMed]
- Virgara, R.; Maher, C.; Van Kessel, G. The comorbidity of low back pelvic pain and risk of depression and anxiety in pregnancy in primiparous women. BMC Pregnancy Childbirth 2018, 18, 288. [Google Scholar] [CrossRef] [PubMed]
- Cakmak, B.; Inanir, A.; Nacar, M.C.; Filiz, B. The effect of maternity support belts on postural balance in pregnancy. PM&R 2014, 6, 624–628. [Google Scholar] [CrossRef]
- O’Hair, B.C.M.; Armstrong, M.K.; Rutherford, H.J. The potential utility for massage therapy during pregnancy to decrease stress and tobacco use. Int. J. Massage Bodyw. Res. Educ. Pract. 2018, 11, 15–19. [Google Scholar] [CrossRef]
- Mparmpakas, D.; Goumenou, A.; Zachariades, E.; Pados, G.; Gidron, Y.; Karteris, E. Immune system function, stress, exercise and nutrition profile can affect pregnancy outcome: Lessons from a Mediterranean cohort. Exp. Med. 2013, 5, 411–418. [Google Scholar] [CrossRef]
- Van Willenswaard, K.C.; Lynn, F.; McNeill, J.; McQueen, K.; Dennis, C.-L.; Lobel, M.; Alderdice, F. Music interventions to reduce stress and anxiety in pregnancy: A systematic review and meta-analysis. BMC Psychiatry 2017, 17, 271. [Google Scholar] [CrossRef]
- Schmidt, F.M.D.; Fiorini, G.P.; Ramires, V.R.R. Psychoanalytic psychotherapy and the pregnant therapist: A literature review. Res. Psychother. Psychopathol. Process. Outcome 2015, 18. [Google Scholar] [CrossRef]
- Khafagy, G.M.; Gamal, M.G.; El-Rafie, M.M. Effect of aerobic exercise during pregnancy on antenatal depression. Int. J. Womens Health 2016, 8, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Marchand, A.-A.; Mottola, M.F.; Poitras, V.J.; E Gray, C.; Garcia, A.J.; Barrowman, N.; Sobierajski, F.; James, M.; Meah, V.L.; et al. Exercise for the prevention and treatment of low back, pelvic girdle and lumbopelvic pain during pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Fieril, K.P.; Glantz, A.; Olsén, M.F. The efficacy of moderate-to-vigorous resistance exercise during pregnancy: A randomized controlled trial. Acta Obs. Gynecol. Scand. 2015, 94, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Perales, M.; Santos-Lozano, A.; Ruiz, J.R.; Lucia, A.; Barakat, R. Benefits of aerobic or resistance training during pregnancy on maternal health and perinatal outcomes: A systematic review. Early Hum. Dev. 2016, 94, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, S.L.; Surita, F.G.; Godoy, A.C.; Kasawara, K.T.; Morais, S.S. Physical activity patterns and factors related to exercise during pregnancy: A cross sectional study. PLoS ONE 2015, 10, e0128953. [Google Scholar] [CrossRef]
- Muller, A.; Hammill, H.V.; Hermann, C. The effects of Pilates and progressive muscle relaxation therapy on maternal stress and anxiety: A literature review. Int. J. Humanit. Soc. Sci. 2016, 6, 195–203. [Google Scholar]
- Hyun, A.-H.; Cho, J.-Y. Effects of 12-weeks Pilates mat exercise on body composition, delivery confidence, and neck disability index in pregnant women. Sports Sci. 2019, 36, 43–55. [Google Scholar] [CrossRef]
- Wells, C.; Kolt, G.S.; Bialocerkowski, A. Defining Pilates exercise: A systematic review. Complement. Med. 2012, 20, 253–262. [Google Scholar] [CrossRef]
- Patti, A.; Bianco, A.; Paoli, A.; Messina, G.; Montalto, M.-A.; Bellafiore, M.; Battaglia, G.; Iovane, A.; Palma, A. Effects of Pilates exercise programs in people with chronic low back pain: A systematic review. Medicine 2015, 94, e383. [Google Scholar] [CrossRef]
- Cruz-Ferreira, A.; Fernandes, J.; Kuo, Y.-L.; Bernardo, L.M.; Fernandes, O.; Laranjo, L.; Silva, A. Does Pilates-based exercise improve postural alignment in adult women? Women Health 2013, 53, 597–611. [Google Scholar] [CrossRef]
- Panhan, A.C.; Gonçalves, M.; Eltz, G.D.; Villalba, M.M.; Cardozo, A.C.; Bérzin, F. Neuromuscular efficiency of the multifidus muscle in pilates practitioners and non-practitioners. Complement. Med. 2018, 40, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Fayh, A.; Brodt, G.A.; Souza, C.; Loss, J.F. Pilates instruction affects stability and muscle recruitment during the long stretch exercise. J. Bodyw. Mov. Ther. 2018, 22, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Xiao, X. The role of gut microbiota in the effects of maternal obesity during pregnancy on offspring metabolism. Biosci. Rep. 2018, 27, 38. [Google Scholar] [CrossRef] [PubMed]
- Mazzarino, M.; Kerr, D.; Morris, M.E. Pilates program design and health benefits for pregnant women: A practitioners’ survey. J. Bodyw. Mov. Ther. 2018, 22, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.C.; Alvares,, R.F.; Nascimento, T.R.; Paranaiba, S.S.W.; Da Silva-Morais, T.K. Pilates for pregnant women: A healthy alternative. J. Womens Health Care 2017, 6, 2167. [Google Scholar] [CrossRef]
- Bo, K.; Herbert, R.D. There is not yet strong evidence that exercise regimens other than pelvic floor muscle training can reduce stress urinary incontinence in women: A systematic review. J. Physiother. 2013, 59, 159–168. [Google Scholar] [CrossRef]
- Coleman, T.J.; Nygaard, I.E.; Holder, D.N.; Egger, M.J.; Hitchcock, R. Intra-abdominal pressure during Pilates: Unlikely to cause pelvic floor harm. Int. Urogynecol. J. 2015, 26, 1123–1130. [Google Scholar] [CrossRef]
- Mazzarino, M.; Kerr, D.; Wajswelner, H.; Morris, M.E. Pilates Method for Women’s Health: Systematic Review of Randomized Controlled Trials. Arch. Phys. Med. Rehabil. 2015, 96, 2231–2242. [Google Scholar] [CrossRef]
- Kim, H.-J.; Kim, J.; Kim, C.S. The effects of Pilates exercise on lipid metabolism and inflammatory cytokines mRNA expression in female undergraduates. J. Exerc. Nutr. Biochem. 2014, 18, 267–275. [Google Scholar] [CrossRef]
- Horjus, D.L.; Bokslag, A.; Hutten, B.A.; Born, B.-J.H.V.D.; Middeldorp, S.; Vrijkotte, T.G. Creatine kinase is associated with blood pressure during pregnancy. J. Hypertens. 2019, 37, 1467–1474. [Google Scholar] [CrossRef]
- Pedersen, E.S.; Tengesdal, S.; Radtke, M.; Langlo, K.A.R.; Radke, M.; Rise, K.A.L. Major increase in creatine kinase after intensive exercise. Tidsskrift for den Norske Laegeforening: Tidsskrift for Praktisk Medicin, ny Raekke 2019, 139. [Google Scholar] [CrossRef]
- Dos Santos, J.M.; Filho, L.F.S.; Carvalho, V.O.; Wichi, R.B.; De Oliveira, E.D. Hemodynamic and creatine kinase changes after a 12-week equipment-based Pilates. A training program in hypertensive women. J. Bodyw. Mov. Ther. 2020, 24, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Ha, M.-S.; Baek, Y.-H.; Kim, J.-W.; Kim, D.-Y. Effects of yoga exercise on maximum oxygen uptake, cortisol level, and creatine kinase myocardial bond activity in female patients with skeletal muscle pain syndrome. J. Phys. Sci. 2015, 27, 1451–1453. [Google Scholar] [CrossRef] [PubMed]
- ACOG. Physical activity and exercise during pregnancy and the postpartum period: ACOG Committee Opinion No. 650. Obstet. Gynecol. 2015, 126, e1326–e1327. [Google Scholar] [CrossRef] [PubMed]
- De Groot, M.; Pool-Goudzwaard, A.; Spoor, C.; Snijders, C. The active straight leg raising test (ASLR) in pregnant women: Differences in muscle activity and force between patients and healthy subjects. Man Ther. 2008, 13, 68–74. [Google Scholar] [CrossRef]
- Amirsasan, R.; Dolgarisharaf, R. Pilates training preventive effects of metabolic syndrome in sedentary overweight females. Int. J. Sport Stud. 2015, 5, 596–602. [Google Scholar]
- Levario-Carrillo, M.; Avitia, M.; Tufiño-Olivares, E.; Trevizo, E.; Corral-Terrazas, M.; Reza-López, S. Body composition of patients with hypertensive complications during pregnancy. Hypertens. Pregnancy 2006, 25, 259–269. [Google Scholar] [CrossRef]
- Duvekot, J.J.; Peeters, L.L. Maternal cardiovascular hemodynamic adaptation to pregnancy. Obs. Gynecol. Surv. 1994, 49, S1–S14. [Google Scholar] [CrossRef]
- Staelens, A.S.; Vonck, S.; Molenberghs, G.; Malbrain, M.L.; Gyselaers, W. Maternal body fluid composition in uncomplicated pregnancies and preeclampsia: A bioelectrical impedance analysis. Eur. J. Obs. Gynecol. Reprod. Biol. 2016, 204, 69–73. [Google Scholar] [CrossRef]
- Ergun, M.; Eyigor, S.; Karaca, B.; Kisim, A.; Uslu, R. Effects of exercise on angiogenesis and apoptosis-related molecules, quality of life, fatigue and depression in breast cancer patients. Eur. J. Cancer Care 2013, 22, 626–637. [Google Scholar] [CrossRef]
- Yoshida, T.; Yamada, Y.; Tanaka, F.; Yamagishi, T.; Shibata, S.; Kawakami, Y. Intracellular-to-total water ratio explains the variability of muscle strength dependence on the size of the lower leg in the elderly. Exp. Gerontol. 2018, 113, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.T.; Oh, H.O.; Han, H.S.; Jin, K.Y.; Roh, H.L. Effect of mat pilates exercise on postural alignment and body composition of middle-aged women. J. Phys. Sci. 2016, 28, 1691–1695. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, L.C.S.; Bertolini, S.M.M.G.; Bennemann, R.M.; Silva, E.S. The effect Mat Pilates practice on muscle mass in elderly women. Rev. Rene 2016, 17, 618. [Google Scholar] [CrossRef]
- Magro-Malosso, E.R.; Saccone, G.; Di Mascio, D.; Di Tommaso, M.; Berghella, V. Exercise during pregnancy and risk of preterm birth in overweight and obese women: A systematic review and meta-analysis of randomized controlled trials. Acta Obs. Gynecol. Scand. 2017, 96, 263–273. [Google Scholar] [CrossRef]
- Pavithralochani, V.; Thangavignesh, R.; Saranya, P.; Ramanathan, K. Efficacy of Kegel’s Exercise vs Pilates in Subject with Urinary Incontinence during Pregnancy. Res. J. Pharm. Technol. 2019, 12, 5943. [Google Scholar] [CrossRef]
- Du, M.; Ouyang, Y.-Q.; Nie, X.; Huang, Y.; Redding, S.R. Effects of physical exercise during pregnancy on maternal and infant outcomes in overweight and obese pregnant women: A meta-analysis. Birth 2018, 46, 211–221. [Google Scholar] [CrossRef]
- Fatemeh, N.; Sepidarkish, M.; Shirvani, M.A.; Habibipour, P.; Tabari, N.S.M. The effect of exercise on the prevention of gestational diabetes in obese and overweight pregnant women: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2019, 11, 72. [Google Scholar]
- Bogaert, J.; Stack, M.; Partington, S.; Marceca, J.; Tremback-Ball, A. The effects of stabilization exercise on low back pain and pelvic girdle pain in pregnant women. Ann. Phys. Rehabil. Med. 2018, 61, e157–e158. [Google Scholar] [CrossRef]
- Pascoal, G.A.; Stuge, B.; Mota, P.; Hilde, G.; Bø, K. Therapeutic Exercise Regarding Musculoskeletal Health of the Pregnant Exerciser and Athlete. In Exercise and Sporting Activity During Pregnancy; Springer Science and Business Media LLC: Berlin, Germany, 2019; pp. 309–326. [Google Scholar]
- Rodríguez-Díaz, L.; Ruiz-Frutos, C.; Vázquez-Lara, J.M.; Ramírez-Rodrigo, J.; Villaverde-Gutiérrez, C.; Torres-Luque, G. Effectiveness of a physical activity programme based on the Pilates method in pregnancy and labour. Enferm. Clín. 2017, 27, 271–277. [Google Scholar] [CrossRef]
- Oktaviani, I. Pilates workouts can reduce pain in pregnant women. Complement. Clin. Pract. 2018, 31, 349–351. [Google Scholar] [CrossRef]
- Phrompaet, S.; Paungmali, A.; Pirunsan, U.; Sitilertpisan, P. Effects of Pilates training on lumbo-pelvic stability and flexibility. Asian J. Sports Med. 2011, 2, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Silva, G.B.; Morgan, M.M.; De Carvalho, W.R.G.; Da Silva, E.F.; De Freitas, W.Z.; Da Silva, F.F.; De Souza, R.A. Electromyographic activity of rectus abdominis muscles during dynamic Pilates abdominal exercises. J. Bodyw. Mov. Ther. 2015, 19, 629–635. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, P.B.; Beales, D.J.; Beetham, J.A.; Cripps, J.; Graf, F.; Lin, I.B.; Tucker, B.; Avery, A. Altered motor control strategies in subjects with sacroiliac joint pain during the active straight-leg-raise test. Spine 2002, 27, E1–E8. [Google Scholar] [CrossRef] [PubMed]
- Gaillard, R.; Rifas-Shiman, S.L.; Perng, W.; Oken, E.; Gillman, M.W. Maternal inflammation during pregnancy and childhood adiposity. Obesity 2016, 24, 1320–1327. [Google Scholar] [CrossRef]
- Lindsay, K.L.; Buss, C.; Wadhwa, P.D.; Entringer, S. The Interactive Effects of Maternal Stress and Diet in Pregnancy on Markers of Inflammation; Institute for Clinical and Translational Science: Iowa City, IA, USA, 2018. [Google Scholar]
- Withee, E.D.; Tippens, K.M.; Dehen, R.; Tibbitts, D.; Hanes, D.; Zwickey, H. Effects of Methylsulfonylmethane (MSM) on exercise-induced oxidative stress, muscle damage, and pain following a half-marathon: A double-blind, randomized, placebo-controlled trial. J. Int. Soc. Sports Nutr. 2017, 14, 24. [Google Scholar] [CrossRef]
- Liu, Y.; Zhao, P.; Cheng, M.; Yu, L.; Cheng, Z.; Fan, L.; Chen, C. AST to ALT ratio and arterial stiffness in non-fatty liver Japanese population:a secondary analysis based on a cross-sectional study. Lipids Health Dis. 2018, 17, 275. [Google Scholar] [CrossRef]
- Pal, S.; Chaki, B.; Chattopadhyay, S.; Bandyopadhyay, A. High-Intensity exercise induced oxidative stress and skeletal muscle damage in postpubertal boys and girls: A comparative study. J. Strength Cond. Res. 2018, 32, 1045–1052. [Google Scholar] [CrossRef]
- Mannaerts, D.; Faes, E.; Cos, P.; Briedé, J.J.; Gyselaers, W.; Cornette, J.; Gorbanev, Y.; Bogaerts, A.; Spaanderman, M.; Van Craenenbroeck, E.; et al. Oxidative stress in healthy pregnancy and preeclampsia is linked to chronic inflammation, iron status and vascular function. PLoS ONE 2018, 13, e0202919. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Modes | Week | Contents | Time (min) | Reps, Set, and Rest | RPE |
|---|---|---|---|---|---|
| Warm-up | 1–12 | (Breathing · Static Stretching) Neck and Shoulder Stretch, Deep Breathing Leg Stretch | 10 | 9 | |
| Main Exercise | 1–6 (Level 1) | Torso Twist, Cat Cow, Kneeling Half Push-up Lying One-Leg Circles One-Leg Side Kick, Pelvic Stretch | 30 | 8~12 reps × 3 set 20 s rest between sets | 9~11 |
| 7–12 (Level 2) | Spine Stretch, Double-Arm Circles Half Roll Down and Up, One-Leg Side Rotation Lying Leg Scissors, Donkey Kick | 30 | 8~12 reps × 3 set 30 s rest between sets | 12~13 | |
| Cool-down | 1–12 | (Breathing · Static Stretching) Neck and Shoulder Stretch Deep Breathing | 10 | 9 |
| Pilates (n = 9) | CON (n = 7) | Diff (Post-Pre) | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | z | p | Cohen’s r | |
| BW (kg) | 57.98 ± 7.91 | 64.01 ± 7.76 ** | 53.67 ± 5.70 | 58.37 ± 5.65 * | −1.590 | 0.112 | 0.398 |
| TBW (L) # | 28.97 ± 3.33 | 31.59 ± 3.50 ** | 27.63 ± 2.45 | 29.26 ± 2.84 * | −2.286 | 0.022 | 0.572 |
| ICW (L) ## | 17.71 ± 2.06 | 19.54 ± 2.12 ** | 16.90 ± 1.54 | 17.99 ± 1.66 * | −2.818 | 0.005 | 0.705 |
| ECW (L) | 11.26 ± 1.28 | 12.04 ± 1.39 ** | 10.73 ± 0.92 | 11.27 ± 1.18 * | −1.232 | 0.218 | 0.308 |
| ECW/ICW ratio # | 0.64 ± 0.01 | 0.62 ± 0.01 * | 0.64 ± 0.01 | 0.63 ± 0.01 | −2.170 | 0.030 | 0.543 |
| BFM (kg) | 18.40 ± 4.92 | 20.70 ± 5.04 ** | 15.86 ± 3.06 | 18.30 ± 3.06 * | −0.106 | 0.916 | 0.027 |
| PBF (%) | 22.50 ± 3.15 | 24.84 ± 3.02 ** | 20.59 ± 1.64 | 22.41 ± 1.67 * | −1.643 | 0.100 | 0.411 |
| SMM (kg) ## | 21.10 ± 2.66 | 23.49 ± 2.76 ** | 20.09 ± 2.00 | 21.41 ± 2.18 * | −2.811 | 0.005 | 0.703 |
| Pilates (n = 9) | CON (n = 7) | Diff (Post-Pre) | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | z | p | Cohen’s r | |
| TG (kg) | 140.67 ± 35.25 | 201.56 ± 54.24 ** | 141.00 ± 38.59 | 205.86 ± 48.46 * | −0.106 | 0.916 | 0.027 |
| TC (mg/dL) | 220.33 ± 27.00 | 236.56 ± 25.93 * | 222.14 ± 28.54 | 248.29 ± 38.10 * | −1.059 | 0.289 | 0.265 |
| HDL (mg/dL) | 92.56 ± 11.67 | 90.11 ± 12.67 | 89.57 ± 13.62 | 85.00 ± 18.91 | −0.638 | 0.524 | 0.160 |
| LDL (mg/dL) | 110.67 ± 26.17 | 135.78 ± 25.25 * | 115.00 ± 18.06 | 152.00 ± 31.25 * | −1.272 | 0.203 | 0.318 |
| HbA1c (%) | 4.91 ± 0.18 | 5.13 ± 0.21 * | 4.91 ± 0.15 | 5.14 ± 0.15 * | −0.108 | 0.914 | 0.027 |
| Ferritin (ng/mL) | 55.44 ± 49.27 | 23.11 ± 11.41 * | 34.14 ± 6.72 | 16.57 ± 8.89 * | −0.530 | 0.596 | 0.133 |
| Pilates (n = 9) | CON (n = 7) | Diff (Post − Pre) | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | z | p | Cohen’s r | |
| CK (U/L) | 34.78 ± 8.66 | 42.22 ± 13.15 | 39.57 ± 16.06 | 59.43 ± 27.72 ** | −1.700 | 0.089 | 0.425 |
| LDH (U/L) ## | 159.00 ± 15.67 | 159.78 ± 15.09 | 162.29 ± 21.40 | 186.57 ± 26.79 ** | −2.603 | 0.009 | 0.651 |
| AST (U/L) # | 20.22 ± 6.32 | 17.78 ± 5.02 | 14.71 ± 4.11 | 16.29 ± 4.03 * | −2.566 | 0.010 | 0.642 |
| CRP (mg/L) | 0.25 ± 0.20 | 0.24 ± 0.23 | 0.10 ± 0.07 | 0.10 ± 0.06 | −1.230 | 0.219 | 0.308 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hyun, A.-H.; Jeon, Y.-J. Effect of Mat Pilates on Body Fluid Composition, Pelvic Stabilization, and Muscle Damage during Pregnancy. Appl. Sci. 2020, 10, 9111. https://doi.org/10.3390/app10249111
Hyun A-H, Jeon Y-J. Effect of Mat Pilates on Body Fluid Composition, Pelvic Stabilization, and Muscle Damage during Pregnancy. Applied Sciences. 2020; 10(24):9111. https://doi.org/10.3390/app10249111
Chicago/Turabian StyleHyun, Ah-Hyun, and Yoo-Jeong Jeon. 2020. "Effect of Mat Pilates on Body Fluid Composition, Pelvic Stabilization, and Muscle Damage during Pregnancy" Applied Sciences 10, no. 24: 9111. https://doi.org/10.3390/app10249111
APA StyleHyun, A.-H., & Jeon, Y.-J. (2020). Effect of Mat Pilates on Body Fluid Composition, Pelvic Stabilization, and Muscle Damage during Pregnancy. Applied Sciences, 10(24), 9111. https://doi.org/10.3390/app10249111