Association of Neutrophil to Lymphocyte Ratio with Patient Reported Outcomes in Knee Osteoarthritis

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
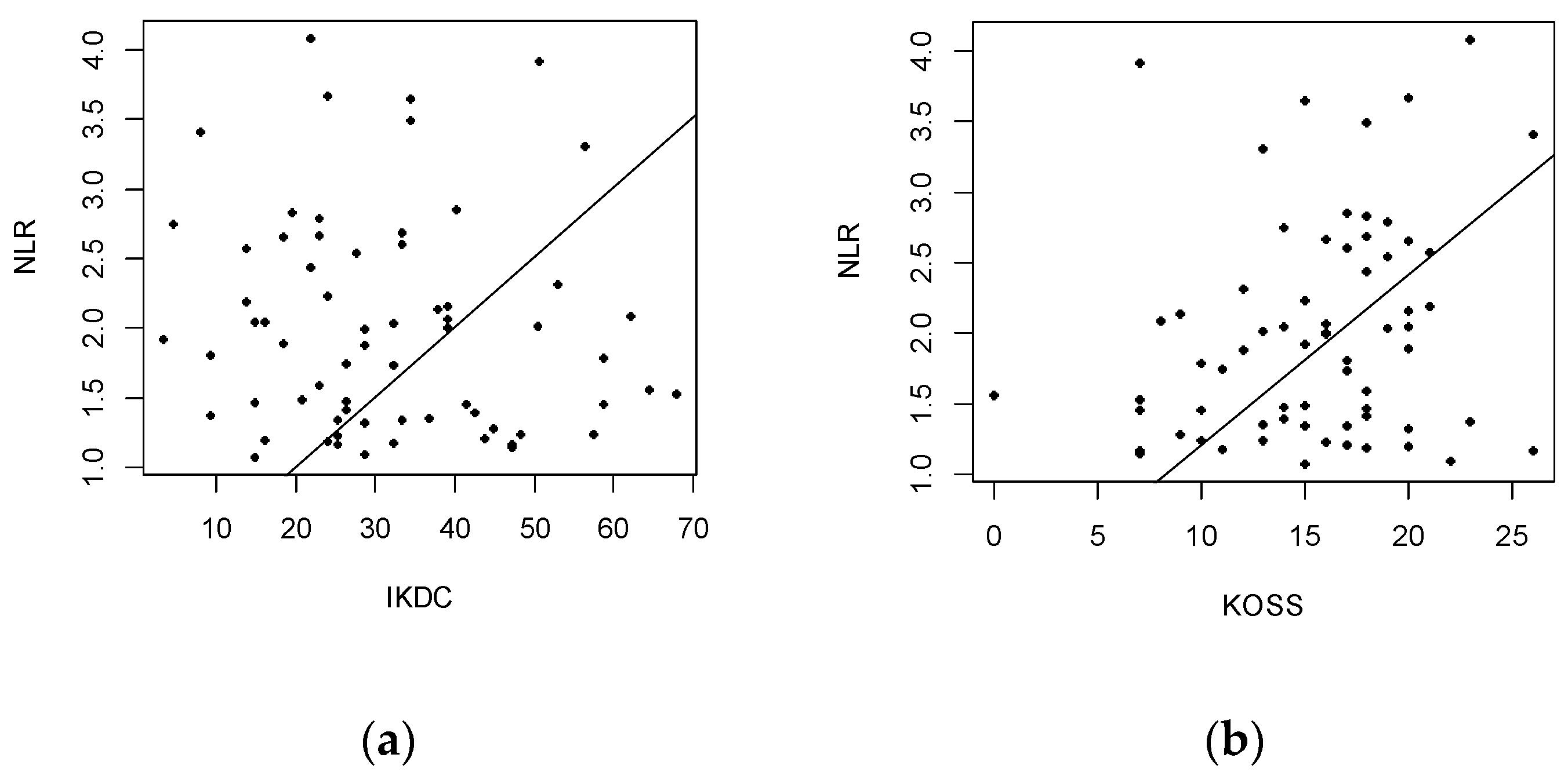
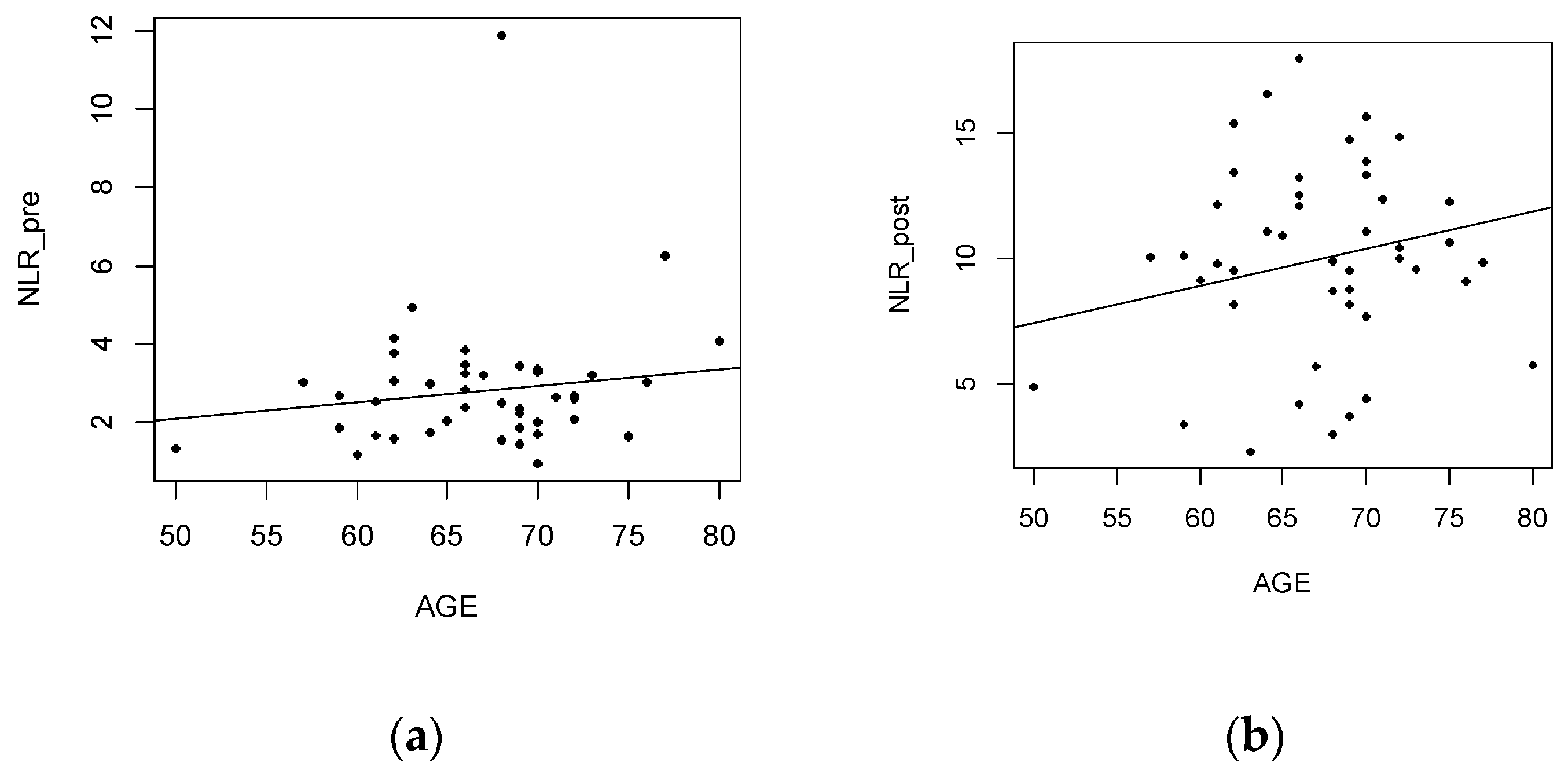
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Wilson, I.; Bohm, E.; Lübbeke, A.; Lyman, S.; Overgaard, S.; Rolfson, O.; W-Dahl, A.; Wilkinson, M.; Dunbar, M. Orthopaedic registries with patient-reported outcome measures. EFORT Open Rev. 2019, 4, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Emery, C.A.; Whittaker, J.L.; Mahmoudian, A.; Lohmander, L.S.; Roos, E.M.; Bennell, K.L.; Toomey, C.M.; Reimer, R.A.; Thompson, D.; Ronsky, J.L.; et al. Establishing outcome measures in early knee osteoarthritis. Nat. Rev. Rheumatol. 2019, 15, 438–448. [Google Scholar] [CrossRef] [PubMed]
- Boehme, K.A.; Rolauffs, B. Onset and Progression of Human Osteoarthritis-Can Growth Factors, Inflammatory Cytokines, or Differential miRNA Expression Concomitantly Induce Proliferation, ECM Degradation, and Inflammation in Articular Cartilage? Int. J. Mol. Sci. 2018, 19, 2282. [Google Scholar] [CrossRef] [PubMed]
- Tateiwa, D.; Yoshikawa, H.; Kaito, T. Cartilage and Bone Destruction in Arthritis: Pathogenesis and Treatment Strategy: A Literature Review. Cells 2019, 8, 818. [Google Scholar] [CrossRef] [PubMed]
- Nees, T.A.; Rosshirt, N.; Zhang, J.A.; Reiner, T.; Sorbi, R.; Tripel, E.; Walker, T.; Schiltenwolf, M.; Hagmann, S.; Moradi, B. Synovial Cytokines Significantly Correlate with Osteoarthritis-Related Knee Pain and Disability: Inflammatory Mediators of Potential Clinical Relevance. J. Clin. Med. 2019, 8, 1343. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Bai, N.; Hu, X.; OuYang, X.W.; Yao, L.; Tao, Y.; Wang, Z. Preoperative inflammatory markers of NLR and PLR as indicators of poor prognosis in resectable HCC. PeerJ 2019, 7, e7132. [Google Scholar] [CrossRef]
- Filh, J.G.M.S.; Torres, D.D.O.C.; Da Silva, M.C.F.C.; Martins, C.M.D.H.; Da Silva, I.K.; Nascimento, M.E.M.D.; Dos Santos, A.C.O.; Montarroyos, U.R.; Filho, D.C.S. Prognostic value of hematological parameters in patients with acute myocardial infarction: Intrahospital outcomes. PLoS ONE 2018, 13, e0194897. [Google Scholar] [CrossRef]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplast. 2018, 33, 1309–1314.e2. [Google Scholar] [CrossRef]
- Taşoğlu, Ö.; Bölük, H.; ŞahinOnat, Ş.; Taşoğlu, İ.; Özgirgin, N. Is blood neutrophil-lymphocyte ratio an independent predictor of knee osteoarthritis severity? Clin. Rheumatol. 2016, 35, 1579–1583. [Google Scholar] [CrossRef]
- Büyükavcı, R.; Aktürk, S.; Sağ, S. Comparison of blood platelet distribution width and neutrophil-lymphocyte ratio in patients with different grades of knee osteoarthritis. J. Back Musculoskelet. Rehabil. 2018, 31, 1035–1039. [Google Scholar] [CrossRef] [PubMed]
- Taşoğlu, Ö.; Şahin, A.; Karataş, G.; Koyuncu, E.; Taşoğlu, İ.; Tecimel, O.; Özgirgin, N. Blood mean platelet volume and platelet lymphocyte ratio as new predictors of hip osteoarthritis severity. Medicine 2017, 96, e6073. [Google Scholar] [CrossRef] [PubMed]
- Yombi, J.C.; Schwab, P.E.; Thienpont, E. Neutrophil-to-lymphocyte ratio (NLR) distribution shows a better kinetic pattern than C-reactive protein distribution for the follow-up of early inflammation after total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3287–3292. [Google Scholar] [CrossRef] [PubMed]
- Suciu, O.; Bereteu, L.; Drǎgǎnescu, G. Determination of mechanical properties of hydroxyapatite doped with magnesium. AIP Conf. Proc. 2013, 1564, 132–137. [Google Scholar]
- Todor, A.; Vermesan, D.; Haragus, H.; Patrascu, J.M., Jr.; Timar, B.; Cosma, D.I. Cross-cultural adaptation and validation of the Romanian International Knee Documentation Committee—subjective knee form. PeerJ 2020, 8, e8448. [Google Scholar] [CrossRef]
- Beaufils, P.; Becker, R.; Kopf, S.; Matthieu, O.; Pujol, N. The knee meniscus: Management of traumatic tears and degenerative lesions. EFORT Open Rev. 2017, 2, 195–203. [Google Scholar] [CrossRef]
- Florescu, S.; Vermesan, D.; Haragus, H.; Patrascu, J.M., Jr.; Timar, B.; Todor, A. Cross-cultural adaptation and validation of the Romanian knee disability and osteoarthritis outcome score for joint replacement (KOOSJR). BMC Musculoskelet. Disord. 2020, 21, 155. [Google Scholar] [CrossRef]
- R 5.3.5 for Windows. Available online: https://cran.r-project.org/bin/windows/base/old/3.5.3/ (accessed on 12 September 2018).
- Jones, L.D.; Bottomley, N.; Harris, K.; Jackson, W.; Price, A.J.; Beard, D.J. The clinical symptom profile of early radiographic knee arthritis: A pain and function comparison with advanced disease. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 161–168. [Google Scholar] [CrossRef]
- Andor, B.; Patrascu, J.; Florescu, S.; Cojocaru, D.; Sandesc, M.; Borcan, F.; Boruga, O.; Bolintineanu, S. Comparison of different knee implants used on patients with osteoarthritis control study. Mater. Plast. 2016, 53, 119–125. [Google Scholar]
- Onofrei, R.R.; Amaricai, E.; Petroman, R.; Suciu, O. Relative and absolute within-session reliability of the modified Star Excursion Balance Test in healthy elite athletes. PeerJ 2019, 7, e6999. [Google Scholar] [CrossRef]
- Forget, P.; Khalifa, C.; Defour, J.-P.; Latinne, D.; Van Pel, M.-C.; De Kock, M. What is the normal value of the neutrophil-to-lymphocyte ratio? BMC Res. Notes 2017, 10, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Azab, B.; Camacho-Rivera, M.; Taioli, E. Average Values and Racial Differences of Neutrophil Lymphocyte Ratio among a Nationally Representative Sample of United States Subjects. PLoS ONE 2014, 9, e112361. [Google Scholar] [CrossRef] [PubMed]
- Chandrashekara, S.; Mukhtar Ahmad, M.; Renuka, P.; Anupama, K.R.; Renuka, K. Characterization of neutrophil-to-lymphocyte ratio as a measure of inflammation in rheumatoid arthritis. Int. J. Rheum. Dis. 2017, 20, 1457–1467. [Google Scholar] [CrossRef] [PubMed]
- Niessen, R.; Bihin, B.; Gourdin, M.; Yombi, J.-C.; Cornu, O.; Forget, P. Prediction of postoperative mortality in elderly patient with hip fractures: A single-centre, retrospective cohort study. BMC Anesthesiol. 2018, 18, 183. [Google Scholar] [CrossRef] [PubMed]
- Boia, E.S.; David, V.L. The Financial Burden of Setting up a Pediatric Robotic Surgery Program. Medicina 2019, 55, 739. [Google Scholar] [CrossRef] [PubMed]
- London, N.J.; Miller, L.E.; Block, J.E. Clinical and economic consequences of the treatment gap in knee osteoarthritis management. Med. Hypotheses 2011, 76, 887–892. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mild OA (n = 66) | Advanced OA (n = 45) | p | |
|---|---|---|---|
| NLR | 1.999 | 2.821 | 0.004 |
| Age | 54.06 | 67.11 | <0.001 |
| M:F ratio | 1:1.75 | 1:5.43 | 0.011 |
| Index | 0.505 | 0.253 | <0.001 |
| VAS | 64.92 | 43.88 | <0.001 |
| IKDC | 31.66 | 20.24 | <0.001 |
| KOOSJR | 1.45 | 18.33 | <0.001 |
| Kellgren-Lawrence | 1.3 | 3.8 | <0.001 |
| n = 111 | p | n = 66 | p |
|---|---|---|---|
| Age | <0.001 | Age | 0.133 |
| Gender | 0.362 | Gender | 0.610 |
| Index | 0.673 | Index | 0.331 |
| VAS | 0.287 | VAS | 0.006 |
| IKDC | 0.091 | IKDC | 0.001 |
| KOOSJR | 0.123 | KOOSJR | <0.001 |
| Neutrophil | <0.001 | Neutrophil | <0.001 |
| Lymphocyte | <0.001 | Lymphocyte | <0.001 |
| n = 45 | p | n = 45 | p |
|---|---|---|---|
| Age | 0.001 | Age | <0.001 |
| Gender | 0.808 | Gender | 0.725 |
| Index | 0.924 | Index | 0.171 |
| VAS | 0.913 | VAS | 0.092 |
| KSS1 | 0.492 | KSS1 | 0.120 |
| KSS2 | 0.290 | KSS2 | 0.074 |
| IKDC | 0.486 | IKDC | 0.062 |
| KOOSJR | 0.799 | KOOSJR | 0.693 |
| Neutro_pre | <0.001 | Neutro_pre | 0.629 |
| Lympho_pre | <0.001 | Lympho_pre | 0.643 |
| Neutro_post | 0.023 | Neutro_post | <0.001 |
| Lympho_post | 0.595 | Lympho_post | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ioniţescu, M.; Vermeşan, D.; Haraguș, H.; Suciu, O.; Todor, A.; Dumitrașcu, C.V.; Negrea, R.; Hoinoiu, T.; Radu, D.; Fruja, D. Association of Neutrophil to Lymphocyte Ratio with Patient Reported Outcomes in Knee Osteoarthritis. Appl. Sci. 2020, 10, 8173. https://doi.org/10.3390/app10228173
Ioniţescu M, Vermeşan D, Haraguș H, Suciu O, Todor A, Dumitrașcu CV, Negrea R, Hoinoiu T, Radu D, Fruja D. Association of Neutrophil to Lymphocyte Ratio with Patient Reported Outcomes in Knee Osteoarthritis. Applied Sciences. 2020; 10(22):8173. https://doi.org/10.3390/app10228173
Chicago/Turabian StyleIoniţescu, Marius, Dinu Vermeşan, Horia Haraguș, Oana Suciu, Adrian Todor, Cristian V. Dumitrașcu, Romeo Negrea, Teodora Hoinoiu, Daniela Radu, and Dan Fruja. 2020. "Association of Neutrophil to Lymphocyte Ratio with Patient Reported Outcomes in Knee Osteoarthritis" Applied Sciences 10, no. 22: 8173. https://doi.org/10.3390/app10228173
APA StyleIoniţescu, M., Vermeşan, D., Haraguș, H., Suciu, O., Todor, A., Dumitrașcu, C. V., Negrea, R., Hoinoiu, T., Radu, D., & Fruja, D. (2020). Association of Neutrophil to Lymphocyte Ratio with Patient Reported Outcomes in Knee Osteoarthritis. Applied Sciences, 10(22), 8173. https://doi.org/10.3390/app10228173