Impact of Alcohol on Occupational Health and Safety in the Construction Industry at Workplaces with Scaffoldings



Abstract
1. Introduction
2. Literature Review
3. Methodology of Research
3.1. Accident Documentation
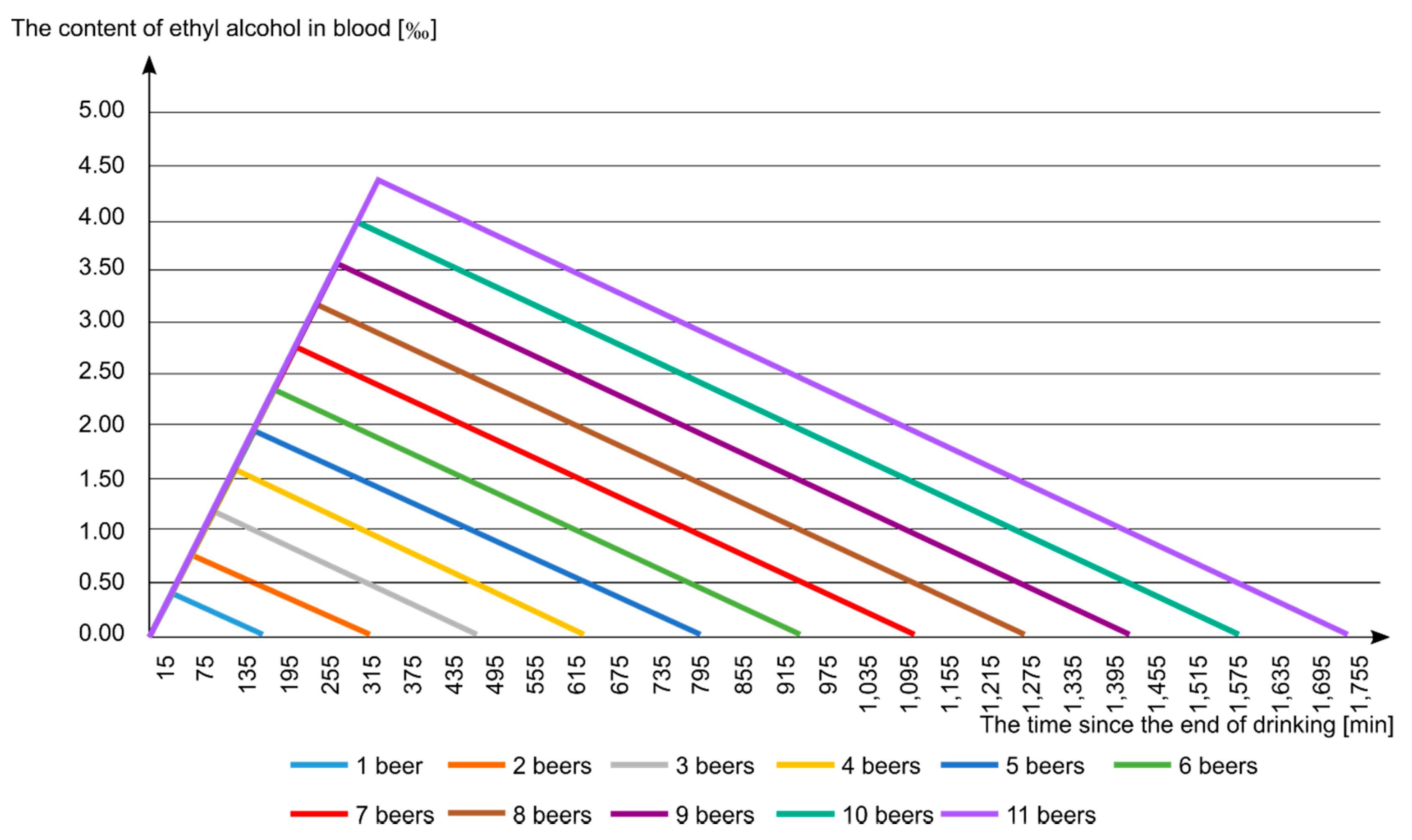
- the maximum blood alcohol content (in ‰);
- the time after finishing drinking and reaching the maximum value (min);
- the time after finishing drinking and reaching the value of 0.00 ‰, i.e., total sobriety (min);
- Scenario 1: the injured person consumed alcohol on the day preceding the accident, while assuming that drinking finished at 21:00;
- Scenario 2: the injured person consumed alcohol during the work break preceding the accident. Three specific cases were assumed: (a) alcohol was consumed before starting work, i.e., 7:00; (b) alcohol was consumed during the breakfast break at 10:00; (c) alcohol was consumed during the lunch break at 13:00.
3.2. Surveys
4. Research Results
4.1. Analysis of Occupational Accidents
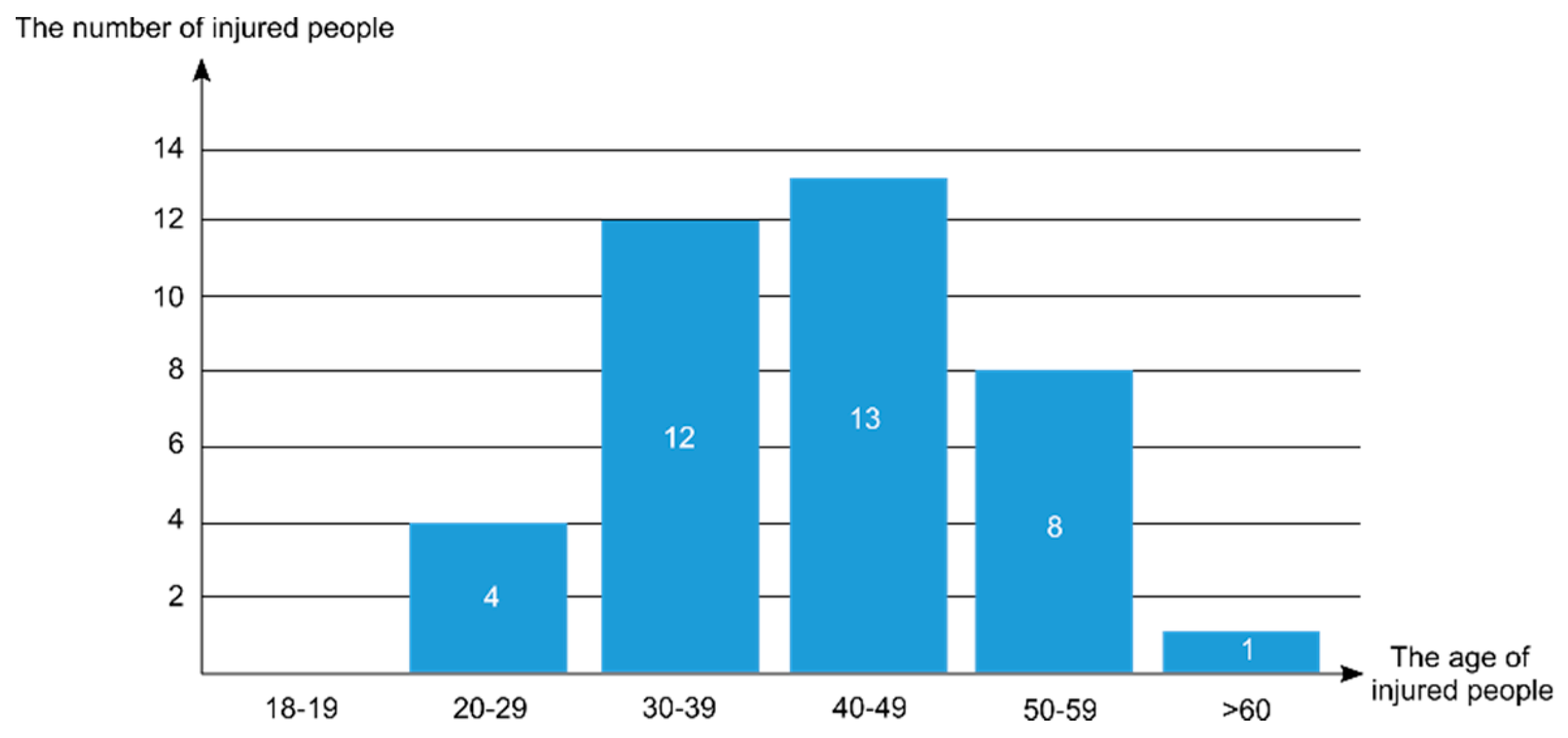
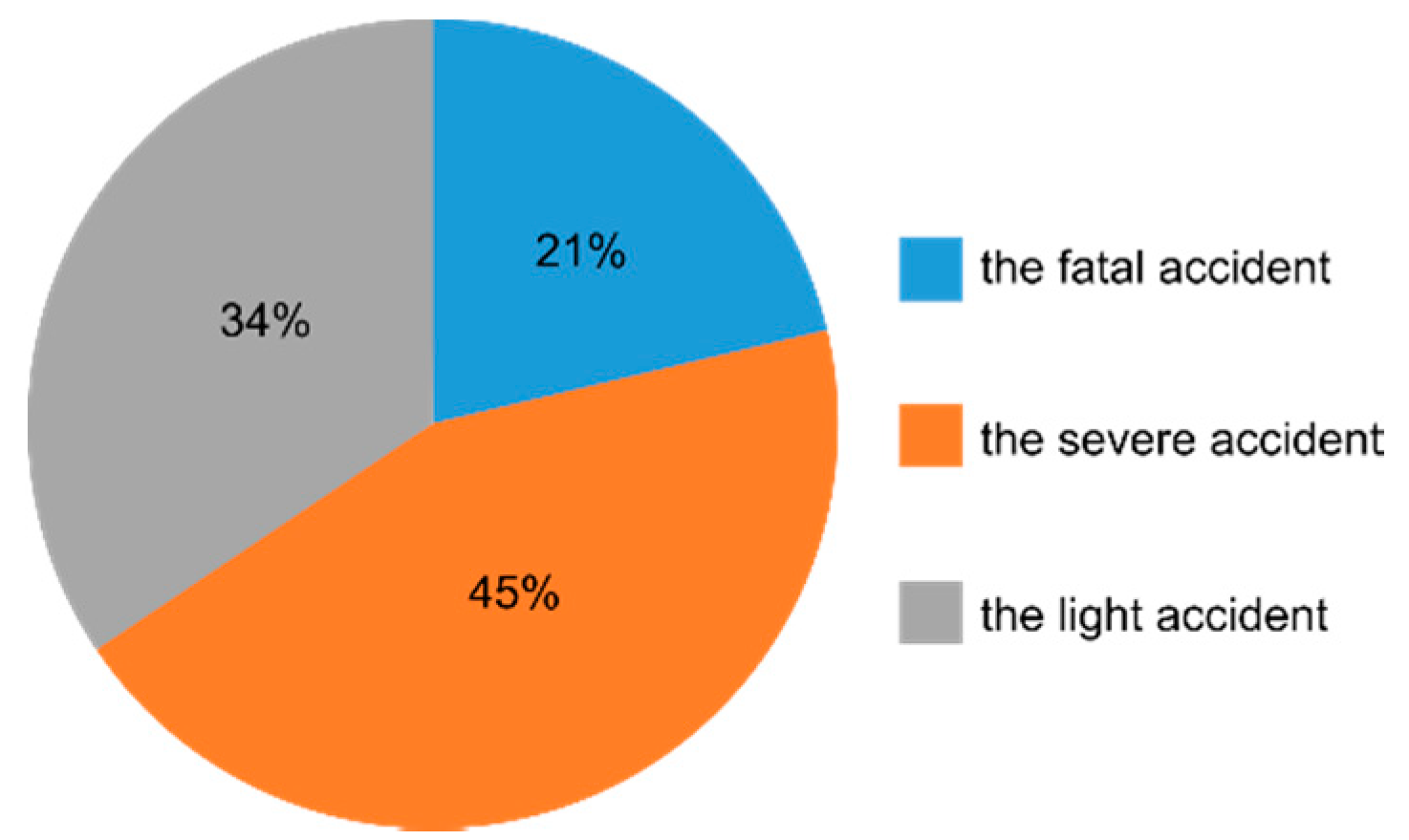
- Eight people had a fatal accident, which was 21% of the analyzed accidents. The alcohol content in five people for whom the blood alcohol content was known ranged from 0.53–4.16‰ (mean value of 1.97 ± 0.94‰). This means that all injured people were intoxicated (alcohol content greater than 0.50‰).
- Seventeen people had a severe accident, which represented 45% of all the analyzed cases. The alcohol content in 10 people for whom their blood alcohol content was known ranged from 0.22–3.40‰ (mean value of 1.47 ± 0.81‰). Two of them were in a state after the consumption of alcohol (alcohol content of less than 0.50‰), and the remaining eight people were drunk.
- Thirteen people suffered a light accident, which represented 34% of all the analyzed cases. The alcohol content in seven people for whom the blood alcohol value was known ranged from 0.44–3.00‰ (mean value 1.37 ± 0.86‰). Two of them were in a state after the consumption of alcohol (alcohol content of less than 0.50‰), and the remaining five people were drunk.
- “L” means light accident;
- “S” means severe accident;
- “F” means fatal accident.
- injured parties were likely to drink alcohol during the work break immediately before the accident: scenario (2a)—cases: 6, 17 (1000–1500 mL of 4.5% beer: 2–3 beers), scenario (b)—cases: 1, 10, 11, 13, 16 (500–1500 mL of 4.5% beer: 1—3 beers), scenario (c)—cases: 7, 14, 15 (500 mL of 4.5% beer: 1 beer);
- injured parties most likely consumed alcohol the day before (scenario 1)—cases: 3, 4, 22 (2500–3500 mL of 4.5% beer: 5—7 beers).
4.2. Analysis of Survey Data
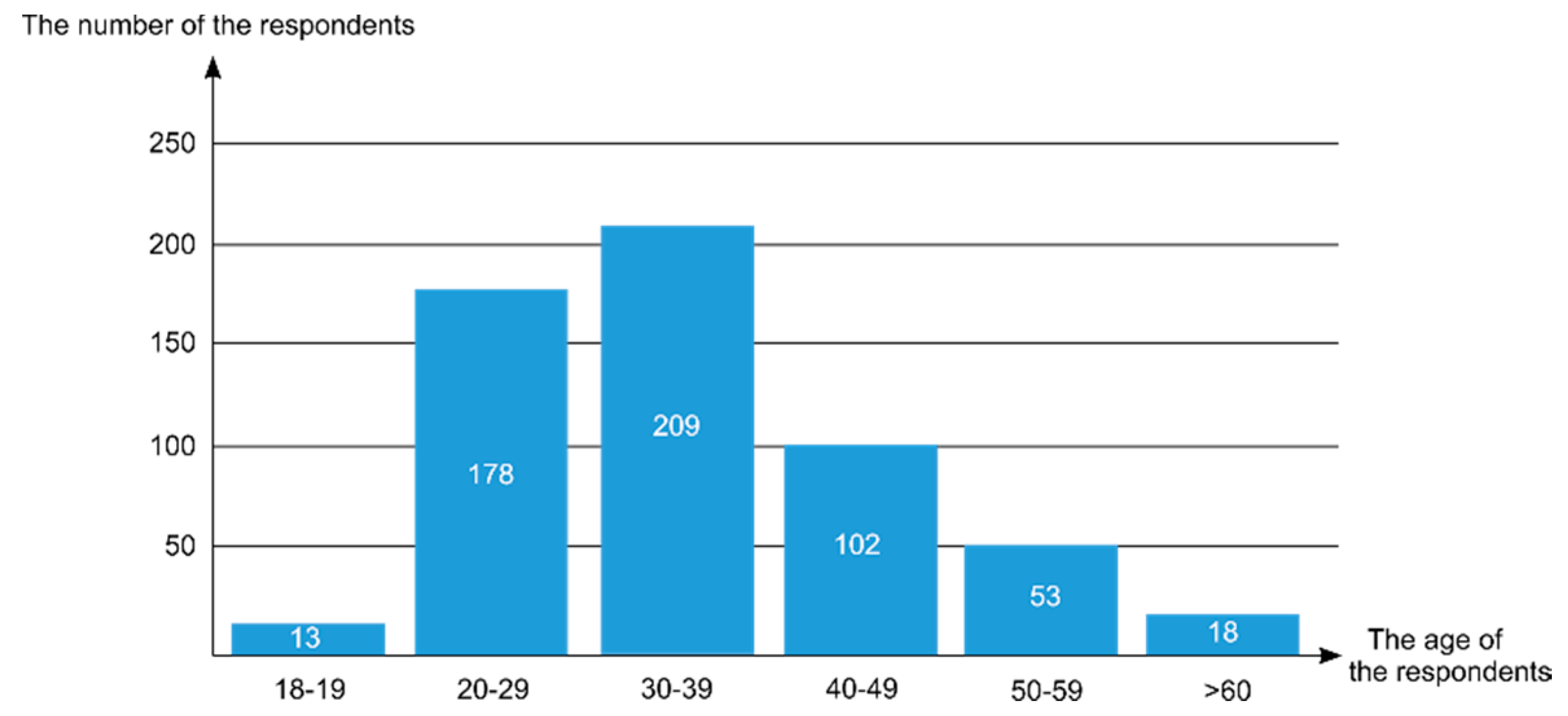
- The largest group of respondents were employees aged 30–39, and they represented 36.5% of all the respondents. They were mainly employees with average experience who had worked for at least 10 years in their profession.
- The second group was made up of young employees aged 20–29 (31.1%), with a much shorter seniority, ranging from several days to a maximum of 10 years.
- Other respondents were experienced employees with more than 15 years of work experience at the age of 40–49 (17.8%) and 50–59 (9.2%), several employees over the age of 60 who were often at retirement age (3.1%), and adolescent employees (2.3%).
- The most numerous group who consumed alcohol during the day were employees aged 30–39 (100 people) and 20–29 (85 people);
- The highest percentage of people consuming alcohol occurred among employees aged over 60 (55.6%) and 50–59 (54.7%);
- The number of people consuming alcohol decreased with age (decreasing tendency) and the ratio of people consuming alcohol to the abstainers changed (the number of people consuming alcohol increased);
- Among younger employees (18–19, 20–29, 30–39), the percentage of people consuming alcohol was smaller than the percentage of abstainers.
4.3. Summary of Results
- Alcohol is one of the causes that leads to occupational accidents. In the analyzed accidents on scaffoldings, the cause related to alcohol consumption occurred in 17.4% of all the victims. This means that every sixth occupational accident was caused by an abnormal sobriety of employees
- The largest group of people consuming alcohol were employees aged 40–49 and 30–39. The average age of victims was 40 ± 8 years. The proportion of drinkers increased with age.
- Analysis of the content of alcohol in blood with regards to the effect of an accident indicated that as the amount of alcohol in the blood rises, the severity of the accident increases. A high alcohol content contributes to the death of a construction worker.
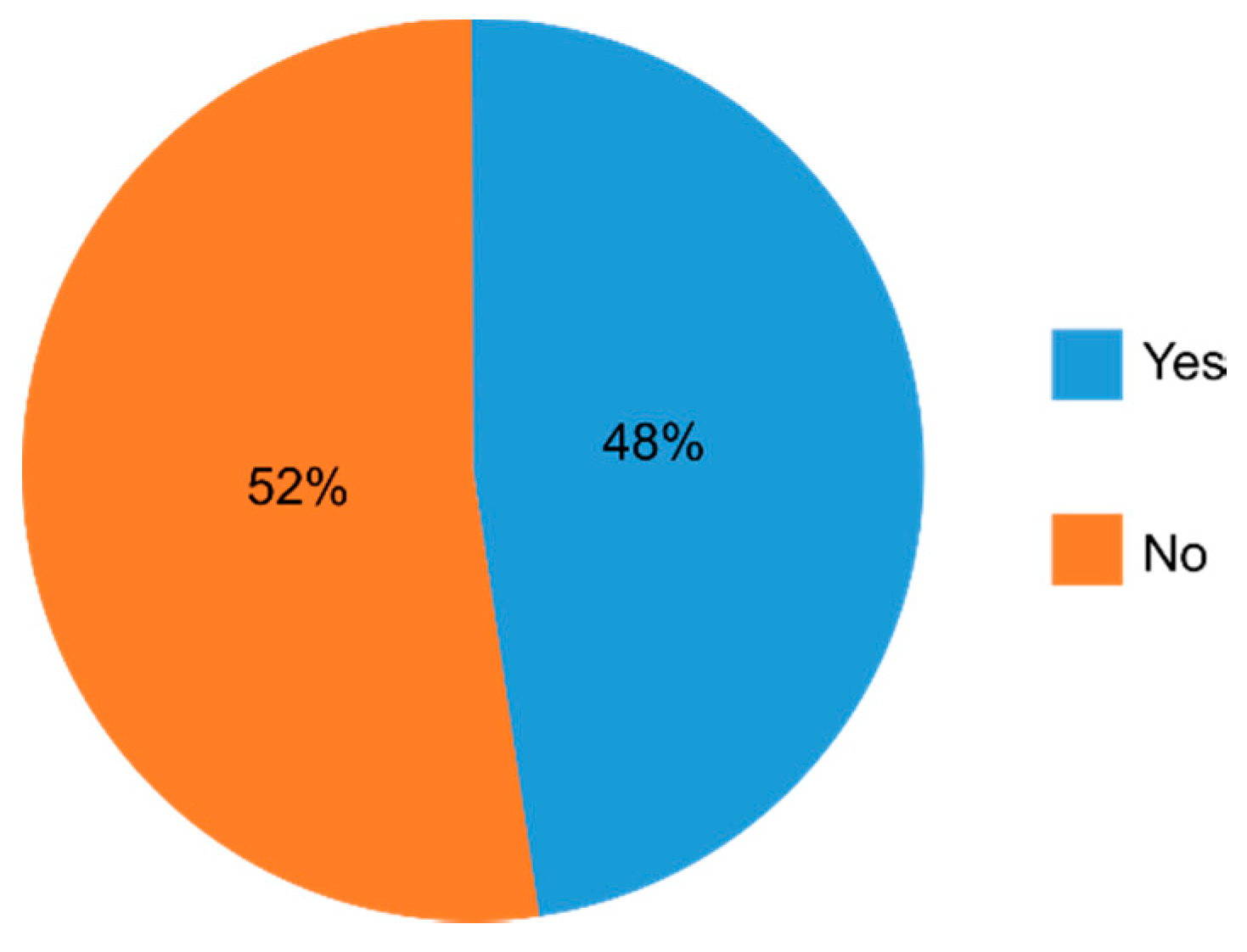
- 47.8% of surveyed employees declared that they drink alcohol during the day;
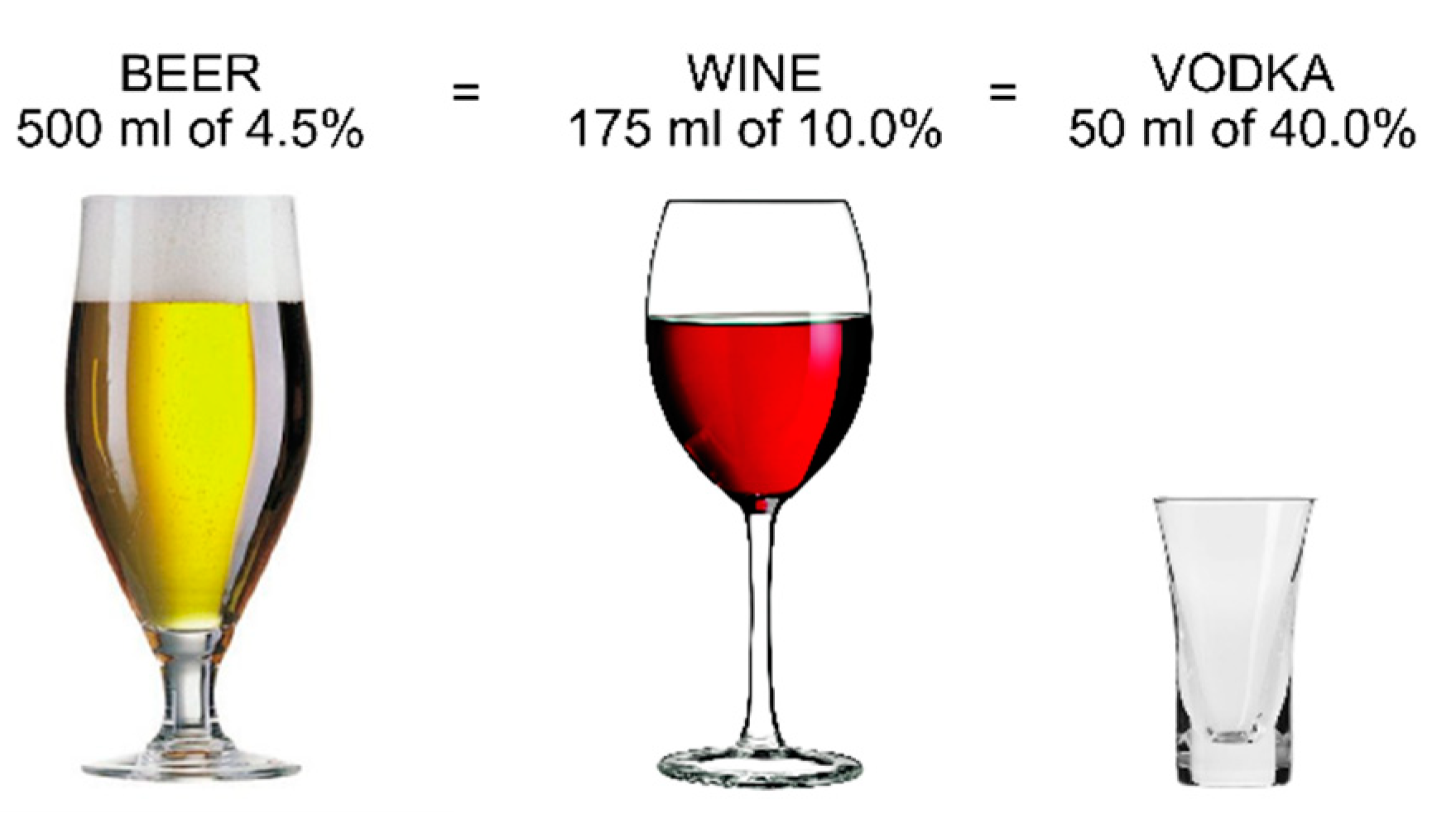
- the most common number of alcohol beverages consumed outside working hours was one “large beer” (500 mL of 4.5% beer);
- analysis of the place of residence showed that people most often declared living in the countryside and in small towns (up to 100,000 inhabitants);
- the proportion of people consuming alcohol increased with age (an increasing trend of consuming alcohol with age), and the proportion of people consuming alcohol to abstainers changed—the number of people consuming alcohol increased.
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Miller, T.R.; Zaloshnja, E.; Spicer, R.S. Effectiveness and benefit-cost of peer-based workplace substance abuse prevention coupled with random testing. Accid. Anal. Prev. 2007, 39, 565–573. [Google Scholar] [CrossRef]
- Appleton, A.; James, R.; Larsen, J. The Association between mental wellbeing, levels of harmful drinking, and drinking motivations: A cross-sectional study of the UK adult population. Int. J. Environ. Res. Public Health 2018, 15, 1333. [Google Scholar] [CrossRef]
- World Health Organization. Global Status Report on Alcohol and Health 2018; World Health Organization: Geneva, Switzerland, 2018; ISBN 978-92-4-156563-9. Available online: www.who.int/substance_abuse/publications/global_alcohol_report/en (accessed on 23 April 2020).
- Anderson, P.; Baumberg, B. Alcohol in Europe—Public health perspective: Report summary. Drugs 2006, 13, 483–488. [Google Scholar] [CrossRef]
- Brooks, A.T.; Raju, S.; Barb, J.J.; Kazmi, N.; Chakravorty, S.; Krumlauf, M.; Wallen, G.R. Sleep regularity index in patients with alcohol dependence: Daytime napping and mood disorders as aorrelates of interest. Int. J. Environ. Res. Public Health 2020, 17, 331. [Google Scholar] [CrossRef] [PubMed]
- John, U.; Hanke, M.; Freyer-Adam, J. Health risk behavior patterns in a national adult population survey. Int. J. Environ. Res. Public Health 2018, 15, 873. [Google Scholar] [CrossRef] [PubMed]
- Roche, A.; Chapman, J.; Duraisingam, V.; Phillips, B.; Finnane, J.; Pidd, K. Construction workers’ alcohol use, knolwedge, perceptions of risk and workplace norms. Drug Alcohol Rev. 2020. [Google Scholar] [CrossRef] [PubMed]
- Strickland, J.; Wagan, S.; Dale, A.; Evanoff, A. Prevalence and perception of risky health behaviors among construction workers. J. Occup. Environ. Med. 2017, 59, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Hoła, B.; Szóstak, M. An occupational profile of people injured in accidents at work in the polish construcion industry. Procedia Eng. 2017, 208, 43–51. [Google Scholar] [CrossRef]
- Hoła, B.; Nowobilski, T.; Szer, I.; Szer, J. Identification of factors affecting the accident rate in the construction industry. Procedia Eng. 2017, 208, 35–42. [Google Scholar] [CrossRef]
- Lim, S.; Chi, S.; Lee, J.; Lee, H.-J.; Choi, H. Analyzing psychological consitions of field-workers in the construction industry. Int. J. Occup. Environ. Health 2017, 23, 261–281. [Google Scholar] [CrossRef]
- Tabernero, C.; Luque, B.; Cuadrado, E. A Multilevel study of alcohol consumption in young adults: Self-efficacy, peers’ motivations and protective strategies. Int. J. Environ. Res. Public Health 2019, 16, 2827. [Google Scholar] [CrossRef]
- Flannery, J.; Ajayi, S.O.; Oyegoke, A.S. Alcohol and substance misuse in the construction industry. Int. J. Occup. Saf. Ergon. 2019, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Ken, P.; Vinita, D.; Roche, A.; Allan, T. Young construction workers: Substance use, mental health, and workplance psychosocial factors. Adv. Dual. Diagn. 2017, 10, 155–165. [Google Scholar] [CrossRef]
- Wang, S.-C.; Chen, Y.-C.; Chen, S.-J.; Lee, C.-H.; Cheng, C.-M. Alcohol addiction, gut microbiota, and alcoholism treatment: A review. Int. J. Mol. Sci. 2020, 21, 6413. [Google Scholar] [CrossRef]
- Tiwary, G.; Gangopadhyay, P.; Biswas, S.; Nayak, K.; Chatterjee, M.; Chakraborty, D.; Mukherjee, S. Socio-economic status of workers of building construction industry. Indian J. Occup. Environ. Med. 2012, 16, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Łyszczarz, B. Production losses associated with alcohol-attributable mortality in the European Union. Int. J. Environ. Res. Public Health 2019, 16, 3536. [Google Scholar] [CrossRef]
- Demirel, B.; Ergin, M.; Özhasenekler, A.; Teke, C.; Tanrıverdi, F.; Kurtoğlu Çelik, G.; Şener, A.; Pamukçu Günaydın, G.; Gökhan, Ş. The influence of alcohol related accidents on health care cost. Disaster Emerg. Med. J. 2018, 3, 71–74. [Google Scholar] [CrossRef]
- Biggs, H.; Williamson, A. Reducing the risk of alcohol and other drugs in construction: An Autralian assessment. In New Developments in Structural Engineering and Construction; Research Publishing Services: Singapore, 2013; pp. 1399–1404. [Google Scholar] [CrossRef]
- Banwell, C.; Dance, P.; Quinn, C.; Davies, R.; Hall, D. Alcohol, other drug use, and gambling among Australian Capital Territory (ACT) workser in the building and related industries. Drugs 2006, 13, 167–178. [Google Scholar] [CrossRef]
- Coggon, D.; Harris, E.; Brown, T.; Rice, S.; Palmer, K. Occupation and mortality related to alcohol, drugs and sexual habits. Occup. Med. 2010, 60, 348–353. [Google Scholar] [CrossRef]
- Rebelo, M.; Silveira, F.; Czarnocka, E.; Czarnocki, K. Construction safety on scaffolding; Building Information Modeling (BIM) and Safety Management—A systematic review. U Porto J. Eng. 2019, 2, 46–60. [Google Scholar] [CrossRef]
- Hoła, B.; Szóstak, M. Modeling of the accidentality phenomenon in the construction industry. Appl. Sci. 2019, 9, 1878. [Google Scholar] [CrossRef]
- Statistical Office of the European Union. Available online: https://ec.europa.eu/eurostat/web/health/data/database (accessed on 10 August 2020).
- Central Statistical Office. Health Status of Population in Poland in 2014. Warsaw. 2016. Available online: https://stat.gov.pl/en/topics/health/health/health-status-of-population-in-poland-in-2014,4,1.html (accessed on 23 April 2020).
- Brenner, H.; Arndt, V.; Rothenbacher, D.; Schuberth, S.; Fraisse, E.; Fliedner, T.M. The association between alcohol consumption and all-cause mortality in a cohort of male employees in the German construction industry. Int. J. Epidemiol. 1997, 26, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Biggs, H.C.; Williamson, A.R. Safety impacts of alcohol and other drugs in construction: Development of an industry policy and cultural change management program. In Proceedings of the 28th Annual Conference (ARCOM 2012), Edinburg, UK, 3–5 September 2012; pp. 445–454. [Google Scholar]
- du Plessis, K.; Corney, T.; Burnside, L. Harmful drinking and experiences of alcohol-related violence in Australian male construction industry apprentices. Am. J. Mens. Health 2013, 7, 423–426. [Google Scholar] [CrossRef] [PubMed]
- Peacock, A.; Leung, J.; Larney, S.; Colledge, S.; Hickman, M.; Rehm, J.; Giovino, G.; West, R.; Hall, W.; Griffths, P.; et al. Global statistics on alcohol, tobacco and illicit drug use: 2017 status report. Addiction 2018, 113, 1905–1926. [Google Scholar] [CrossRef] [PubMed]
- Roche, A.M.; Lee, N.K.; Battams, S.; Fischer, J.A.; Cameron, J.; McEntee, A. Alcohol use among workers in male-dominated industries: A systematic review of risk factors. Saf. Sci. 2015, 78, 124–141. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics National Survey of Mental Health and Wellbeing: Summary of Results; Sydney. 2008. Available online: www.abs.gov.au/AUSSTATS/abs@.nsf/Lookup/4326.0Main+Features32007?OpenDocument (accessed on 23 April 2020).
- Central Statistical Office. Employment in National Economy in 2018. Warsaw. 2019. Available online: https://stat.gov.pl/en/topics/labour-market/working-employed-wages-and-salaries-cost-of-labour/employment-in-national-economy-in-2018,7,15.html (accessed on 23 April 2020).
- Elliott, K.; Shelley, K. Effects of drugs and alcohol on behavior, job performance, and workplace safety. J. Employ. Couns. 2006, 43, 130–134. [Google Scholar] [CrossRef]
- Karriker-Jaffe, K.; Tam, C.; Cook, W.; Greenfield, T.; Roberts, S. Gender equality, drinking cultures and second-hand harms from alcohol in the 50 US States. Int. J. Environ. Res. Public Health 2019, 16, 4619. [Google Scholar] [CrossRef]
- Martin, J.L.; Gadegbeku, B.; Wu, D.; Viallon, V.; Laumon, B. Cannabis, alcohol and fatal road accidents. PLoS ONE 2017, 12. [Google Scholar] [CrossRef]
- Marchand, A.; Parent-Lamarche, A.; Blanc, M.-È. Work and high-risk alcohol consumption in the Canadian workforce. Int. J. Environ. Res. Public Health 2011, 8, 2692–2705. [Google Scholar] [CrossRef]
- Zhang, J.; Wu, L. Cigarette smoking and alcohol consumption among chinese older adults: Do living arrangements matter? Int. J. Environ. Res. Public Health 2015, 12, 2411–2436. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rabassa, M.; López, P.; Sánchez, R.; Hernández, C.; Rodríguez, C.; Rodríguez-santiago, R.E.; Orengo, J.C.; Green, V.; Yamamura, Y.; Rivera-amill, V. Inflammatory biomarkers, microbiome, depression, and executive dysfunction in alcohol users. Int. J. Environ. Res. Public Health 2020, 17, 689. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.-H.; Li, R.-H.; Huang, S.-L.; Sia, H.-K.; Chen, Y.-L.; Tang, F.-C. Lifestyle factors and metabolic syndrome among workers: The role of interactions between smoking and alcohol to nutrition and exercise. Int. J. Environ. Res. Public Health 2015, 12, 15967–15978. [Google Scholar] [CrossRef] [PubMed]
- van de Loo, A.; Mackus, M.; van Schrojenstein Lantman, M.; Kraneveld, A.; Brookhuis, K.; Garssen, J.; Scholey, A.; Verster, J. Susceptibility to alcohol hangovers: The association with self-reported immune status. Int. J. Environ. Res. Public Health 2018, 15, 1286. [Google Scholar] [CrossRef]
- Howland, J.; Rohsenow, D.J.; Cote, J.; Gomez, B.; Mangione, T.W.; Laramie, A.K. Effects of low-dose alcohol exposure on simulated merchant ship piloting by maritime cadets. Accid. Anal. Prev. 2001, 33, 257–265. [Google Scholar] [CrossRef]
- Marques, P.H.; Jesus, V.; Olea, S.A.; Vairinhos, V.; Jacinto, C. The effect of alcohol and drug testing at the workplace on individual’s occupational accident risk. Saf. Sci. 2014, 68, 108–120. [Google Scholar] [CrossRef]
- Yi, W.; Chan, A. Health profile of construction workers in Hong Kong. Int. J. Environ. Res. Public Health 2016, 13, 1232. [Google Scholar] [CrossRef]
- Liu, R.; Chen, L.; Zhang, F.; Zhu, R.; Lin, X.; Meng, X.; Li, H.; Lei, X.; Zhao, Y. Trends in alcohol intake and the association between socio-demographic factors and volume of alcohol intake amongst adult male drinkers in China. Int. J. Environ. Res. Public Health 2019, 16, 573. [Google Scholar] [CrossRef]
- Kilian, C.; Manthey, J.; Moskalewicz, J.; Sieroslawski, J.; Rehm, J. How attitudes toward alcohol policies differ across european countries: Evidence from the Standardized European Alcohol Survey (SEAS). Int. J. Environ. Res. Public Health 2019, 16, 4461. [Google Scholar] [CrossRef]
- Berry, J.G.; Pidd, K.; Roche, A.M.; Harrison, J.E. Prevalence and patterns of alcohol use in the Australian workforce: Findings from the 2001 National Drug Strategy Household Survey. Addiction 2007, 102, 1399–1410. [Google Scholar] [CrossRef]
- The National Program for Prevention of Alcohol Problems for the Years 2011–2015. 2010. Available online: http://www.parpa.pl/images/image/NP%202011_2015_11_011.pdf (accessed on 23 April 2020).
- Ronksley, P.E.; Brien, S.E.; Turner, B.J.; Mukamal, K.J.; Ghali, W.A. Association of alcohol consumption with selected cardiovascular disease outcomes: A systematic review and meta-analysis. BMJ 2011, 342, 479. [Google Scholar] [CrossRef] [PubMed]
- ICAP. International Recommendations on Alcohol Consumption. 2003. Available online: http://alkoholizm.eu/pub/zalecenia_ICAP.pdf (accessed on 23 April 2020). (In Polish).
- Biggs, H.C.; Williamson, A.R.; Davey, T.M. The role of education and awareness in workplace alcohol and drug use in the Australian construction industry: Proposed program of research and preliminary results. Vulnerable Groups Incl. 2012, 3, 17284. [Google Scholar] [CrossRef]
- Koob, G.; Arends, M.; Moal, M. Alcohol. In Drugs, Addiction, and the Brain; Academic Press: Cambridge, MA, USA, 2014; Chapter 6; pp. 173–219. [Google Scholar] [CrossRef]
- The Penal Code of 06 June 1997 (Law Gazette, No. 88, it. 553, as amended). In Polish. 1997. Available online: http://prawo.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU19970880553 (accessed on 23 April 2020).
- Promille Calculator. In Polish. Available online: www.medme.pl/kalkulatory/alkohol (accessed on 24 April 2020). (In Polish).
- Caderbaum, A. Alcohol metabolism. Clin. Liver. Dis. 2012, 16, 667–685. [Google Scholar] [CrossRef] [PubMed]
- Edenberg, H. The Genetics of alcohol metabolism: Role of alcohol dehydrogenase and aldehyde dehydrogenase variants. Alcohol Res. Health 2007, 30, 5–13. [Google Scholar]
- Iriste, S.; Katane, I. Expertise as a research method in education. Rural Environ. Educ. Person. 2018, 11, 74–80. [Google Scholar] [CrossRef]
- Krzysztof, C.; Bojar, H.; Silveira, F.; Rebelo, M.; Elżbieta, C. Health behaviours in scaffold use risk assessment model—SURAM. Annals Agric. Environ. Med. 2019, 26, 138–142. [Google Scholar] [CrossRef]
- World Mecidal Association, WMA Declaration of Helsinki—Ethical Pricniples for Medical Research Involving Human Subjects, 1964 as Amended. Available online: www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 10 August 2020).
- The Supreme Medical Court. The Polish Code of Medical Ethics. 2003. In Polish. Available online: http://nil.org.pl/dokumenty/kodeks-etyki-lekarskiej (accessed on 10 August 2020).
- Pannucci, C.; Wilkins, E. Identyfying and avoiding bias in research. Plast. Reconstr. Surg. 2011, 126, 619–625. [Google Scholar] [CrossRef]
- Althubaiti, A. Information bias in jealth research: Definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef]
- Davis, R.; Couper, M.; Janz, N.; Caldwell, C.; Resnicow, K. Interviewer effects in public health surveys. Health Educ. Res. 2010, 25, 14–26. [Google Scholar] [CrossRef]
- Mishra, P.; Pandey, C.; Singh, U.; Gupta, A.; Sahu, C.; Keshri, A. Desciptive statistics and mornality tests for statistical data. Ann. Card. Anaesth. 2019, 22, 67–72. [Google Scholar] [CrossRef]
- Sijtsma, K.; Emons, W. Nonparametric statistical methods. In International Encyclopedia of Education, 3rd ed.; Elsevier: Oxford, UK, 2010; pp. 347–353. [Google Scholar] [CrossRef]
- Kelley, K. Confidence intervals for standardized effect sizes: Theory, application, and implementation. J. Stat. Soft. 2007, 20. [Google Scholar] [CrossRef]
- Peng, C.-Y.; Lee, K.; Ingersoll, G. An introduction to logistic regression analysis and reporting. Int. J. Educ. Res. 2010, 96, 3–14. [Google Scholar] [CrossRef]
- López-Martínez, A.; Exteve-Zarazaga, R.; Ramirez-Maestre, C. Perceived social support and coping responses are independent variables explaining pain adjustment among chronic pain patients. J. Pain 2008, 9, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Peng, J.; Wang, B.; Lu, X.; Zheng, J.; Wand, K.; Tu, X.; Feng, C. Inconsistency between univariate and multiple logistic regressions. Shanghai Arch. Psychiatr. 2017, 25, 124–128. [Google Scholar] [CrossRef]
- Mayo, D. Statistical Inference as Severe Testing; Cambridge University Press: Cambridge, UK, 2018; ISBN 9781107286184. [Google Scholar] [CrossRef]
- Hoła, A.; Sawicki, M.; Szóstak, M. Methodology of classifying the causes of occupational accidents involving construction scaffolding using Pareto-Lorenz analysis. Appl. Sci. 2018, 8, 48. [Google Scholar] [CrossRef]
- Yang, K.; Ahn, C.; Vuran, M.; Kim, H. Collective sensing of workers’ gait patterns to identify fall hazards in construction. Automat. Constr. 2017, 82, 166–178. [Google Scholar] [CrossRef]
- Albert, A.; Hallowell, M.; Kleiner, B.; Chen, A. Enhancing construction hazard recognition with high-fidelity augmented virtuality. J. Constr. Eng. Manag. 2014, 140, 4014024. [Google Scholar] [CrossRef]
- Szóstak, M. Analysis of occupational accidents in the construction industry with regards to selected time parameters. Open Eng. 2019, 9, 312–320. [Google Scholar] [CrossRef]
- Sanchez, F.; Pelaez, G.; Alis, J. Occupational safety and health in construction: A review of applications and trends. Ind. Health 2017, 55, 210–218. [Google Scholar] [CrossRef]
- Act. of 26 October 1982 on Upbringing in Sobriety and Counteracting Alcoholism (Law Gazette, No. 35, it. 230 as amended). 1982. Available online: http://prawo.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU19820350230 (accessed on 23 April 2020).















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Alcohol Dose | Content of Ethyl Alcohol in Blood | Blood Alcohol Concentration (BAC) | Time Since the End of Drinking | ||
|---|---|---|---|---|---|
| Number of 4.5% Beers/(mL) | Number of 10.0% Glasses of Wine/(mL) | Number of 40.0% Glasses of Vodka/(mL) | (‰) | (g/100 mL) | (min) |
| 1/500 | 1/175 | 1/50 | 0.39 | 0.04 | 30 |
| 0.00 | 0.00 | 160 | |||
| 2/1000 | 2/350 | 2/100 | 0.78 | 0.08 | 60 |
| 0.00 | 0.00 | 320 | |||
| 3/1500 | 3/525 | 3/150 | 1.18 | 0.12 | 90 |
| 0.00 | 0.00 | 480 | |||
| 4/2000 | 4/700 | 4/200 | 1.56 | 0.16 | 120 |
| 0.00 | 0.00 | 640 | |||
| 5/2500 | 5/875 | 5/250 | 1.95 | 0.21 | 150 |
| 0.00 | 0.00 | 800 | |||
| 6/3000 | 6/1050 | 6/300 | 2.34 | 0.25 | 180 |
| 0.00 | 0.00 | 960 | |||
| 7/3500 | 7/1225 | 7/350 | 2.73 | 0.29 | 210 |
| 0.00 | 0.00 | 1120 | |||
| 8/4000 | 8/1400 | 8/400 | 3.12 | 0.34 | 240 |
| 0.00 | 0.00 | 1280 | |||
| 9/4500 | 9/1575 | 9/450 | 3.51 | 0.38 | 270 |
| 0.00 | 0.00 | 1440 | |||
| 10/5000 | 10/1750 | 10/500 | 3.90 | 0.42 | 300 |
| 0.00 | 0.00 | 1600 | |||
| 11/5500 | 11/1925 | 11/550 | 4.290.00 | 0.460.00 | 3301760 |
| No. | Severity | Content of Alcohol in Blood | Scenario 1 | Scenario 2 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| (a) | (b) | (c) | ||||||||
| Time | Number of Beers | Time | Number of Beers | Time | Number of Beers | Time | Number of Beers | |||
| (-) | (-) | (‰) | (min) | (pcs) | (min) | (pcs) | (min) | (pcs) | (min) | (pcs) |
| 1 | L | 0.70 | 900 | 7 | 270 | 3 | 90 | 2 | - | - |
| 2 | S | 2.13 | 1080 | 10 | 480 | 7 | 300 | 6 | 120 | im |
| 3 | L | 0.53 | 720 | 5 | 120 | 2 | - | - | - | - |
| 4 | S | 1.23 | 680 | 7 | 80 | im | - | - | - | - |
| 5 | S | 1.85 | 1020 | 10 | 420 | 6 | 240 | 5 | 60 | im |
| 6 | S | 1.30 | 690 | 7 | 90 | 3 | - | - | - | - |
| 7 | L | 0.22 | 1070 | 7 | 470 | 3 | 290 | 2 | 110 | 1 |
| 8 | F | 3.00 | 810 | >10 | 210 | im | 30 | im | - | - |
| 9 | F | 4.16 | 1075 | >10 | 475 | 11 | 295 | im | - | - |
| 10 | S | 1.33 | 900 | 8 | 300 | 4 | 120 | 3 | - | - |
| 11 | S | 1.11 | 860 | 8 | 260 | 4 | 80 | 3 | - | - |
| 12 | F | 1.70 | 1070 | 10 | 470 | 6 | 290 | 5 | 110 | im |
| 13 | L | 1.00 | 840 | 7 | 240 | 3 | 60 | 2 | - | - |
| 14 | L | 0.46 | 1020 | 7 | 420 | 3 | 240 | 2 | 60 | 1 |
| 15 | L | 0.44 | 1020 | 7 | 420 | 3 | 240 | 2 | 60 | 1 |
| 16 | S | 1.30 | 885 | 8 | 285 | 4 | 105 | 3 | - | - |
| 17 | L | 0.20 | 780 | 5 | 180 | 2 | - | - | - | - |
| 18 | F | 2.74 | 990 | >10 | 390 | 8 | 210 | 7 | 30 | im |
| 19 | F | 3.40 | 1110 | >10 | 510 | 10 | 330 | 9 | 150 | im |
| 20 | S | 2.67 | 840 | 10 | 240 | 7 | 60 | im | - | - |
| 21 | S | 2.00 | 1110 | >10 | 510 | 7 | 330 | 6 | 150 | im |
| 22 | S | 0.63 | 610 | 5 | 10 | im | - | - | - | - |
| Age of Employee | |||
|---|---|---|---|
| Age Range | Number of People | Percentage | p |
| 18–19 | 13 | 2.3% | <0.01 |
| 20–29 | 178 | 31.1% | |
| 30–39 | 209 | 36.5% | |
| 40–49 | 102 | 17.8% | |
| 50–59 | 53 | 9.2% | |
| >60 | 18 | 3.1% | |
| Marital Status | |||
| Marital Status | Number of People | Percentage | p |
| Single | 251 | 43.8% | <0.01 |
| Married | 304 | 53.1% | |
| Divorced | 11 | 1.9% | |
| Widower | 7 | 1.2% | |
| Permanent Residence | |||
| Place | Number of People | Percentage | p |
| A city of over 100,000 residents | 179 | 31.2% | <0.01 |
| A small town with up to 100,000 residents | 204 | 35.6% | |
| Village | 190 | 33.2% | |
| Age Range | Number of People | Answer | Number of People | Percentage |
|---|---|---|---|---|
| 18–19 | 13 | Yes | 3 | 23.1% |
| No | 10 | 76.9% | ||
| 20–29 | 178 | Yes | 85 | 47.8% |
| No | 93 | 52.2% | ||
| 30–39 | 209 | Yes | 100 | 47.8% |
| No | 109 | 52.2% | ||
| 40–49 | 102 | Yes | 47 | 46.1% |
| No | 55 | 53.9% | ||
| 50–59 | 53 | Yes | 29 | 54.7% |
| No | 24 | 45.3% | ||
| >60 | 18 | Yes | 10 | 55.6% |
| No | 8 | 44.4% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sawicki, M.; Szóstak, M. Impact of Alcohol on Occupational Health and Safety in the Construction Industry at Workplaces with Scaffoldings. Appl. Sci. 2020, 10, 6690. https://doi.org/10.3390/app10196690
Sawicki M, Szóstak M. Impact of Alcohol on Occupational Health and Safety in the Construction Industry at Workplaces with Scaffoldings. Applied Sciences. 2020; 10(19):6690. https://doi.org/10.3390/app10196690
Chicago/Turabian StyleSawicki, Marek, and Mariusz Szóstak. 2020. "Impact of Alcohol on Occupational Health and Safety in the Construction Industry at Workplaces with Scaffoldings" Applied Sciences 10, no. 19: 6690. https://doi.org/10.3390/app10196690
APA StyleSawicki, M., & Szóstak, M. (2020). Impact of Alcohol on Occupational Health and Safety in the Construction Industry at Workplaces with Scaffoldings. Applied Sciences, 10(19), 6690. https://doi.org/10.3390/app10196690