Development and Assist-As-Needed Control of an End-Effector Upper Limb Rehabilitation Robot


Abstract
1. Introduction
- (1)
- In view of the insufficiency that the current existing end-effector upper limb rehabilitation robots can only carry on the training in a specific plane, such as [6], the EULRR developed in this paper can assist the patient’s arm with motor dysfunction to realize training in three-dimension space.
- (2)
- Comparing with the existing impedance-based assistance strategy, such as [24,25,26], the assisted-as-needed controller presented in this paper enables the patient’s arm to have spatial freedom by constructing a virtual channel around the predetermined training trajectory. Patients could move their arm freely in the allowed virtual channel during rehabilitation training, while the robot provides assistance when deviating from the virtual channel.
- (3)
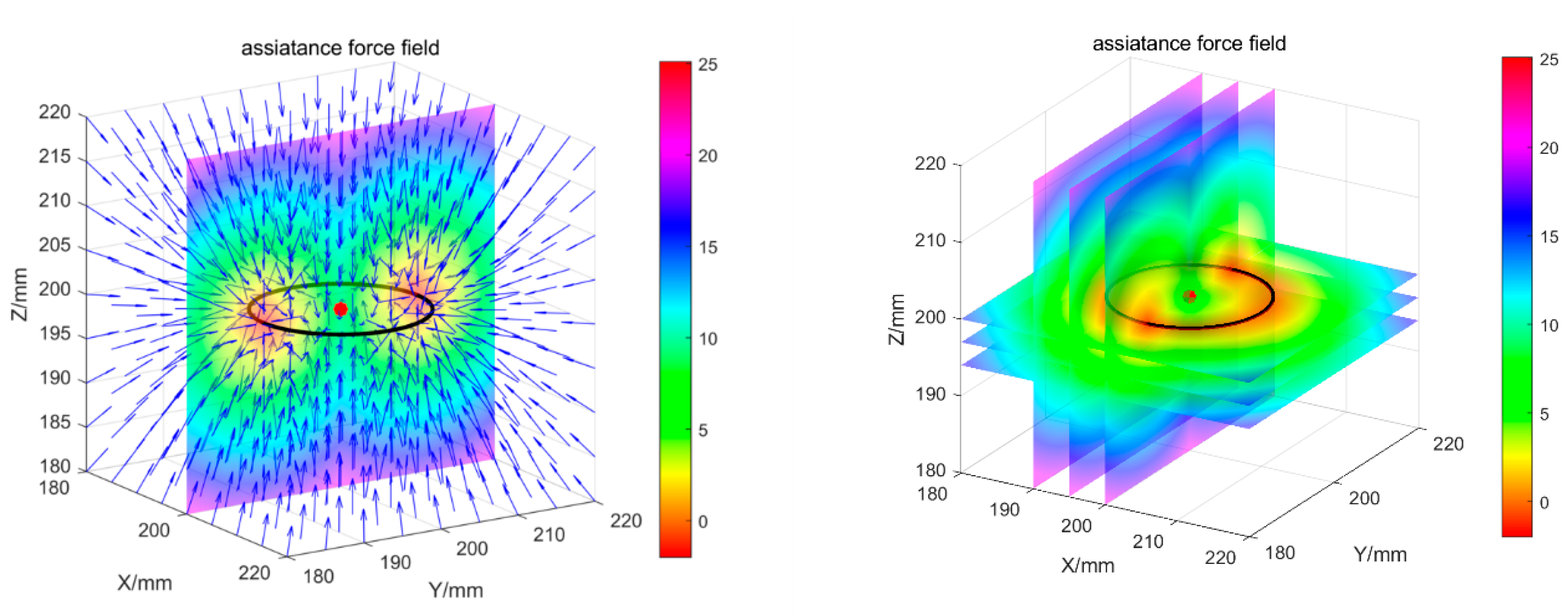
- Among the controller presented in this paper, a virtual stiffness gradient field is constructed around the virtual channel to avoid large deviation from the desired path. The controller forms a bounded controllable spatial normal force field around the desired trajectory.
2. Development of the End-Effector Upper Limb Rehabilitation Robot (EULRR)
2.1. Mechanical Design of the EULRR
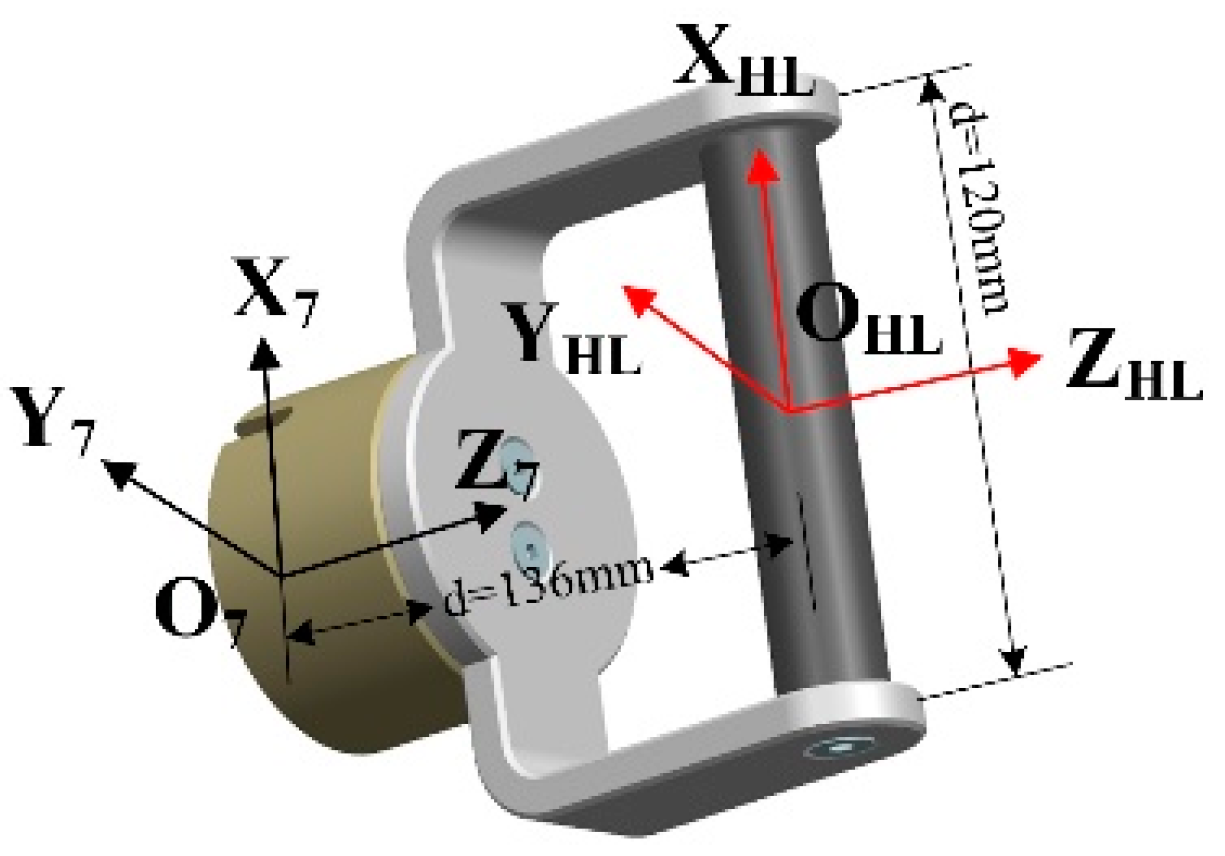
2.2. Kinematics Modeling of EULRR
3. Assist-As-Needed Control of the EULRR
3.1. Dynamic Modeling and Impedance Control of Robot
3.2. Assist-As-Needed Control Based on Cartesian Impedance Control
4. Experiments and Results
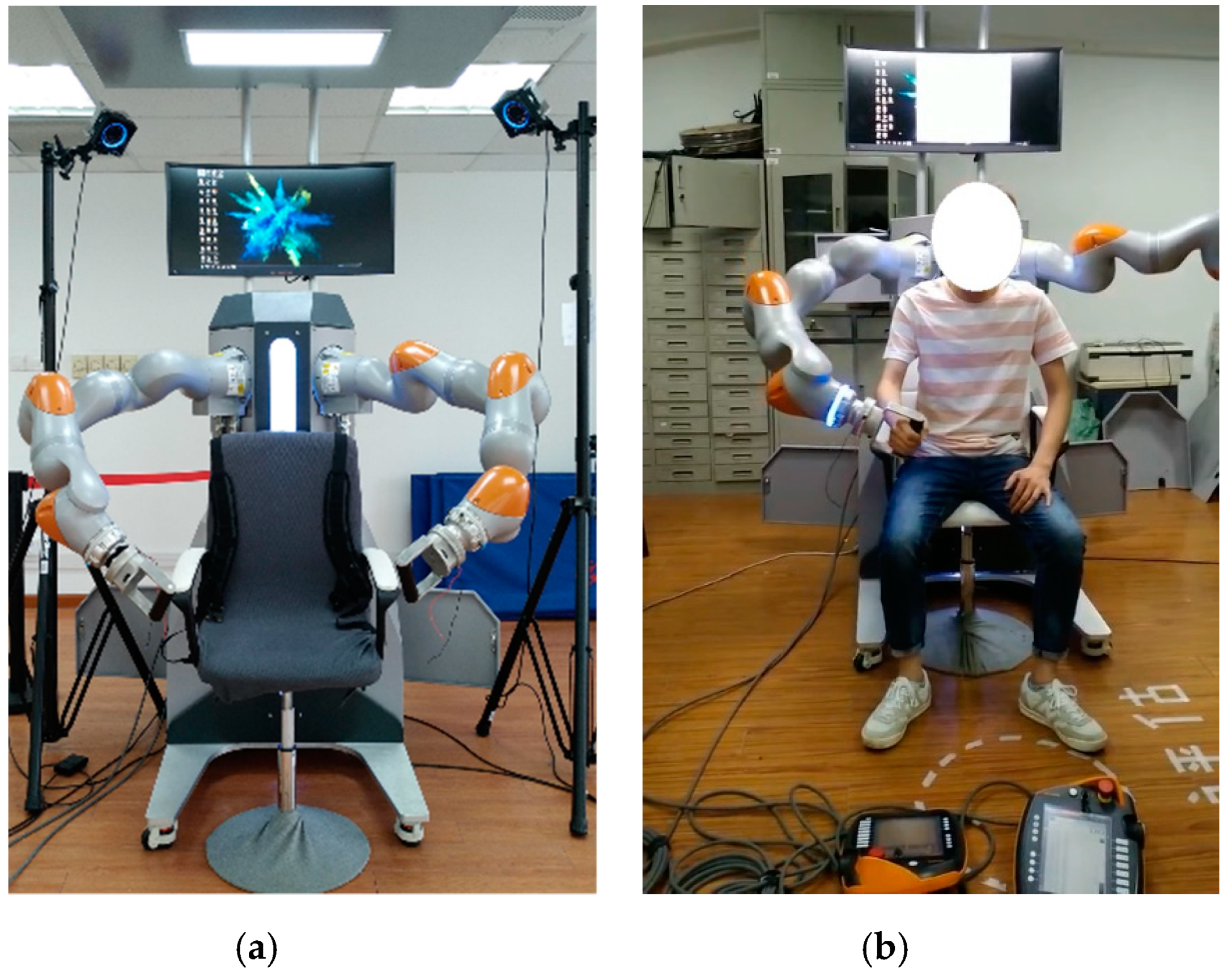
4.1. Experiment Setup
4.2. Data Analysis
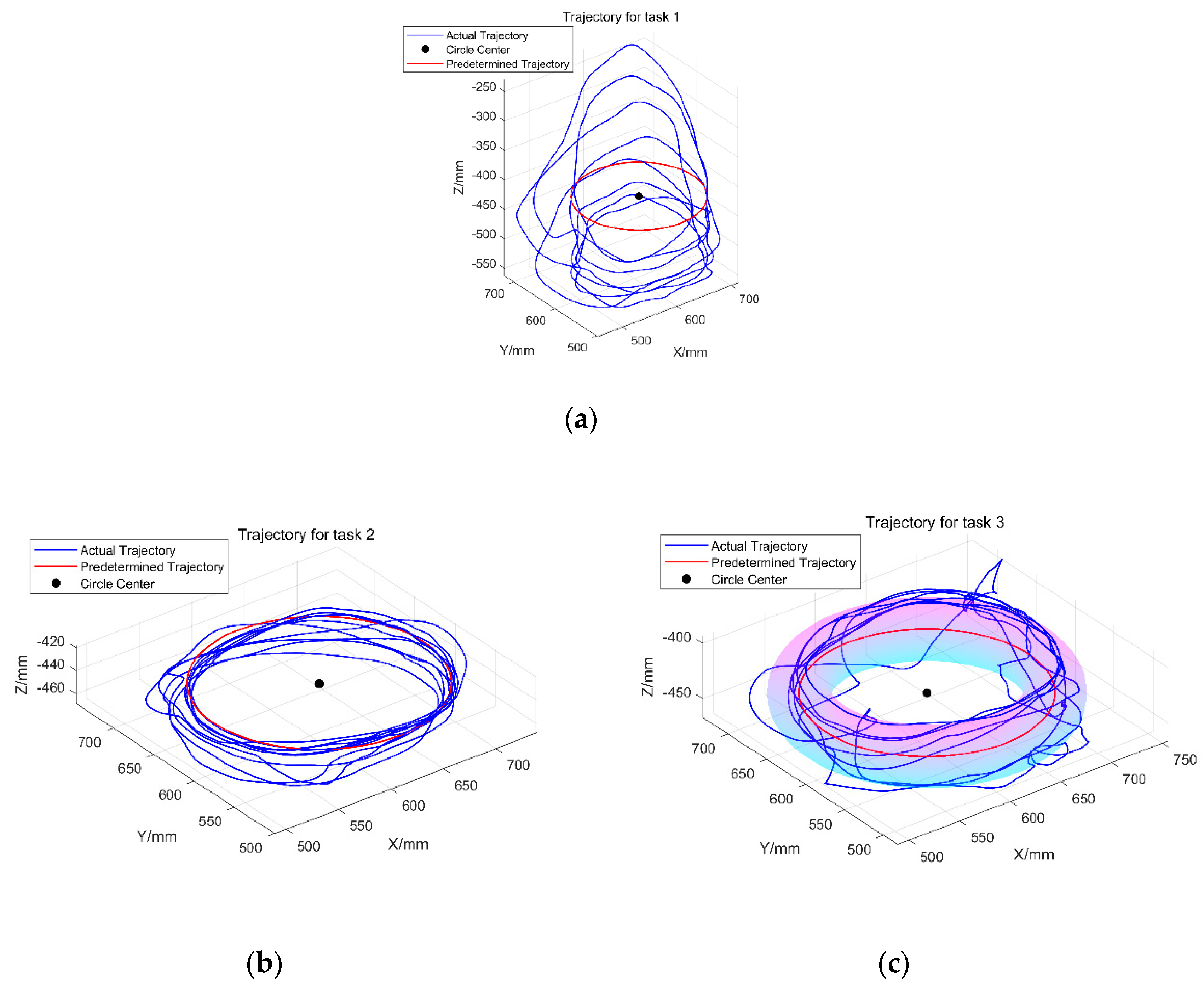
4.3. Experiment Results
5. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Battiston, B.; Titolo, P.; Ciclamini, D.; Panero, B. Peripheral Nerve Defects: Overviews of Practice in Europe. Hand Clin. 2017, 33, 545. [Google Scholar] [CrossRef] [PubMed]
- Bertani, R.; Melegari, C.; Maria, C.; Bramanti, A.; Bramanti, P.; Calabrò, R.S. Effects of robot-assisted upper limb rehabilitation in stroke patients: A systematic review with meta-analysis. Neurol. Sci. 2017, 38, 1561–1569. [Google Scholar] [CrossRef] [PubMed]
- Milot, M.; Spencer, S.J.; Chan, V.; Allington, J.P.; Klein, J.; Chou, C.; Bobrow, J.E.; Cramer, S.C.; Reinkensmeyer, D.J. A crossover pilot study evaluating the functional outcomes of two different types of robotic movement training in chronic stroke survivors using the arm exoskeleton BONES. J. Neuroeng. Rehabil. 2013, 10, 112. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Hädrich, A.; Platz, T.; Kugler, J.; Pohl, M. Electromechanical and robot-assisted arm training for improving generic activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst. Rev. 2012, 6, CD006876. [Google Scholar]
- Roger, G.; Volker, D. Rehabilitation robots for the treatment of sensorimotor deficits: A neurophysiological perspective. J. Neuroeng. Rehabil. 2018, 15, 46. [Google Scholar]
- Krebs, H.I.; Ferraro, M.; Buerger, S.P.; Newbery, M.J.; Makiyama, A.; Sandmann, M.; Lynch, D.; Volpe, B.T.; Hogan, N. Rehabilitation robotics: Pilot trial of a spatial extension for MIT-Manus. J. Neuroeng. Rehabil. 2004, 1, 5. [Google Scholar] [CrossRef]
- Rui, L.; Amirabdollahian, F.; Topping, M.; Driessen, B.; Harwin, W. Upper Limb Robot Mediated Stroke Therapy—GENTLE/s Approach. Auton. Robots 2003, 15, 35–51. [Google Scholar]
- Toth, A.; Nyitrai, D.; Jurak, M.; Merksz, I.; Fazekas, G.; Denes, Z. Safe robot therapy: Adaptation and usability test of a three-position enabling device for use in robot mediated physical therapy of stroke. In Proceedings of the IEEE International Conference on Rehabilitation Robotics, Kyoto, Japan, 23–26 June 2009. [Google Scholar]
- Nef, T.; Guidali, M.; Riener, R. ARMin III—Arm therapy exoskeleton with an ergonomic shoulder actuation. Appl. Bionics Biomech. 2009, 6, 127–142. [Google Scholar] [CrossRef]
- Sugar, T.G.; He, J.; Koeneman, E.J.; Koeneman, J.B.; Herman, R.; Huang, H.; Schultz, R.S.; Herring, D.E.; Wanberg, J.; Balasubramanian, S. Design and control of RUPERT: A device for robotic upper extremity repetitive therapy. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 336–346. [Google Scholar] [CrossRef]
- Ruffaldi, E.; Barsotti, M.; Leonardis, D.; Bassani, G.; Frisoli, A.; Bergamasco, M. Evaluating Virtual Embodiment with the ALEx Exoskeleton[M]// Haptics: Neuroscience, Devices, Modeling, and Applications; Springer: Heidelberg, Germany, 2014. [Google Scholar]
- Akiyama, Y.; Yamada, Y.; Okamoto, S. Interaction forces beneath cuffs of physical assistant robots and their motion-based estimation. Adv. Robot. 2015, 29, 15. [Google Scholar] [CrossRef]
- Chang, W.H.; Kim, Y.H. Robot-assisted Therapy in Stroke Rehabilitation. J. Stroke 2013, 15, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Proietti, T.; Crocher, V.; Roby-Brami, A.; Jarrasse, N. Upper-limb robotic exoskeletons for neurorehabilitation: A review on control strategies. IEEE Rev. Biomed. Eng. 2016, 9, 4–14. [Google Scholar] [CrossRef]
- Babaiasl, M.; Mahdioun, S.H.; Jaryani, P.; Yazdani, M. A review of technological and clinical aspects of robot-aided rehabilitation of upper-extremity after stroke. Disabil. Rehabil. Assist. Technol. 2016, 11, 263–280. [Google Scholar] [CrossRef]
- Tucker, M.R.; Olivier, J.; Pagel, A.; Bleuler, H.; Bouri, M.; Lambercy, O.; Millán, J.D.R.; Riener, R.; Vallery, H.; Gassert, R. Control strategies for active lower extremity prosthetics and orthotics: A review. J. NeuroEng. Rehabil. 2015, 12, 1. [Google Scholar] [CrossRef]
- Brunnstrom, S.; Sawner, K.A.; Lavigne, J.M. Brunnstrom’s Movement Therapy in Hemiplegia: A Neurophysiological Approach; Lippincott: Philadelphia, PA, USA, 1992. [Google Scholar]
- Hogan, N.; Krebs, H.I.; Rohrer, B.; Palazzolo, J.J.; Dipietro, L.; Fasoli, S.E.; Stein, J.; Hughes, R.; Frontera, W.R.; Lynch, D. Motions or muscles? Some behavioral factors underlying robotic assistance of motor recovery. J. Rehabil. Res. Dev. 2006, 43, 605. [Google Scholar] [CrossRef] [PubMed]
- Emken, J.L.; Bobrow, J.E.; Reinkensmeyer, D.J. Robotic movement training as an optimization problem: Designing a controller that assists only as needed. In Proceedings of the 9th International Conference on Rehabilitation Robotics, Chicago, IL, USA, 28 June–1 July 2005. [Google Scholar]
- Pehlivan, A.U.; Losey, D.P.; Ormalley, M.K. Minimal Assist-as-Needed (mAAN) Controller for Upper Limb Robotic Rehabilitation. IEEE Trans. Robot. 2015, 32, 113–124. [Google Scholar] [CrossRef]
- Pehlivan, A.; Sergi, F.; O’Malley, M. A Subject-Adaptive Controller for Wrist Robotic Rehabilitation. IEEE/ASME Trans. Mechatron. 2014, 20, 1338–1350. [Google Scholar] [CrossRef]
- Jabbari Asl, H.; Narikiyo, T.; Kawanishi, M. An assist-as-needed control scheme for robot-assisted rehabilitation. In Proceedings of the 2017 American Control Conference (ACC), Seattle, WA, USA, 24–26 May 2017; pp. 198–203. [Google Scholar]
- Grosmaire, A.G.; Duret, C. Does assist-as-needed upper limb robotic therapy promote participation in repetitive activity-based motor training in sub-acute stroke patients with severe paresis? Neurorehabilitation 2017, 41, 31–39. [Google Scholar] [CrossRef]
- Hogan, N. Impedance control: An approach to manipulation. Part I, II, III. In Proceedings of the American Control Conference, San Diego, CA, USA, 6–8 June 1984. [Google Scholar]
- Hui, G.; Misgeld, B.J.E.; Shi, Y.; Ji, L. Dynamic Modeling and Interactive Performance of PARM: A Parallel Upper-Limb Rehabilitation Robot Using Impedance Control for Patients after Stroke. J. Healthc. Eng. 2018, 2018, 8647591. [Google Scholar]
- Huo, J.; Zhang, X.; Ji, R.; Liu, Y.; Bi, S.; Ji, L.; Li, C. Development and Implementation of an End-Effector Upper Limb Rehabilitation Robot for Hemiplegic Patients with Line and Circle Tracking Training. J. Healthc. Eng. 2017, 2017, 4931217. [Google Scholar]
- Perez-Ibarra, J.C.; Siqueira, A.A.; Silva-Couto, M.A.; de Russo, T.L.; Krebs, H.I. Adaptive Impedance Control Applied to Robot-Aided Neuro-Rehabilitation of the Ankle. IEEE Robot. Autom. Lett. 2018, 4, 185–192. [Google Scholar] [CrossRef]
- Cui, X.; Chen, W.; Jin, X.; Agrawal, S.K. Design of a 7-DOF Cable-Driven Arm Exoskeleton (CAREX-7) and a Controller for Dexterous Motion Training or Assistance. IEEE/ASME Trans. Mechatron. 2017, 22, 161–172. [Google Scholar] [CrossRef]
- Asl, H.J.; Yamashita, M.; Narikiyo, T.; Kawanishi, M. Field-Based Assist-As-Needed Control Schemes for Rehabilitation Robots. IEEE/ASME Trans. Mechatron. 2020, 25, 2100–2111. [Google Scholar] [CrossRef]
- Brokaw, E.B.; Murray, T.; Nef, T.; Lum, P.S. Retraining of interjoint arm coordination after stroke using robot-assisted time-independent functional training. J. Rehabil. Res. Dev. 2011, 48, 299–316. [Google Scholar] [CrossRef]
- Proietti, T.; Guigon, E. Modifying upper-limb inter-joint coordination in healthy subjects by training with a robotic exoskeleton. J. Neuroeng. Rehabil. 2017, 14, 55. [Google Scholar] [CrossRef]
- Agarwal, P. and Deshpande, A.D. Subject-Specific Assist-as-Needed Controllers for a Hand Exoskeleton for Rehabilitation. IEEE Robot. Autom. Lett. 2018, 3, 508–515. [Google Scholar] [CrossRef]
- Khairuddin, I.M.; Sidek, S.N.; Yusof, H.M.; Baarath, K.; Majeed, A.P. Assistive-as-Needed Strategy for Upper-Limb Robotic Systems: An Initial Survey. IOP Conf. Ser. Mater. Sci. Eng. 2017, 260, 12027. [Google Scholar] [CrossRef]
- Klopčar, N.; Lenarčič, J. Kinematic Model for Determination of Human Arm Reachable Workspace. Meccanica 2005, 40, 203–219. [Google Scholar] [CrossRef]
- Kaya, M.D.; Hasiloglu, A.S.; Bayramoglu, M.; Yesilyurt, H.; Ozok, A.F. A new approach to estimate anthropometric measurements by adaptive neuro-fuzzy inference system. Int. J. Ind. Ergon. 2003, 32, 105–114. [Google Scholar] [CrossRef]
- Fransson, C.; Winkel, J. Hand strength: The influence of grip span and grip type. Ergonomics 1991, 34, 881–892. [Google Scholar] [CrossRef]
- Jordan, M.; Benitez, L.M.V.; Schmidt, S.; Folgheraiter, M.; Albiez, J. Model-Based Control and Design of a Low-Pressure Fluid Actuation System for Haptic Devices. In Proceedings of the ACTUATOR 2012, 13th International Conference on New Actuators, Bremen, Germany, 18–20 June 2012. [Google Scholar]
- Rodrigues, T.A.; Goroso, D.G.; Westgate, P.M.; Carrico, C.; Batistella, L.R.; Sawaki, L. Slow Versus Fast Robot-Assisted Locomotor Training After Severe Stroke. Am. J. Phys. Med. Rehabil. 2017, 96, S165–S170. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, R.; Kurth, J.; Schreiber, G.; Koeppe, R.; Hirzinger, G. The KUKA-DLR Lightweight Robot arm—A new reference platform for robotics research and manufacturing. In Proceedings of the ISR 2010 (41st International Symposium on Robotics) and ROBOTIK 2010 (6th German Conference on Robotics), Munich, Germany, 7–9 June 2010. [Google Scholar]
- Schreiber, G.; Stemmer, A.; Bischoff, R. The Fast Research Interface for the KUKA Lightweight Robot. In Proceedings of the Workshop on IEEE ICRA 2010 Workshop on Innovative Robot Control Architectures for Demanding (Research) Applications—How to Modify and Enhance Commercial Controllers, Anchorage, AK, USA, 3–8 May 2010. [Google Scholar]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Link | Motion Range/(°) | ||||
|---|---|---|---|---|---|
| 1 | −90 | 0 | 340 | −170~170 | |
| 2 | 90 | 0 | 0 | −120~120 | |
| 3 | 90 | 0 | 400 | −170~170 | |
| 4 | −90 | 0 | 0 | −120~120 | |
| 5 | −90 | 0 | 400 | −170~170 | |
| 6 | 90 | 0 | 0 | −120~120 | |
| 7 | 0 | 0 | 152 | −175~175 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, L.; Guo, S.; Sun, Q. Development and Assist-As-Needed Control of an End-Effector Upper Limb Rehabilitation Robot. Appl. Sci. 2020, 10, 6684. https://doi.org/10.3390/app10196684
Zhang L, Guo S, Sun Q. Development and Assist-As-Needed Control of an End-Effector Upper Limb Rehabilitation Robot. Applied Sciences. 2020; 10(19):6684. https://doi.org/10.3390/app10196684
Chicago/Turabian StyleZhang, Leigang, Shuai Guo, and Qing Sun. 2020. "Development and Assist-As-Needed Control of an End-Effector Upper Limb Rehabilitation Robot" Applied Sciences 10, no. 19: 6684. https://doi.org/10.3390/app10196684
APA StyleZhang, L., Guo, S., & Sun, Q. (2020). Development and Assist-As-Needed Control of an End-Effector Upper Limb Rehabilitation Robot. Applied Sciences, 10(19), 6684. https://doi.org/10.3390/app10196684