Urinary 1H-NMR Metabolic Signature in Subjects Undergoing Colonoscopy for Colon Cancer Diagnosis

 , ,
, , 
 ,
, 
Abstract
Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Sample Collection
2.2. Urine Samples Preparation
2.3. 1H-NMR Spectroscopic Analysis
2.4. NMR Data Preprocessing and Multivariate Statistical Analysis
2.5. Serum Carcinoembryonic Antigen Level Determination
3. Results
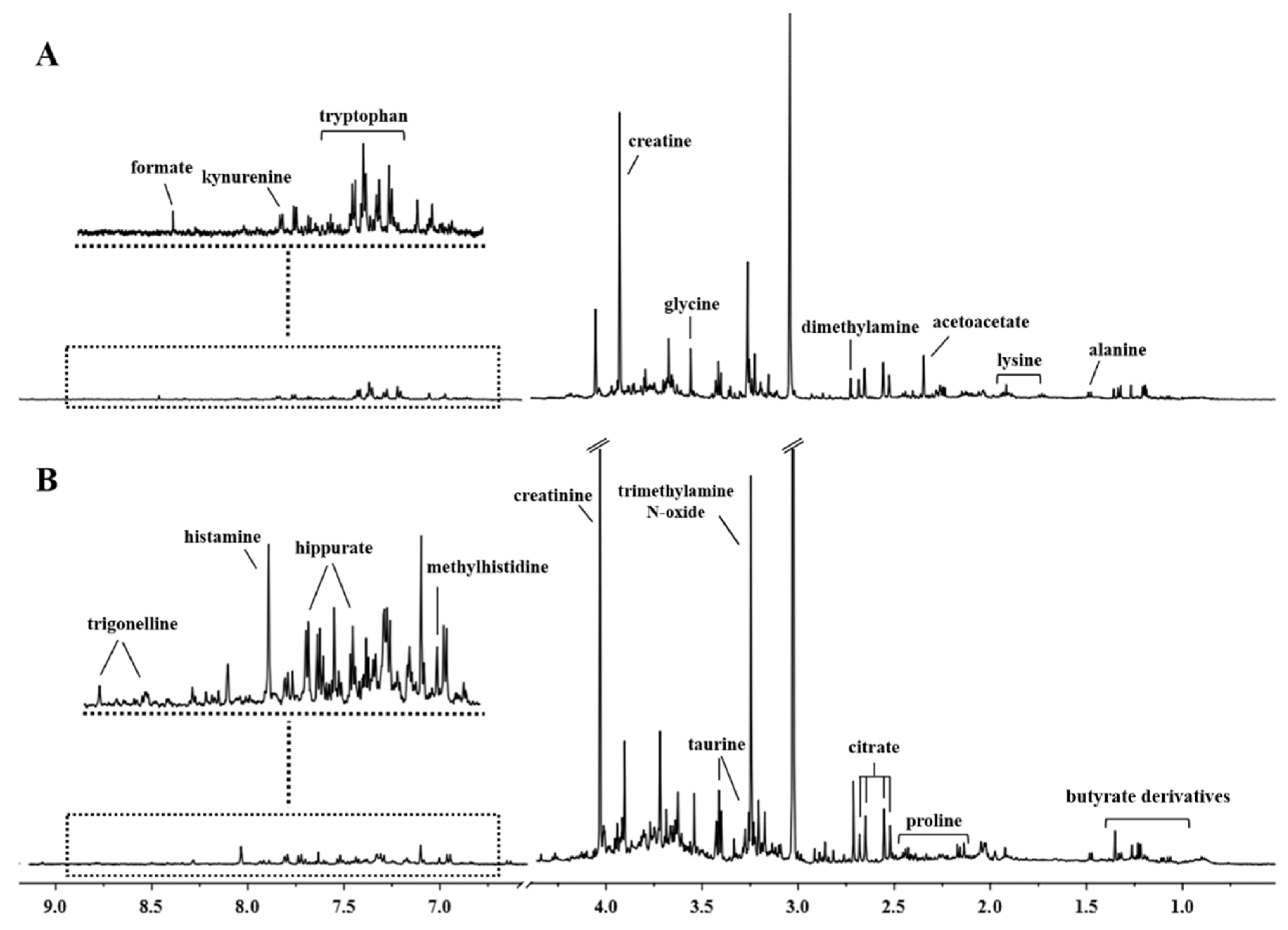
3.1. 1H-NMR Spectra of Urine Samples
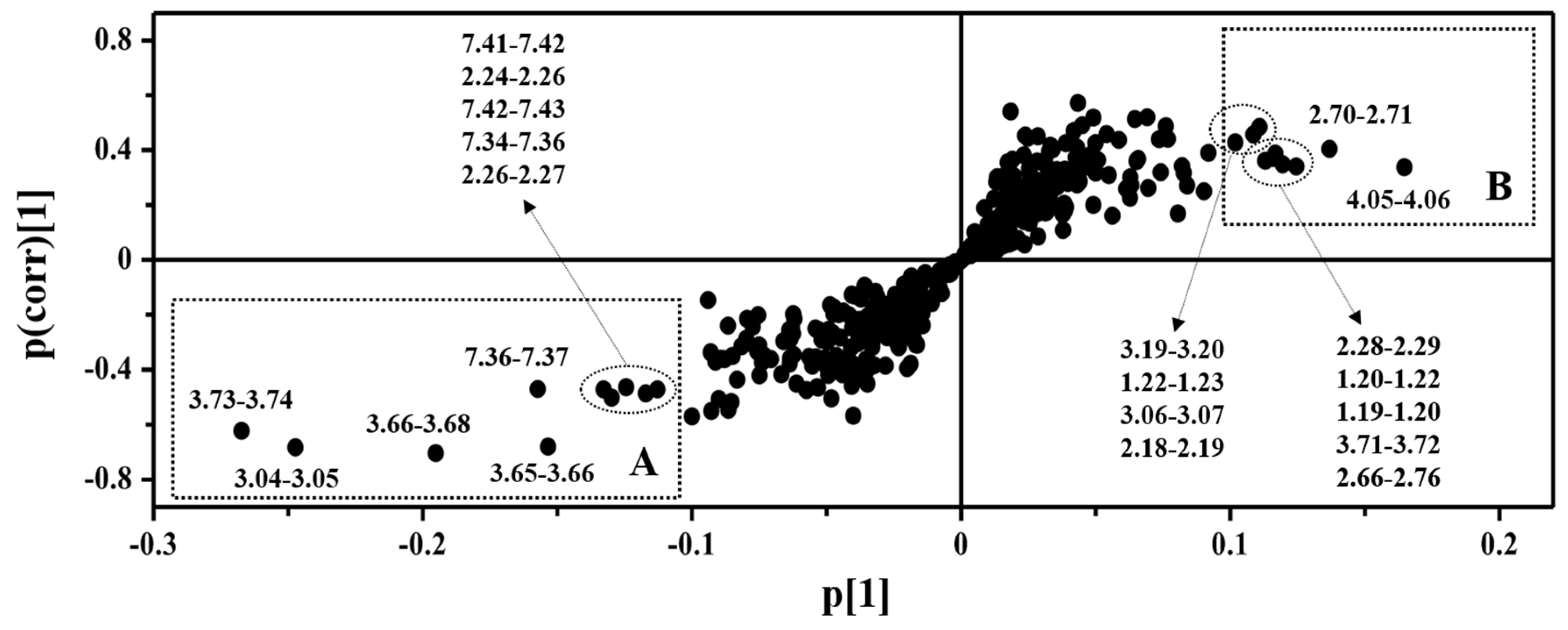
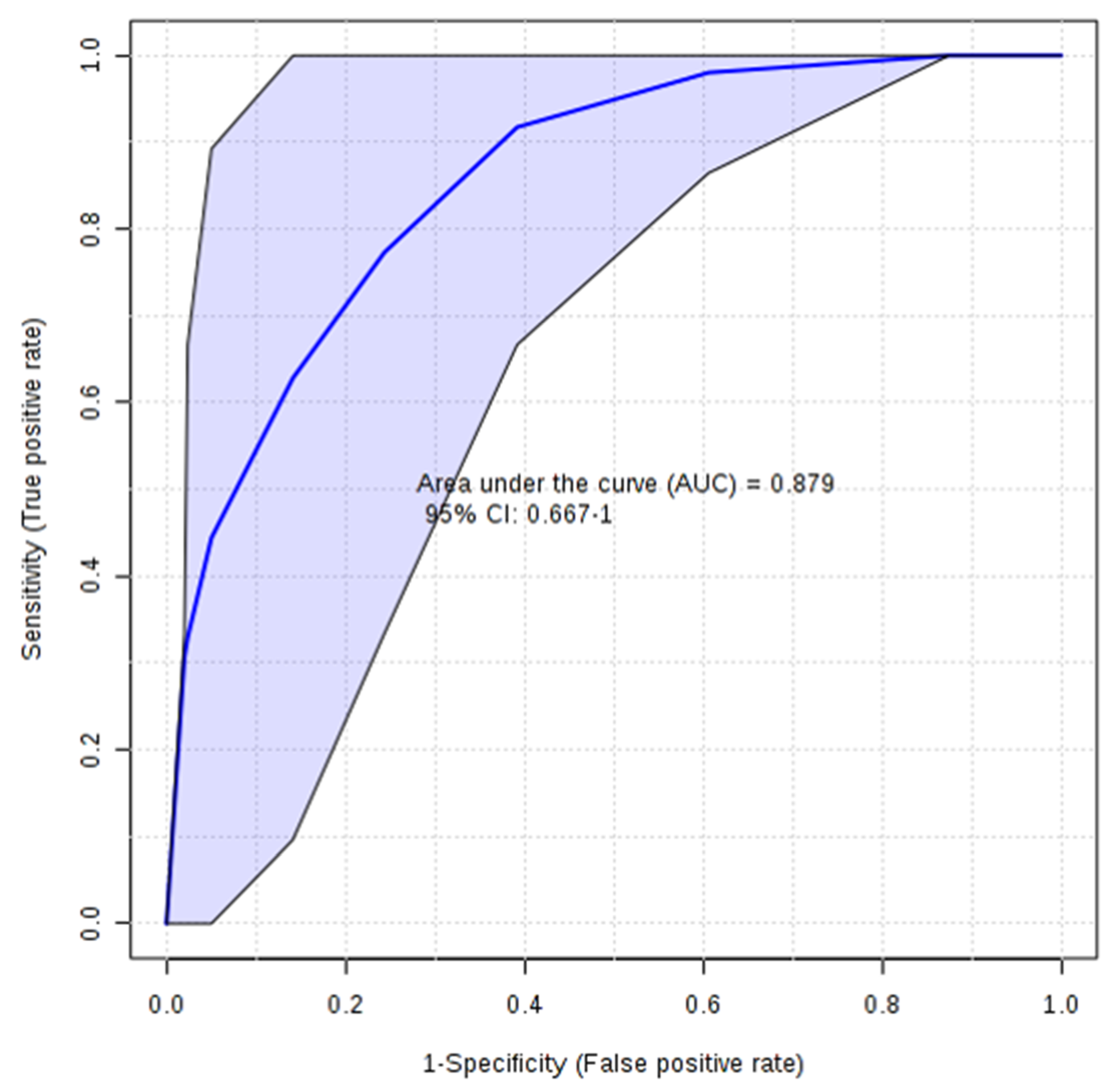
3.2. Multivariate Statistical Analysis of NMR Data
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Soerjomataram, I.; Lortet-Tieulent, J.; Parkin, D.M.; Ferlay, J.; Mathers, C.; Forman, D.; Bray, F. Global burden of cancer in 2008: A systematic analysis of disability-adjusted life-years in 12 world regions. Lancet 2012, 380, 1840–1850. [Google Scholar] [CrossRef]
- El-Awady, S.; Lithy, R.; Morshed, M.; Khafagy, W.; Abd Monem, H.; Waleed, O.; Badr, S.; Fekry, A.; El Nakeeb, A.; Ghazy, H.; et al. Utility of serum preoperative carcinoembryonic antigen in colorectal cancer patients. Hepato-Gastroenterology 2009, 56, 361–366. [Google Scholar] [PubMed]
- Hewitson, P.; Glasziou, P.; Watson, E.; Towler, B.; Irwig, L. Cochrane systematic review of colorectal cancer screening using the fecal occult blood test (hemoccult): An update. Am. J. Gastroenterol. 2008, 103, 1541–1549. [Google Scholar] [CrossRef] [PubMed]
- Ahlquist, D.A.; Hongzhi, Z.; Domanico, M.; Mahoney, D.W.; Yab, T.C.; Taylor, W.R.; Butz, M.L.; Thibodeau, S.N.; Rabeneck, L.; Paszat, L.F.; et al. Next-Generation Stool DNA Test Accurately Detects Colorectal Cancer and Large Adenomas. Gastroenterology 2012, 142, 248–256. [Google Scholar] [CrossRef]
- Grady, W.M.; Markowitz, S.D. The molecular pathogenesis of colorectal cancer and its potential application to colorectal cancer screening. Dig. Dis. Sci. 2015, 60, 762–772. [Google Scholar] [CrossRef]
- Jung, J.; Jung, Y.; Bang, E.J.; Cho, S.; Jang, Y.J.; Kwak, J.M.; Ryu, D.H.; Park, S.; Hwang, G.S. Noninvasive diagnosis and evaluation of curative surgery for gastric cancer by using NMR-based metabolomic profiling. Ann. Surg. Oncol. 2014, 21, 736–742. [Google Scholar] [CrossRef]
- Nicholson, J.K.; Holmes, E.; Kinross, J.M.; Darzi, A.W.; Takats, Z.; Lindon, J.C. Metabolic phenotyping in clinical and surgical environments. Nature 2012, 491, 384–392. [Google Scholar] [CrossRef]
- Chan, E.C.Y.; Koh, P.K.; Mal, M.; Cheah, P.Y.; Eu, K.W.; Backshall, A.; Cavill, R.; Nicholson, J.K.; Keun, H.C. Metabolic profiling of human colorectal cancer using high-resolution magic angle spinning nuclear magnetic resonance (HR-MAS NMR) spectroscopy and gas chromatography mass spectrometry (GC/MS). J. Proteome Res. 2009, 8, 352–361. [Google Scholar] [CrossRef]
- Barberini, L.; Restivo, A.; Noto, A.; Deidda, S.; Fattuoni, C.; Fanos, V.; Saba, L.; Zorcolo, L.; Mussap, M. A gas chromatography-mass spectrometry (GC-MS) metabolomics approach in human colorectal cancer (CRC): The emerging role of monosaccharides and amino acids. Ann. Transl. Med. 2019, 7, 727. [Google Scholar] [CrossRef]
- Cheng, Y.; Xie, G.; Chen, T.; Qiu, Y.; Zou, X.; Zheng, M.; Tan, B.; Feng, B.; Don, T.; He, P.; et al. Distinct urinary metabolic profile of human colorectal cancer. J. Proteome Res. 2012, 11, 1354–1363. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Lin, Y.; Liang, J.; Huang, Y.; Ma, C.; Liu, X.; Yang, J. NMR-based metabolomic techniques identify potential urinary biomarkers for early colorectal cancer detection. Oncotarget 2017, 8, 105819–105831. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, B.D.; Shinkins, B.; Pathiraja, I.; Roberts, N.W.; James, T.J.; Mallett, S.; Perera, R.; Primrose, J.N.; Mant, D. Blood CEA levels for detecting recurrent colorectal cancer. Cochrane Database Syst. Rev. 2015, 12, CD011134. [Google Scholar] [CrossRef] [PubMed]
- Piras, C.; Pintus, R.; Pruna, D.; Dessì, A.; Atzori, L.; Fanos, V. Pediatric Acute-onset Neuropsychiatric Syndrome and Mycoplasma PneumoniaeInfection: A Case Report Analysis with a Metabolomics Approach. Curr. Pediatr. Rev. 2019, 15. [Google Scholar] [CrossRef] [PubMed]
- Sousa, S.A.A.; Magalhaes, A.; Ferreira, M.M.C. Optimized bucketing for NMR spectra: Three case studies. Chemometr. Intell. Lab. 2013, 122, 93–102. [Google Scholar] [CrossRef]
- Wu, Y.; Li, L. Sample normalization methods in quantitative metabolomics. J. Chromatogr. A 2016, 1430, 80–95. [Google Scholar] [CrossRef]
- Weljie, A.M.; Newton, J.; Mercier, P.; Carlson, E.; Slupsky, C.M. Targeted Profiling: Quantitative Analysis of 1HNMR Metabolomics Data. Anal. Chem. 2006, 2, 4430–4442. [Google Scholar] [CrossRef]
- Chong, J.; Soufan, O.; Li, C.; Caraus, I.; Li, S.; Bourque, G.; Wishart, D.S.; Xia, J. MetaboAnalyst 4.0: Towards more transparent and integrative metabolomics analysis. Nucl. Acids Res. 2018, 46, W486–W494. [Google Scholar] [CrossRef]
- Schicho, R.; Shaykhutdinov, R.; Ngo, J.; Nazyrova, A.; Schneider, C.; Panaccione, R.; Kaplan, G.G.; Vogel, H.J.; Storr, M. Quantitative metabolomic profiling of serum, plasma, and urine by 1H-NMR spectroscopy discriminates between patients with inflammatory bowel disease and healthy individuals. J. Proteome Res. 2012, 11, 3344–3357. [Google Scholar] [CrossRef]
- Bathe, O.F.; Farshidfar, F. From Genotype to Functional Phenotype: Unraveling the Metabolomic Features of Colorectal Cancer. Genes 2014, 5, 536–560. [Google Scholar] [CrossRef]
- Lin, J.K.; Lin, C.C.; Yang, S.H.; Wang, H.S.; Jiang, J.K.; Lan, Y.T.; Lin, T.C.; Li, A.F.Y.; Chen, W.S.; Chang, S.C. Early postoperative CEA level is a better prognostic indicator than is preoperative CEA level in predicting prognosis of patients with curable colorectal cancer. Int. J. Colorectal Dis. 2011, 26, 1135–1141. [Google Scholar] [CrossRef]
- Wang, H.; Tso, V.; Wong, C.; Sadowski, D.; Fedorak, R.N. Development and Validation of a Highly Sensitive Urine-Based Test to Identify Patients with Colonic Adenomatous Polyps. Clin. Trans. Gastroenterol. 2014, 5, e54. [Google Scholar] [CrossRef] [PubMed]
- Jobard, E.; Pontoizeau, C.; Blaise, B.J.; Bachelot, T.; Elena-Herrmann, B.; Trédan, O. A serum nuclear magnetic resonance-based metabolomic signature of advanced metastatic human breast cancer. Cancer Lett. 2014, 343, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Argiles, J.; Azco Bieto, J. The metabolic environment of cancer. Mol. Cell. Biochem. 1988, 81, 3–17. [Google Scholar] [CrossRef] [PubMed]
- Eisner, R.; Stretch, C.; Eastman, T.; Xia, J.; Hau, D.; Damaraju, S.; Greiner, R.; Wishart, D.S.; Baracos, V.E. Learning to predict cancer-associated skeletal muscle wasting from 1H-NMR profiles of urinary metabolites. Metabolomics 2011, 7, 25–34. [Google Scholar] [CrossRef]
- Wyss, M.; Kaddurah-Daouk, R. Creatine and creatinine metabolism. Physiol. Rev. 2000, 80, 1107–1213. [Google Scholar] [CrossRef]
- Bryan, G.T. The role of urinary tryptophan metabolites in the etiology of bladder cancer. Am. J. Clin. Nutr. 1971, 24, 841–847. [Google Scholar] [CrossRef]
- Denz, H.; Orth, B.; Weiss, G.; Herrmann, R.; Huber, P.; Wachter, H.; Fuchs, D. Weight loss in patients with hematological neoplasias is associated with immune system stimulation. Clin. Investig. 1993, 71, 37–41. [Google Scholar] [CrossRef]
- Carlin, J.M.; Ozaki, Y.; Byrne, G.I.; Brown, R.R.; Borden, E.C. Interferons and indoleamine 2,3-dioxygenase: Role in antimicrobial and antitumor effects. Experientia 1989, 45, 535–541. [Google Scholar] [CrossRef]
- Murr, C.; Bergant, A.; Widschwendter, M.; Heim, K.; Schrocksnadel, H.; Fuchs, D. Neopterin is an independent prognostic variable in females with breast cancer. Clin. Chem. 1999, 45, 1998–2004. [Google Scholar] [CrossRef]
- Platten, M.; Wick, W.; Van den Eynde, B.J. Tryptophan catabolism in cancer: Beyond IDO and tryptophan depletion. Cancer Res. 2012, 72, 5435–5440. [Google Scholar] [CrossRef]
- Medina, V.A.; Rivera, E.S. Histamine receptors and cancer pharmacology. Br. J. Pharmacol. 2010, 161, 755–767. [Google Scholar] [CrossRef] [PubMed]
- Cricco, G.P.; Mohamad, N.A.; Sambuco, L.A.; Genre, F.; Croci, M.; Gutiérrez, A.S.; Medina, V.A.; Bergoc, R.M.; Rivera, E.S.; Martín, G.A. Histamine regulates pancreatic carcinoma cell growth through H3 and H4 receptors. Inflamm. Res. 2008, 57, 23–24. [Google Scholar] [CrossRef] [PubMed]
- Medina, V.; Croci, M.; Crescenti, E.; Mohamad, N.; Sanchez-Jiménez, F.; Massari, N.; Nuñez, M.; Cricco, G.; Martin, G.; Bergoc, R.; et al. The role of histamine in human mammary carcinogenesis: H3 and H4 receptors as potential therapeutic targets for breast cancer treatment. Cancer Biol. Ther. 2008, 7, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Cai, G.; Su, M.; Chen, T.; Liu, Y.; Xu, Y.; Ni, Y.; Zhao, A.; Cai, S.; Xu, L.X. Urinary metabonomic study on colorectal cancer. J. Proteome Res. 2010, 9, 1627–1634. [Google Scholar] [CrossRef]
- Deng, L.; Ismond, K.; Liu, Z.; Constable, J.; Wang, H.; Alatise, O.I.; Weiser, M.R.; Kingham, T.P.; Chang, D. Urinary Metabolomics to Identify a Unique Biomarker Panel for Detecting Colorectal Cancer: A Multicentre Study. Cancer Epidemiol. Prev. Biomark. 2019, 28, 1283–1291. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CRC Patients | Controls | |
|---|---|---|
| Number | 14 | 10 |
| Age (median, range) | 67.4, 40–88 | 56.3, 47–67 |
| Male/female ratio | 11/3 | 7/3 |
| CEA (>2.5 ng/mL) | 5 | 0 |
| Cancer site | ||
| Colon | 6 | - |
| Rectum | 7 | - |
| Caecum | 1 | - |
| FOBT | ||
| Positive | 9 | N/A |
| Negative | 5 | N/A |
| Dukes’ Stage | ||
| A | 3 | - |
| B | 7 | - |
| C | 3 | - |
| D | 1 | - |
| Metabolites | Mean (SD) of Group (mM) a | p-Value b | FC c (log2 CRC/C) | |
|---|---|---|---|---|
| C | CRC | |||
| Phenylacetylglycine | 2.07 ± 0.65 | 1.34 ± 0.72 | 0.01 | −0.623 |
| Histamine | 1.14 ± 0.49 | 2.26 ± 0.85 | 0.02 | 0.988 |
| Creatine | 6.64 ± 3.34 | 1.49 ± 0.98 | 0.03 | −2.150 |
| Tryptophan | 1.01 ± 0.46 | 0.71 ± 0.27 | 0.03 | −0.517 |
| Acetoacetate | 0.85 ± 0.28 | 1.64 ± 1.37 | 0.05 | 0.970 |
| Creatinine | 26.12 ± 17.96 | 37.83 ± 14.59 | 0.05 | 0.535 |
| 3-hydroxybutyrate | 1.00 ± 0.54 | 1.64 ± 1.45 | 0.10 | 0.706 |
| Tyrosine | 0.82 ± 0.41 | 0.62 ± 0.37 | 0.12 | −0.409 |
| Proline | 2.93 ± 1.12 | 3.38 ± 0.59 | 0.13 | 0.202 |
| 3-Aminoisobutyrate | 1.09 ± 0.54 | 2.08 ± 2.87 | 0.15 | 0.933 |
| Sn-glycero-3-phosphocholine | 1.62 ± 0.67 | 1.88 ± 0.71 | 0.19 | −0.215 |
| Fucose | 1.28 ± 0.54 | 1.16 ± 2.87 | 0.25 | 0.145 |
| Methylhistidine | 1.09 ± 0.67 | 1.23 ± 0.37 | 0.26 | −0.180 |
| Citrate | 8.57 ± 4.12 | 7.53 ± 6.94 | 0.34 | 0.187 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piras, C.; Pibiri, M.; Leoni, V.P.; Cabras, F.; Restivo, A.; Griffin, J.L.; Fanos, V.; Mussap, M.; Zorcolo, L.; Atzori, L. Urinary 1H-NMR Metabolic Signature in Subjects Undergoing Colonoscopy for Colon Cancer Diagnosis. Appl. Sci. 2020, 10, 5401. https://doi.org/10.3390/app10165401
Piras C, Pibiri M, Leoni VP, Cabras F, Restivo A, Griffin JL, Fanos V, Mussap M, Zorcolo L, Atzori L. Urinary 1H-NMR Metabolic Signature in Subjects Undergoing Colonoscopy for Colon Cancer Diagnosis. Applied Sciences. 2020; 10(16):5401. https://doi.org/10.3390/app10165401
Chicago/Turabian StylePiras, Cristina, Monica Pibiri, Vera Piera Leoni, Francesco Cabras, Angelo Restivo, Julian Leether Griffin, Vassilios Fanos, Michele Mussap, Luigi Zorcolo, and Luigi Atzori. 2020. "Urinary 1H-NMR Metabolic Signature in Subjects Undergoing Colonoscopy for Colon Cancer Diagnosis" Applied Sciences 10, no. 16: 5401. https://doi.org/10.3390/app10165401
APA StylePiras, C., Pibiri, M., Leoni, V. P., Cabras, F., Restivo, A., Griffin, J. L., Fanos, V., Mussap, M., Zorcolo, L., & Atzori, L. (2020). Urinary 1H-NMR Metabolic Signature in Subjects Undergoing Colonoscopy for Colon Cancer Diagnosis. Applied Sciences, 10(16), 5401. https://doi.org/10.3390/app10165401