Diagnostic Performance of Serological Assays in the Detection of SARS-CoV-2: A Review


 and
and 
Abstract
Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.2.1. Clinical Question (PICO)
2.2.2. Inclusion and Exclusion Criteria
- -
- Studies that reported serological assay quantitative data (percentages, rates) about the IgM and IgG titers of the analyzed blood samples.
- -
- Studies that tested serological assays recording both IgM and IgG titers.
- -
- Studies in which the analyzed blood samples were taken from patients with certain diagnosis of SARS-CoV-2 infection, obtained through real-time RT-PCR.
- -
- Articles written in the English language.
2.3. Search
2.4. Study Selection and Data Collection Process
2.5. Quality Assessment
3. Results
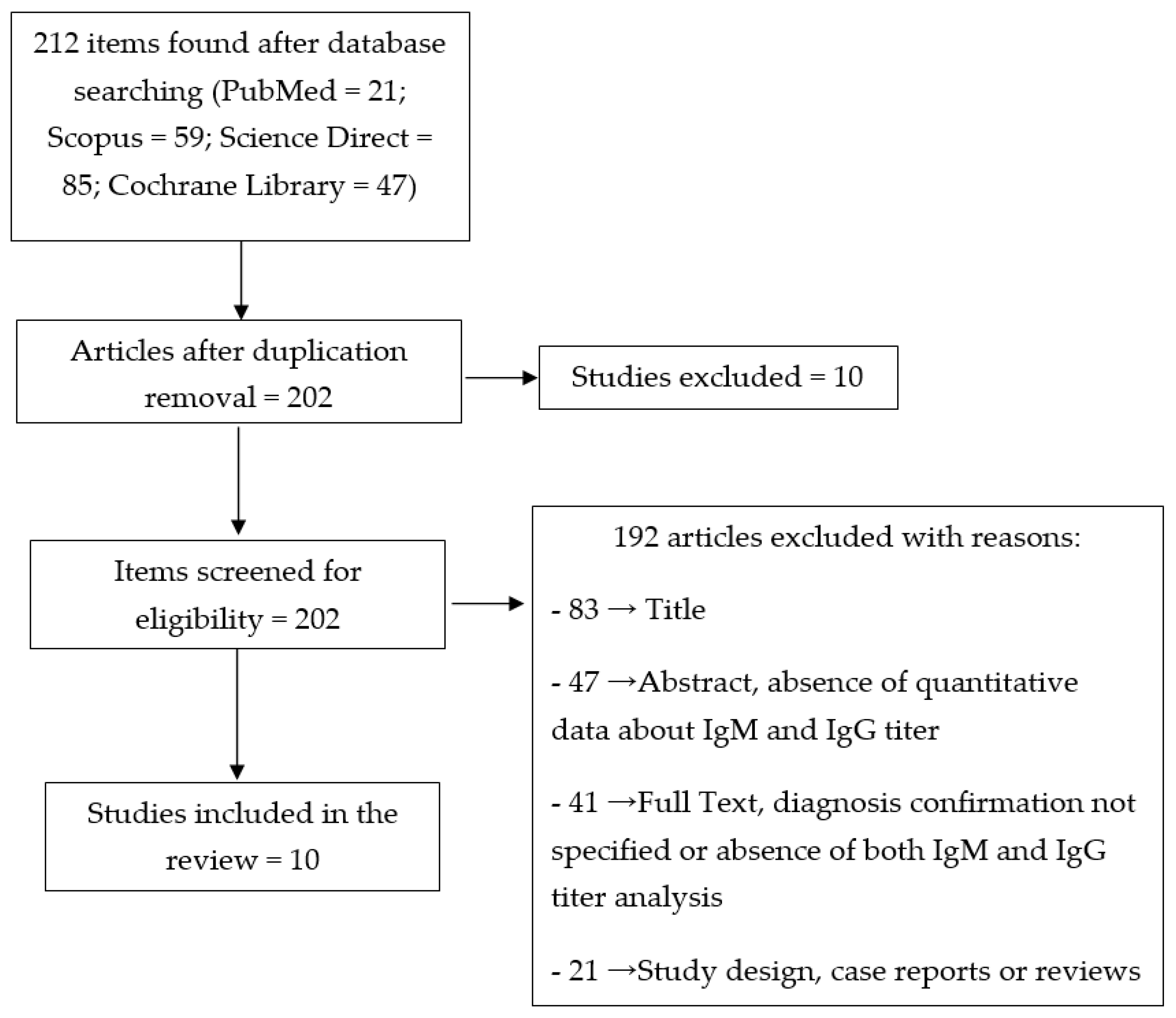
3.1. Study Selection and Characteristics
3.2. Results of Individual Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hu, Y.; Sun, J.; Dai, Z.; Deng, H.; Li, X.; Huang, Q.; Wu, Y.; Sun, L.; Xu, Y. Prevalence and severity of corona virus disease 2019 (COVID-19): A systematic review and meta-analysis. J. Clin. Virol. 2020, 127, 104371. [Google Scholar] [CrossRef] [PubMed]
- Rothan, H.A.; Byrareddy, S.N. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J. Autoimmun. 2020, 109, 102433. [Google Scholar] [CrossRef] [PubMed]
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-jabir, A.; Losifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Ahn, D.G.; Shin, H.J.; Kim, M.H.; Lee, S.; Kim, H.S.; Myoung, J.; Kim, B.T.; Kim, S.J. Current status of epidemiology, diagnosis, therapeutics, and vaccines for novel coronavirus disease 2019 (COVID-19). J. Microbiol. Biotechnol. 2020, 30, 313–324. [Google Scholar] [CrossRef]
- Astuti, I.; Ysrafi. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): An overview of viral structure and host response. Diabetes Metab. Syndr. 2020, 14, 407–412. [Google Scholar] [CrossRef]
- Li, L.Q.; Huang, T.; Wang, Y.Q.; Wang, Z.P.; Liang, Y.; Huang, T.B.; Zhang, H.Y.; Sun, W.; Wang, Y. COVID-19 patients’ clinical characteristics, discharge rate, and fatality rate of meta-analysis. J. Med. Virol. 2020. [Google Scholar] [CrossRef]
- Zhang, J.J.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Akdis, C.A.; Gao, Y.D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020. [Google Scholar] [CrossRef]
- Chakraborty, C.; Sharma, A.R.; Sharma, G.; Bhattacharya, M.; Lee, S.S. SARS-CoV-2 causing pneumonia-associated respiratory disorder (COVID-19): Diagnostic and proposed therapeutic options. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 4016–4026. [Google Scholar] [CrossRef]
- Tu, Y.F.; Chien, C.S.; Yarmishyn, A.A.; Lin, Y.Y.; Luo, Y.H.; Lin, Y.T.; Lai, W.Y.; Yang, D.M.; Chou, S.J.; Yang, Y.P.; et al. A review of SARS-CoV-2 and the ongoing clinical trials. Int. J. Mol. Sci. 2020, 21, 2657. [Google Scholar] [CrossRef]
- Hassan, S.A.; Sheikh, F.N.; Jamal, S.; Ezeh, J.K.; Akhtar, A. Coronavirus (COVID-19): A review of clinical features, diagnosis, and treatment. Cureus 2020, 12, e7355. [Google Scholar] [CrossRef]
- Law, S.; Leung, A.W.; Xu, C. Severe acute respiratory syndrome (SARS) and coronavirus disease-2019 (COVID-19): From causes to preventions in Hong Kong. Int. J. Inf. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission routes of 2019-nCoV and controls in dental practice. Int. J. Oral Sci. 2020, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Singhal, T. A review of coronavirus disease-2019 (COVID-19). Indian J. Pediatr. 2020, 87, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Malik, Y.A. Properties of coronavirus and SARS-CoV-2. Malays. J. Pathol. 2020, 42, 3–11. [Google Scholar]
- Şimşek-Yavuz, S.; Ünal, S. Antiviral treatment of COVID-19. Turk. J. Med. Sci. 2020, 50, 611–619. [Google Scholar] [CrossRef]
- Lombardy Section Italian Society Infectious and Tropical Diseases. Vademecum for the treatment of people with COVID-19. Infez Med. 2020, 28, 143–152. [Google Scholar]
- Gao, J.; Tian, Z.; Yang, X. Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studies. Biosci. Trends. 2020, 14, 72–73. [Google Scholar] [CrossRef]
- Zhai, P.; Ding, Y.; Wu, X.; Long, J.; Zhong, Y.; Li, Y. The epidemiology, diagnosis and treatment of COVID-19. Int. J. Antimicrob. Agents 2020, 105955. [Google Scholar] [CrossRef]
- Hong, K.H.; Lee, S.W.; Kim, T.S.; Huh, H.J.; Lee, J.; Kim, S.Y.; Park, J.S.; Kim, G.J.; Sung, H.; Roh, K.H.; et al. Guidelines for laboratory diagnosis of coronavirus disease 2019 (COVID-19) in Korea. Ann. Lab. Med. 2020, 40, 351–360. [Google Scholar] [CrossRef]
- Jin, Y.H.; Cai, L.; Cheng, Z.S.; Cheng, H.; Deng, T.; Fan, Y.P.; Fang, C.; Huang, D.; Huang, L.Q.; Huang, Q.; et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil. Med. Res. 2020, 7, 4. [Google Scholar] [CrossRef]
- Li, Y.; Xia, L. Coronavirus disease 2019 (COVID-19): Role of chest CT in diagnosis and management. AJR Am. J. Roentgenol. 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: A report of 1014 cases. Radiology 2020, 200642. [Google Scholar] [CrossRef] [PubMed]
- Vashist, S.K. In vitro diagnostic assays for COVID-19: Recent advances and emerging trends. Diagnostics 2020, 10, 202. [Google Scholar] [CrossRef] [PubMed]
- Petherick, A. Developing antibody tests for SARS-CoV-2. Lancet 2020, 395, 1101–1102. [Google Scholar] [CrossRef]
- Xie, L.X. Interpretation of the 7th edition of the “diagnosis and treatment guidelines of coronavirus disease 2019 in China”: Progress and challenges. Chronic Dis. Transl. Med. 2020. [Google Scholar] [CrossRef]
- Patel, R.; Babady, E.; Theel, E.S.; Storch, G.A.; Pinsky, B.A.; St George, K.; Smith, T.C.; Bertuzzi, S. Report from the american society for microbiology COVID-19 international summit, 23 March 2020: Value of diagnostic testing for SARS-CoV-2/COVID-19. mBio 2020, 11. [Google Scholar] [CrossRef]
- Infectious Diseases Society of America (IDSA). IDSA COVID-19 Antibody Testing Primer. Available online: https://www.idsociety.org/globalassets/idsa/public-health/covid-19/idsa-covid-19-antibody-testing-primer.pdf (accessed on 29 April 2020).
- Bao, L.; Deng, W.; Gao, H.; Xiao, C.; Liu, J.; Xue, J.; Lv, Q.; Liu, J.; Yu, P.; Xu, Y.; et al. Reinfection could not occur in SARS-CoV-2 infected rhesus macaques. bioRxiv 2020. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–34. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 24 April 2020).
- National Health Commission & State Administration of Traditional Chinese Medicine. Diagnosis and Treatment Protocol for Novel Coronavirus Pneumonia (Trial Version 7). Available online: https://www.fmprc.gov.cn/mfa_eng/topics_665678/kjgzbdfyyq/CERC/P020200318837942843337.pdf (accessed on 28 April 2020).
- Cassaniti, I.; Novazzi, F.; Giardina, F.; Salinaro, F.; Sachs, M.; Perlini, S.; Bruno, R.; Mojoli, F.; Baldanti, F. Performance of VivaDiag COVID-19 IgM/IgG Rapid Test is inadequate for diagnosis of COVID-19 in acute patients referring to emergency room department. J. Med. Virol. 2020. [Google Scholar] [CrossRef]
- Infantino, M.; Grossi, V.; Lari, B.; Bambi, R.; Perri, A.; Manneschi, M.; Terenzi, G.; Liotti, I.; Ciotta, G.; Taddei, C.; et al. Diagnostic accuracy of an automated chemiluminescent immunoassay for anti-SARS-CoV-2 IgM and IgG antibodies: An Italian experience. J. Med. Virol. 2020. [Google Scholar] [CrossRef]
- Jin, Y.; Wang, M.; Zuo, Z.; Fan, C.; Ye, F.; Cai, Z.; Wang, Y.; Cui, H.; Pan, K.; Xu, A. Diagnostic value and dynamic variance of serum antibody in coronavirus disease 2019. Int. J. Infect. Dis. 2020, 94, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.L.; Liao, C.H.; Liu, P.Y.; Cheng, C.Y.; Chung, M.Y.; Liu, C.E.; Chang, S.Y.; Hsueh, P.R. Dynamics of anti-SARS-Cov-2 IgM and IgG antibodies among COVID-19 patients. J. Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Yi, Y.; Luo, X.; Xiong, N.; Liu, Y.; Li, S.; Sun, R.; Wang, Y.; Hu, B.; Chen, W.; et al. Development and clinical application of a rapid IgM-IgG combined antibody test for SARS-CoV-2 infection diagnosis. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Li, X.; Yang, G.; Fan, J.; Tang, Y.; Zhao, J.; Long, X.; Guo, S.; Zhao, Z.; Liu, Y.; et al. Serological immunochromatographic approach in diagnosis with SARS-CoV-2 infected COVID-19 patients. J. Infect. 2020. [Google Scholar] [CrossRef]
- Xiang, F.; Wang, X.; He, X.; Peng, Z.; Yang, B.; Zhang, J.; Zhou, Q.; Ye, H.; Ma, Y.; Li, H.; et al. Antibody detection and dynamic characteristics in patients with COVID-19. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J.; et al. Antibody responses to SARS-CoV-2 in patients of novel coronavirus disease 2019. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Yongchen, Z.; Shen, H.; Wang, X.; Shi, X.; Li, Y.; Yan, J.; Chen, Y.; Gu, B. Different longitudinal patterns of nucleic acid and serology testing results based on disease severity of COVID-19 patients. Emerg. Microbes Infect. 2020, 9, 833–836. [Google Scholar] [CrossRef]
- Zhang, W.; Du, R.H.; Li, B.; Zheng, X.S.; Yang, X.L.; Hu, B.; Wang, Y.Y.; Xiao, G.F.; Yan, B.; Shi, Z.L.; et al. Molecular and serological investigation of 2019-nCoV infected patients: Implication of multiple shedding routes. Emerg. Microbes Infect. 2020, 9, 386–389. [Google Scholar] [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of immune response in patients with COVID-19 in Wuhan, China. Clin. Infect. Dis. 2020, 12. [Google Scholar] [CrossRef]
- di Cristina, S.M.G.; Concetta, R.; Francesco, R.; Annalisa, C. SARS-Cov-2 infection: Response of human immune system and possible implications for the rapid test and treatment. Int. Immunopharmacol. 2020, 84, 106519. [Google Scholar] [CrossRef]
- Castro, R.; Luz, P.M.; Wakimoto, M.D.; Veloso, V.G.; Grinsztejn, B.; Perazzo, H. COVID-19: A meta-analysis of diagnostic test accuracy of commercial assays registered in Brazil. Braz J. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Demey, B.; Daher, N.; François, C.; Lanoix, J.-P.; Duverlie, G.; Castelain, S.; Brochot, E. Dynamic profile for the detection of anti-SARS-CoV-2 antibodies using four immunochromatographic assays. J. Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- Thevarajan, I.; Nguyen, T.H.O.; Koutsakos, M.; Druce, J.; Caly, L.; van de Sandt, C.E.; Jia, X.; Nicholson, S.; Catton, M.; Cowie, B.; et al. Breadth of concomitant immune responses prior to patient recovery: A case report of non-severe COVID-19. Nat. Med. 2020, 26, 453–455. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.H.; Baumgarth, N. The multifaceted B cell response to influenza virus. J. Immunol. 2019, 202, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Baumgarth, N. How specific is too specific? B-cell responses to viral infections reveal the importance of breadth over depth. Immunol. Rev. 2013, 255, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Infantino, M.; Damiani, A.; Gobbi, F.L.; Grossi, V.; Lari, B.; Macchia, D.; Casprini, P.; Veneziani, F.; Villalta, D.; Bizzaro, N.; et al. Serological assays for SARS-CoV-2 infectious disease: Benefits, limitations and perspectives. Isr. Med. Assoc. J. 2020, 22, 203–210. [Google Scholar]
- Wu, X.; Fu, B.; Chen, L.; Feng, Y. Serological tests facilitate identification of asymptomatic SARS-CoV-2 infection in Wuhan, China. J. Med. Virol. 2020. [Google Scholar] [CrossRef]
- Cheng, M.P.; Papenburg, J.; Desjardins, M.; Kanjilal, S.; Quach, C.; Libman, M.; Dittrich, S.; Yansouni, C.P. Diagnostic testing for severe acute respiratory syndrome-related Coronavirus-2: A narrative review. Ann. Intern. Med. 2020. [Google Scholar] [CrossRef]


{kind=link}
| Studies | Definition of Cases | Representativeness of Cases | Selection of Controls | Definition of Controls | Comparability | Exposure | Total |
|---|---|---|---|---|---|---|---|
| Cassaniti et al. 2020 | + | + | + | + | +− | ++− | 7 |
| Infantino et al. 2020 | + | + | + | + | +− | +−− | 6 |
| Jin et al. 2020 | + | + | + | + | +− | ++− | 7 |
| Lee et al. 2020 | + | + | + | + | +− | ++− | 7 |
| Li et al. 2020 | + | + | + | + | +− | ++− | 7 |
| Pan et al. 2020 | + | + | − | − | +− | ++− | 5 |
| Xiang et al. 2020 | + | + | + | + | +− | ++− | 7 |
| Yongchen et al. 2020 | + | + | − | − | +− | ++− | 5 |
| Zhang et al. 2020 | + | + | − | − | +− | ++− | 5 |
| Zhao et al. 2020 | + | + | − | − | +− | ++− | 5 |
| Study | Number of Enrolled Subjects/Blood Samples | Diagnosis of SARS-CoV-2 | Patient/Blood Sample Source | Serological Test |
|---|---|---|---|---|
| Cassaniti et al. 2020 | 110 subjects: 30 healthy volunteers 30 positive patients * 50 patients with fever and respiratory syndrome | Respiratory samples tested by real-time RT-PCR | Fondazione IRCCS Policlinico San Matteo | VivaDiag COVID-19 IgM/IgG Rapid Test LFIA |
| Infantino et al. 2020 | 125 subjects: 61 positive patients * 64 negative controls | Oropharyngeal and nasopharyngeal swabs tested by RT-PCR | San Giovanni di Dio Hospital (Florence, Italy) | iFlash1800 fully automated CLIA analyzer from Shenzhen YHLO Biotech Co., Ltd. (China) |
| Jin et al. 2020 | 76 subjects: 43 positive patients * 33 patients with suspected infection (control group) | Oral swab or sputum tested by real-time RT-PCR | XiXi Hospital of Hangzhou (Zhejiang Province, China) | iFlash3000 fully automated CLIA analyzer from Shenzhen YHLO Biotech Co., Ltd. (China) |
| Lee et al. 2020 | 42 subjects: 14 positive patients */33 serum samples 28 negative controls/28 serum samples | Oropharyngeal and nasopharyngeal swabs, oral gargling and sputum tested by real-time RT-PCR for SARS-CoV-2 | Enrolled patients were treated at six hospitals in Taiwan between January and March 2020 | ALLTEST 2019-nCoV IgM/IgG Rapid Test Cassette (Hangzhou ALLTEST Biotech Co., Ltd. Hangzhou, China) |
| Li et al. 2020 | 525 subjects: 397 positive patients * 128 negative controls | Guideline for diagnosis and treatment of COVID-19 | Eight hospitals and Chinese CDC agencies | SARS-CoV-2 rapid IgM/IgG combined antibody test (LFIA) kit designed and manufactured by Jiangsu Medomics Medical Technologies (Nanjing, China) |
| Pan et al. 2020 | 104 subjects: 67 positive patients */86 serum samples subjects: 37 clinically diagnosed patients/39 serum samples | Throat swab tested by real-time RT-PCR for SARS-CoV-2 | Zhongnan Hospital of Wuhan University (Hubei, China) | Colloidal gold-based immunochromatographic (ICG) strip targeting IgM/IgG, conducted in Zhongnan Hospital of Whuan University (Hubei, China) |
| Xiang et al. 2020 | 169 subjects: 85 positive patients */216 blood samples 24 patients with suspected infection 60 negative controls | Nasopharyngeal and/or oropharyngeal swab samples tested by RT-PCR for SARS-CoV-2 | Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (China) | ELISA kits, Livzon Inc, Zhuhai, P.R.China, lot number of IgM: 20200308, IgG: 20200308 |
| Yongchen et al. 2020 | 21 positive patients *: 11 non-severe 5 severe 5 asymptomatic | Throat swabs samples tested by real-time RT-PCR for SARS-CoV-2 | Second Hospital of Nanjing and Affiliated Hospital of Xuzhou Medical University (Jiangsu Province, China) | Gold immunochromatography assay supplied by Innovita Co., LTd, China (CFDA approved) |
| Zhang et al. 2020 | 16 positive patients * | Oral, anal and blood samples tested by qPCR | Wuhan Pulmonary Hospital (China) | In-house anti-SARS-CoV IgG/IgM ELISA kits (using a cross-reactive nucleocapsid protein from another SARS-related virus Rp3, which is 92% identical to COVID-2019 nucleocapsid protein) |
| Zhao et al. 2020 | 535 serial plasma samples from 173 positive patients * | Respiratory tract samples tested by real-time RT-PCR | Shenzhen Third People’s Hospital (China) | ELISA kits supplied by Beijing Wantai Biological Pharmacy Enterprise Co.,Ltd, |
| Study | Total Sample | IgM/IgG-Positive Patients | IgM/IgG-Negative Patients | IgM-Positive | IgG-Positive |
|---|---|---|---|---|---|
| [32] | 30 | 19/30 (63.3%) 5/30 (16.7%) weakly positive | 5/30 (16.7%) | 1/30 (3.3%): IgM-positive and IgG-negative | |
| [33] | 64 | 41/64 (64.1%) | 3/64 (4.7%) | 5/64 (7.8%) | |
| [34] | 27 | 3/27 (11.1%) | 13/27 (48%) | 24/27 (88.9%) | |
| [35] | 6 with symptoms 8 without symptoms/mild symptoms | 4/6 (66.6%) 0/8 (0%) | 6/6 (100%) 3/8 (37.5%) | ||
| [36] | 397 | 256/397 (64.4%) | 72/397 (18%) | 24/397 (6.04%) | |
| [37] | 86 blood samples | 48/86 (55.8%) | 47/86 (54.7%) | ||
| [38] | 66 | 51/66 (77.2%) | 55/66 (83.3%) | ||
| [39] | 173 | 143/173 (82.7%) | 112/173 (64.7%) |
| Study | Total Sample | IgM/IgG-Positive Patients | IgM/IgG-Negative Patients | IgM-Positive | IgG-Positive |
|---|---|---|---|---|---|
| [32] | 50 patients at their first access to emergency department, later tested for COVID-19 by RT-PCR: 12 negative 38 positive | 1/12 negative patients (8.3%) 7/38 positive patients (18.4%) | 31/38 positive patients | ||
| [37] | 22 blood samples | 8/22 (36.4%) | 13/22 (59.1%) | ||
| [38] | 24 | 21/24 (87.5%) | 17/24 (70.8%) |
| P | Total Sample | IgM/IgG-Positive Patients | IgM/IgG-Negative Patients | IgM-Positive | IgG-Positive |
|---|---|---|---|---|---|
| [32] | 30 | 30 (100%) | |||
| [34] | 33 | 0 (0%) | 3 (9.1%) | ||
| [35] | 28 | 28 (100%) | |||
| [36] | 128 | 1/128 (0.7%) | 10/128 (7.8%) | 1/128 (0.7%) | |
| [38] | 60 | 0/60 (0%) | 3/60 (5%) |
| Serological Test | Number of Collected Blood Samples | Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value |
|---|---|---|---|---|---|
| VivaDiag COVID-19 IgM/IgG Rapid Test LFIA | 18.4% ** | 91.7% ** | 87.5% ** | 26.2% ** | |
| iFlash1800 fully automated CLIA analyzer from Shenzhen YHLO Biotech Co., Ltd. (China) | 73.3% (IgM) 76.7% (IgG) | 92.2% (IgM) 100% (IgG) | 81.5% (IgM) 100% (IgG) | 88.1% (IgM) 92.8% (IgG) | |
| iFlash3000 fully automated CLIA analyzer from Shenzhen YHLO Biotech Co., Ltd. (China): | 43 positive patients→98 samples | 48.1% (IgM) * 88.9% (IgG) * | 100% (IgM) * 90.9% (IgG) * | 100% (IgM) * 88.9% (IgG) * | 70.2% (IgM) * 90.9% (IgG) * |
| ALLTEST 2019-nCoV IgM/IgG Rapid Test Cassette (Hangzhou ALLTEST Biotech Co., Ltd. Hangzhou, China) | 14 positive patients→33 samples 28 controls →28 samples | 90.9% (IgM) * 99.9% (IgG) * | 97.0% (IgM) * 98.0% (IgG) * | ||
| SARS-CoV-2 rapid IgM/IgG combined antibody test kit designed and manufactured by Jiangsu Medomics Medical Technologies (Nanjing, China) | 397 positive patients→397 samples 128 controls→128 samples | 88.66% * | 90.63% *** | ||
| ELISA kits, Livzon Inc, Zhuhai, P.R.China, lot number of IgM: 20200308, IgG: 20200308 | 85 positive patients→216 samples | 77.3% (IgM) * 83.3% (IgG) * 100% (IgM) ** 96.6% (IgG) ** | 100% (IgM) * 94.8% (IgG) * 87.5% (IgM) 70.8% (IgG) | 100% (IgM) * 83.8% (IgG) * 100% (IgM) 85.0% (IgG) | 80.0% (IgM) * 88.9% (IgG) * 95.2% (IgM) 89.1% (IgG) |
| ELISA kits supplied by Beijing Wantai Biological Pharmacy Enterprise Co., Ltd. | 173 positive patients→535 samples | 66.7% (early phase of illness) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carinci, F.; Moreo, G.; Limongelli, L.; Testori, T.; Lauritano, D. Diagnostic Performance of Serological Assays in the Detection of SARS-CoV-2: A Review. Appl. Sci. 2020, 10, 4506. https://doi.org/10.3390/app10134506
Carinci F, Moreo G, Limongelli L, Testori T, Lauritano D. Diagnostic Performance of Serological Assays in the Detection of SARS-CoV-2: A Review. Applied Sciences. 2020; 10(13):4506. https://doi.org/10.3390/app10134506
Chicago/Turabian StyleCarinci, Francesco, Giulia Moreo, Luisa Limongelli, Tiziano Testori, and Dorina Lauritano. 2020. "Diagnostic Performance of Serological Assays in the Detection of SARS-CoV-2: A Review" Applied Sciences 10, no. 13: 4506. https://doi.org/10.3390/app10134506
APA StyleCarinci, F., Moreo, G., Limongelli, L., Testori, T., & Lauritano, D. (2020). Diagnostic Performance of Serological Assays in the Detection of SARS-CoV-2: A Review. Applied Sciences, 10(13), 4506. https://doi.org/10.3390/app10134506