A Novel Approach Using Customized Miniplates as Skeletal Anchorage Devices in Growing Class III Patients: A Case Report


 and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Case Report
2.1. Diagnosis and Etiology
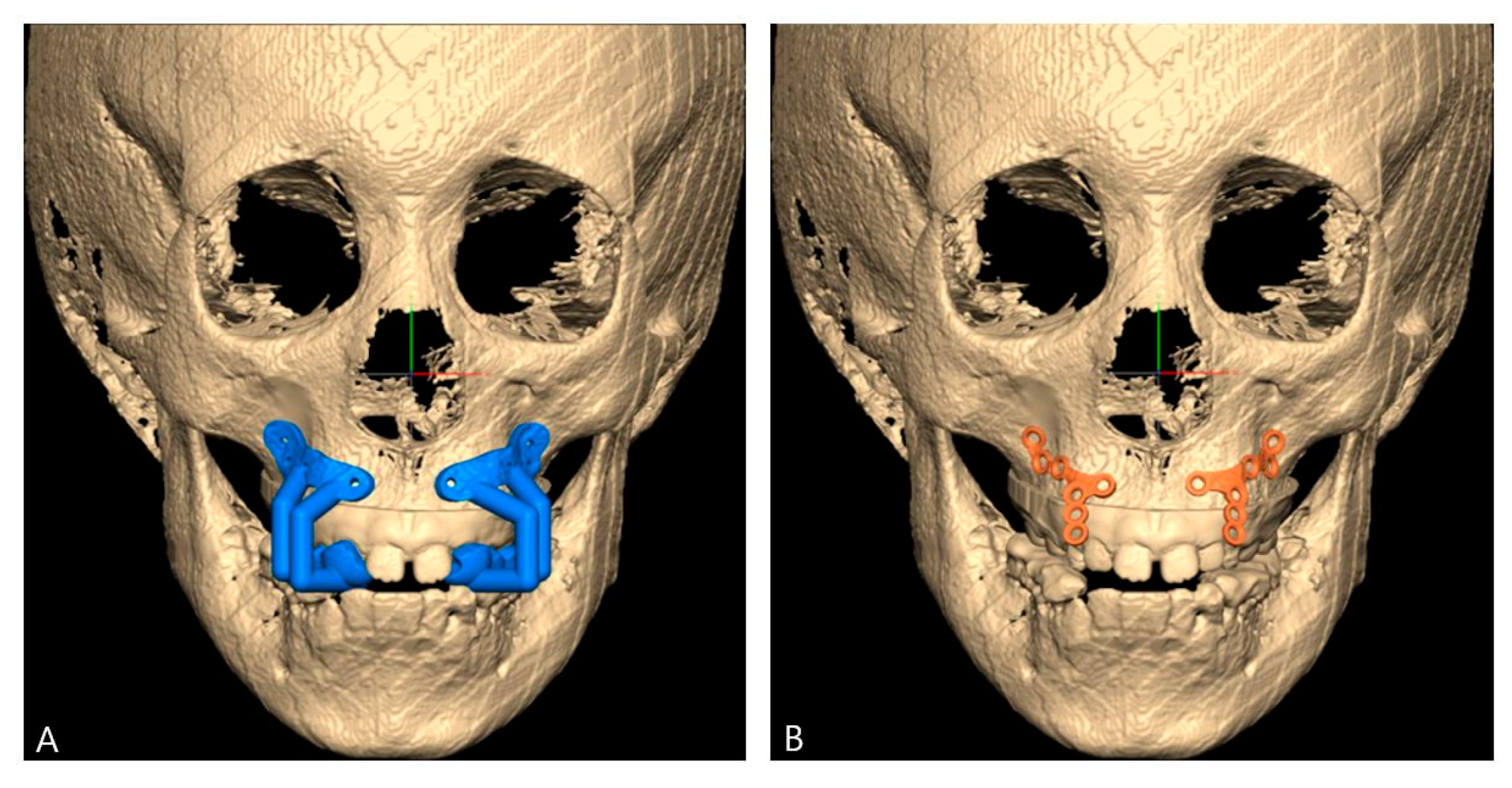
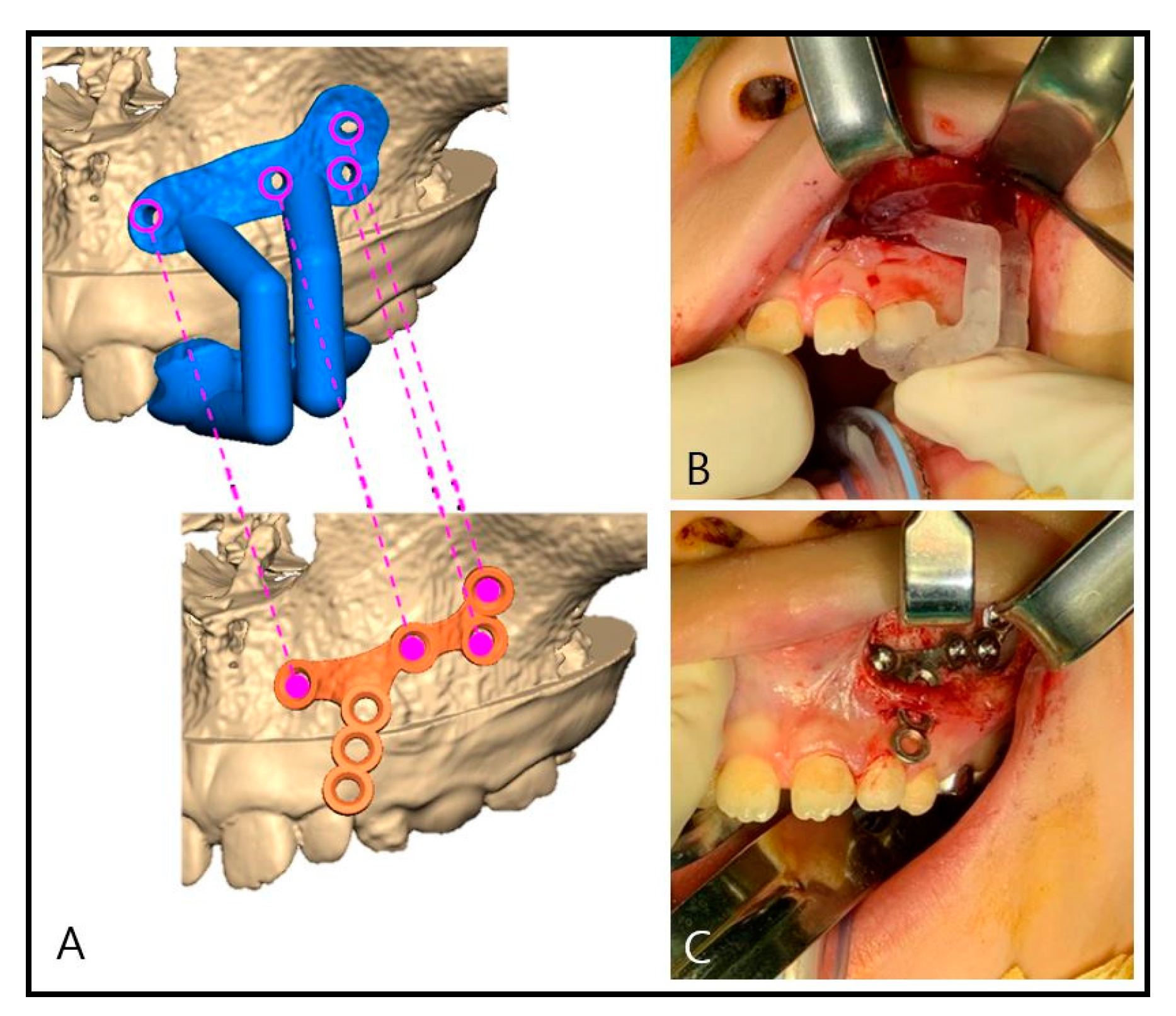
2.2. Computer-Assisted Surgical Planning
2.3. Surgical Procedure
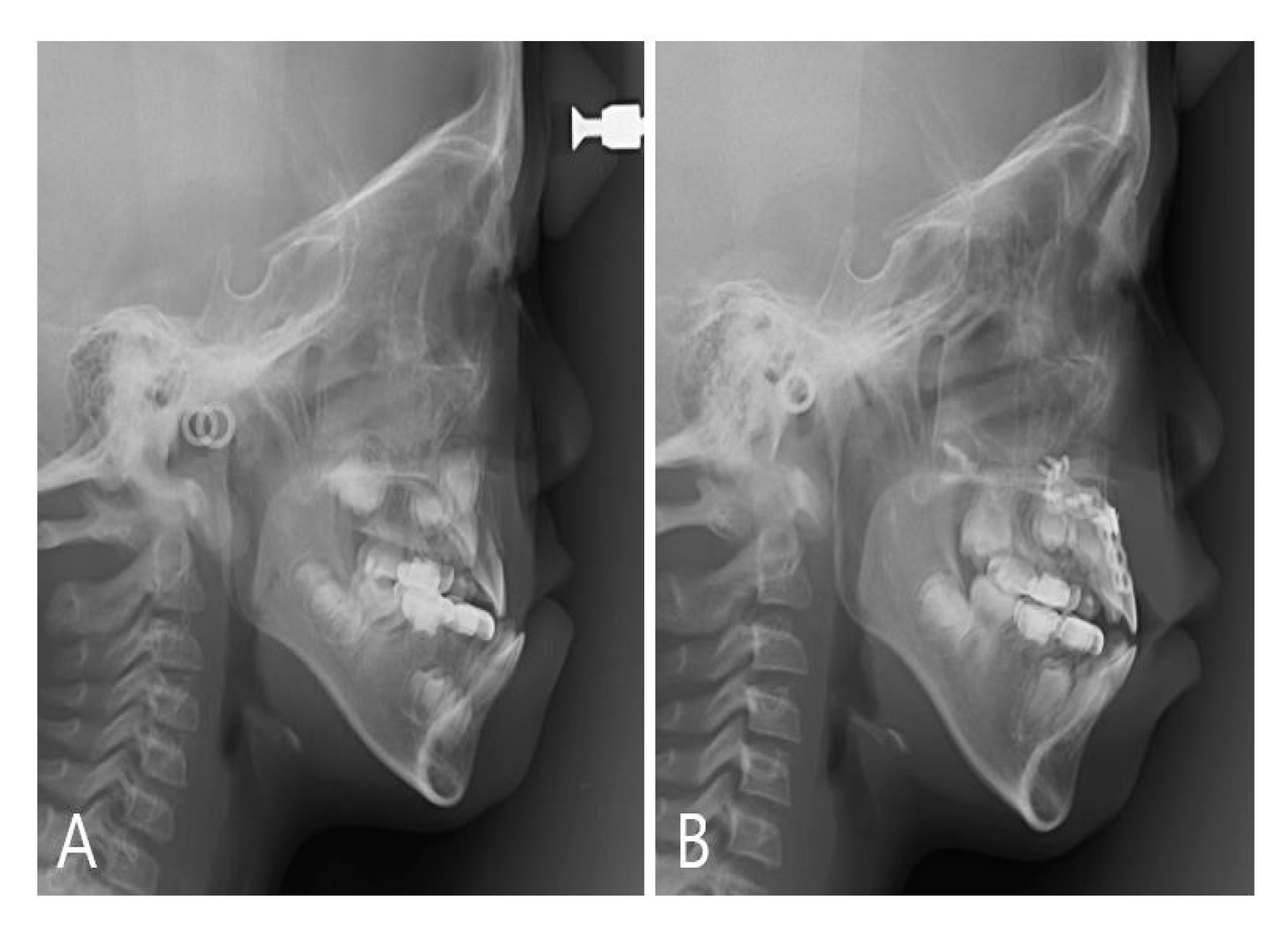
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kambara, T. Dentofacial changes produced by extraoral forward force in the Macaca irus. Am. J. Orthod. 1977, 71, 249–277. [Google Scholar] [CrossRef]
- Cha, B.-K.; Ngan, P.W. Skeletal Anchorage for Orthopedic Correction of Growing Class III Patients. Semin. Orthod. 2011, 17, 124–137. [Google Scholar] [CrossRef]
- Kapust, A.J.; Sinclair, P.M.; Turley, P.K. Cephalometric effects of face mask/expansion therapy in Class III children: A comparison of three age groups. Am. J. Orthod. Dentofac. Orthop. 1998, 113, 204–212. [Google Scholar] [CrossRef]
- Hickham, J.H. Maxillary protraction therapy: Diagnosis and treatment. J. Clin. Orthod. 1991, 25, 102–113. [Google Scholar] [PubMed]
- Smalley, W.M.; Shapiro, P.A.; Hohl, T.H.; Kokich, V.G.; Branemark, P.I. Osseointegrated titanium implants for maxillofacial protraction in monkeys. Am. J. Orthod. Dentofac. Orthop. 1988, 94, 285–295. [Google Scholar] [CrossRef]
- Cha, B.K.; Choi, D.S.; Ngan, P.; Jost-Brinkmann, P.G.; Kim, S.M.; Jang, I.S. Maxillary protraction with miniplates providing skeletal anchorage in a growing Class III patient. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Cope, J.B. Temporary anchorage devices in orthodontics: A paradigm shift. Semin. Orthod. 2005, 11, 3–9. [Google Scholar] [CrossRef]
- Branemark, P.I. Osseointegration and its experimental background. J. Prosthet Dent. 1983, 50, 399–410. [Google Scholar] [CrossRef]
- Chen, Y.J.; Chang, H.H.; Huang, C.Y.; Hung, H.C.; Lai, E.H.; Yao, C.C. A retrospective analysis of the failure rate of three different orthodontic skeletal anchorage systems. Clin. Oral Implant. Res. 2007, 18, 768–775. [Google Scholar] [CrossRef]
- Kimura, A.; Nagasan, T.; Kaneko, T.; Miyamoto, J.; Nakajima, T. A comparative study of most suitable miniplate fixation for mandibular symphysis fracture using a finite element model. Keio J. Med. 2006, 55, 1–8. [Google Scholar] [CrossRef][Green Version]
- Kim, J.W.; Kim, J.C.; Jeong, C.G.; Cheon, K.J.; Cho, S.W.; Park, I.Y.; Yang, B.E. The accuracy and stability of the maxillary position after orthognathic surgery using a novel computer-aided surgical simulation system. BMC Oral Health 2019, 19, 18. [Google Scholar] [CrossRef] [PubMed]
- Lancellotta, V.; Pagano, S.; Tagliaferri, L.; Piergentini, M.; Ricci, A.; Montecchiani, S.; Saldi, S.; Chierchini, S.; Cianetti, S.; Valentini, V.; et al. Individual 3-dimensional printed mold for treating hard palate carcinoma with brachytherapy: A clinical report. J. Prosthet. Dent. 2019, 121, 690–693. [Google Scholar] [PubMed]
- Lee, N.K.; Yang, I.H.; Baek, S.H. The short-term treatment effects of face mask therapy in Class III patients based on the anchorage device: Miniplates vs rapid maxillary expansion. Angle Orthod. 2012, 82, 846–852. [Google Scholar] [PubMed]
- Sar, C.; Arman-Ozcirpici, A.; Uckan, S.; Yazici, A.C. Comparative evaluation of maxillary protraction with or without skeletal anchorage. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 636–649. [Google Scholar]
- Woo, I.H.; Kim, J.W.; Kim, J.Y.; Yang, B.E. A New Method of Fixation with the Yang’s Keyhole Plate System for the Treatment of Mandible Fractures. J. Craniofacial Surg. 2017, 28, 508–512. [Google Scholar]
- Liu, Y.F.; Fan, Y.Y.; Jiang, X.F.; Baur, D.A. A customized fixation plate with novel structure designed by topological optimization for mandibular angle fracture based on finite element analysis. Biomed. Eng. Online 2017, 16, 131. [Google Scholar]
- Kanomi, R. Mini-implant for orthodontic anchorage. J. Clin. Orthod. 1997, 31, 763–767. [Google Scholar]
- Crismani, A.G.; Bertl, M.H.; Celar, A.G.; Bantleon, H.P.; Burstone, C.J. Miniscrews in orthodontic treatment: Review and analysis of published clinical trials. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, S.; Yamada, K.; Deguchi, T.; Hashimoto, T.; Kyung, H.M.; Takano-Yamamoto, T. Root proximity is a major factor for screw failure in orthodontic anchorage. Am. J. Orthod. Dentofac. Orthop. 2007, 131, S68–S73. [Google Scholar]
- Sugawara, J.; Nishimura, M. Minibone plates: The skeletal anchorage system. Semin. Orthod. 2005, 11, 47–56. [Google Scholar] [CrossRef]
- Lee, H.S.; Choi, H.M.; Choi, D.S.; Jang, I.; Cha, B.K. Bone thickness of the infrazygomatic crest area in skeletal Class III growing patients: A computed tomographic study. Imaging Sci. Dent. 2013, 43, 261–266. [Google Scholar] [CrossRef] [PubMed]
- De Clerck, H.; Geerinckx, V.; Siciliano, S. The Zygoma Anchorage System. J. Clin. Orthod. 2002, 36, 455–459. [Google Scholar] [PubMed]
- Kaya, B.; Arman, A.; Uckan, S.; Yazici, A.C. Comparison of the zygoma anchorage system with cervical headgear in buccal segment distalization. Eur. J. Orthod. 2009, 31, 417–424. [Google Scholar] [CrossRef] [PubMed]









© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryu, J.-I.; Cho, S.-W.; Oh, S.-H.; Park, I.-Y.; Kim, J.-W.; Byun, S.-H.; Yang, B.-E. A Novel Approach Using Customized Miniplates as Skeletal Anchorage Devices in Growing Class III Patients: A Case Report. Appl. Sci. 2020, 10, 4067. https://doi.org/10.3390/app10124067
Ryu J-I, Cho S-W, Oh S-H, Park I-Y, Kim J-W, Byun S-H, Yang B-E. A Novel Approach Using Customized Miniplates as Skeletal Anchorage Devices in Growing Class III Patients: A Case Report. Applied Sciences. 2020; 10(12):4067. https://doi.org/10.3390/app10124067
Chicago/Turabian StyleRyu, Ji-In, Seoung-Won Cho, So-Hee Oh, In-Young Park, Ju-Won Kim, Soo-Hwan Byun, and Byoung-Eun Yang. 2020. "A Novel Approach Using Customized Miniplates as Skeletal Anchorage Devices in Growing Class III Patients: A Case Report" Applied Sciences 10, no. 12: 4067. https://doi.org/10.3390/app10124067
APA StyleRyu, J.-I., Cho, S.-W., Oh, S.-H., Park, I.-Y., Kim, J.-W., Byun, S.-H., & Yang, B.-E. (2020). A Novel Approach Using Customized Miniplates as Skeletal Anchorage Devices in Growing Class III Patients: A Case Report. Applied Sciences, 10(12), 4067. https://doi.org/10.3390/app10124067